
Abstract
As more and more technologies are infused into service delivery, service providers must continuously renegotiate the ways in which they understand service delivery across increasingly high-tech, low-touch modalities. This exploratory qualitative study examines what health care service providers experience when offering separated services in the empirical context of telehealth. In-depth phenomenographic interviews sourced across multiple hospital and health care sites revealed that service providers experience (1) depersonalization, (2) clinical voyeurism, (3) intangibility negotiation, and (4) a need to manage change around identities and roles. These emergent understandings highlight the individual and qualitatively distinct differences in the ways in which service providers experience service separation in telehealth. Our findings address current service science priorities to leverage technology for service delivery as a way to advance separated service design. Further they provide an understanding-based approach toward building new theories from the service provider’s perspective on separation in technology-infused services. Our findings suggest strategies and tactics service providers use to overcome the potential challenges arising from not being physically colocated with their customers during service separation.
With the advent of enhanced technology, many services are evolving to a virtual service delivery platform. Within the context of health care, the adoption of new forms of technology-infused service delivery modes is increasingly prevalent. Pharmacists now respond to medication prescription requests forwarded online and offer customers advice through online chat functions. Medical specialists can now instantaneously videoconference with their patients rather than have them travel hundreds of kilometers for a 10-minute appointment. More recently, surgeons have been utilizing robotic arms to assist with surgical operations in place of the direct use of their own hands on patients. The phenomenon of transitioning from low-tech, high-touch to high-tech, low-touch service delivery has never been more salient (Wunderlich, von Wangenheim and Bitner 2012), as service providers are increasingly confronted with a plethora of service delivery modalities. This begs the question, what is problematic about the advent of enhanced virtualized (technology-infused) service delivery from a service provider’s prospective?
With increased infusion of technology in the way health care services are now delivered, service providers (medical specialists) are ultimately transcending the boundaries of physical and geographical distance between themselves and their customers (patients). Service separation is becoming a phenomenon of increasing conceptual and empirical interest to services scholars, yet to date, the emerging literature on service separation has focused on the customer’s perspective. This is to the detriment of understanding the view and experience of the service provider in delivering separated services.
While we acknowledge that customers are indeed central to the fundamental marketing proposition, the decision to offer a separated service in the first place rests with service providers. If service providers are not willing or equipped to deliver separated services in the first place, then customer demands and perceptions become a secondary concern. For example, service providers may not offer a separated service because they do not feel formally equipped (through training) or personally equipped (through a lack of enthusiasm and/or resilience to change and adaptation to new technologies). We believe that separated service delivery becomes all the more complex and salient when situated within the context of health care. Health care represents a rare service context in which most, if not all, service encounters must include the presence and expertise of the service provider (i.e., doctor, specialist, surgeon, and pharmacist). Hence, technology-infused advancements in fields such as telehealth are reliant upon uptake, acceptance, and usage by the health care service providers.
Service separation has been defined as the “… customer’s absence from service production, denoting the spatial separation between service production and consumption” (Keh and Pang 2010, p. 55). In this study, we add to an understanding of service separation, the notion of temporal distance in terms of a time lag that is inevitably incited by certain technologies. For example, with technology infusion via videoconferencing, there is spatial separation since service providers and customers are not physically colocated. However, the service delivery is synchronous, and production is not entirely separate from consumption in this sense. With the infusion of robotic telepresence, there is spatial separation as the service providers and customers are not physically colocated; however, there is a predictable time lag that renders the service delivery asynchronous. Lastly, with e-mail communication between a service provider and customer, there is not only spatial separation but also temporal separation as the communication is asynchronous and there is an unpredictable time lag. In our view the degree of service separability is inherent to the nature of the technology infused into the service. Thus, we posit that there are differing degrees or intensities of service separation, with spatial separation alone indicating one level of intensity, whereas temporal separation added on top of this serves to separate production from consumption in its purest form.
With the advent of telehealth, health care providers face changing realities to their professional service delivery landscape. The choice to adopt telehealth as a form of virtualized service delivery currently rests with the service provider, who selectively chooses which, if any, patients to treat virtually. Hence, telehealth has received varying levels of adoption across health care settings and specialties. We believe this is an important and interesting time and setting to examine the service providers’ perspective of separated service delivery. Subsequently, our article explores how service providers adapt to the transition to service separation. To our knowledge, service separation is a phenomenon that has not been examined from the service provider’s perspective, let alone in the context of telehealth. This is despite the proliferation of technology infusion in sectors such as education, banking, and retail, not to mention health care.
Our work contributes to two streams of services marketing literature. First, we advance theory as to service provider’s experiences of service separation in the context of telehealth, extending an important stream of emerging literature on service separation (e.g., Keh and Pang 2010; Paluch and Blut 2013). In contrast to prior work, our study is framed from the service provider’s perspective. This is important because if service separation is only understood from the customer’s perspective, then the co-created nature of the service delivery (Vargo and Lusch 2004) is not theoretically addressed. Thus, the service provider’s perspective is fundamental to developing a better theoretical understanding of service separation as a phenomenon of services marketing interest. We present telehealth as a theoretically rich empirical context within which to investigate service providers’ experiences of separated services.
Second, our work contributes to the burgeoning literature focused on the intersection between health care and services marketing (e.g., Berry and Bendapudi 2007; McColl-Kennedy et al. 2012; Sweeney, Danaher, and McColl-Kennedy 2015) by understanding how clinical service providers negotiate the transition to service separation and virtual service delivery. Our study extends Schumann, Wünderlich, and Wangenheim’s (2012) recent theorization of high-tech, high-touch service delivery by identifying the potential difficulties of service separation from the provider’s perspective bounded around high-tech but low-touch health care interactions. We see this as particularly interesting in the current empirical context, given the strong norms around physical examination and hands-on treatment in health care contexts. Moreover, health care is typically characterized by information asymmetries between doctors and their patients that incite relationships of (inter)dependence and vulnerability. These relationships are made all the more complex, and to our minds subverted, for the service provider when virtual.
Our article is organized as follows. First, to ground our work in current services marketing literature, we review current thinking around service separation and technology-infused services with a focus on high-tech service delivery. We then outline our qualitative methodology and the findings from our extensive in-depth interviews conducted with specialist health care providers currently engaged in telehealth provision. We found four qualitative differences or understandings of service separation from the provider’s perspective. We next discuss the managerial and theoretical implications of the research and conclude by highlighting future research avenues arising from our findings.
Literature Development
Technology-Infused Services
A burgeoning conversation has sought to address the phenomenon of technology infusion in service delivery since the early 2000s (e.g., Bitner, Brown, and Meuter 2000; Bitner 2001; Meuter et al. 2000). This early work paved the way for understanding the increasing role of technology-infused service delivery in terms of uptake, customer experience, and satisfaction. More recent research shows that the inseparability assumption from the services marketing paradigm bounded around intangibility, heterogeneity, inseparability, and perishability is flawed (Lovelock and Gummeson 2004; Vargo and Lusch 2004). This argument is based on the premise that most services marketing knowledge arose from a goods-based dominant logic to the neglect of developing an organic theory of services unique to the field in its own right (see Vargo and Lusch 2004). Hence, with the proliferation of high-tech and high-touch phenomena through enhanced adoption of technology in service delivery (Schumann, Wünderlich, and Wangenheim 2012), the need to advance a new paradigm is more salient than ever.
Self-Service Versus Remote Service Technologies
Complementary to this stream of research is a literature focused on customers’ use of self-service technologies (SSTs) in the context of virtual service delivery (e.g., Meuter et al. 2003, 2005). SSTs are a subset within virtual service delivery because with SSTs the customer is at the forefront of the service delivery process. These services are characterised by the reduced role of the service provider, sometimes to the complete removal of a human-based provider and full replacement with a robot or technology, such as with automatic teller machines. This is in contrast to remote service provision, which is how telehealth can be characterized, where the “humanity” of the service provider remains paramount and their decisions and interactions with a customer occur virtually. Paluch and Blut (2013) elaborate on this notion by contrasting self-services where the customer produces the service “… remote services are defined as technology-infused services that exclusively allow the service provider to access and modify connected service objects over long distances” (p. 415). In telehealth, where the service object is the patient, illustrative examples involve using robotic telepresence surgery, the use of video-based teleconferencing to treat patients at a virtual arm’s length, and the use of e-mail store-and-forward to diagnose patients virtually without physically examining them based on still images. It is these spatially and/or temporally remote, high-tech services that are the focus of this research.
