
Abstract
Rhabdomyomatous mesenchymal hamartoma (RMH) is a rare congenital malformation. We report a case involving a 20-month-old girl who presented with a congenital midline philtral mass. Histopathological examination revealed mature striated muscle fibers interspersed with adipose tissue and prominent adnexal structures, including sebaceous glands originating from hair follicles. The lesion’s prominent folliculosebaceous components initially suggested folliculosebaceous cystic hamartoma (FSCH). However, the presence of striated muscle hyperplasia, midline location, congenital onset, and the absence of characteristic cleft formation confirmed the diagnosis of RMH. The patient underwent complete surgical excision and was recurrence-free after 5 years of follow-up. This case highlights the importance of considering RMH in the differential diagnosis of congenital midline facial lesions, including those with adnexal components.
Keywords
Introduction
Rhabdomyomatous mesenchymal hamartoma (RMH) is a rare congenital malformation characterized by disorganized proliferation of mature skeletal muscle fibers admixed with other mesenchymal and adnexal elements. 1 It typically presents as a solitary lesion in the midline facial region (e.g., the philtrum, nose, or chin), and is evident from birth/early infancy.2,3
Herein, we present a case involving an infant with a congenital subcutaneous mass in the philtrum initially considered to be a lipoma with an intradermal nevus based on clinical and imaging findings. Histopathological analysis revealed striated muscle hyperplasia with prominent folliculosebaceous components, leading to a diagnosis of RMH. This case is instructive due to the prominence of adnexal features, which required careful histological differentiation from folliculosebaceous cystic hamartoma (FSCH) and other follicular proliferative lesions.
