
Abstract
Fetiform teratoma (FT) and fetus-in-fetu (FIF) represent a spectrum of rare retroperitoneal masses containing organoid structures. While FIF is classically defined by the presence of a vertebral axis, FT lacks this organized skeletal development. Distinguishing between these entities is critical given the malignant potential associated with FT, estimated at approximately 10%. We report a case of a 5-month-old male presenting with a large (12 cm) retroperitoneal mass and elevated alpha-fetoprotein (AFP 56.8 IU/mL; age-matched reference <7 IU/mL). Macroscopically, the resected tumor featured a distinct rudimentary digitiform projection with a nail bed. Histopathology demonstrated extensive organoid differentiation, including gastrointestinal loops with muscular layers, respiratory epithelium, and well-formed pancreatic parenchyma and adrenal cortex. Despite the complex organogenesis and limb-like morphology, the absence of a vertebral column or ossified long bones supported a diagnosis of mature cystic teratoma with fetiform features (FT) over FIF. This report highlights the diagnostic ambiguity within the “gray zone” of these lesions and emphasizes the role of axial skeletal organization and serum AFP levels as complementary tools for classification and oncologic surveillance.
Keywords
Introduction
Infantile retroperitoneal masses include fetiform teratoma (FT) and fetus-in-fetu (FIF). Traditionally, Willis’s criteria (1935) define FIF by the presence of a vertebral column, representing a parasitic monozygotic twin. 1 Conversely, FT is a highly organized mature teratoma lacking axial skeletal organization.
However, recent systematic reviews and molecular theories suggest that FT and FIF likely exist on the pathological continuum rather than as distinct entities.2,3 While FIF is generally benign and curable by excision, FT carries a potential for malignancy (approximately 10%) or recurrence, necessitating accurate classification.2,4 We present a case of a giant retroperitoneal mass in a male infant that challenges the traditional binary classification. The tumor exhibited a “digit-like” appendage and complex organogenesis (including adrenal and pancreatic tissues) typical of FIF, yet lacked a vertebral axis and presented with elevated alpha-fetoprotein, fulfilling the criteria for FT.
Case Report
A 5-month-old male infant (born at term, unremarkable perinatal course) presented with progressive abdominal distension and regurgitation. No clinical features suggestive of syndromic associations were observed, and as such specific genetic screening modalities (karyotype or microarray) were not performed. Physical examination revealed a palpable, large, firm abdominal mass.
Abdominal ultrasound and subsequent contrast-enhanced computed tomography revealed a massive, heterogeneous retroperitoneal mass measuring approximately 12 cm × 10 cm × 9.7 cm. The lesion demonstrated varying attenuation values corresponding to macroscopic fat components, multiple coarse polymorphic calcifications, and mixed cystic and solid areas. The tumor was accompanied by significant homogeneous ascites and exerted a dramatic mass effect, displacing most peritoneal and retroperitoneal structures to the right hemiabdomen. Notably, the left kidney was displaced into the right iliac fossa, and the pancreas was pushed anterolaterally to the right. The stomach and bowel loops were also significantly deviated, a presentation pattern consistent with a mature teratoma by imaging, as observed in complex infantile retroperitoneal masses4,5 (Figure 1).
