
Abstract
Background:
Hypospadias is a congenital anomaly characterized by ectopic placement of the urethral meatus on the ventral surface of the penis. Surgical manipulation of the urethral plate during urethroplasty induces tissue injury and wound-healing responses that may lead to fibrosis and altered tissue remodeling. However, histopathological differences of the urethral plate between distal and proximal hypospadias remain incompletely characterized.
Methods:
This retrospective analytical study included pediatric patients with hypospadias who underwent primary surgical repair between 2013 and 2023. Urethral plate specimens excised from the dartos fascia to the tunica albuginea were collected intraoperatively and examined histopathologically. Hematoxylin-eosin and Masson trichrome staining were used to assess fibrosis severity, collagen density, and inflammatory cell infiltration. Associations between histopathological parameters and hypospadias type were analyzed statistically.
Results:
A total of 96 patients met the inclusion and exclusion criteria and were included in the analysis. Fibrosis severity was significantly associated with hypospadias type (P = .028), with distal hypospadias demonstrating a higher risk of moderate to severe fibrosis compared with proximal hypospadias (risk ratio, 2.56; 95% CI, 1.098-5.97). In contrast, no significant differences were observed between distal and proximal hypospadias with respect to collagen density or inflammatory cell infiltration.
Conclusions:
Fibrosis severity of the urethral plate differs significantly between distal and proximal hypospadias, indicating that fibrotic remodeling represents a distinct histopathological feature associated with hypospadias severity. Collagen density and inflammatory cell presence did not differ significantly between groups. These findings may have implications for surgical planning and tissue handling in hypospadias repair.
Introduction
Hypospadias is a common congenital anomaly of the male external genitalia characterized by ectopic placement of the urethral meatus on the ventral surface of the penis rather than at the glans tip. It represents the second most frequent congenital anomaly in males and the most prevalent congenital abnormality affecting the penis. 1 The reported prevalence of hypospadias varies considerably across geographic regions, ranging from approximately 2.0 to 43.2 cases per 10 000 live births, with several epidemiological studies suggesting a gradual increase in incidence over recent decades. 2 This variation has been attributed to differences in genetic susceptibility, environmental exposures, and reporting practices. In Indonesia, a multicenter study conducted across 12 pediatric urology referral hospitals documented 591 cases of hypospadias in 2017, reflecting a substantial national disease burden. 3 Similarly, institutional data from RSUP Prof. Dr. I.G.N.G. Ngoerah Denpasar reported 83 cases during the same year, emphasizing the consistent prevalence of this condition at tertiary referral centers. 4
Beyond its anatomical abnormality, hypospadias is associated with significant functional, cosmetic, and psychosocial consequences. Affected children may experience urinary dysfunction, abnormal penile appearance, and long-term psychological distress, particularly during adolescence and adulthood. 5 These considerations underscore the importance of timely and appropriate surgical management. Surgical repair of hypospadias remains technically demanding, with multiple operative strategies described in the literature, including single-stage and 2-stage urethroplasty techniques. 6 The selection of surgical approach is influenced by several factors, including the severity of hypospadias, degree of penile curvature, urethral plate quality, and surgeon experience.
Despite advances in surgical techniques, hypospadias repair continues to be associated with a substantial risk of postoperative complications. Common complications include urethrocutaneous fistula, meatal stenosis, residual chordee, unsatisfactory cosmetic outcomes, weak urinary stream, and trapped penis.6,7 Reported complication rates for proximal hypospadias repair range from 6% to 30%, depending on defect severity, surgical technique, and operator expertise. 8 These complications frequently necessitate secondary procedures and may adversely affect long-term urinary and sexual function, reinforcing the need for improved understanding of factors influencing surgical outcomes.
From a pathological perspective, tissue response following urethroplasty plays a critical role in postoperative healing and complication risk. Surgical manipulation of the urethral plate inevitably induces cellular injury, triggering an inflammatory response that initiates wound healing. While this response is essential for tissue regeneration, excessive or dysregulated healing may lead to fibrosis. Fibrosis develops through complex biological mechanisms involving activation and proliferation of myofibroblasts, excessive deposition of extracellular matrix (ECM) components, and progressive tissue stiffening. 9 This pathological process replaces normal tissue with dense scar tissue, compromising elasticity and functional integrity.
