
Abstract
Telemedicine services leverage information and communication technologies toward innovating and enabling the delivery of healthcare. We propose and empirically analyze a framework for understanding the impact of telemedicine services on health outcomes at scale across communities in the United States. Our analysis of county-level panel data reveals that increased availability of telemedicine services improves community health that is central to the well-being of a community. We evaluate the benefits of telemedicine services in aggregate—that is, overall health outcomes—and along specific dimensions of reductions in premature death rate, low birthweight rate, preventable hospital stays, smoking rate, and the need for diabetes monitoring. In addition, we find that greater availability of telemedicine services is associated with decreased COVID-19-related mortality. Heterogeneity analyses further show that lower socioeconomic status reduces the effectiveness of telemedicine services while superior digital infrastructure and greater innovation capacity enhance its effectiveness. Demographics by way of higher proportions of Black and female community members enhance the effectiveness of telemedicine services, whereas a higher proportion of older adults reduces its effectiveness. Taken together, the proposed framework and the findings underscore the potential of telemedicine services to improve community health while recognizing the moderating effects of contextual factors. This study makes a significant contribution toward advancing the literature on seamless coordination of digital service innovations to drive community-wide health benefits.
Keywords
“The current (COVID-19) crisis has demonstrated the relevance of telehealth and created an opening to modernize the care delivery system. This modernization will be achieved by embedding telehealth in the care continuum at scale.” (Bestsennyy et al. 2021, p. 13) “Telehealth has huge potential to improve equity and access to care.” Sofi Bergkvist, President of the Center for Care Innovations (Smith 2022)
Introduction
Telemedicine services are a viable and integral approach for expanding healthcare access and delivery of services at scale, pushing the frontier of digitization in services (Bestsennyy et al. 2021; Huang et al. 2021). Telemedicine services leverage information and communication technologies (ICTs) to innovate and enable the delivery of healthcare while overcoming geographical barriers by connecting patients with healthcare providers located at distant sites (Srivastava and Shainesh 2015; World Health Organization (WHO) 2010). This includes “delivery of healthcare services through the use of real time two-way interactive audio and visual communications to provide or support healthcare delivery and facilitate the assessment, diagnosis, consultation, treatment, education, and care management of a patient’s healthcare” (Minnesota Telehealth Act 2022; National Institutes of Health (NIH) 2022). Our study addresses collaborations between local and remote providers that are carried out in clinic settings, including interactions between providers and patients (provider–patient) as well as interactions among multiple healthcare actors (provider–provider).
Our study is motivated by acknowledgment in the academic and practitioner literature that telemedicine services are a powerful driver of service innovation, offering a new healthcare service delivery model with the potential to improve community health that is central to the well-being of a community (Anderson and Ostrom 2015; Drago, Gatto, and Ruggeri 2023; Forjaz et al. 2025; Osmundsen et al. 2015). Telemedicine is fundamentally reshaping how healthcare services can leverage ICTs to design for seamless coordination and service delivery at scale (Barrett et al. 2015; Randhawa and Scerri 2015). Seamless coordination is the alignment and efficient integration of infrastructure, information, roles, interactions, and tasks among multiple stakeholders—particularly healthcare providers and patients—to enable a streamlined and enhanced care process with demonstrated societal benefits (Breidbach, Antons, and Salge 2016; Berry, Yadav, and Hole 2024; Go Jefferies, Bishop, and Hibbert 2021). Two examples from Mayo Clinic are: (i) implementation of Telemedicine Monitoring for Community Intensive Care Units (tele-ICU) in 2013, which connected six Minnesota hospitals to support care of critically ill patients through efficient inter-hospital transfers when necessary (Pannu et al. 2017); and (ii) a nurse-led home-based patient monitoring program for continuous connection between patients and providers (Coffey et al. 2022). Given this potential, studies have explored the drivers of telemedicine adoption and utilization, and associated outcomes at the patient, specialty, or hospital level (refer to Supplemental Appendix B.2 for a detailed summary of the literature). Managing telemedicine to innovate and enable delivery of healthcare services should help uplift “changes among individuals and collectives” and enhance “the well-being of consumer entities: individuals (consumers and employees), communities and the ecosystem” (Blocker and Barrios 2015, p. 265). While attempts to define such communities can reflect relational ties that are either physically proximal or virtual and based on shared interests or activities, we adopt a geographical definition (county, rural, urban, metropolitan, etc.) to align with healthcare research, policy frameworks, and intended delivery of telemedicine services across distances (e.g., Aljafari et al. 2024; Bell, Lee, and Gruca 2024; Farmer et al. 2001; Nilsen 2006).
Despite acknowledgement in the literature of the role telemedicine plays in service innovation, empirical support linking telemedicine services to community health remains limited. Further theoretical work on the effectiveness of telemedicine in contributing toward seamless coordination as a service innovation is much needed (Anderson et al. 2013; Blocker and Barrios 2015; Danaher and Gallan 2016; Ostrom et al. 2021). We infer from the extant service research literature that customer value co-creation requires extending beyond standard service metrics for quality, satisfaction, and customer behavioral intention to include assessment of customer or broader community quality of life and well-being (Danaher and Gallan 2016; Danaher et al. 2023; 2024). Go Jefferies, Bishop, and Hibbert (2021), in their study of UK telemedicine services, highlighted that provider organizations enhance their value proposition by inviting experiential inputs from patients and doctors as co-creators in the telemedicine care delivery process. This requires patients to develop knowledge and understanding of how to adapt to the system, facilitate effective self-care, and take control and responsibility for managing their health. Rather than passive recipients, patients actively shape their care experiences during telemedicine visits. To support this, clinics must adapt their operations and make institutional changes around telemedicine integration, and in this way, the telemedicine value proposition is co-created by patients and clinics.