Defining High-Tech Delivered Services
Schumann and colleagues (2012) define high-tech services as being “… services provided by a technological interface between a provider and customer, which allows for an immediate exchange of information over long distances” (p. 133). To date, most research has focused on understanding the consumer’s experience, particularly regarding customer trial of SSTs (e.g., Meuter et al. 2000, 2003, 2005). The understanding of services within a “low-tech, high-touch” paradigm (Bitner, Brown, and Meuter 2000) has become gradually repositioned as a “high-tech, low-touch” paradigm. As a result, two predominant shifts in services marketing thought have occurred. The first encapsulates technology’s impact on virtual interactions between providers and customers. Technology-infused service interactions such as those seen in telehealth incite a high-tech, yet low-touch paradigm, whereby direct hands-on contact between practitioners and their customers is compromised or completely removed. The second shift refers to instances where service providers are replaced by technology altogether (Bitner, Brown, and Meuter 2000). This occurs with the use of machines to replace individuals and where the role of the service provider is relegated to the background and the customer has relative control over the (self) delivered technology-infused service experience.
Service Separation
Reflecting a long-held adherence to the idea of service inseparability, Berry and Bendapudi made the following observation: Because health care services are provided for people, rather than for people’s property, they typically are inseparable. Patients must be physically present where the service is rendered (such as a doctor’s office or hospital) when the doctor or nurse is available to deliver the service. (2007, p. 113)
Keh and Pang (2010) have shown that technology-infused service delivery is perceived by customers as risky and that customers react differently to service separation based on whether the service is credence based or experience based. Moreover, customers can exhibit differing levels of satisfaction with a service based on their level of involvement in the virtual encounter (Paluch and Blut 2013). To date, most of the emerging literature on service separation in the services marketing literature, and indeed on technology-infused service delivery, has been constructed from the customer’s perspective. In contrast, research from the service provider’s perspective is scarce. While the customer’s perspective on technology acceptance and usage is vital to the success of virtual service delivery (Wünderlich et al. 2012), the service providers perspective is also important. Accepting Vargo and Lusch’s (2004) proposition of co-created service delivery, by definition service delivery is a joint collaboration which needs to focus on both sides of the equation—customers and providers. In short, services cannot be delivered without a service provider.
Although significant advances in our understanding of technology-infused service delivery have been made across a multitude of service contexts, to our knowledge, no context as rich as health care has been studied to date. As Berry and Bendapudi (2007) highlight, health care is indeed a fertile field for research; yet, we have barely scratched the surface in understanding the virtual service possibilities that service separation can now afford health care. Berry and Bendapudi (2007) state as one of their health care research priorities that there is much service research can offer health care in terms of better understanding the experiences of service providers due to the physical and emotional stresses which belie health care service provision. To understand how this is made manifest when the service provision is virtually separated, as in our study, adds even finer nuances.
The services marketing literature has been slow to understand the various aspects of telehealth and the specific implications for service providers. However, the practitioner literature has been more responsive. For example, recent research in medicine has qualitatively examined frontline service worker’s (i.e., matrons, nurses) experiences of telehealth (e.g., Macneill et al. 2014). Others have specifically focused on the experiences of peripheral service workers who complement the telehealth service delivery for the specialist (e.g., Purc-Stephenson et al. 2010). Others have looked at specific contexts of care to which telehealth seems to be particularly conducive, such as chronic disease management spanning diabetes (e.g., Tudiver et al. 2007) and mental health management such as depression (Montero-Marin et al. 2013) and moreover from the perspective of mental health professionals (Gibson et al. 2011). Further work by Wade, Eliott, and Hiller (2014) found that “… clinician acceptance is the key factor or most important influence on the successful operation of telehealth services” (p. 686). This makes for an important and complex service context which we believe warrants more systematic, in-depth exploration from the service providers’ perspective so as to learn from those who have chosen to uptake telehealth as a form of separated service delivery.
A 2013 article by Forbes suggested that the top health trend for 2014 was that telehealth would grow by over 50% in the United States, with a report by RNCOS Business Consultancy suggesting 18.5% worldwide telehealth growth through to 2018 (Graham 2013). Within Australia (the location of this research), fundamental concerns arise from the geographic vastness of the country coupled with the disproportionate location of specialists in coastal cities and the diseconomies of scale in funding specialists to be posted rurally to provide equitable care to rural and remote patients. This highlights the relevance of understanding the experiences of those who are using telehealth technologies and have separated health care service production (i.e., clinical consultations, the offering of medical advice, provision of a treatment plan, administration of medical prescriptions, onward referrals for further investigation) from health care service consumption (i.e., the receipt of the abovementioned service provider processes by patients). This research focuses on the experiences of service providers offering traditional hands-on medical services at a virtual distance through technology-infused service delivery. As such, the purpose of this study is to investigate how service providers experience service separation through technology infusion in the context of telehealth.
Method
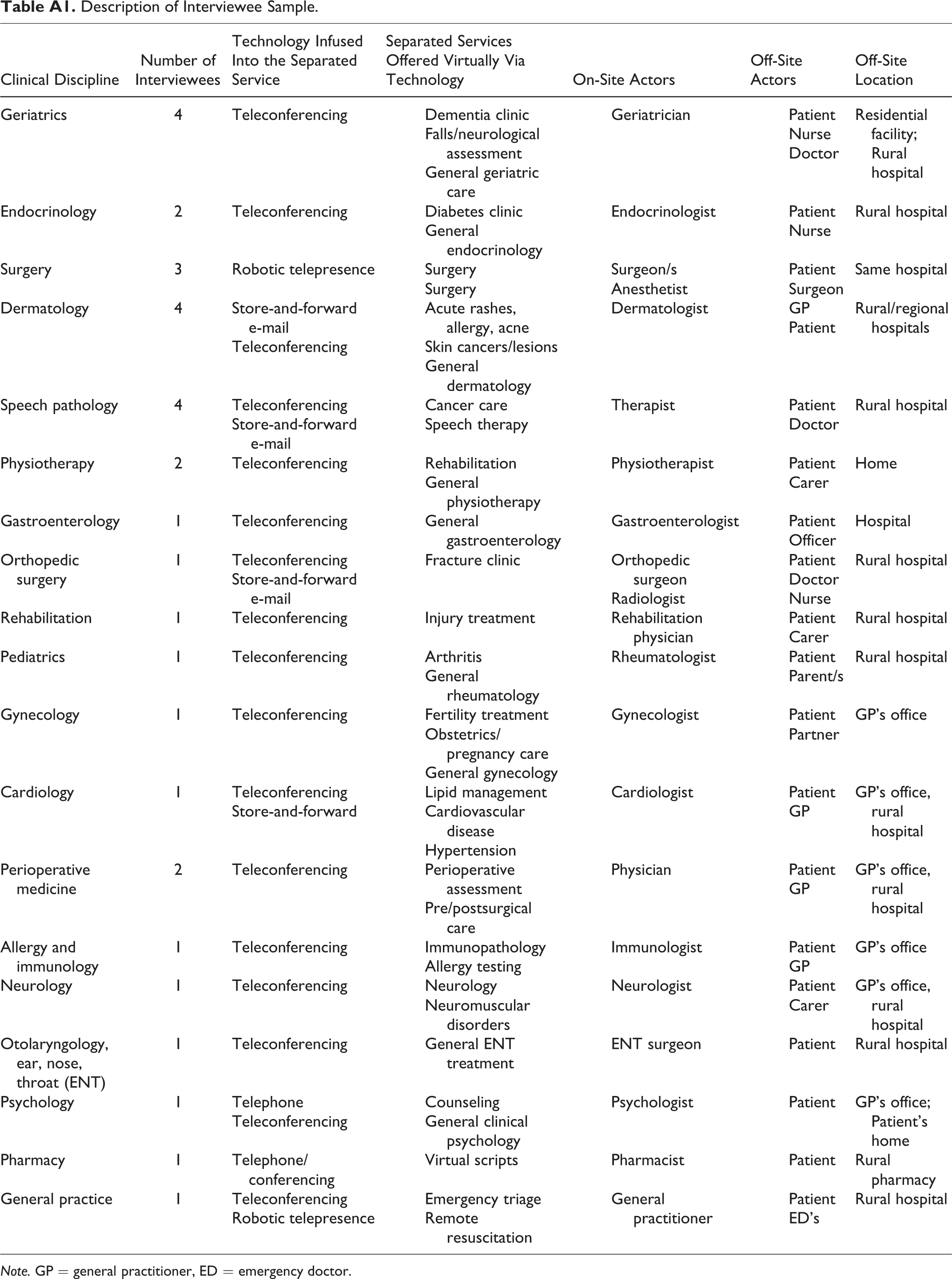
Our investigation of telehealth and health care providers’ experiences of service separation represents approximately 12 months of field work. Telehealth providers were defined as medical practitioners and specialists who had adopted telehealth. Data collection for this article comprised in-depth interviews with 33 telehealth specialists and medical practitioners drawn from both public and private practice across 19 different fields of telemedicine (see Appendix). The qualitative interpretive technique of phenomenology was adopted, whereby the objective was to capture the lived experiences of participants’ lifeworld as it related to the given phenomenon of research interest (Sandberg 2000). In this context, lived experiences refers to the reality of the everyday “quotidian,” such that the researcher uses very few questions to elucidate rich descriptions from research participants regarding their conception of their world view. The task of the researcher then becomes to document the experiences of the interviewee and to look within and across interview cases to understand whether an individual’s experiences are isolated cases (i.e., the elusive black swan) or more indicative of some broader theoretical phenomenon of interest. Phenomenography is a technique derived from educational researchers in Sweden around the 1970s; however, the technique has gained traction as a useful qualitative approach to gain an interviewee-oriented perspective on the research phenomenon of interest. The educational approach or “learner-centered” perspective inherent to phenomenography (Sandberg 1997) is particularly useful in this study, as service providers are viewed as having to learn how to adapt to the external changes in their operating environment (i.e., technology infusion). Technology infusion in the form of telehealth is not taught to them by others but rather something that organically emerges through interactions with technology and patients virtually over time and across an array of platforms.