Collagen remodeling is a central feature of fibrotic processes. Physiological wound healing is characterized by a dynamic balance between collagen synthesis and degradation, with early deposition of type III collagen followed by gradual replacement with type I collagen. In pathological fibrosis, this balance is disrupted, resulting in excessive accumulation of type I collagen and relative deficiency of type III collagen. 10 Such alterations reduce tissue compliance and may predispose to adverse surgical outcomes, including urethral stricture formation and impaired urethral elasticity. Experimental and clinical studies have demonstrated that abnormal collagen deposition and inflammatory responses significantly influence wound healing outcomes in urogenital tissues.11,12
Although numerous studies have evaluated surgical techniques and clinical outcomes in hypospadias repair, limited data are available regarding the histopathological characteristics of the urethral plate itself. In particular, comparative histological analyses between distal and proximal hypospadias remain scarce. Most existing studies focus primarily on clinical endpoints, while the underlying tissue properties that may contribute to differing complication rates receive less attention. Furthermore, the extent to which fibrosis severity, collagen density, and inflammatory cell infiltration differ between hypospadias subtypes has not been clearly established.
Given the critical role of tissue remodeling in postoperative healing, improved understanding of urethral plate histopathology may provide valuable insights for optimizing surgical planning and reducing complication rates. Therefore, the present study aims to compare the histological features of the urethral plate in distal and proximal hypospadias, with particular emphasis on fibrosis severity, collagen density, and inflammatory cell presence. By elucidating these histopathological differences, this study seeks to contribute to a more comprehensive understanding of hypospadias pathology and to support evidence-based refinement of surgical management strategies. 13
Methods
Study Design and Setting
This study employed an analytical retrospective design to evaluate histopathological characteristics of the urethral plate in pediatric patients with hypospadias. Patient recruitment and tissue sampling were conducted at Prof. Dr. I.G.N.G. Ngoerah Hospital Denpasar and Surya Husadha Hospital, both tertiary referral centers providing specialized pediatric urology services. Histopathological processing and evaluation were performed in collaboration with the Department of Anatomical Pathology at Prof. Dr. I.G.N.G. Ngoerah Hospital Denpasar.
All surgical procedures were performed by a single experienced urologist (G.W.K.D.) with subspecialty expertise in pediatric urology. The use of a single surgeon was intended to minimize variability in surgical technique, intraoperative tissue handling, and specimen collection, thereby reducing potential operator-related bias that could influence histological outcomes.
Study Population and Sampling
The study population consisted of pediatric patients diagnosed with hypospadias who underwent surgical repair between January 2013 and December 2023. A total sampling method was applied, whereby all eligible patients within the defined study period were considered for inclusion.
The inclusion criteria are pediatric hypospadias patients undergoing primary surgical repair for the first time who agree to tissue preparation for research. Patients who had undergone previous hypospadias repair or revision surgery were excluded to avoid confounding effects related to prior surgical manipulation and tissue remodeling. Additional exclusion criteria included damaged paraffin blocks, incomplete medical records, active infection, postoperative wound dehiscence, and patients who failed to attend follow-up appointments.
Tissue Collection and Specimen Handling
Urethral plate tissue samples were obtained intraoperatively during hypospadias repair. Specimens were excised from the urethral plate extending from the ventral dartos fascia to the tunica albuginea with a U-shaped incision, ensuring inclusion of both epithelial and stromal components. The illustration of tissue collection form the urethral plate was shown in Figure 1.