More generally, this study addresses the significant need for research on healthcare services that extends beyond the traditional focus on providers and individual patients to explore broader effects on community health that is central to the well-being of a community (Anderson and Ostrom 2015; Anderson et al. 2013; Berry et al. 2022; Forjaz et al. 2025; Ostrom et al. 2021). This is especially crucial for telemedicine which transcends distance yet operates within geographic regions defined by geographical, demographic, and socioeconomic factors that are often the primary targets of health programs and policies (Farmer et al. 2001; Nilsen 2006; Polonsky et al. 2024). Thus, we investigate the role of telemedicine services for improving population-level health outcomes and community well-being in terms of premature death, preventable hospital stays, chronic illness care, and others (Danaher and Gallan 2016; Huang et al. 2021; Keiningham, Aksoy, and Malthouse 2024).
Availability of telemedicine services can increase remote patient visits, reduce patient travel costs, and increase care delivery efficiency, yet may not affect medical cost or care quality (Delana et al. 2023; Rajan, Tezcan, and Seidmann 2019; Sun et al. 2020). Some patients may even be worse off when telemedicine services are available (Sunar and Staats 2022). Overall social welfare may be undermined by inefficiencies in triaging patients to appropriate treatments and healthcare service offerings driven by telemedicine’s imprecision and associated costs in the virtual screening processes (Guan, Li, and Wu 2025). Notwithstanding the promise and potential of ICTs, their applications in enabling telemedicine services may lead to unintended consequences, and some health outcomes could, in fact, deteriorate (Berry, Yadav, and Hole 2024; Blocker Davis, and Anderson 2022; Jacobson 2023; Polonsky et al. 2024). For example, telemedicine may threaten “high-quality communication” for effective cancer treatment and is unlikely to fully replace in-person visits, especially when physical examination is crucial for accurate diagnosis (Hwei and Octavius 2021; Jacobson 2023, p. 512; Saljoughian 2021). Potential negative impact of telemedicine services and limited community-level empirical evidence motivate our deeper exploration of its impact.
This study is among the very first to expand on the scope of earlier studies that have shown individual, clinic, or hospital benefits from telemedicine services by investigating their impact on health outcomes at scale in communities, that is, at the county level. We identify the need for such investigation after conducting a comprehensive review of the relevant literature (e.g., Neufeld, Doarn, and Aly 2016; Patel et al. 2021; Shachar et al. 2020). Consistent with Berry, Yadav, and Hole (2024), our study also considers heterogeneity in the impact of telemedicine services on health outcomes by accounting for contextual factors of a county’s socioeconomic status, digital infrastructure, innovation capacity, and demographics. Service innovations often exhibit disassortative, imbalanced, and long-tailed usage patterns (Harvey et al. 2020), and macro‑level environmental heterogeneity may impact typical outcomes from telemedicine services (Aljafari et al. 2024; Castrogiovanni 1991). Notably, Aljafari et al. (2024) offered a theoretical framework on the moderating effects of regional contingencies, including access to computing resources and insurance coverage, and show how they can shape hospitals’ digital service performance, including readmission and patient satisfaction. Other studies emphasize rural–urban service differences in telemedicine service use or outcomes (Bell, Lee, and Gruca 2024). Specifically, our line of inquiry is aligned with and contributes to the well-documented recognition in the service literature that pervasive health disparities across communities should be addressed (Anderson et al. 2013; Berry, Yadav, and Hole 2024). Like other applications of ICTs in enabling service delivery heterogeneity in the impact of telemedicine is a relevant concern when aiming for equitable and consistent healthcare outcomes across communities (Berry, Yadav, and Hole 2024; Fisk et al. 2023; Sunar and Staats 2022).
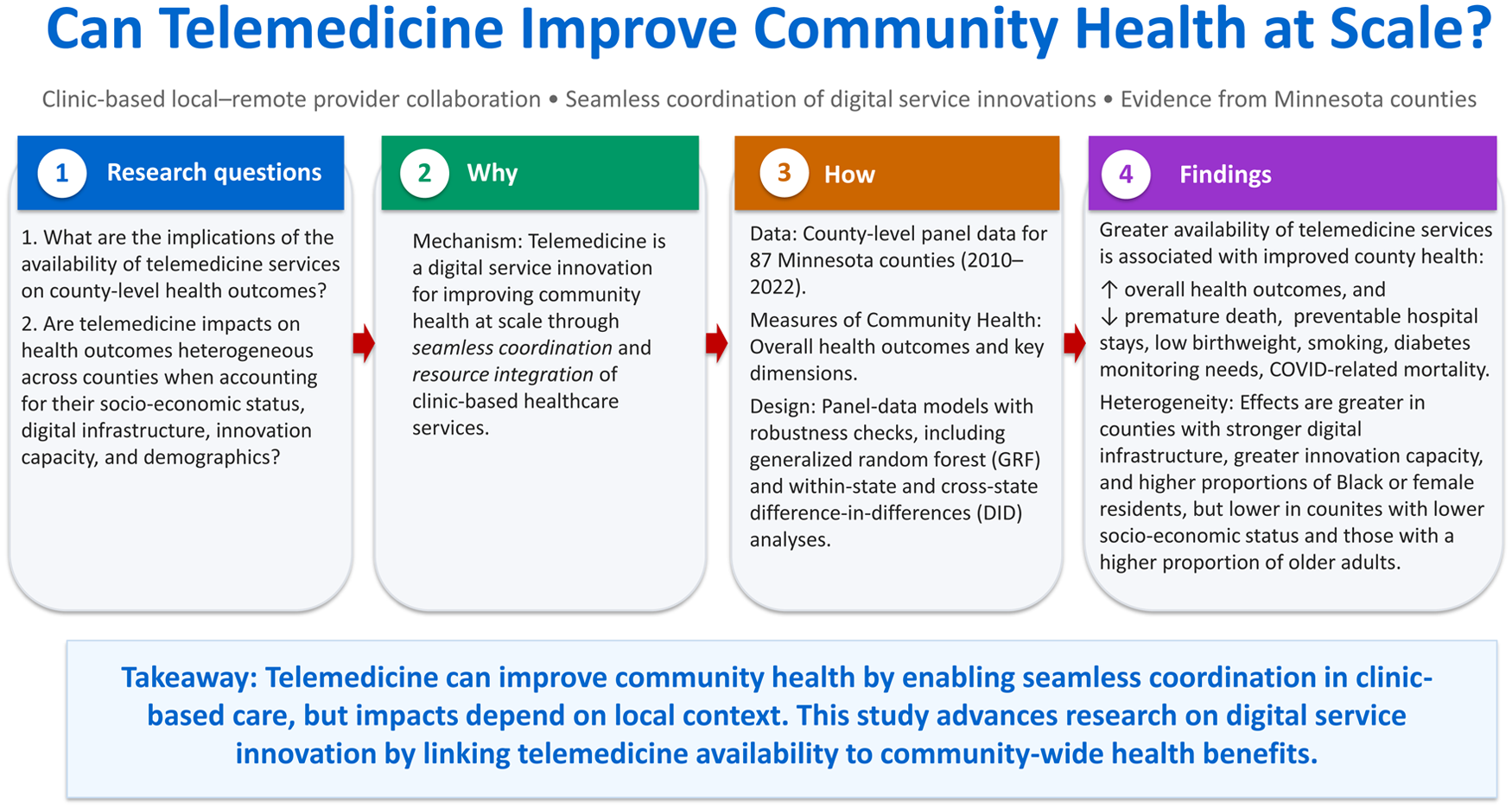
Considering the above discussion, the research questions (RQs) that serve as the motivation of this study are:
RQ1. What are the implications of the availability of telemedicine services on county-level health outcomes?