To access a sufficient number of telehealth providers, a snowball sampling technique was used. Individuals were sought who practiced across a variety of medical fields. Other criteria used to inform the sampling process included seeking to maximize “naturally” occuring variance in terms of the following: gender, age, level of experience (ranging from registrar to full professor), level of telehealth experience (ranging from new user to experienced user), length of time using telehealth (ranging from 12 months to over 10 years), type of clinical specialty (adult and paediatric care), and type of technology used. Undergraduate medical students were not recruited.
Data Analysis
The in-depth interviews generally lasted around 45 minutes each. The interview data were first examined as source material in meticulous detail in an iterative process that evolved during and after data collection. This iterative process was employed to identify the underlying themes within the data and reflected Lincoln and Guba’s (1985) constant comparative method, an approach which has been similarly used in health care service contexts for qualitative data sets (e.g., McColl-Kennedy et al. 2012; Sweeney, Danaher, and McColl-Kennedy 2015). As our data set grew (and grew), this process involved moving back and forth between the field, collecting more data, reflecting on the data, and subsequently returning to the field for more data over the period of a year. In the initial phase of the research, all of the interview data were manually coded by hand by the first author to get an initial sense of what was “in” the data in terms of interest and also in relation to the overarching research question. A second intensive phase was performed involving monthly meetings with the three-person research team from which a revised set of codes and a set of understandings began to emerge from the data. At around 11 interviews, saturation and repetition of themes began to emerge and the research team concurred with the co-created codifications of the interview data. Grounded theory as advocated by Strauss and Corbin (1990) informed the initial coding work, using open coding, structural coding, and axial coding.
Results
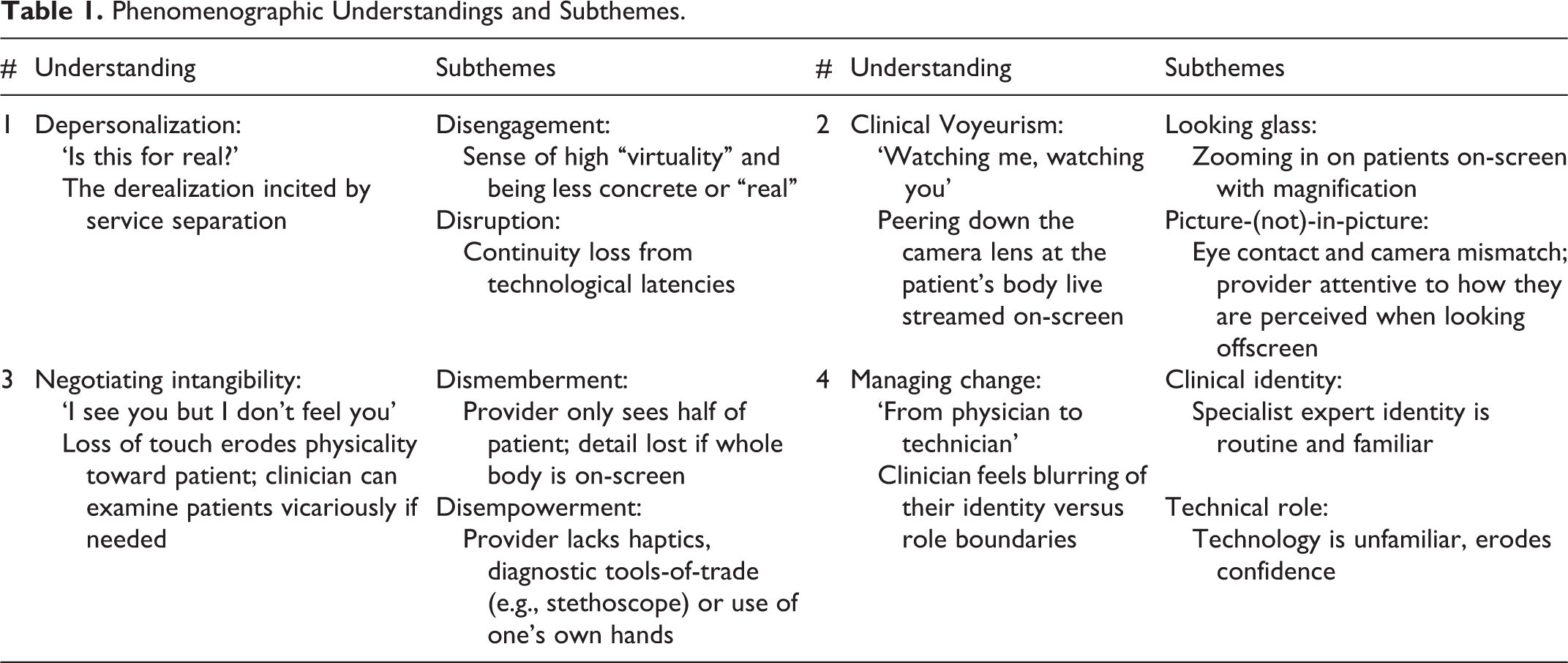
Given our aim of exploring service provider’s experiences of service separation, our focus was on phenomenographic conceptions, that is, health care providers’ understandings of their lived experiences of telehealth. Table 1 summarizes the four main understandings that emerged as conceptually distinct from the phenomenographic interview analysis.
Phenomenographic Understandings and Subthemes.
Health Care Provider Understandings of Service Separation Through Telehealth
Understanding 1: Depersonalization
The first emergent understanding was the notion of depersonalization. Depersonalization refers to the service provider’s perception of the unreal, digital-based nature of technology infusion in telehealth. This can lead to a sense of telehealth being like a kind of virtual reality. The loss of physical touch that comes from interacting at a virtual arm’s length is a feature of telehealth that depersonalizes the experience for health care providers. Often providers reported that touch is a very “human” thing to do, which personalizes the consult and their perception that they are psychologically “there” with the patient. While we acknowledge that virtual interactions can still be personal, we argue that there is an element of depersonalization due to the lack of direct touch and face-to-face contact. For example, as one interviewee stated, … I think that is crucial {i.e., touch}, also in many practices as a doctor I see that if you touch a patient or if you shake their hand it puts a different level on it, but over telemedicine it is going to be a bit harder to do. (i30M) … all they must do is just put one finger on a person’s knee and say ‘Hey, you will be alright.’ That is just such a reassurance; it just turns a patient’s whole day around. It is that sort of intimacy, and often patients say ‘Oh thank you so much, I feel so much better’… with all those things I can see an immediate response from the patient … because people are people and they want interaction … (i5M)
Subtheme 1: Disengagement
This occurs in the sense that it makes the provider’s lived experience more “virtual” and less concrete or “real,” which can lead to potentially negative consequences. For example, in the context of robotic surgery, as a spatially and temporally separated form of telehealth, one provider expressed:
I worry that you might take risks that you might not necessarily take if you were just that little bit closer to the reality of the fact that this is living flesh attached to a real person because you are just handling plastic knobs and stuff … I am just wondering if it starts feeling like a simulation and there is no risk involved because you just hit game over and restart and go around again. In a simulation environment if you have killed the person, perhaps psychologically you might distance yourself a little bit too far and end up taking unnecessary risks because it looks like a virtual environment rather than a real one. (i2F) I think there could be a tendency to not be as engaged with telehealth as with face-to-face? I think if you have got someone sitting over the other side of the table from you they have got your full attention for the entire time. (i10F)
Subtheme 2: Disruption
Disruption represents the failure of technology during a telehealth consultation, whether this is a complete loss of connectivity, through to latency issues that cause a time lag or pixilation which distorts the visual image on-screen. Telehealth interactions can become fragmented as a result of these transient and unpredictable experiences of disruption and can also increase the provider’s frustration with the service separation because of the need to repeat themselves and spend time reestablishing the lost connection. For example, “… there have been a few technical problems. Sometimes the audio quality can be a bit bad. It is quite frustrating and you have to repeat everything” (i15F). Repeating content adds time on top of the temporal lag of technology. Some providers develop coping mechanisms to adjust to the disruption of technology failure, for example, “this is a normal thing with a high-tech service” (i6F), “… it is technology, we expect it to fail” (i5M). Prefacing the potential for technological failure at the start of a consultation can be a way for a provider to minimize the potential that the patient may attribute the failure to the competence of the provider rather than reflecting the nature of technology itself.