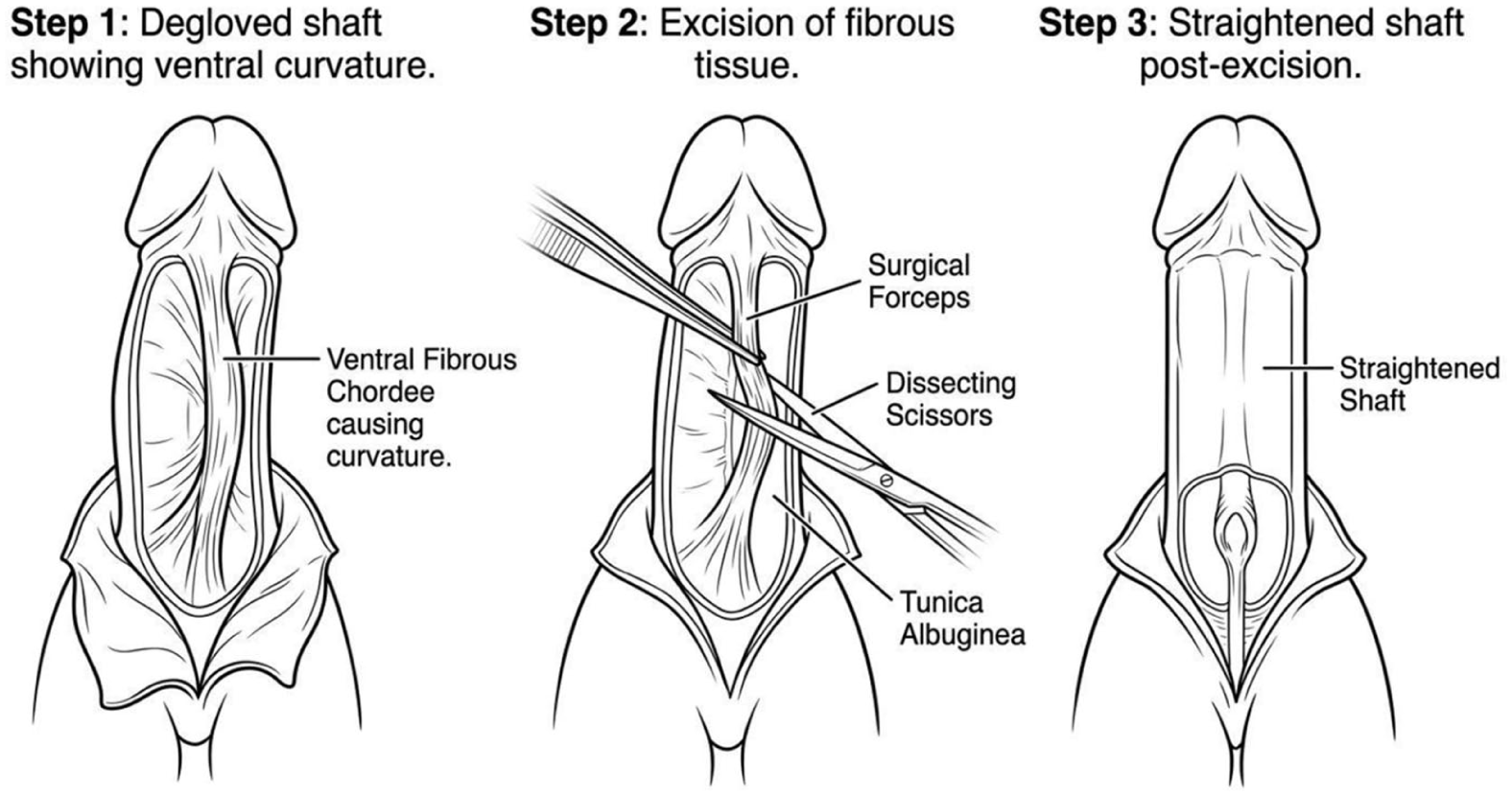
Tissue collection consists of cordectomy and urethral plate excision to straighten the shaft of the penis.
Immediately after excision, tissue samples were fixed in 10% buffered formalin and processed according to standard histopathological protocols. Following fixation, specimens were embedded in paraffin blocks, sectioned at standard thickness, and mounted on glass slides for histological evaluation. All specimens were anonymized prior to analysis to maintain patient confidentiality.
Histopathological Examination
Histopathological evaluation was performed using routine Hematoxylin and Eosin (HE) staining to assess general tissue architecture, cellularity, and inflammatory cell infiltration. Masson Trichrome (MT) staining was used to evaluate collagen deposition and fibrosis within the urethral plate tissue.