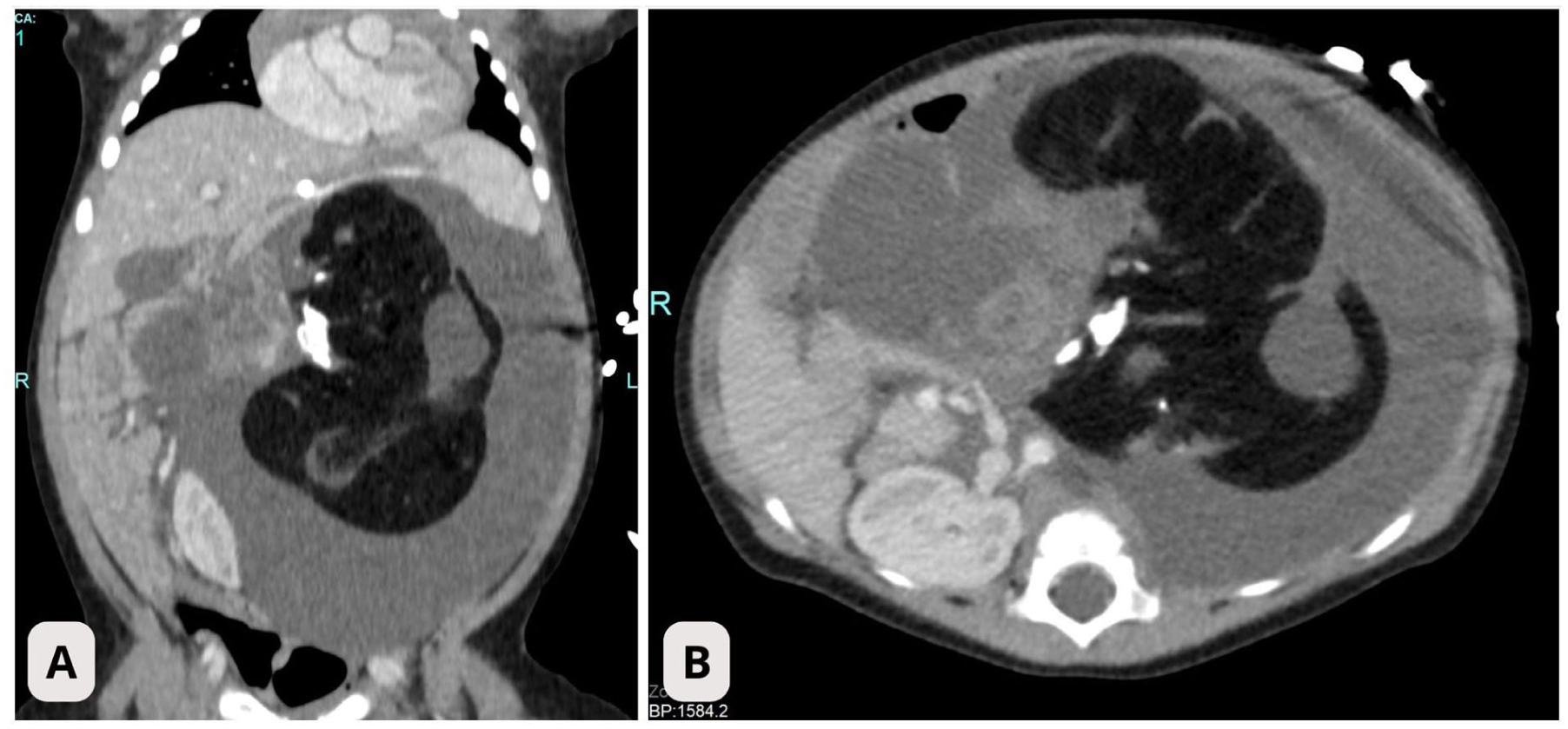
Preoperative imaging. Coronal (A, left) and axial (B, right) views of contrast-enhanced abdominal computed tomography showing a massive, heterogeneous retroperitoneal mass. The lesion exhibits varied attenuation values consistent with macroscopic fat, coarse calcifications, and cystic areas. There is a significant mass effect displacing the left kidney and intestinal loops toward the right hemiabdomen, accompanied by prominent ascites.
Preoperative serum alpha-fetoprotein (AFP) was 56.8 IU/mL (reference <7.0 IU/mL). Other markers, including beta-human chorionic gonadotropin (β-HCG) and lactate dehydrogenase (LDH), were within expected infant ranges, which supported the exclusion of more aggressive germ cell tumors or non-teratomatous elements. The patient underwent a transverse laparotomy. The mass was found to be encapsulated, retroperitoneal, and surrounded by yellowish fluid. Complete excision was performed.
The patient was discharged in stable condition on postoperative day 5. Although post-operative serum AFP monitoring was not available in the records, clinical and radiological follow-up at 31 months confirmed anatomical restitution of the kidneys with no evidence of residual or recurrent disease.