RQ2. Are the impacts of the availability of telemedicine services on county-level health outcomes heterogeneous across counties when accounting for their socioeconomic status, digital infrastructure, innovation capacity, and demographics?
We address the two questions, empirically, by developing and testing five hypotheses, drawing on the seamless-coordination framework of service innovation. This framework relates to value co-creation in communities (Anderson and Ostrom 2015; Barrett et al. 2015; Blocker and Barrios 2015; Danaher and Gallan 2016; Go Jefferies, Bishop, and Hibbert 2021; Ostrom et al. 2021; Vargo and Lusch 2008) and incorporates community heterogeneity (Aljafari et al. 2024; Castrogiovanni 1991; Nilsen 2006; Polonsky et al. 2024). The first hypothesis corresponds to RQ1, and the remaining four hypotheses correspond to RQ2. We integrate the relationships posited in the hypotheses to propose a conceptual framework for understanding the impact of telemedicine services on health outcomes at scale across communities in the United States.
This study focuses on clinic-based telemedicine service delivery in settings involving interactions among multiple healthcare actors. Specifically, the studied clinic-based service system meets the legal requirement of having a telemedicine license, delivers quality of care comparable to traditional practice, provides equal access, ensures safety, complies with privacy regulations, and accepts private and Medicaid payments for telemedicine services (Minnesota Statutes 2017). To conduct empirical analysis, we collect relevant panel data from several sources. Specifically, our analysis is based on county-level data from 2010 to 2022 for all 87 counties in the state of Minnesota in the United States. Our results indicate that greater availability of telemedicine services in a county improves county-level health outcomes both in aggregate—that is, overall health outcomes—as well as along specific dimensions that include reductions in premature death rate, low birthweight rate, preventable hospital stays, smoking rate, and the need for diabetes monitoring. In addition, analysis of relevant data from the COVID-19 pandemic period shows that greater availability of telemedicine services is associated with decreased COVID-19-related mortality, underscoring its effectiveness and reinforcing its lasting value in the community healthcare service system (Minnesota Department of Health (MDH) 2024). Our main results are supported by robustness checks and causal inference strategies addressing potential endogeneity concerns, including generalized random forest (GRF) analysis, controls for clinical care quality, instrumental variable and control function analysis, and both within-state and cross-state difference-in-differences (DID) analyses.
In analyzing heterogeneity in the impact of telemedicine services, we find that lower socioeconomic status significantly reduces the effectiveness of telemedicine services on overall health outcomes. Digital infrastructure reflected by higher internet speed and greater innovation capacity strengthen the impact of telemedicine services on overall health outcomes. We also find that the effectiveness of telemedicine services is greater when counties have relatively higher proportions of Black and female community members, whereas a higher proportion of older adults reduces its effectiveness.
Our empirical findings and the proposed framework, taken together, contribute toward advancing the service literature by underscoring the potential of ICT-enabled service innovations for improving community health at scale through seamless coordination and resource integration of clinic-based healthcare services (Go Jefferies, Bishop, and Hibbert 2021). The empirical findings include recognizing the moderating effects of contextual factors—namely, socioeconomic status, digital infrastructure, innovation capacity, and demographics—toward realizing the potential (cf. Anderson et al. 2013; Blocker and Barrios 2015; Danaher and Gallan 2016; Parasuraman and Colby 2015). Our study is among the first to advance understanding of the impact of telemedicine services as an ICT-enabled service innovation at a broad community perspective (Blocker and Barrios 2015; Ostrom et al. 2021). By characterizing telemedicine services as a service innovation for value co-creation through seamless coordination (Barrett et al. 2015; Huang and Rust 2017; Ollier et al. 2023; Randhawa and Scerri 2015), our study makes a contribution by highlighting the importance of using a multi-stakeholder, community-based approach (CBA) to assess the effect of telemedicine services on community health that is central to the well-being of a community (Anderson and Ostrom 2015; Forjaz et al. 2025; Freeman 1984; Nilsen 2006). At a more nuanced level, our findings on the heterogeneous impact of telemedicine services contribute toward advancing the service literature by showing how community-level geographic and socioeconomic heterogeneity can amplify, attenuate, or diversify the effectiveness of digital service innovation (Aljafari et al. 2024; Berry, Yadav, and Hole 2024; Castrogiovanni 1991; Patel et al. 2021). By acknowledging the moderating effects of socioeconomic status, digital infrastructure, innovation capacity, and demographics of counties, our study sheds light on the heterogeneous impacts of telemedicine services. These insights offer guidance on configuring the availability of telemedicine services to sustainably and equitably improve community health (Berry, Yadav, and Hole 2024; Huang et al. 2021; Keiningham, Aksoy, and Malthouse 2024).