Collagen density was assessed semi-quantitatively based on MT staining intensity and distribution and categorized as low collagen density (MT 1− and MT 1+) or high collagen density (MT 2+ and MT 3+), as previously described. 11 Fibrosis severity was evaluated according to the proportion of fibrotic tissue relative to the total tissue area and classified as mild (≤10% of tissue area) or moderate to severe (>10% of tissue area). Inflammatory response was assessed by quantifying lymphocytic infiltration within the stromal compartment and categorized as absent or minimal (≤10 lymphocytes per high-power field) or present (>10 lymphocytes per high-power field), following established histopathological criteria. 12
All histological assessments were performed by qualified pathologists who were blinded to the clinical classification of hypospadias to minimize observer bias.
Outcome Measures
Penile curvature differed between groups based on a goniometer intraoperatively before performing urethroplasty. It was classified into 3 groups: mild (<30°), moderate (30°-60°), and severe (>60°).
The primary outcome measures of this study were fibrosis severity, collagen density, and presence of inflammatory cell infiltration within the urethral plate tissue. These histopathological parameters were compared between distal and proximal hypospadias to identify potential differences related to disease severity.
Statistical Analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS) software, version 25.0. Descriptive statistics were used to summarize patient characteristics and histopathological findings. Categorical variables were presented as frequencies and percentages.
Comparative proportion analyses were conducted to evaluate the association between hypospadias type (distal vs proximal) and histopathological parameters, including fibrosis severity, collagen density, and inflammatory cell presence. Cross-tabulation tables were generated for each comparison. The strength of association was expressed using risk ratios (RRs) with corresponding 95% confidence intervals (CIs). Statistical significance was assessed using the Chi-square test, with a 2-tailed P-value of <.05 considered statistically significant.
Ethical Considerations
This study was conducted in accordance with the principles of the Declaration of Helsinki. Ethical approval was obtained from the relevant institutional ethics committee before data collection. It allows for the retrospective nature of the study and the use of archived tissue specimens without interference with the surgical correction. All patient data were anonymized to ensure confidentiality.
Results
Study Population and Clinical Characteristics
A total of 102 pediatric patients with hypospadias underwent surgical repair between January 2013 and December 2023. Of these, 96 patients fulfilled the inclusion and exclusion criteria and were included in the final analysis. The study population consisted of 51 patients (53.1%) with distal hypospadias and 45 patients (46.9%) with proximal hypospadias.
The median age at the time of surgery was lower in the distal hypospadias group compared with the proximal hypospadias group (4 years [IQR = 3] vs 6 years [IQR = 5.5], respectively). Regarding surgical technique, all patients with distal hypospadias underwent single-stage repair, including tubularized incised plate (TIP) urethroplasty (n = 34) and inner preputial skin graft urethroplasty (n = 17). In contrast, all patients with proximal hypospadias underwent staged repair, which consisted of cordectomy, urethral plate excision, and Byars flap for the first stage and Thiersch Duplay for the second stage (n = 45).
Patients with distal hypospadias predominantly exhibited mild to moderate curvature, with severe curvature observed in only 2 cases. The proximal hypospadias group was dominated by moderate curvature, without a case of severe curvature. Baseline demographic and clinical characteristics are summarized in Table 1.
Characteristic of Study Population.