Depending on the regularity at which telehealth is used, providers may not be able to reap the rewards of their time invested in learning telehealth, which creates diseconomies of scale in terms of the impost on their time which could be put to better use treating patients face-to-face. One way to adapt to change more efficiently is for providers to leverage the knowledge of those more experienced. For example, “… it was quite challenging because I was not aware of the set-up functions, and what the set-up was, but the nurses led me through it and it was a pretty good experience” (i4M). However, in the case of more complex telehealth offerings, such as robotic surgery, this learning curve and the requirement for provider adaptability to change is even more paramount. This is because robotic surgery enables the operation and synchronous treatment of a patient at a virtual distance, which requires practice. For example, “to do the full operation there is a huge learning curve … we like to think that we are fairly well trained, we like to think that we have to do thousands of different cases before we qualify” (i5M). In this instance, practice or frequent repeated exposure to telehealth is a coping mechanism by which providers can familiarize themselves with technology.
However, what appears to be the most challenging about the providers’ experience of disruption is that when it occurs, time must then be spent (often by the provider themselves) in trying to (a) either reestablish the connection with the telehealth technology that was being used or (b) attempt to use another form of technology to reconnect with the patient. For example, … {the video conferencing technology} let me down. We could not hear each other. We had good visuals but we had no sound. We solved it—they rang me on my mobile, and so I sat there with the mobile to my ear, and she had the phone on at the other end, and we just watched each other and did the voice stuff by phone. (i3F)
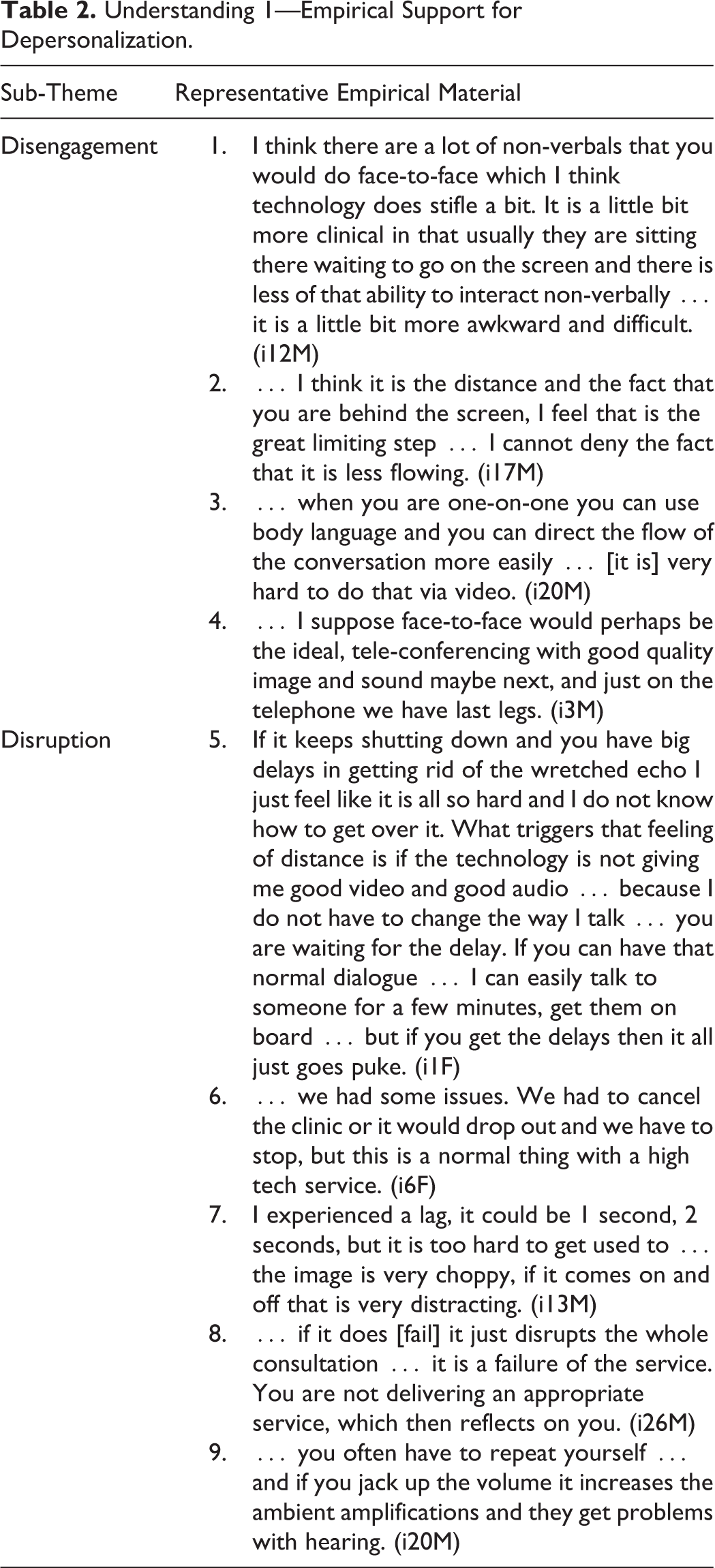
Understanding 1—Empirical Support for Depersonalization.
Understanding 2: Clinical voyeurism
Clinical voyeurism reflected providers’ experiences of being uncomfortable watching a patient on-screen. This seemed to particularly occur in the context of a clinical consultation, where sensitive information or personal parts that are normally “covered” are “revealed” for examination. Specialty fields where this can occur includes gynecology, urology, or dermatology (for skin conditions in “personal” areas) to name a few. For example, it can be uncomfortable for a provider to ask a patient to undress for a visual examination on-screen. The sense of privacy is not the same as in face-to-face interactions, where an image of the patient is not being streamed live over the Internet. For example, as one telehealth specialist indicates … telehealth technologies make it a little bit less comfortable in front of the camera, rather than face-to-face … because there is a big camera in the room. They worry about that, where it is broadcasting … whereas if you are in a cubicle and there are curtains all around it gives you a bit more comfort. (i12M)
Subtheme 1: Looking glass effect
The looking glass effect describes a provider’s heightened experience of watching and observing the patient on-screen. The ability of the provider to zoom in on a particular part of a patient’s body and to magnify it on-screen results in the sensation of how a looking glass makes an object appear larger than its real-life form. Aspects of clinical voyeurism appeared to stem from (a) cultural group differences (where being virtually represented is taboo) and (b) problematic symptoms that have to be “displayed” on-screen for diagnosis. The looking glass effect and the feeling of being observed could become even more exacerbated for patients from certain cultural backgrounds (e.g., indigenous populations), and providers need to be aware of this: … if you walk in and go ‘Hi, I’m here to test you or study you’ you are going to get an atrocious response rate and no one will want to engage you. So basically for us, when we knew we were going to be involved, we went up to [location anonymized] and on our very first visit we did not do any examination, no testing, nothing. (i1F)
Similarly, when observing a problematic symptom that is embarrassing or self-limiting for a patient (such as dysphagia), providers must also be cognizant of how the live streaming of the behavior (which must be performed in front of the clinician for an appropriate diagnosis to be made) is a challenge: … my area covers having problems with swallowing {i.e., dysphagia}. At first they {i.e., patients} did not like that. Even when I was there in person they did not like eating and did not like someone watching them eating …. But that changed with the facilitator up there saying ‘Come on, she’s got to watch you eat, this is why she is here, come on, one or two mouthfuls will do. (i1F)
Subtheme 2: Picture-(not)-in-picture
The provider’s picture-(not)-in-picture experience is defined by (a) the eye contact mismatch that often occurs with teleconferencing and (b) the presence of the inset picture of themselves shown on-screen. In this understanding, the provider must simultaneously negotiate how they themselves are portrayed to the patient by looking at the inset picture of themselves (to make sure they are on-screen and visible to the patient) versus actually looking at the patient to observe “their body.” The disorienting experience of this action lies in that when looking at the patient on-screen, the provider can actually appear to not in fact be looking at the patient because the line of eye contact is mismatched. This can create an uncomfortable sensation of clinical voyeurism for providers, as one explains: I think it is a little challenging to do eye contact, because where you look at the person on the screen, you are actually looking below the line of where the camera is. So it looks like to them that you are looking at their lap. (i2F)
Moreover, occasionally the service provider has to look down or away from camera or lean over to reach something or write something down (e.g., patient case notes) thereby moving “off-screen.” This can create the need for the provider to verbalize why they are “not in picture.” If left unexplained, this could give the provider concerns that the patient thinks they are inattentive—when in fact they are being attentive because of the very fact that the provider is accessing or writing case notes. This was described “… in terms of a laptop you are looking down at things … it is the odds between looking at them and typing” (i32M).