Literature Review and Conceptual Foundation
Our study is informed by emerging streams of service literature on innovation related to seamless coordination (Barrett et al. 2015; Go Jefferies, Bishop, and Hibbert 2021; Huang et al. 2021) and community health (Anderson and Ostrom 2015; Blocker and Barrios 2015; Danaher and Gallan 2016; Ostrom et al. 2021). Furthermore, we consider how macro‑level environmental heterogeneity can impact the community health outcomes associated with telemedicine services (Aljafari et al. 2024; Berry, Yadav, and Hole 2024; Castrogiovanni 1991). We also review the literature on the unintended consequences of telemedicine services to ensure that we take a balanced view of their impact on community health while acknowledging their limitations.
Telemedicine and the Service Literature on Innovation
Increasingly, ICT-enabled telemedicine services are being used to deliver complex, off-site healthcare services that were once the sole domain of in-person interactions with onsite tools (Osmundsen et al. 2015), and support seamless coordination and resource integration (Go Jefferies, Bishop, and Hibbert 2021). Telemedicine services allow patients to remotely access medical specialists by visiting local hospitals and clinics rather than traveling to distant ones to access this care—a critical factor given that a five-minute increase in travel time can reduce hospital demand by up to 41%, a phenomenon known as “home bias” (Raval and Rosenbaum 2021). More generally, telemedicine services exemplify a fast-growing category of ICT-enabled innovations that have emerged to be among the key service research priorities with the potential to shed light on how services should be managed and delivered, including in “turbulent times” (Barrett et al. 2015; Ostrom et al. 2021; Srivastava and Shainesh 2015). In particular, during the COVID-19 pandemic, remote patient diagnosis and treatment using telemedicine services experienced substantial, unanticipated growth (Berry, Yadav, and Hole 2024; Bestsennyy et al. 2021; Dudley and Sung 2020; Hollander and Carr 2020; Rotenstein and Friedman 2020), with peak use accounting for 69% of doctor-patient visits in the United States in April 2020; similar use patterns were also observed in Europe and Asia (Pearl and Wayling 2022).
We characterize telemedicine as high human social presence and low automated social presence (van Doorn et al. 2017). In essence, telemedicine services reflect ICT-mediated interactions that remain substantively human-driven by both patients and providers. As such, telemedicine services represent a promising frontier for ICT-enabled innovations in the health sector, offering new opportunities for service innovation and enhancing the efficiency and effectiveness of healthcare delivery (Barrett et al. 2015). Furthermore, telemedicine is not a standalone ICT-enabled innovation but is deeply interconnected with other ICT advancements. According to Huang and Rust (2018), the integration of rapid technology evolution and applications into service processes is fundamentally altering service delivery and consumption by unbundling and enabling remote delivery of services, leading to the emergence of new types of technology-enabled services (Makridis and Mishra 2022).
Telemedicine and the Literature on Community Health
By defining community geographically at the county level in our study, telemedicine services are intended to complement conventional health services and benefit community health (Berry et al. 2022; Danaher and Gallan 2016; Ostrom et al. 2021). Thus, it is critical to examine how telemedicine services which (i) involve novel and innovative avenues of delivering care (Berry, Yadav, and Hole 2024; Danaher and Gallan 2016; Fisk et al. 2023; Parasuraman and Colby 2015), (ii) address health disparities (Sunar and Staats 2022), and (iii) integrate healthcare services for seamless coordination (Bavafa, Hitt, and Terwiesch 2018; Go Jefferies, Bishop, and Hibbert 2021; Rajan, Tezcan, and Seidmann 2019; Saghafian et al. 2018) impact community health. Investigating community health which involves multiple stakeholders of a service system—such as the clinic-based service system in this study—has emerged to be among the key priority areas in service research (Anderson et al. 2013; Blocker and Barrios 2015; Danaher and Gallan 2016; Danaher et al. 2024; Huang et al. 2021; Keiningham, Aksoy, and Malthouse 2024; Ostrom et al. 2021).
This line of inquiry aligns with the CBA to health and safety programs (e.g., Aljafari et al. 2024; Bell, Lee, and Gruca 2024; Farmer et al. 2001; Nilsen 2006) and stakeholder theory (Freeman 1984). CBA provides a useful lens for examining the role of telemedicine services in local communities because “the belief that the community-based approach is beneficial appears to have become a deeply held conviction in public health. . .. ‘It is almost an article of faith that locating programs in the community and involving community members in planning, implementation, and evaluation can be an effective strategy for improving population health’” (Nilsen 2006, p. 140). Based on critical analyses of the important principles, Nilsen (2006) suggested that substantial resource requirements, a long-term program view, and multifaceted interventions are the most important dimensions of successful application of CBA. This framing contrasts with most extant studies that take the adoption and implementation of telemedicine service programs (or online/digital platforms) as given or “free.” Therefore, our analysis of heterogeneity in the impact of telemedicine services is further informed by stakeholder theory (Freeman 1984), emphasizing relationships among and needs of all community stakeholders who are integral to healthcare services. The CBA to stakeholders has been frequently adopted to examine operations of firms and their impact on the sustainability and corporate social responsibility around various communities. In this vein, our research is akin to recently published studies examining how recent technology developments, such as chatbots, can support population-level health (Ollier et al. 2023), and how AI-related jobs contribute to community-level economic activity, well-being, and social welfare (Makridis and Mishra 2022).