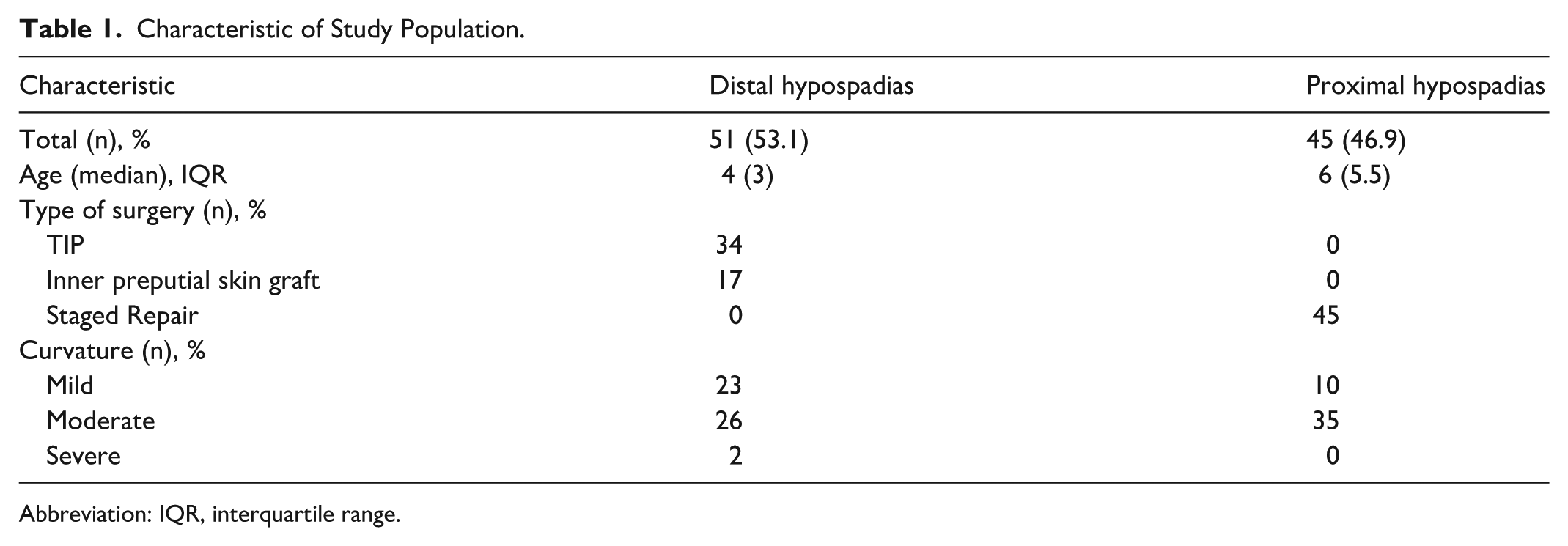
Abbreviation: IQR, interquartile range.
Histopathological Findings of the Urethral Plate
Histopathological evaluation of urethral plate specimens was performed using Hematoxylin and Eosin and Masson Trichrome staining. The assessed parameters included collagen density, fibrosis severity, and inflammatory cell infiltration. The distribution of these histopathological features according to hypospadias type is presented in Table 2.
The Analysis of Histopathological Examination and Type of Hypospadias.
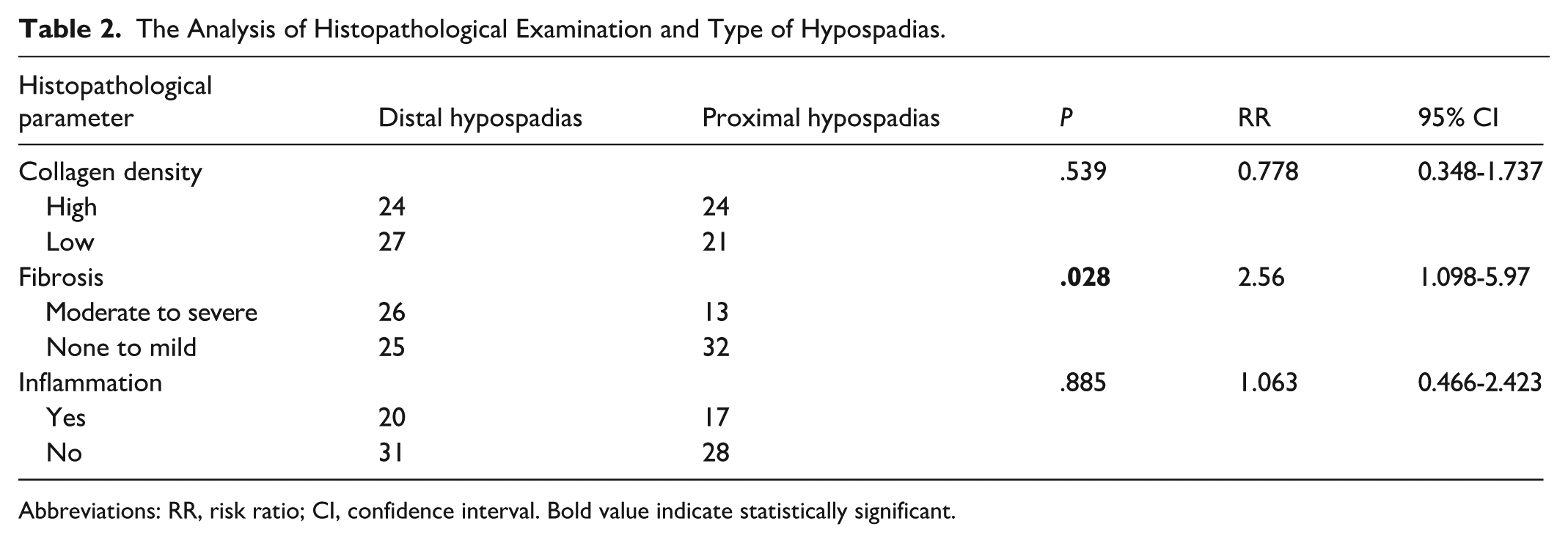
Abbreviations: RR, risk ratio; CI, confidence interval. Bold value indicate statistically significant.