Case Report
The patient was a 20-month-old girl, delivered at 39 weeks 4 days of gestation via normal vaginal delivery (birth weight, 3458 g; length, 51.5 cm). She had a history of infantile eczema, but no other medical conditions. At 4 days old, her mother noted a subcutaneous bulge in the midline of the upper lip (Figure 1A). This lesion had enlarged by the 3-month checkup (Figure 1B), promoting a referral to our dermatology department.
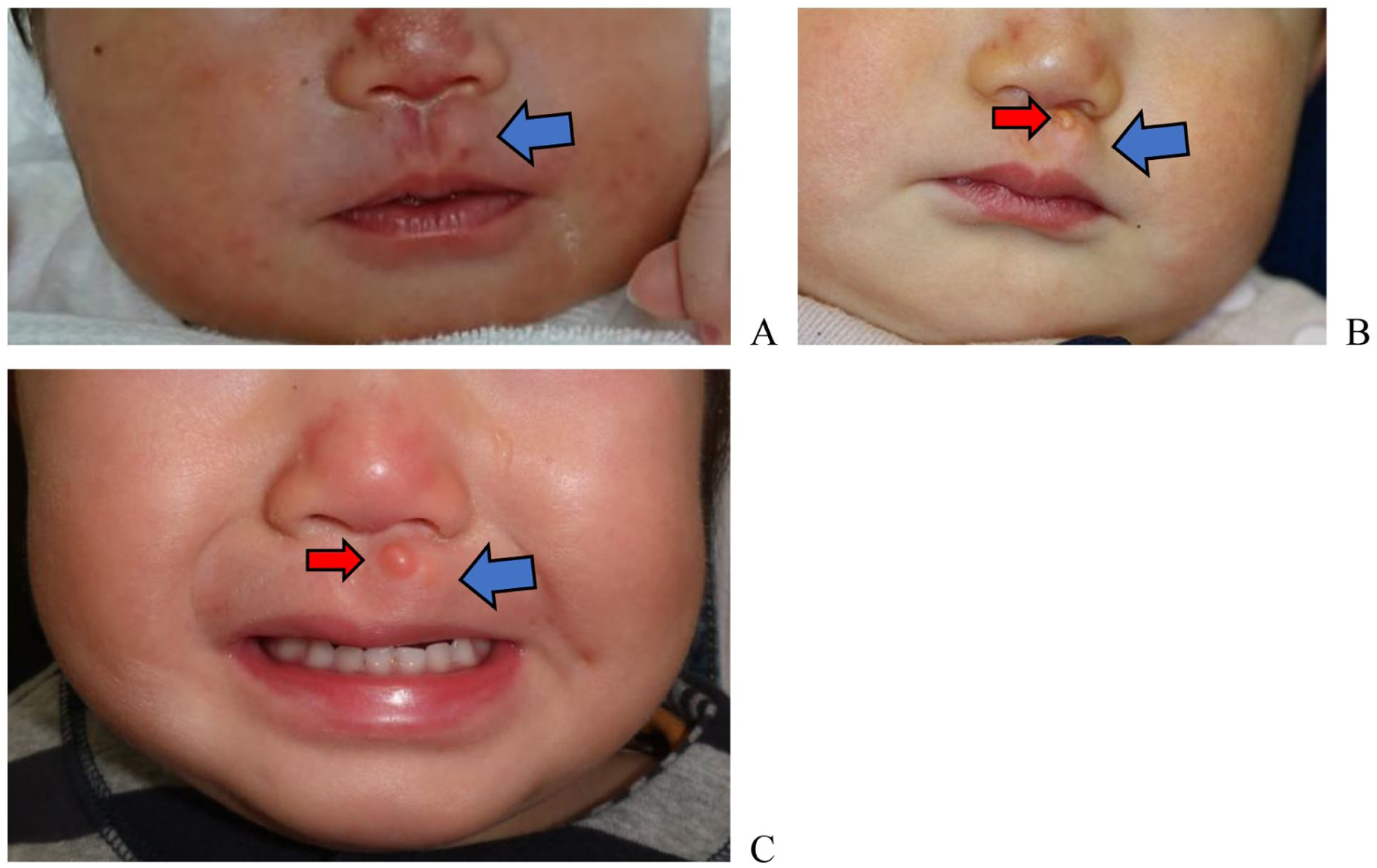
Clinical images from birth to the first dermatology department visit. (A) Image taken at 4 days of age. No evident masses are visible on the skin surface. A slightly bulging subcutaneous mass is visible on the left side of the median ridge (blue arrow). (B) Images from the initial dermatology visit at 3 months of age. A slight mass-like lesion is visible on the skin surface (red arrow). The subcutaneous bulge appears slightly enlarged compared to panel A (blue arrow). (C) Image taken at 20 months of age. The tumor on the skin surface measures 5 mm, and the subcutaneous mass measures approximately 10 mm. The subcutaneous tumor is poorly mobile, elastic, and soft.
Initial ultrasound examination revealed a subcutaneous, highly echogenic mass measuring 9.1 mm × 5.98 mm (Figure 2(A)). At 20 months of age, magnetic resonance imaging showed a lesion with high signal intensity on both T1- and T2-weighted images, which was suppressed on fat-suppression sequences (Figure 2(B)), radiologically suggestive of lipoma. Subsequently, the patient was referred to our plastic surgery department for excision.