Unintended Consequences of Telemedicine and the Gap in Literature
Telemedicine services, while offering numerous potential benefits, may have limitations and unintended consequences. Mindful of the wisdom in Brock and von Wangenheim’s (2019, p. 129) observation, that “AI certainly holds a lot of promise but it is not a panacea,” it is conceivable that telemedicine-enabled service transformation can lead to unintended failures and unforeseen harms (cf. Berry et al. 2022; Polonsky et al. 2024). Hence, it is imperative that we take a balanced approach to telemedicine services, acknowledging the barriers and challenges.
Effective implementation of telemedicine services requires seamless coordination among the multiple stakeholders of clinic-based services. System-level complexity and dynamism—characterized by multiple stakeholders, relationships, interactions, and constant changes in activities and progress—make it susceptible to failures and unforeseen harms (cf. Polonsky et al. 2024). A significant limitation is the inability of telemedicine services to fully replace in-person visits, especially when physical examination is crucial for accurate diagnosis, such as for chest pain or weight-based medication adjustments (Saljoughian 2021). The absence of hands-on assessment can compromise diagnostic accuracy and the quality of treatment and care, as a telemedicine service setting is not amenable to direct touch, physical presence, and emotional connection. Some patients may have limited capability to effectively communicate with doctors in a telemedicine service setting (Hwei and Octavius 2021). Online interactions can be impersonal and even alienating (Haimi 2023).
Inequity is another substantial barrier to telemedicine services, particularly for older adults, those with disabilities, or those lacking the necessary technology literacy, infrastructure, or trust (Berry, Yadav, and Hole 2024; Haimi 2023; Hwei and Octavius 2021). Even preference for technology-enabled healthcare options can vary (Ostrom et al. 2015; Saljoughian 2021). Telemedicine services may not meet all the needs of all community members (Berry, Yadav, and Hole 2024; Haimi 2023). There are concerns that the benefits of telemedicine services may disproportionately favor a small sub-population of tech-savvy individuals. Privacy and security are also major concerns, with complex terms and regulatory challenges that can discourage engagement in telemedicine services (Hwei and Octavius 2021). These issues can paradoxically exacerbate healthcare disparities rather than reduce them.
Overall, we find that most studies, to date, focus on addressing drivers of telemedicine service adoption and utilization (e.g., broadband subscription, cost, insurance, patient characteristics, infectious and contagious diseases and other care types; see Supplemental Appendix B.2 for a detailed summary of the literature). Similarly, some studies examine one or a few performance metrics at the patient, specialty, and/or hospital levels (e.g., patient travel distance, patient visits, chronic care management, and physician productivity). Yet, questions regarding the effectiveness of telemedicine services in improving health outcomes at scale in communities, as we do in this study, still remain largely unaddressed (Danaher and Gallan 2016). As noted earlier, we operationalize community health in terms of county-level health outcomes that include overall health outcomes, premature mortality, preventable hospital stay, chronic illness care, and others (Anderson et al. 2013; Berry et al. 2022; Ostrom et al. 2021), using counties as the geographic units commonly employed in research on the delivery of healthcare services (e.g., Aljafari et al. 2024; Bell, Lee, and Gruca 2024; Farmer et al. 2001; Nilsen 2006).
Hypothesis Development
The Impact of Telemedicine Services on Community Health
Individuals, families, and communities are stakeholders integral to achieving community health that is central to the well-being of a community (Anderson and Ostrom 2015; Anderson et al. 2013; Danaher and Gallan 2016; Forjaz et al. 2025; Freeman 1984; Nilsen 2006; Ostrom et al. 2021). Telemedicine services represents a transformative institutional arrangement that integrates dispersed healthcare resources through a digital “network-of-networks” (Barrett et al. 2015; Vargo and Lusch 2008). Telemedicine services exemplify the importance of technology-enabled, dynamic interactions in services—reminiscent of the “servuction” process (Miles 2010). Ultimately, telemedicine services enable seamless coordination and resource integration among healthcare providers, patients, and broader community members (Go Jefferies, Bishop, and Hibbert 2021).
Beyond supporting coordination, we infer from the extant literature that telemedicine can help strengthen healthcare services through networks by enhancing resource sharing, mutual value creation, and stakeholder alignment and integration within a shared institutional framework (Breidbach, Antons, and Salge 2016; Go Jefferies, Bishop, and Hibbert 2021; Vargo and Lusch 2008). With telemedicine, local and remote providers use shared information to refine and improve decision making, such as scheduling, staffing, technology use, and space allocation, while utilizing digital adaptation to foster innovation. Through collaborative engagement, healthcare partners can identify shared opportunities, establish best practices, and clarify their interdependent roles to enhance patient participation and improve treatment outcomes, thereby advancing mutual value creation for both clinics and the patients they serve. Stakeholder alignment can extend to indirectly involved stakeholders, including insurers and government entities, in defining shared expectations and coordinated processes. The diffusion of telemedicine services demonstrates how collaborative learning, absorptive capacity, and institutional support can be critical for sustaining system-wide service innovation (Cohen and Levinthal 1990), generating benefits that extend beyond individual providers or patients to the broader community.
Leveraging telemedicine services to enhance community health is driven by the need to expand care access and disease management in rural healthcare systems (Barrett et al. 2015; Harrison 2019; Ishfaq and Raja 2015; Srivastava and Shainesh 2015), reduce readmissions (Queenan et al. 2019), and increase physician acceptance of the technology (Smith et al. 2020). However, the literature also highlights persistent barriers, including uncertainty regarding cost-effectiveness and concerns pertaining to quality, safety, privacy, regulation, and reimbursement (Mitka 2003).
Despite these challenges, telemedicine services can alter the existing model of in-person delivery of care (Čaić, Odekerken-Schröder, and Mahr 2018; Green, Hartley, and Gillespie 2016; Jacobson 2023). Recent studies provide evidence of improved operational efficiency and care performance: telemedicine enhances specialist productivity and overall welfare (Rajan, Tezcan, and Seidmann 2019), increases office visits (Bavafa, Hitt, and Terwiesch 2018), improves triage efficiency (Saghafian et al. 2018), and shortens emergency room stays by 31% (Sun et al. 2020). At the system level, opening a telemedicine center reduced patient travel by 30% and increased visits by 31% (Delana et al. 2023). Hospitals with stronger digital capabilities, including telemedicine, report lower readmissions and higher patient satisfaction (Aljafari et al. 2024).