Association Between Hypospadias Type and Collagen Density
Collagen density did not differ significantly between distal and proximal hypospadias. High collagen density was observed in 24 patients with distal hypospadias and 24 patients with proximal hypospadias, while low collagen density was identified in 27 and 21 patients, respectively. Statistical analysis demonstrated no significant association between hypospadias type and collagen density (P = .539). The risk ratio for high collagen density in distal compared with proximal hypospadias was 0.778 (95% CI, 0.348-1.737).
Association Between Hypospadias Type and Fibrosis Severity
A statistically significant association was identified between hypospadias type and fibrosis severity. Moderate to severe fibrosis was observed in 26 patients with distal hypospadias and 13 patients with proximal hypospadias, whereas none to mild fibrosis was identified in 25 and 32 patients, respectively. Distal hypospadias was associated with a significantly higher risk of moderate to severe fibrosis compared with proximal hypospadias (P = .028), with a risk ratio of 2.56 (95% CI, 1.098-5.97).
Association Between Hypospadias Type and Inflammatory Cell Infiltration
No significant association was observed between hypospadias type and inflammatory cell infiltration. Inflammatory cell presence was identified in 20 patients with distal hypospadias and 17 patients with proximal hypospadias, while absence of inflammation was observed in 31 and 28 patients, respectively. The difference between groups was not statistically significant (P = .885). The risk ratio for inflammatory cell presence in distal compared with proximal hypospadias was 1.063 (95% CI, 0.466-2.423).
Summary of Results
Overall, fibrosis severity of the urethral plate differed significantly between distal and proximal hypospadias, with distal hypospadias demonstrating a higher risk of moderate to severe fibrosis. In contrast, collagen density and inflammatory cell infiltration did not show significant differences between hypospadias subtypes.
Discussion
Hypospadias is a congenital anomaly of the male external genitalia resulting from abnormal development of the urethral folds and ventral foreskin, leading to ectopic positioning of the urethral meatus. In the present study, the median age of patients undergoing hypospadias repair was 5 years. This finding is consistent with a multicenter study conducted in 12 pediatric urology referral centers in Indonesia, which reported that the majority of patients underwent surgery after the age of 4 years. 3 In contrast, studies from high-income countries, such as the United Kingdom, have reported earlier surgical intervention, with a mean age of approximately 2.5 years. 13 These differences likely reflect variations in healthcare access, referral systems, and sociocultural factors influencing the timing of surgical management.
The principal finding of this study was the presence of a significant difference in fibrosis severity of the urethral plate between distal and proximal hypospadias. In contrast, no significant differences were observed with respect to collagen density or inflammatory cell infiltration. These findings suggest that fibrosis represents a distinct histopathological characteristic that may differ according to hypospadias severity, independent of overall collagen quantity or inflammatory burden.
Previous clinical studies have primarily focused on surgical outcomes rather than underlying tissue characteristics. Hoy et al 14 reported no significant difference in median stricture length between single-stage and 2-stage urethroplasty, concluding that staged repair may reduce the need for subsequent procedures while maintaining comparable success rates. Similarly, Zhu et al 15 demonstrated higher success rates in 2-stage repairs compared with single-stage procedures, although stricture formation was not observed in either group. While these studies provide valuable clinical insights, they do not directly address histopathological differences within the urethral plate that may contribute to divergent outcomes.