Pathological Findings
The resected specimen consisted of a cystic structure with thin walls containing a solid, ovoid mass. A specimen radiograph was not performed. However, the presence of a vertebral axis was rigorously excluded through serial macroscopic sectioning of the entire specimen at 0.5 cm intervals and subsequent histological examination of representative sections of solid and skeletal components. Sections containing bony and cartilaginous elements were subjected to standard decalcification to facilitate precise histological analysis.
The most striking feature was a 3 cm × 1 cm × 1 cm external projection with clear digitiform morphology, covered by skin and presenting a structure compatible with a nail bed (Figure 2(A)). Serial sectioning and histological examination of this rudimentary appendage confirmed an organized architecture with epidermis, dermis, subcutaneous fat, and a central core of cartilage representing a developing phalanx (ossification was absent), supporting the fetiform architectural pattern of the mass (Figure 2(B)).
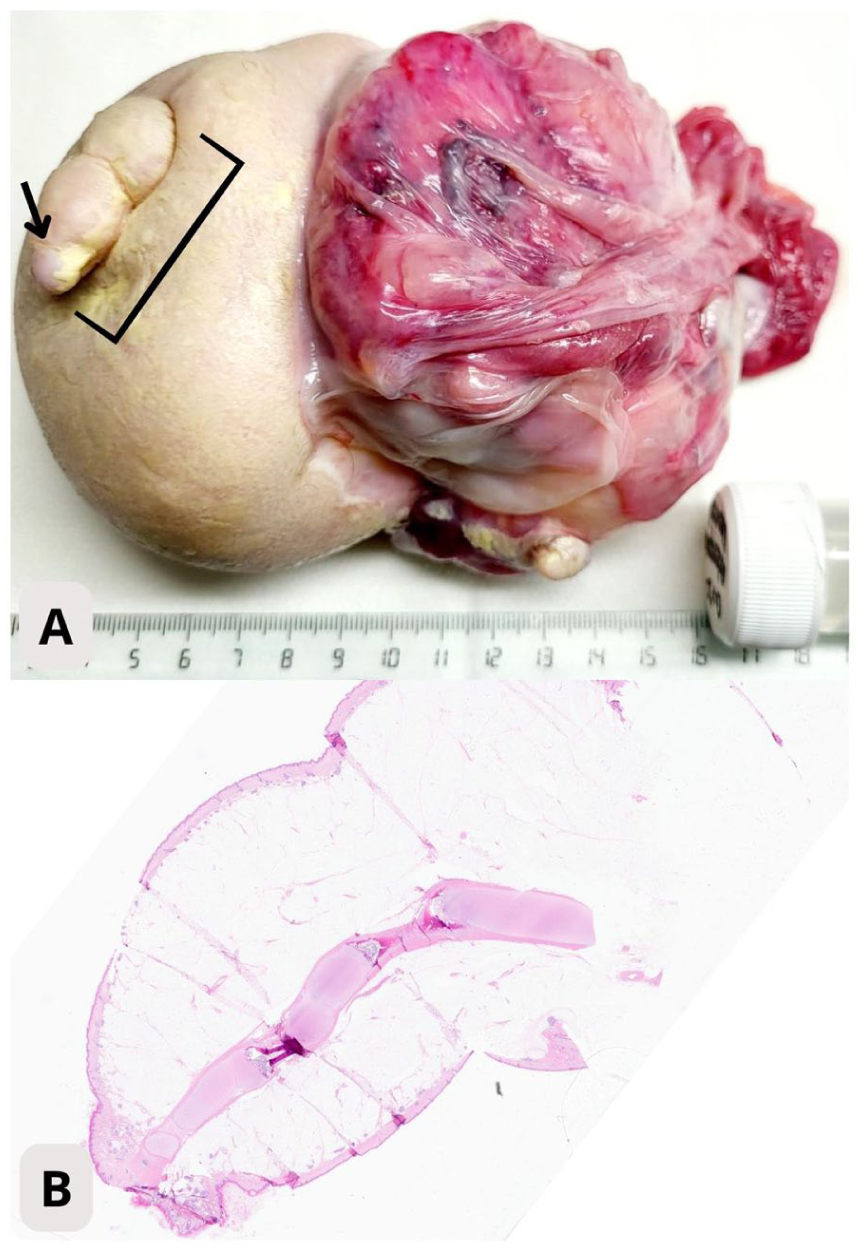
Macroscopic and microscopic correspondence of the digitiform projection. (A) Gross appearance of the resected tumor showing a distinct skin-covered projection (bracket) resembling a rudimentary appendage. Note the presence of a structure compatible with a nail bed at the distal tip (arrow). (B) Low-power histological view (panoramic scan, hematoxylin & eosin, original magnification ×10) of the rudimentary appendage confirming organized architecture with epidermis, dermis, subcutaneous fat, and a central core of cartilage representing a developing phalanx.