Toward seamless coordination of care, telemedicine services strengthen links among providers, patients, community stakeholders, and resources—enhancing access, participation, and knowledge co-creation in service innovation (Barrett et al. 2015; Danaher et al. 2024; Farmer et al. 2001; Randhawa and Scerri 2015). Through iterative cycles of assessment, learning, and process redesign, telemedicine empowers community members and providers to mitigate potential downsides and enhance community well-being (Polonsky et al. 2024). With such continuous coordination, telemedicine services enable clinics to provide access to expanded resources such as specialty expertise during regular in-person visits, so it becomes feasible for clinics to provide an integrated set of appropriate care options to patients (Bavafa, Hitt, and Terwiesch 2018; Rajan, Tezcan, and Seidmann 2019; Saghafian et al. 2018). These digitally mediated connections generate system-wide synergies that link patients with both local and distant providers, facilitating timely feedback and continuous innovation in clinical practice. Such recursive exchanges expand the collective knowledge base and enhance value co-creation across the care network.
Furthermore, Nilsen (2006) suggested that substantial resource requirements, long-term program view, and multifaceted interventions are the most important dimensions of successful CBAs, while Freeman (1984) emphasized relationships among community stakeholders. Telemedicine supports stakeholder alignment by strengthening relationships and fostering shared expectations among patients, providers, insurers, and government entities. Taken together, the above discussion suggests that it is critical to assess the impact of availability of telemedicine services through a broader community-level lens. Thus, we posit the following hypothesis:
Heterogeneity in the Impact of Telemedicine Services
The impact of telemedicine service on community health depends on coordination among stakeholders; thus, local community contexts and broader institutional environments are critical (Aljafari et al. 2024; Nilsen 2006; Polonsky et al. 2024). Polonsky et al. (2024) proposed that policymakers and system designers are essential enablers, since successful adaptive service systems require adequate resources and institutional support. Theoretically, community heterogeneity reflects macro-level environmental munificence “caused by demographic, technological, or other discontinuities” (Castrogiovanni 1991, p. 552). Aljafari et al. (2024) extended this theoretical framework by incorporating local environmental moderating contingencies such as metropolitan computing resources and insurance coverage.
Our investigation is guided by the European Commission’s European Collaboration of Health-Care Optimization (ECHO) initiative, which calls for building a “knowledge infrastructure” to promote better healthcare delivery and advance “equity, effectiveness, safety and efficiency at international, national, regional, and even provider level” (ECHO 2021). Danaher and Gallan (2016) highlighted the need for impactful research linking healthcare access to community health and health disparities. Fisk et al. (2023, p. 543) drew attention to detrimental effects of the digital divide, and propose that “access to computing devices and the Internet provided by schools, public libraries, and community centers helps address the first form of inequality.” We contend that telemedicine services can address these challenges by bridging gaps in access to healthcare services. Specifically, we adopt a contingency perspective and study how community contextual factors moderate the effect of availability of telemedicine services on county-level health outcomes (e.g., Aljafari et al. 2024; Berry, Yadav, and Hole 2024; Ramdas and Swaminathan 2021).
We examine heterogeneity in the community-level impact of availability of telemedicine services while accounting for the socioeconomic status, digital infrastructure, innovation capacity, and demographics of a county. Such county-level contingencies are crucial when resources are limited, and social issues may alter the effectiveness of telemedicine services when healthcare programs are largely embedded in communities (Ramdas and Swaminathan 2021).
Socioeconomic status
Service research needs to “address the dilemmas of inequality and deprivations of poverty . . . particularly in contexts of vulnerability . . . discrimination and urban poverty” (Blocker and Barrios 2015, p. 265). Recent studies show that socioeconomic status can alter the impact of technology or programs, as communities with sufficient resources can support seamless coordination, whereas those lacking such resources face higher risks of unforeseen harms and implementation failures (Aljafari et al. 2024; Go Jefferies, Bishop, and Hibbert 2021; Polonsky et al. 2024). Availability of telemedicine services can reduce health disparities for rural low-income patients (Srivastava and Shainesh 2015), but this benefit may not transfer to urban low-income patients (Sunar and Staats 2022). For example, Zepeda and Sinha (2016) found that community socioeconomic status moderates the relationship between affordability of behavioral healthcare services and behavioral health outcomes. Sunar and Staats (2022) showed patient income levels, rural versus urban locations, and care quality differences affect telemedicine service outcomes. Similarly, Yancy (2020, p. 1891) noted that: “Low socioeconomic status alone is a risk factor for total mortality independent of any other risk factors.” Therefore, we investigate the moderating effect of socioeconomic status of a county by positing the following hypothesis:
Digital infrastructure
We examine the role of digital infrastructure by considering the internet speed in a county. Internet speed plays an important role in healthcare and medical information seeking, as well as in communication between patients and providers of healthcare services (Perrin and Atske 2021; MDH 2024). Moreover, regional digital literacy and internet connectivity enhance residents’ ability to adopt and use digital health tools, with possible spill-over effects on healthcare engagement and outcomes (Aljafari et al. 2024). Fisk et al. (2023) reported that internet access helps to address inequality and increase digital inclusion. However, in 2021, 7% of all Americans and 25% of older adults (aged 65 and above) did not use the internet at all (Perrin and Atske 2021). Internet non-adoption is more prevalent among low-income, less educated, and rural populations. A recent report suggests that federal funding to improve internet speed holds some promise for reducing healthcare disparities (Rabbani 2024). Thus, we study the moderating effect of digital infrastructure by way of internet speed on county-level health outcomes because this is essential for fully realizing the benefits of telemedicine services (Daniel and Sulmasy 2015). Hence, we posit the following hypothesis:
Innovation capacity
We also examine the moderating effect of innovation capacity on the relationship between availability of telemedicine services and county health outcomes. As noted earlier, ICTs enable service innovations that are revolutionizing the service landscape (Huang et al. 2021) and shifting the core dynamics of service (Makridis and Mishra 2022).