A systematic review by Anggriant et al 16 highlighted that single-stage urethroplasty is attractive due to reduced healthcare costs, shorter hospital stays, lower anesthetic exposure, and faster achievement of functional outcomes. However, 2-stage urethroplasty offers specific advantages, including the creation of a more favorable urethral bed and potential reduction in scar tissue formation. The interval between graft placement and urethral tubularization in staged procedures allows for stabilization of tissue remodeling processes, which may influence fibrosis development. Although surgical technique selection is influenced by multiple clinical factors, the present findings suggest that intrinsic histopathological differences of the urethral plate may also play a role.
From a pathological standpoint, fibrosis is not solely determined by the quantity of collagen present but rather by dysregulated extracellular matrix (ECM) remodeling. Fibrosis arises from an imbalance between collagen synthesis and degradation, accompanied by persistent activation of myofibroblasts and altered ECM composition. 17 Collagen, as the principal ECM component, plays a critical role in maintaining tissue integrity, elasticity, and cellular signaling. Alterations in collagen organization and subtype composition—particularly an increased ratio of type I to type III collagen—can lead to increased tissue stiffness and impaired functional properties. These mechanisms may explain why fibrosis severity differed between hypospadias subtypes in the present study, despite comparable collagen density and inflammatory cell presence.
The study by Sennert et al 18 analyzed the Hematoxylin and Eosin, smooth muscle actin, factor 8, and elastic van Gieson staining. The Hematoxylin and Eosin staining showed that the urethra was lined with pseudostratified epithelium, then became a non-keratinized stratified squamous epithelium in the meatus urethra. However, in the urethral plate distally, it became keratinized epithelium. The smooth muscle actin staining showed a regular circular pattern of muscles in the urethra, which changed into a U-shaped pattern in the meatus urethra. Conversely, in the urethral plate distally, it showed irregular, disorganized smooth muscles. Moreover, the elastic van Gieson staining showed that hypospadias patients have fewer elastic fibres in the urethra than normal skin and subcutaneous tissues.
The absence of a significant association between hypospadias type and inflammatory infiltration suggests that inflammation alone may not be the primary driver of fibrosis in urethral plate tissue. Instead, downstream ECM remodeling processes may exert a more substantial influence on fibrotic progression. This observation aligns with emerging evidence indicating that fibrosis can persist even after resolution of acute inflammation, driven by sustained fibroblast activation and matrix deposition. 17
This study has several important clinical and pathological implications. To our knowledge, this represents one of the first studies to systematically compare histopathological features of the urethral plate between distal and proximal hypospadias. The use of standardized tissue sampling and analysis, combined with surgical procedures performed by a single experienced pediatric urologist, minimized variability related to operative technique and specimen handling. These methodological strengths enhance the reliability of the observed histological differences.
Nevertheless, several limitations should be acknowledged. First, collagen assessment was performed using semi-quantitative methods and did not distinguish between specific collagen subtypes, such as type I and type III collagen. More detailed molecular or immunohistochemical analyses could provide deeper insights into the role of collagen composition in fibrosis development. Second, the retrospective design of the study relies on the accuracy and completeness of medical records, which may introduce information bias. Future prospective studies incorporating quantitative collagen analysis and multi-center participation may further elucidate the pathological mechanisms underlying hypospadias repair outcomes.
Conclusion
This study demonstrates that fibrosis severity of the urethral plate differs significantly between distal and proximal hypospadias, indicating that fibrotic remodeling represents a distinct histopathological feature associated with hypospadias severity. In contrast, collagen density and inflammatory cell presence did not differ significantly between groups, suggesting that fibrosis progression may be driven primarily by dysregulated extracellular matrix remodeling rather than by collagen quantity or inflammatory burden alone.
These findings highlight the importance of considering intrinsic urethral plate tissue characteristics when planning hypospadias repair. Improved understanding of fibrosis-related histopathology may contribute to more informed surgical decision-making and optimization of reconstructive strategies. Further prospective studies incorporating detailed collagen subtype analysis and molecular assessment are warranted to clarify the mechanisms underlying fibrosis development and their impact on surgical outcomes.
Footnotes
Ethical Considerations
This research has received approval from the research ethics committee of the Faculty of Medicine, Universitas Udayana, Prof. I.G.N.G. Ngoerah General Hospital, Denpasar with No. 2488/UN14.2.2.VII.14/LT/2023.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.