Microscopic analysis showed a disorganized yet distinct arrangement of mature tissues from all 3 germ layers:
Despite extensive sampling, no vertebral column, notochordal tissue, or primitive streak elements were identified. Immature neuroepithelium was absent. Given the lack of a vertebral axis, the lesion was diagnosed as a mature cystic teratoma with fetiform features (FT).
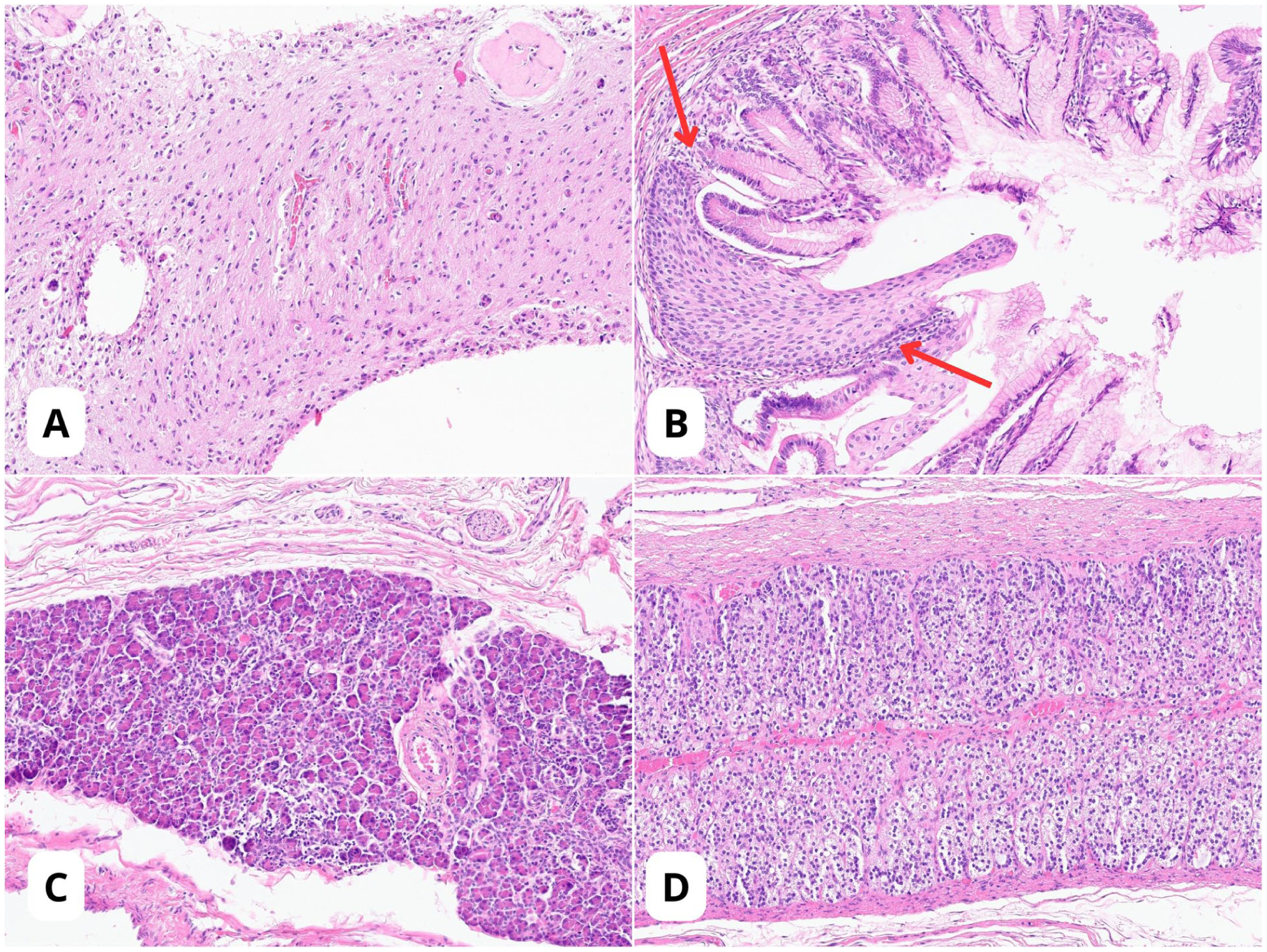
Representative histopathological findings (hematoxylin & eosin, original magnification ×200). The tumor demonstrates remarkable organoid differentiation. (A) Ectoderm: Mature glial tissue with a fibrillary background. (B) Endoderm (gastrointestinal): A striking squamocolumnar junction (red arrows) where stratified squamous epithelium transitions into columnar glandular mucosa, mimicking a gastroesophageal junction. (C) Endoderm (pancreas): Well-defined lobules of pancreatic parenchyma composed of serous acini. (D) Mesoderm (adrenal): Nests of cells with clear, lipid-rich cytoplasm and central nuclei, morphologically characteristic of adrenal cortical tissue.
Written informed consent for publication of the case details and accompanying images was obtained from the patient’s parents.
Discussion
The distinction between FT and FIF is often debated. Historically, the presence of a vertebral column has been the classic pathognomonic sign of FIF, indicating the prior existence of a primitive streak or axial skeleton.1,7 However, rare cases of FT—like the 1 presented here, or the “homunculus” found in ovarian teratomas 8 —exhibit a degree of organization that may mimic fetal morphology without axial skeletal development. For the practicing pathologists, these cases underscore how advanced organoid differentiation in teratomas can obscure traditional boundaries, directly affecting patient management.
Diagnostic Criteria and the Gray Zone
Palo et al 2 recently refined diagnostic criteria, labeling masses as FIF only if they possess a vertebral column or ossified long tubular limb bones. Our case highlights this dilemma: despite a rudimentary digitiform structure with phalangeal cartilage and complex organogenesis (pancreas and adrenal), the lack of ossified bones confirms the FT diagnosis. This places the tumor in the “gray zone” described by Morovic et al, 9 where FT achieves advanced organoid organization—resembling a malformed fetus—without crossing the threshold into the axial organization of a parasitic twin.