Innovation capacity of a county captures dimensions such as human capital, knowledge creation, business dynamics, employment, and productivity. Accumulation of the effects of the dimensions underlying innovation capacity can shift the scale of interactions between businesses and service activities as evidenced in a study situated at the intersections among ICTs, healthcare, and knowledge creation in Massachusetts (Porter 1998). Some cities and regions are even incentivized to establish service hubs to scale exports (Makridis and Mishra 2022; Porter 1998). Across 343 US cities, Makridis and Mishra (2022, p. 509) found, empirically, that emerging-technology-related job growth leads to higher economic growth and increased subjective well-being that is inclusive of “health and medical conditions.”
We contend that availability of telemedicine services and innovation capacity are complementary in their relationship to community health due to increased service quality and coordination among clinics, hospitals, patients, and other stakeholders of the healthcare system. These benefits arise from stakeholder involvement in rapid recognition of community health needs, new care delivery options, care delivery flexibility, and reduced costs. Community stakeholders are closely involved in these processes and provide timely support and feedback. For example, integration among various ICTs reflects organizational and operational decisions and practices for enabling service innovation (Barrett et al. 2015; Randhawa and Scerri 2015). Knowledge and experience acquired from use of one technology can diffuse to use of related technologies, and thus, contribute to improved learning processes (Angst et al. 2011). Furthermore, learning that results from greater innovation capacity may enhance use of telemedicine services because the knowledge applies broadly to service innovation functions and features (Barrett et al. 2015). Thus, absorptive capacity increases when providers use telemedicine services (Cohen and Levinthal 1990). In summary, we posit the following hypothesis:
Demographics
Structural racism and societal service disparities for vulnerable groups, such as older adults (65 years and above), present substantial challenges to sustain service offerings (Huang et al. 2021). In studying the impact of digital services on hospital-level outcomes, Aljafari et al. (2024) controlled for regional demographics such as education level, age distribution, loneliness prevalence, and gender composition. We consider the moderating effects of county demographics to understand contexts in which telemedicine services may amplify or attenuate health outcomes. Specifically, we consider race, gender, and age with respect to their interaction with availability of telemedicine services and impact on county-level health outcomes.
In his call to address healthcare disparities in the United States, Yancy (2020, p. 1891) noted that “underrepresented minorities are developing COVID-19 infection more frequently and dying disproportionately,” and that “the communities where many black people reside are in poor areas characterized by high housing density, high crime rates, and poor access to healthy foods.” Given these disparities, we contend that availability of telemedicine services may be more effective in counties with higher ratios of Black community members. Thus, leveraging telemedicine services has the potential to increase access to care, improving health outcomes for underserved sub-populations (cf. Ganju et al. 2020).
We also consider the moderating effect of the population gender ratio. Gender composition is known to be related to healthcare delivery effectiveness (Tang et al. 2024). For instance, in their investigation of patient preferences for telemedicine services, Narcisse et al. (2022) presented empirical evidence that females have greater odds of using such services.
Finally, we examine how the effectiveness of telemedicine services is moderated by the proportion of older adults in a county’s population. Customer service preferences and experiences can significantly vary across age groups, suggesting that age should be considered as a moderating factor in examining the effect of telemedicine services on health outcomes (Berry, Yadav, and Hole 2024; Haimi 2023; Hwei and Octavius 2021). For example, patients who are older adults often lack the requisite technology literacy (Berry, Yadav, and Hole 2024), and not enough telemedicine service solutions are tailored for older adults (Haimi 2023).
Considering Black, female, and older adult community members as markers of county demographics—by way of race, gender and age—the availability of telemedicine services in counties with higher proportions of these sub-populations may result in varied healthcare outcomes. In other words, the benefits of telemedicine services may be more pronounced in counties with higher ratios of Black and female community members, while the opposite effect is likely in counties with higher ratio of older adults. Based on these considerations, we hypothesize the following moderating effects for the three demographic characteristics:
Proposed Conceptual Framework
We integrate the relationships posited in the above hypotheses into a conceptual framework depicted in Figure 1. The framework provides a nuanced understanding of how availability of telemedicine services can improve community health while acknowledging the moderating effects of the salient contextual factors relevant to a community—that is, socioeconomic status, digital infrastructure, innovation capacity, and demographics.
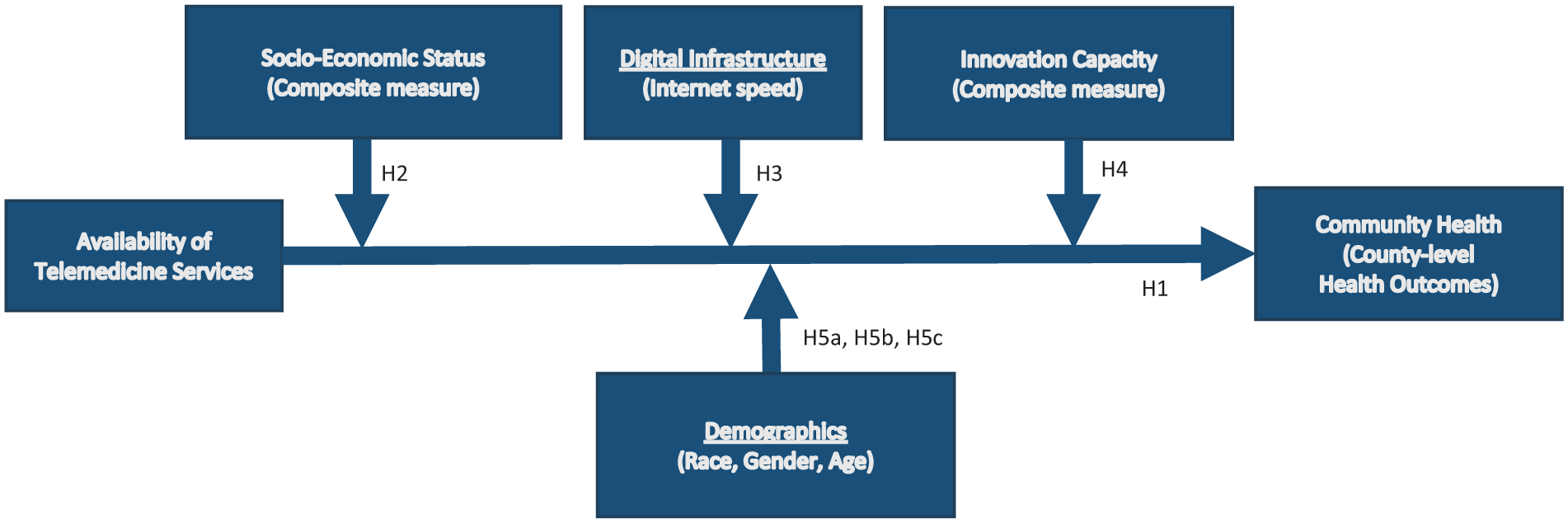
Conceptual framework for the impact of availability of telemedicine services on community health.