Clinical voyeurism can also manifest for a service provider in that they should also be cognizant of the fact that other individuals may legally be required to be present during the consultation but may not always declare themselves or make themselves known to the provider. This can heighten the providers’ experience of picture-(not)-in-picture voyeurism because they are discussing potentially sensitive patient information without knowing who is not in picture: The interview is set up with the camera and the patient and there are often people who are behind the camera who I cannot see. They never identify themselves during the consultations. There is usually a nurse there and some others as well.… There are issues with patient confidentiality … so if you are asking the patients about some personal things, they may not want to divulge that they have got a virus. So I think that is a negative factor … and I think it is partly because you are not getting what else is going on in the room, if there are other distractions that are playing a role as well—you are just with them. I do not know whether the people who are not on screen are pulling faces or how they are responding to what is being said. (i3M)
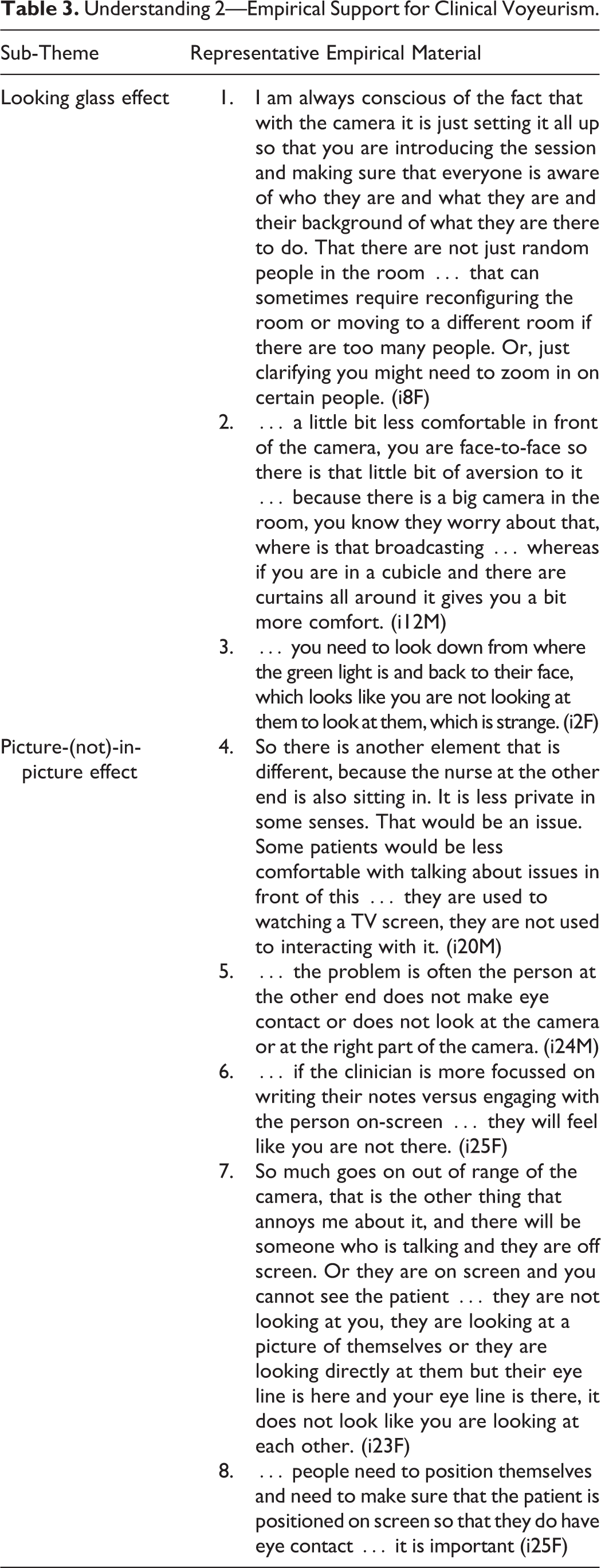
Understanding 2—Empirical Support for Clinical Voyeurism.
Understanding 3: Negotiating intangibility
Intangibility encompasses the providers’ experience of the loss of physical feedback through the inability for a provider to perform a hands-on clinical examination. This is a challenge that needs to be negotiated, and depending on the clinical specialty, this can be more or less important to the overall diagnostic information required for a clinician to treat a patient. The need to negotiate intangibility was commonly expressed by clinicians across two subthemes: (a) dismemberment and (b) disempowerment.
Subtheme 1: Dismemberment
Several interviewees described the “eeriness” or “unfamiliarity” of interacting with a patient who instantly appears on-screen in front of them, something that is unique to telehealth. In such instances of video-based teleconferencing, the patient is already often seated. Accordingly, dismemberment can impede a provider’s ability to gauge an initial assessment of the patient in terms of their demeanor, body language, approximate physical agility, and overall physical state in the moments from when the patient is called from the physical waiting room into the doctor’s consultation room. In the case of telehealth, this “traditional” part of the service interaction is removed. This impacts the provider’s ability to conduct the “end of bed test”: … just by observing a patient walk in, smile, and talk to you, you can get so much information. For example, one extreme would be say yourself {i.e., interviewee refers to interviewer} you are young, you look fit, you just walk into the room and you smile and shake hands, and we talk. I know that you are going to understand the consultation; I know that you are healthy and I know that you will go through surgery fine. On the other hand, let us just say your grandparent walks in with an oxygen tank, struggling to get onto the chair and they do not quite understand the concept—well that is not obviously suitable. Then you have people in between. Often the ‘end-of bed-test’—just visualizing them—gives you so much information. (i5M) That is really important about how you position yourself. The camera should be positioned above the screen—see that there {interviewee points to how their camera is set up to the interviewer}? The other thing is to sit back a fair distance so that you do not have the thing coming down on top of your head. (i6M)
Subtheme 2: Disempowerment
Tactile sensation or haptic feedback is a crucial aspect of doctor’s training. Physical examination of the patient is ingrained as a part of standard practice for most providers. The inability to physically examine a patient is disempowering for some providers. This is because they must either rely on (a) vicarious examination through self-reported data from patients or a third party such as a nurse, general practitioner, or other health care provider off-site with the patient; or (b) forego the physical exam altogether and adapt their clinical practice or defer the clinical exam until another time. Both of these create the potential for diagnostic uncertainty in that the provider does not have the direct interaction with the patient to support their own clinical judgment.
The stereotype of a “traditional” face-to-face consultation, whereby the provider has the option of physically examining the patient themselves, ceases in telehealth. Moreover, the “tools of the trade” that providers might typically carry around on their person—such as a stethoscope—are rendered useless. As the following experience indicates, negotiating intangibility can be challenging particularly in very hands-on disciplines such as physiotherapy: We use a lot of measurement devices to look for things like range of motion of joints or looking at muscle strength … that is hard remotely … we do a lot of manual therapy with our hands … which is hands-on so the challenge with telehealth is looking at those things and seeing if you can invent or use conventional equipment to get an alternative way of doing things. (i12M) That is one of the reasons they {i.e., the medical profession} have not done obstetrics. It is a very hands-on thing; you need to be able to lay your hands on a woman’s belly. Just looking at a picture on a screen, with someone at the other end who does not know how to feel a belly is just not going to work.” (i2F)
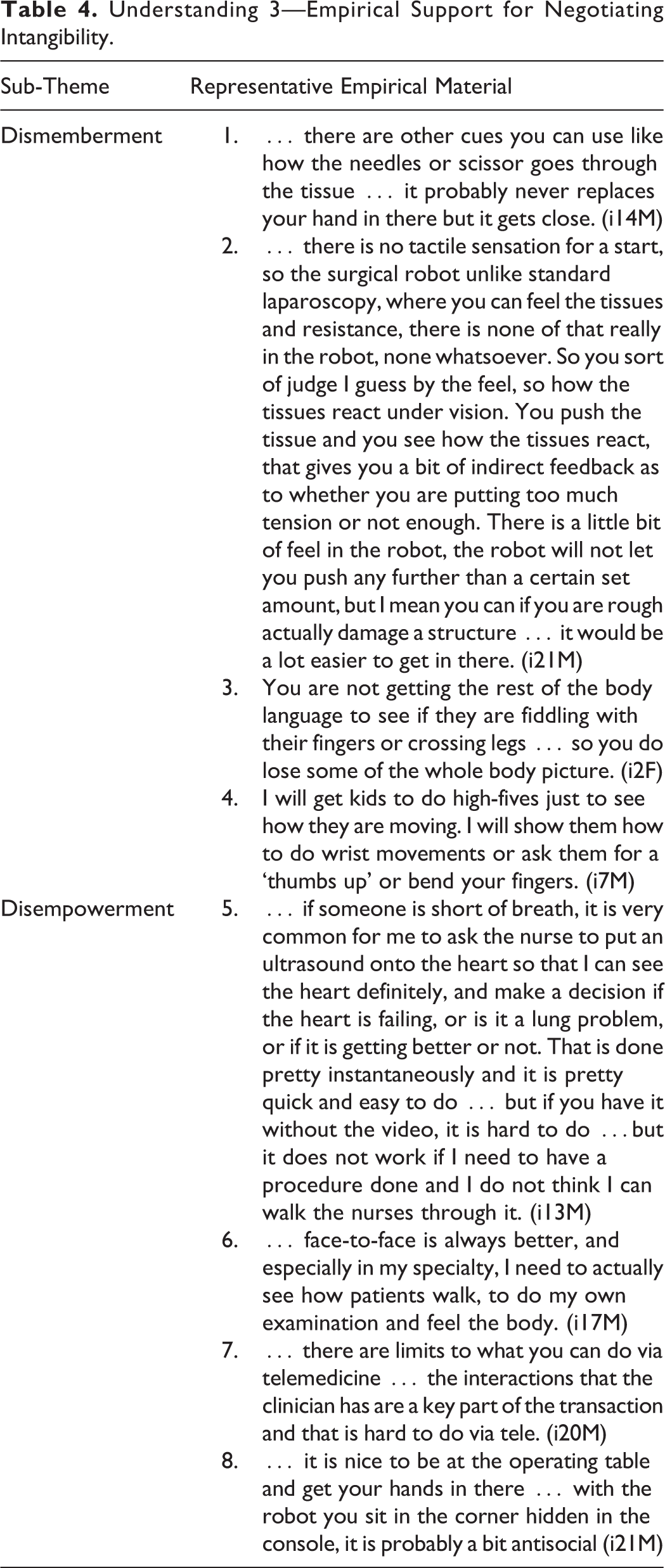
Understanding 3—Empirical Support for Negotiating Intangibility.