Current molecular theories support this “continuum” concept. Both FT and FIF have been linked to methylation defects in imprinted loci, specifically the overexpression of IGF2 and hypomethylation of H19 on chromosome 11p15.5. 10 These shared molecular alterations suggest that FIF and FT may represent different degrees of maturation of the same developmental anomaly, where FIF achieves a higher level of organization potentially due to a later onset of developmental arrest.
Conversely, cases like that of Araújo Couto et al, 3 where a second head with brain tissue was identified without a spine, show that organization can occur in the cephalic pole independently of the axis. Crucially, this case confirms that advanced organoid differentiation alone does not warrant a classification of FIF if the axial skeletal framework is absent.
The Role of AFP
Serum AFP levels may provide valuable diagnostic clues, although they must be interpreted cautiously given the wide reference ranges in infants. In confirmed cases of FIF, AFP levels are often markedly elevated (e.g., >3000 IU/mL in neonates), reflecting the presence of a functional fetal liver within the parasitic mass. 4 In our patient, the AFP level (56.8 IU/mL) was only moderately elevated, which is more characteristic of FT. Therefore, in ambiguous fetiform lesions, AFP levels may serve as a complementary biomarker for diagnosis and follow-up, particularly where molecular profiling is unavailable.
Prognostic Implications
Accurate classification is vital; while FIF is a benign anomaly cured by resection, FT is a true neoplasm with a reported potential for malignancy or recurrence estimated at 10%. 2 Although the risk is significantly lower for entirely mature FT without immature elements or yolk sac components, close oncological surveillance remains mandatory. Misclassifying FT as FIF could lead to premature cessation of follow-up. Thus, despite a benign histological appearance in our case, the patient requires serial AFP monitoring and imaging.