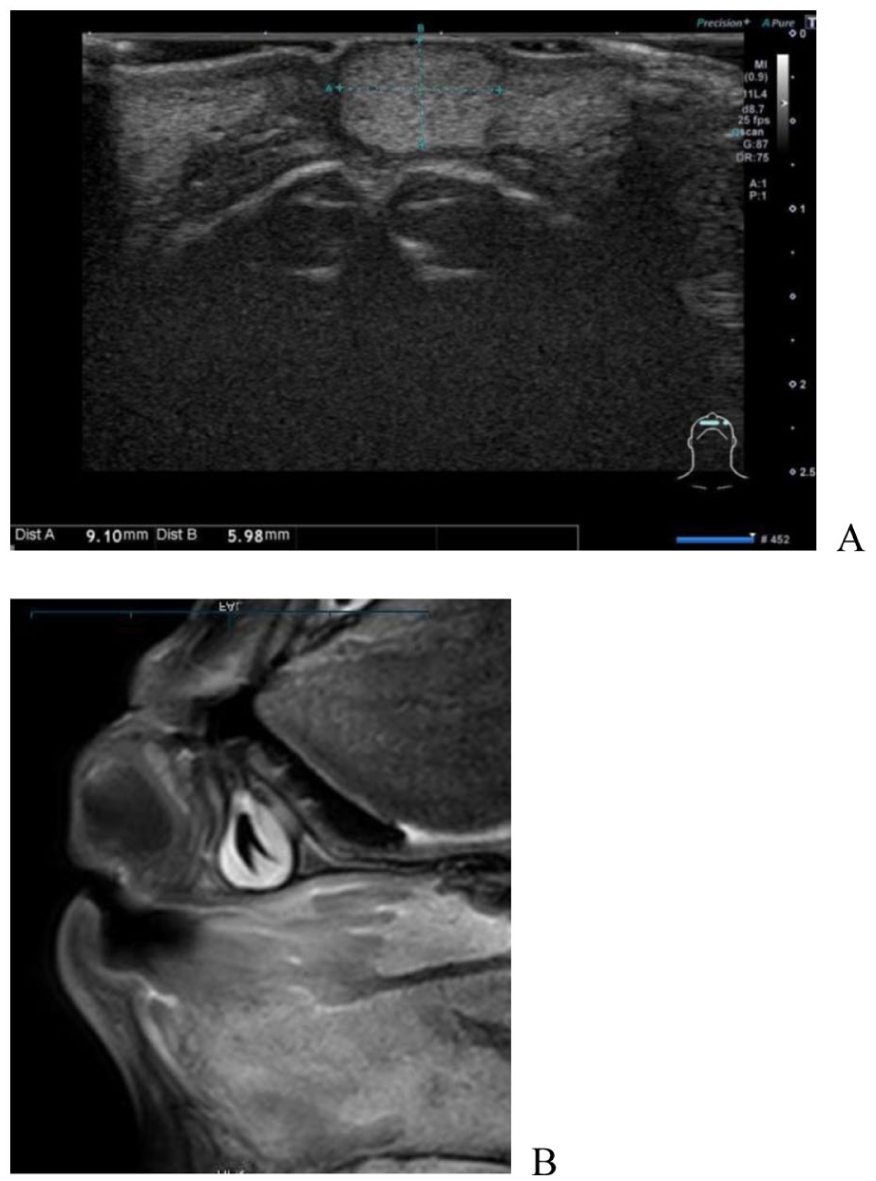
Ultrasound and magnetic resonance imaging findings. (A) Ultrasonographic image showing a 9.1 mm × 5.98 mm echogenic, well-defined, smooth, round subcutaneous tumor in the orbicularis oris muscle. (B) Magnetic resonance imaging scan obtained at age 20 months showing a 12 mm subcutaneous mass with high signal intensity. The signal is suppressed on spectral inversion recovery sequence, consistent with fat content.
On physical examination, a 5 mm skin-colored papule was observed on the left side of the median ridge of the philtrum. A subcutaneous mass, approximately 10 mm in diameter, was palpable beneath the papule. The mass was elastic and soft, with limited mobility. The patient underwent surgical excision under general anesthesia. Intraoperatively, a thin capsule of fat-like tissue was observed beneath the dermis, and a portion of the underlying orbicularis oris muscle was identified and excised with the lesion (Figure 3).

Gross specimen findings. The extracted specimen consists of fat-like tissue (approximately 10 mm) covered with a thin, continuous layer of skin.
Histopathological examination revealed a well-circumscribed lesion. The upper dermis contained sebaceous glands centered around hair follicles. The middle to lower regions contained mature adipocytes and bundles of mature skeletal muscle fibers interspersed among the tissue components. Marked adipocyte proliferation was observed, particularly in the deeper region (Figure 4(A)).