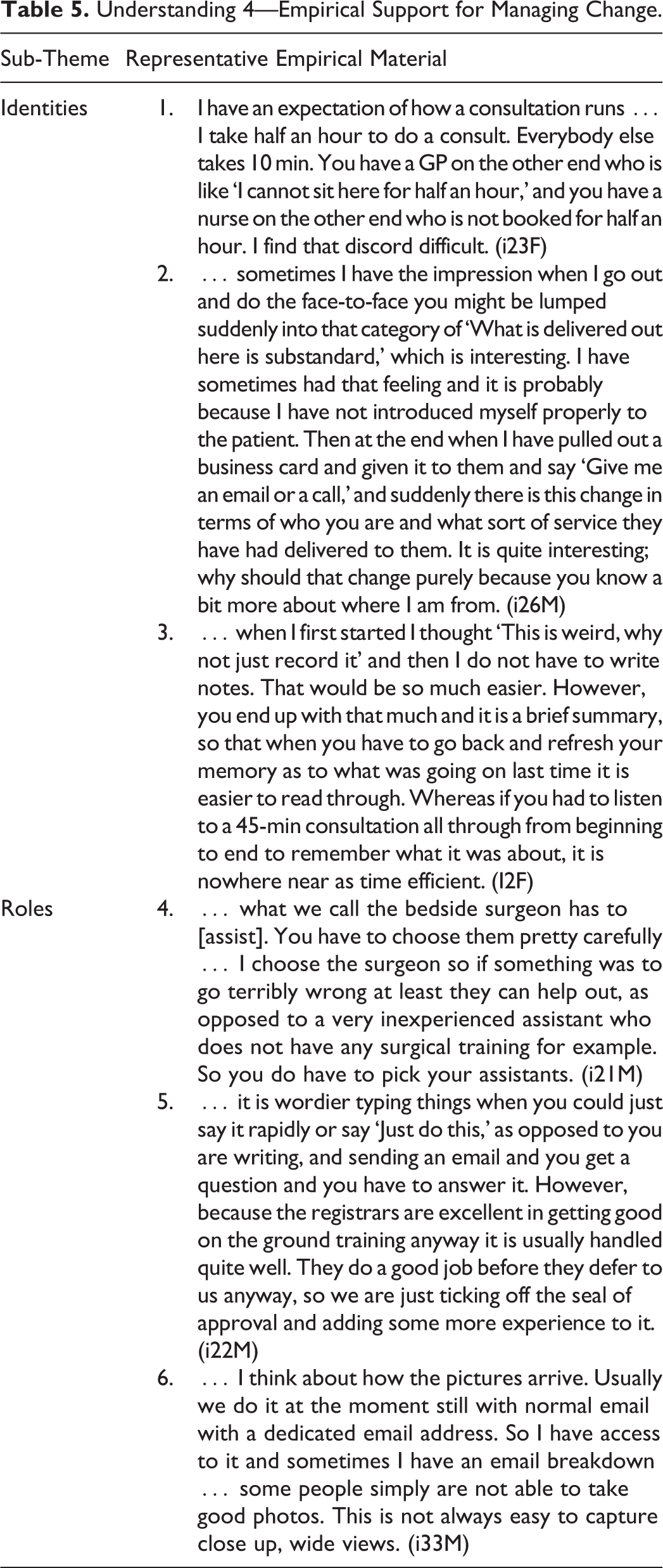
Understanding 4: Managing Change
This fourth and final understanding encapsulates the service provider’s experience of the emergent tension that seems to exist between the provider’s somewhat stable identity (i.e., as a physician) versus their relatively shifting role (i.e., as a technician) when engaged in telehealth. Hence, this fourth understanding was expressed across two subthemes: (1) stable identity and (2) shifting role.
Subtheme 1: Identity as a health care provider
Identity is taken to refer to the way in which a given individual professionally defines oneself. In terms of the sample of interviewees selected for inclusion in this study, it emerged that there is not one single “identity” that a service provider may adopt, but rather that one wears many professional “hats” throughout a typical day, let alone a single telehealth service interaction. For example, there may be multiple—even potentially competing—identities that are enacted by the one service provider which are experienced as a result of technology infusion in the separated service delivery interaction. One might define oneself as a health provider, then a telehealth provider, then specifically by affiliation to one’s tribe (i.e., geriatrics, endocrinology, orthopedics). A tribe here is taken to mean a group of similarly minded (i.e., telehealth enthusiasts) or similarly trained (i.e., geriatricians) individuals. Further to such classifications (which may be either self- or other imposed), a provider might exhibit further specializations or identifications based on the physical site in which the service provider is located (e.g., their hospital name or business practice location). The orientation or mindfulness of one’s physical location is exemplified in the below citation: … I teach something called situation awareness …. It means that you need to be aware of where you are in space, before the resident {i.e., registrar} calls them {i.e., the off-site patient} in. I get him to hold the file up so I can see the name very clearly, we pull out the file, and we usually have a piece of paper with “Charlie Brown.” As they sit down I usually say “Hi Charlie, how are you going?” I just try to give them welcoming feedback early. I let the resident go for a little while, sometimes it is a little difficult to understand the conversation and you miss things on telehealth where you might not miss them as much in the clinic. (i7M)
On top of negotiating the shift in responsibility with one’s identity is the deference of professional duties associated with one’s identity as a (telehealth) specialist to the hands, and therefore subjectivities, of another. This can be challenging to negotiate, particularly on top of the transition from “physician” to “technician.” As such, it seems apparent that there is some emergent sense of a hierarchy of identities that shape how a given individual interacts with others, particularly the patient in the context of a separated telehealth service interaction. A single overarching identity can fracture into many fragments of a service provider’s identity, simply through the infusion of technology to separate the service interaction with their patient. It is helpful to understand the different ways in which a service provider may come to understand their identity as a “physician,” before transitioning to the ensuing discussion of how service providers understand their role as a “technician.”
Subtheme 2: Role as a telehealth technician
The term role is taken to refer to the tasks and processes that one actually does in carrying out work-related duties, which may or may not be jarring in relation to one’s identity. In using telehealth technologies to separate the health care service delivery, providers often must implement, navigate, troubleshoot, repair, and deliver a technology-infused service as best they possibly can to an off-site patient who watches the whole interaction (i.e., these italicized terms are some of the role-related tasks of being a telehealth physician). The following interview excerpt points to the virtual domain that the service provider has to negotiate while managing the transition from one’s stable, secure, familiar, and experienced identity as a “physician” to one’s somewhat unstable, insecure, unfamiliar, or inexperienced role as a (telehealth) “technician”: If they {i.e., administration} change the software, if somebody changes the software it is always a bit of a pain for me but that does not happen very often. (i7M) There is a condition called Morphea. A photo of Morphea can just look like a shiny bit of skin with a bit of colouration around the outside. When you feel it, it feels like a scar, it feels quite firm. That is a nice little confirmatory test. But I can just ask them {i.e., patients}; I do not have a feely vision unfortunately [laughs], which would be nice! Palpation is not a huge thing, the big things I find are inadequate history, especially drug histories … and the images can be a problem. (i9M)
Understanding 4—Empirical Support for Managing Change.