A limitation of this report is the absence of molecular genotyping to assess zygosity or specific methylation patterns and detailed post-operative AFP tracking. However, the long-term disease-free survival (31 months) supports the benign nature of the resected lesion. Although molecular analysis is increasingly valuable for distinguishing these entities, in resource-limited settings or clear morphological cases, the combination of Willis’s criteria and serum AFP levels provides a robust and clinically safe diagnostic framework.
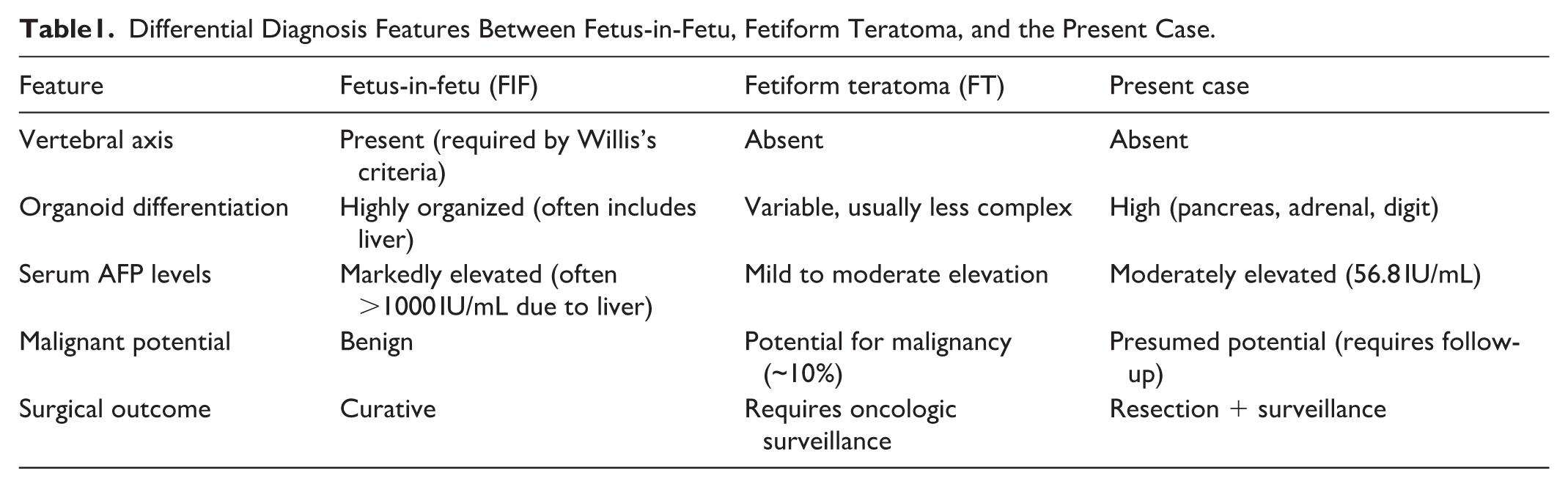
The key distinguishing features between classic FIF, FT, and the characteristics observed in the present case are summarized in Table 1.
Differential Diagnosis Features Between Fetus-in-Fetu, Fetiform Teratoma, and the Present Case.
This case shows that FT can achieve exceptional organoid differentiation while remaining biologically distinct from FIF. Distinguishing these entities is essential for prognosis and surveillance. Axial skeletal assessment, organ development, and serum AFP remain the cornerstones of this diagnostic challenge.
Footnotes
Acknowledgements
We thank the multidisciplinary team at Hospital Balmis for their collaboration.
Author Note
ORCID iDs
Ethical Considerations
IRB approval waived by Hospital Balmis (case report).
Consent for Publication
Written informed consent for publication obtained from the patient’s representative.
Author Contributions
SS and LGS: drafting, literature review, and figures. JGP: clinical data. DPCM: radiology. MFPM and GPC: diagnosis and supervision. All authors approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration of Generative AI
ChatGPT was used for language clarity; take full responsibility for the content.