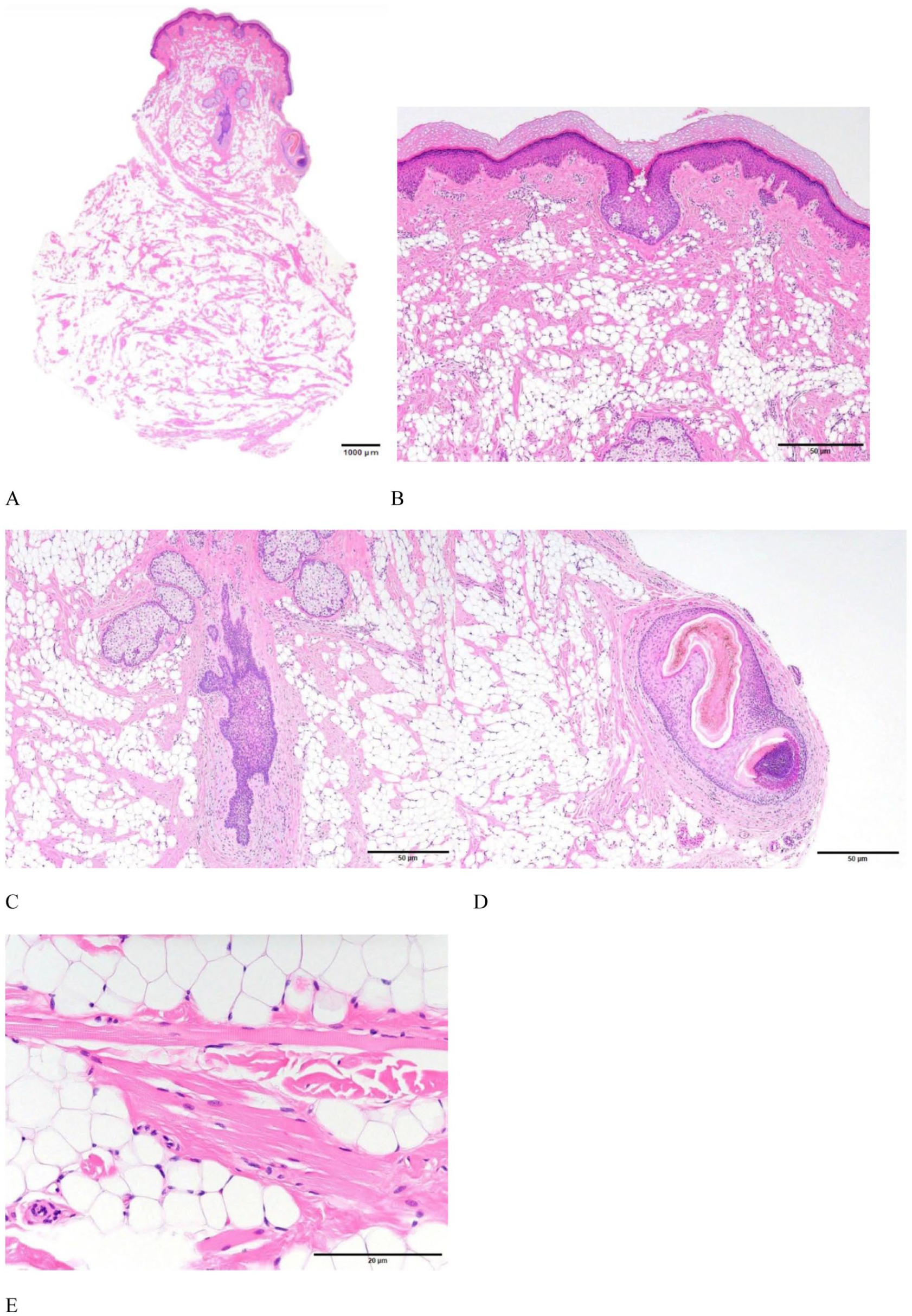
Histopathological findings (hematoxylin and eosin stain). (A) Low-power overview of the lesion, showing an admixture of skeletal muscle, adipose tissue, collagen bundles, and aberrant folliculosebaceous structures. Scale bar: 1000 μm. (B) Isolated adipocytes and small adipocytic clusters in the superficial dermis resemble nevus lipomatosus superficialis. Scale bar: 50 μm. (C) Dilated follicular structures are present, and aberrant follicles and sebaceous glands appear to proliferate continuously from a central follicle. Scale bar: 50 μm. (D) Large aberrant follicles are observed. Scale bar: 50 μm. (E) Mature adipocytes are interspersed among rhabdomyocytes and collagen bundles. Scale bar: 20 μm.
High magnification confirmed mature sebaceous glands proliferating throughout the central hair follicles, with mature adipocytes scattered throughout the dermis (Figure 4(B)). The hair follicles and sebaceous glands were hyperplastic and contiguous with the central hair follicles, forming enlarged, aberrant follicular structures (Figure 4(C) and (D)). In the deepest portions, adipocytes were interspersed among mature striated muscle fibers (rhabdomyocytes) and collagen bundles (Figure 4(E)).