Discussion
Advancing Service Delivery Through Technology Infusion
In their work on service research priorities in a rapidly changing context, Ostrom et al. (2015) highlight that when leveraging technology to advance service, it is paramount to focus on accelerating adoption and usage of emergent technology-enabled services by customers and employees. While in other service contexts, such as retail, banking, and education, the use of online service delivery, telephone communication, e-mail, video-based teleconferencing, and even some aspects of robotics have become somewhat ubiquitous, in health care these technologies remain a relatively uncommon service modality and somewhat novel for service providers. Our study contributes to the services literature by advancing understanding of service separation in the context of telehealth from the service providers’ perspective. Such an understanding is yet to be well understood in the extant services marketing literature. Arguably, this could be partly due to the unique risk, vulnerability, and fragility that is inherent to health care services (Berry and Bendapudi 2007). Our findings highlight that—while technology can be infused into the health care service delivery—the health care provider and their role cannot be replaced by technology alone. In this way, our study contributes to the service research priority of understanding ways to leverage technology to improve service design.
Toward a New Understanding-Based Theory of Service Separation Practices
Our phenomenographic data analysis process yielded four dominant understandings that interviewees’ collectively shared as part of their reported experience with service separation in the context of telehealth. Specifically, the categories of understanding that emerged as conceptually distinct were (a) depersonalization, (b) clinical voyeurism, (c) negotiating intangibility, and (d) managing change. Table 6 summarizes the outcomes of each of the four emergent understandings. These outcomes relate to the behavioral changes experienced by telehealth providers in embracing technology infusion to separate health care service delivery. We discuss these outcomes and then offer some nascent suggestions for how service providers working in the field of telehealth might overcome some of the challenges inherent in the understandings of their clinical practice.
Summary of the Outcomes of Service Providers’ Understandings.
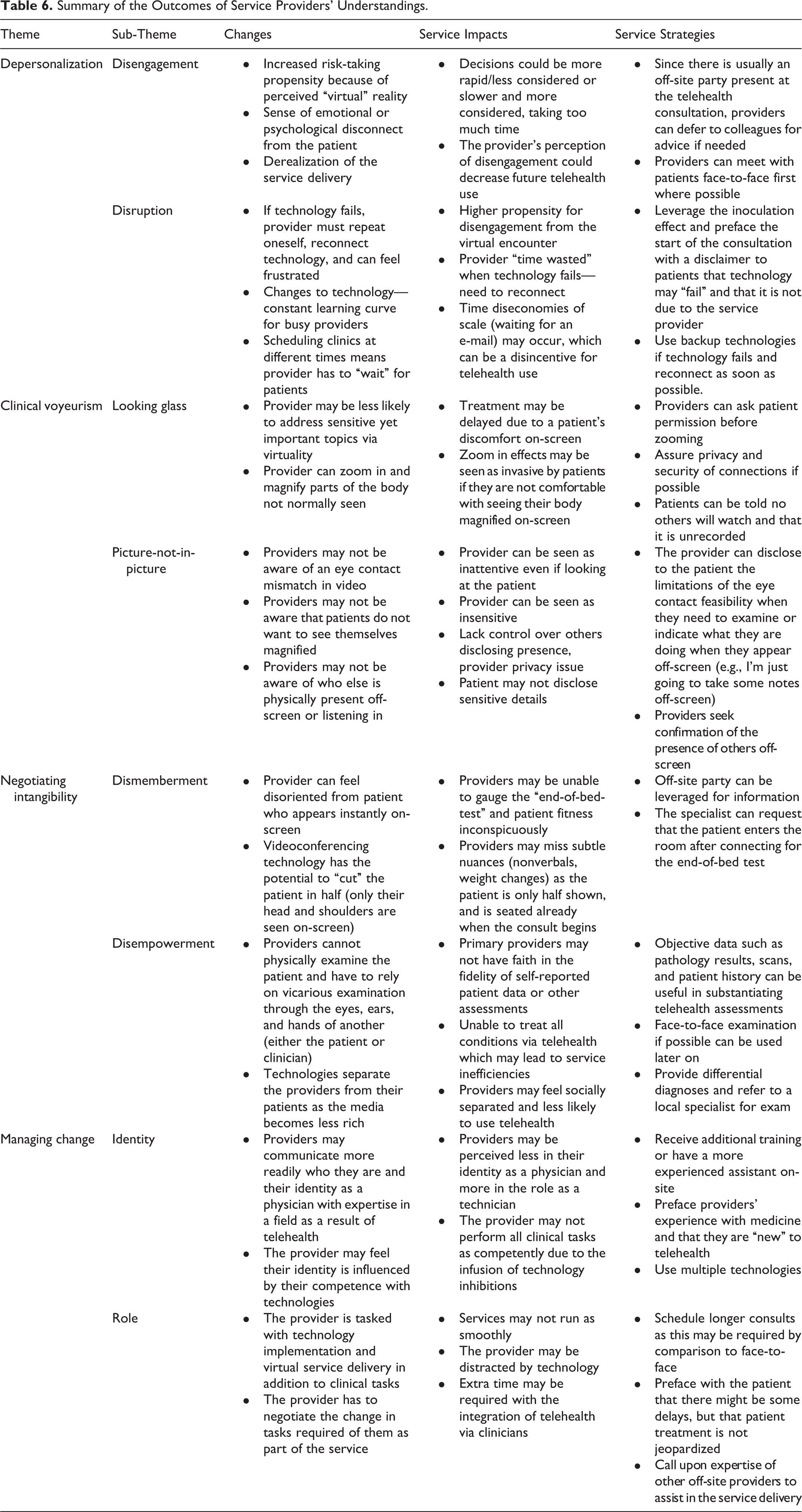
The understandings illustrate the four prominent ways that service separation affects the experiences of service providers during technology-infused service delivery. These shared understandings offer new insights into how the practice of technology infusion impacts service outcomes for providers. More specifically, this research identifies possible barriers to the adoption of telehealth which stem directly from providers’ lived experiences. We find that tensions exist for telehealth providers around depersonalization (virtual reality sensation), clinical voyeurism (visual disjointedness), how aspects of intangibility (such as loss of touch) are negotiated, and how health care providers manage juxtapositions between their clinical identity and their “technician” role. Examining the provider’s perspective on adopting a technology-infused service mode advances understanding of service elements that may detract from the perceived benefits of adopting these service modes—such as enhanced access and convenience (Keh and Pang 2010).
Overall, the results of this study suggest a need for a more encompassing definition of service separation. Existing literature has defined service separation as the spatial decoupling of service production and consumption, but what does this actually mean? We sought to identify the specific ways in which service separation is understood by those who engage with it as a part of their daily practice. The efficacy with which the separated service is delivered relies on the provider’s experience of integrating technology successfully to deliver health care virtually. In this way, the experiences of the service provider are extremely important and should be subject to further investigation both within the field of health care and in other service industries that are increasingly being virtualized.
While the service provider understandings revealed in our study are unique in many ways to the empirical context of telehealth, some degree of generalization to other service contexts is warranted. Increasingly many services are becoming virtualized including online education, banking, and shopping. An understanding of how service providers experience depersonalization from their customers, or how they negotiate intangibility when unable to directly interact with their customers, is of theoretical interest to advance our understanding of the phenomenon of service separation generally.
Practical Insights for the Field of Telehealth
A key challenge for the field of telehealth is uptake and this research offers several insights that health care providers, policy makers, and other vested stakeholders in the field of telehealth may find useful. Table 6 outlines several practical strategies for addressing the service changes and outcomes experienced by telehealth providers and may prove helpful for providers looking to adopt telehealth as a form of service delivery. These can more broadly be summarized around the need for enhanced formalized training and mentorship programs. To maximize effectiveness, these initiatives should be supplemented with enhanced support (i.e., technicians) for service providers adopting telehealth as well as practical guidelines that offer strategies to enhance telehealth service encounter experiences for both providers and patients. While doctors and other health care providers are required to undergo extensive training to engage in the professional arenas of their desired clinical specialty, when it comes to telehealth and its application, there is little formalized training for specialists. Training in terms of using the technology is separate from the issue of formalized training programs applying agreed upon social norms governing the practice of virtual medicine. As such, policy makers in the field of telehealth would be well placed to develop formalized guidelines outlining scope of practice documents for what can and cannot be treated via telehealth based on consultation with clinicians.
Understanding the similarities and differences in clinical practice and the way in which providers come to understand, and are subsequently socialized into, different clinical fields may help identify how to best train and mentor clinicians to adapt to and successfully take up telehealth. Current medical training is, by and large, still based around a service design model which operates on the assumptions that physical examination of patients face-to-face with the conventional tools of the trade (e.g., stethoscope, thermometer) is the norm. Telehealth is viewed as something novel and peripheral to the mainstream mode of service delivery. But what happens when one’s tools of the trade are removed—a stethoscope, for example, compared to an otoscope—and the provider has to rely more on their clinical judgment and potentially the hands-on assessment of another? Training programs should include modules based on practical guidelines and strategies that can be adopted by providers in the uptake of telehealth. These guidelines should address the service impacts that seek to decrease the provider’s (and patient’s) experiences of depersonalization, clinical voyeurism, as well as how to best negotiate service intangibility and maintain their identity as a health care practitioner. Second, it would be helpful to understand in further detail the psychological inhibitions that providers may have toward telehealth. Providing support and professional training programs, as well as implementing mentor programs between more experienced telehealth practitioners and less experienced telehealth practitioners, may assist in this role. This can help facilitate the training of upcoming health care providers across areas of clinical competence (i.e., identity) and technical role (i.e., telehealth expertise).
Finally, providers should be afforded the opportunity to leverage the knowledge of other more experienced telehealth colleagues (i.e., nurses, technicians) either within consultations or as a means to up-skill themselves. Further, telehealth coordinators could be employed to assist providers with the setup and maintenance of telehealth, so that they are able to remain focused on their clinical tasks rather than on technical tasks. The majority of research participants who were interviewed for our study developed their own adaptations and coping mechanisms to transfer their face-to-face practice to the virtual realm.
It is important for the clinician to be able to negotiate the potential challenges that can be presented by service separation in the following ways (see Table 6 for elaboration). First, to overcome the experience of depersonalization, the off-site clinician can prove invaluable in assisting with physical examination of the patient as well as facilitating rapport as they are often the primary carer. However, in instances where the off-site clinician is unable to assist, such as when the physical examination is too specialized, then specialist clinicians need to have alternative strategies which may require a face-to-face meeting to obtain the necessary diagnostic information. Similarly, it is important to recover from potential technology disruptions to minimize the perception of service failure; this requires either having backup technologies or prefacing the consultation with a disclaimer that technology is unpredictable and may not cooperate at all times and that this is not a reflection on the service provider but a reflection on the technology and its capacity. Second, to minimize the sense of clinical voyeurism, clinicians are able to use tactics such as gaining patient consent prior to zooming in with technology, acknowledging an eye contact mismatch if there is one, and confirming the security of the connection in terms of privacy and confidentiality. It is important to acknowledge who else may or may not be in the virtual consultation room, given that only a limited view of either end is portrayed to each party on-screen.
Third, to negotiate intangibility, service providers can engage in training if they are unfamiliar with a technology or engage the services of a telehealth coordinator for technology assistance where possible. The presence of the off-site party can be helpful in such situations as two providers are available to troubleshoot should the need arise; however, the clinician who is delivering the service is primarily tasked with using the technology effectively. Lastly, the tension between service providers’ clinical identity versus their potential role as a telehealth technician could be alleviated somewhat by scheduling longer consults until the provider is familiar with the technology and by ensuring that providers are portrayed first and foremost to the patient in terms of their clinical expertise without the technology getting in the way. Having backup technologies at hand and holding face-to-face consultations prior to telehealth consults may also be helpful strategies.
Limitations and Further Research
Although our study offers new insights into how service providers experience service separation in the context of telehealth, it is important to acknowledge the boundaries of the research. First, although we conducted an in-depth qualitative study by using an interpretive phenomenographic interviewing method, our insights are limited to one geographical context—Australia—and future research should examine other countries and service industries. Second, although data collection spanned almost a year, the data collected and analyzed was cross-sectional. A promising area for future research is to longitudinally examine the changes service provider’s experience over time from first adopting a separated service delivery mode.
Third, we examined service separation from the perspective of clinical health care service providers; however, as previously mentioned in doing so, we delimited the research scope to doctors and telehealth clinical specialists only. While to the best of our knowledge, this is the first qualitative study focused entirely on the experiences of service providers, rather than on customers, this negates the role of other actors. Telehealth service encounters can accommodate a whole host of service providers simultaneously including telehealth coordinators, technical sales personnel, nurses, and other allied health professions. As Sweeney, Danaher, and McColl-Kennedy (2015) highlight in their work on customer effort in value cocreation in health care contexts, such interactions between service providers are crucial. We acknowledge though that without the patient, the cocreated service encounter would be near impossible to accomplish. Finally, our focus on the health care service provider has opened up an initial conversation for future scholars in the area by starting to pave the way—within existing literature which is largely consumer centric and patient focused—in the health care service space (e.g., McColl-Kennedy et al. 2012; Sweeney, Danaher, and McColl-Kennedy 2015).
Telehealth can save time, money, patient, and clinician travel; improve access to and immediacy of treatment; and represent a more efficient delivery of health care services. Future research could focus attention on better understanding the implications of separating health care services across different clinical disciplines and from using different types of technologies fused into the service delivery. This would address the current research priority highlighted by Ostrom et al. (2010) and again elaborated by Ostrom et al. (2015) regarding the need to leverage technology to advance service science research.
Footnotes
Appendix
Description of Interviewee Sample.
| Clinical Discipline | Number of Interviewees | Technology Infused Into the Separated Service | Separated Services Offered Virtually Via Technology | On-Site Actors | Off-Site Actors | Off-Site Location |
|---|---|---|---|---|---|---|
| Geriatrics | 4 | Teleconferencing |
Dementia clinic Falls/neurological assessment General geriatric care |
Geriatrician |
Patient Nurse Doctor |
Residential facility; Rural hospital |
| Endocrinology | 2 | Teleconferencing |
Diabetes clinic General endocrinology |
Endocrinologist |
Patient Nurse |
Rural hospital |
| Surgery | 3 | Robotic telepresence |
Surgery Surgery |
Surgeon/s Anesthetist |
Patient Surgeon |
Same hospital |
| Dermatology | 4 | Store-and-forward e-mail Teleconferencing |
Acute rashes, allergy, acne Skin cancers/lesions General dermatology |
Dermatologist |
GP Patient |
Rural/regional hospitals |
| Speech pathology | 4 | Teleconferencing Store-and-forward e-mail |
Cancer care Speech therapy |
Therapist |
Patient Doctor |
Rural hospital |
| Physiotherapy | 2 | Teleconferencing |
Rehabilitation General physiotherapy |
Physiotherapist |
Patient Carer |
Home |
| Gastroenterology | 1 | Teleconferencing |
General gastroenterology |
Gastroenterologist |
Patient Officer |
Hospital |
| Orthopedic surgery | 1 | Teleconferencing Store-and-forward e-mail |
Fracture clinic |
Orthopedic surgeon Radiologist |
Patient Doctor Nurse |
Rural hospital |
| Rehabilitation | 1 | Teleconferencing |
Injury treatment |
Rehabilitation physician |
Patient Carer |
Rural hospital |
| Pediatrics | 1 | Teleconferencing |
Arthritis General rheumatology |
Rheumatologist |
Patient Parent/s |
Rural hospital |
| Gynecology | 1 | Teleconferencing |
Fertility treatment Obstetrics/pregnancy care General gynecology |
Gynecologist |
Patient Partner |
GP’s office |
| Cardiology | 1 | Teleconferencing Store-and-forward |
Lipid management Cardiovascular disease Hypertension |
Cardiologist |
Patient GP |
GP’s office, rural hospital |
| Perioperative medicine | 2 | Teleconferencing |
Perioperative assessment Pre/postsurgical care |
Physician |
Patient GP |
GP’s office, rural hospital |
| Allergy and immunology | 1 | Teleconferencing |
Immunopathology Allergy testing |
Immunologist |
Patient GP |
GP’s office |
| Neurology | 1 | Teleconferencing |
Neurology Neuromuscular disorders |
Neurologist |
Patient Carer |
GP’s office, rural hospital |
| Otolaryngology, ear, nose, throat (ENT) | 1 | Teleconferencing |
General ENT treatment |
ENT surgeon |
Patient |
Rural hospital |
| Psychology | 1 | Telephone Teleconferencing |
Counseling General clinical psychology |
Psychologist |
Patient |
GP’s office; Patient’s home |
| Pharmacy | 1 | Telephone/conferencing |
Virtual scripts |
Pharmacist |
Patient |
Rural pharmacy |
| General practice | 1 | Teleconferencing Robotic telepresence |
Emergency triage Remote resuscitation |
General practitioner |
Patient ED’s |
Rural hospital |
Note. GP = general practitioner, ED = emergency doctor.
Acknowledgment
This research was conducted with the support of the Centre of Research Excellence in Telehealth funded by the National Health and Medical Research Council (NHMRC; grant ID: APP1061183). The authors would like to particularly acknowledge Associate Professor Anthony Smith. the staff at the University of Queensland Centre for Online Health, and the staff of the UQ Centre for Research Excellence in Telehealth for their assistance in recruiting initial interviewees for this research and for insightful feedback on earlier presentations of this research. The authors are very grateful to the editors and the three anonymous reviewers for their helpful comments through the review process.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.