The diagnosis of RMH was established based on the histopathological findings, particularly the presence of mature striated muscle fibers in a congenital midline facial lesion with admixed adipose tissue and adnexal structures. The patient was followed for 5 years postoperatively, with no recurrence.
Discussion
RMH, a rare benign congenital lesion first described by Hendrick et al in 1986,¹ is characterized by a heterogeneous composition of mature skeletal muscle fibers admixed with mesenchymal components and adnexal structures. RMH typically occurs in the midline facial region, presenting at birth or early infancy.2,3 Histopathologically, RMH demonstrates heterogeneous composition with tissue types derived from both the mesoderm and ectoderm. 4
The prominent folliculosebaceous hyperplasia in our case initially suggested FSCH. 5 However, several key features distinguished our case from FSCH: (i) the congenital presentation in an infant, contrasting with the typical onset of FSCH in adults aged >30 years 6 ; (ii) the characteristic midline facial location of RMH; (iii) the absence of cleft-like epidermal invaginations and cystic follicular structures pathognomonic for FSCH,6,7 and (iv) the presence of mature striated muscle fibers, which is a defining feature of RMH but not of FSCH. Follicular induction and adnexal proliferation are not uncommon in hamartomatous lesions and represent the characteristic heterogeneous composition of RMH. Other considered diagnoses, such as nevus lipomatosus cutaneous superficialis and intramuscular lipoma, were excluded because of a lack of either the muscular component, midline specificity, or the complex tissue admixture observed in RMH.
The pathogenesis of RMH is considered to involve aberrant embryological development. 8 Its midline location suggests a disruption during fusion of embryonic facial processes, leading to the proliferation of both mesodermal (striated muscle and adipose tissue) and ectodermal (hair follicles and sebaceous glands) derivatives. 9 Dysregulation of key developmental signaling pathways, such as the Wnt, Sonic Hedgehog, and BMP pathways,8-13 may contribute to RMH formation with prominent adnexal components.
Preoperative diagnosis of RMH is challenging, with imaging frequently indicative of a lipoma. Complete surgical excision is the treatment of choice, with excellent prognosis and no reported malignant transformation or recurrence.2-4
We report a case of RMH in the philtrum of an infant, characterized histopathologically by mature striated muscle fibers admixed with adipose tissue and prominent folliculosebaceous structures. Although the adnexal components suggested FSCH, the presence of striated muscle hyperplasia, congenital onset, midline location, and the absence of characteristic cleft formation confirmed RMH. This case underscores the importance of considering RMH in the differential diagnosis of congenital midline facial lesions and illustrates the histopathological heterogeneity of this rare entity. While this single case report limits generalizability, it contributes to recognizing RMH’s variable presentation.
Footnotes
Acknowledgements
The authors thank the patient’s family for their cooperation and consent to publish this case report, the technical staff of the Department of Pathology for histopathological preparation, the medical photography unit for image documentation, and Claude (Anthropic) and Editage for editorial assistance.
Authors’ Note
Mikiko Inada is now affiliated with Department of Dermatology, Numazu City Hospital, Shizuoka, Japan.
Ethical Considerations
This case report was conducted in accordance with the Declaration of Helsinki and the ethical standards of our institution. As this is a single case report describing routine clinical care, formal ethics committee approval was not required according to our institutional guidelines. All procedures were performed as part of standard medical care.
Consent to Participate
Written informed consent was obtained from the patient’s parents for participation and publication, including clinical photographs, histopathological images, and clinical information, while maintaining patient anonymity.
Consent for Publication
Written informed consent for publication was obtained from the patient’s parents. This consent includes permission to publish clinical photographs, histopathological images, and all relevant clinical information while maintaining patient anonymity. The parents understand that the information will be published without the patient’s name attached, but complete anonymity cannot be guaranteed.
Author Contributions
Mikiko Inada: Designed and conceived the case report, collected data, and drafted the manuscript; Masaru Morita: Provided valuable advice and assisted with the surgery. Miki Izumi: Supervised and advised on histopathological findings. All authors have read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated during this study are included in this published article. No additional data will be made available in accordance with patient privacy protection.