Data Variables and Measures
The unit of analysis in this study is a county. We obtained US county-level health outcome data from County Health Ranking & Roadmaps (CHR 2022), and data on availability of telemedicine services from the Minnesota e-Health Initiative (Soderberg 2014). CHR compiles detailed annual county-level data on health outcomes from national and state sources, including Centers for Disease Control and Prevention, Behavioral Risk Factor Surveillance System, and Dartmouth Atlas of Healthcare. These measures capture local population health under the broader categorization of population health and well-being, serving to identify areas needing improvement for healthcare services as “elementary service that applies to every individual” in the community (Aljafari et al. 2024, p. 1346). We obtained data on the following county-level health outcomes for all 87 counties in Minnesota from 2010 to 2022 (see Supplemental Appendix A.1 for details):
(i) Overall health outcomes (CHR-created measure based on indicators of premature death, poor or fair health, poor physical health days, poor mental health days and low birthweight; the measure is a normalized z-score).
(ii) Premature death rate (years of life lost before age 75 per 100,000 population)
(iii) Preventable hospital stay rate (discharges per 1000 Medicare enrollees for outpatient-treatable conditions)
(iv) Low birthweight rate (percentage of all births)
(v) Smoking rate (percentage of adults)
(vi) Diabetes monitoring (number of diabetic Medicare enrollees)
These measures include direct health outcomes related to quality of life, health status, mortality, hospitalizations, and chronic disease management—conditions with severe health implications and high treatment costs. For example, the Minnesota Department of Health emphasizes telemedicine as a critical tool to “help prevent diabetes in adults at risk for developing type 2 diabetes and to provide self-management and monitoring support for people with diabetes” (MN Department of Health 2024, p. 28). The first and sixth measures are reverse coded by CHR so that, like the other measures, lower values indicate desirable outcomes. We use a (natural) logarithmic transformation of the county health outcome data to reduce skewness across counties [ln (1 + y)], except the first category—overall health outcomes—which is already normalized by CHR. For example, the CHR-reported diabetes monitoring ranges from 16 to 4,185, with a mean of 294, median 152, skewness 4.7, and kurtosis 26.7.
Our data on availability of telemedicine services come from the Minnesota e-Health Initiative (Soderberg 2014), which provides detailed annual clinic-level information. The Minnesota e-Health Initiative, coordinated by Minnesota Department of Health and Center for Health Information Policy and Transformation, is a legislatively-authorized public−private collaborative to advise and advance the use of health information technology in Minnesota (MDH 2020). We combine annual data from 2010 through 2018 and biannual data for the years 2020 and 2022, adapting to a change in data collection frequency promoted by the state policy shift, to construct a structured, unbalanced panel dataset. In the combined panel, 2,549 unique clinics (based on consolidated unique IDs, clinic names, and locations) are represented in the study sample; 263 clinics are present in all years, and 1,507 clinics are present in four or more years. The annual response rate of the Minnesota e-Health Initiative survey averaged over 80%. We identify the county of each clinic through a geocoding process of converting addresses to latitude/longitude coordinates. Our two main data sources for geocoding are Nokia’s Here map and Google’s Map Application Programming Interface (API).
Independent Variables and the Sample
We develop a county-level measure of telemedicine services by aggregating clinic-level data on the availability of telemedicine services. We first identify the yearly availability of telemedicine services for each clinic based on whether the following telemedicine activities are conducted at a clinic: (i) host site where service is provided via telecommunication systems; (ii) host site for referral provider, with providers at another site who provide services; or (iii) host site for general practitioner, with specialists at another site who assist in rendering a diagnosis. Clinics respond to the three items: Yes or No. For each study year (2010–2022), we construct an indicator of availability of telemedicine services at the clinic level: (1) if a clinic indicated any of the three measured items, and (0) otherwise (see Supplemental Appendix A.2 for details).
To investigate the effect of availability of telemedicine services on county-level health outcomes, we aggregate the clinic-level telemedicine measure to the county level. Thus, in the second step, we determine how many clinics have (1) for availability of telemedicine services for each county and year and then divide by the number of clinics in the county that year to calculate a proportion measure for each county-year. Thus, using this proportion measure, we can examine the effect of availability of telemedicine services at the county level.
With the two data sources, county-level data on health outcomes and clinic-level data on availability of telemedicine services, we match these data using county as the matching criterion. Our matched sample includes 87 counties over 11 years, resulting in 957 county-year observations before accounting for missing values.
In Figure 2, we plot trends in the proportion of availability of telemedicine services for clinics and counties over the study time interval. Both plots indicate an increasing proportion of clinics providing telemedicine services, reflecting the level of availability of telemedicine services is increasing in Minnesota clinics.
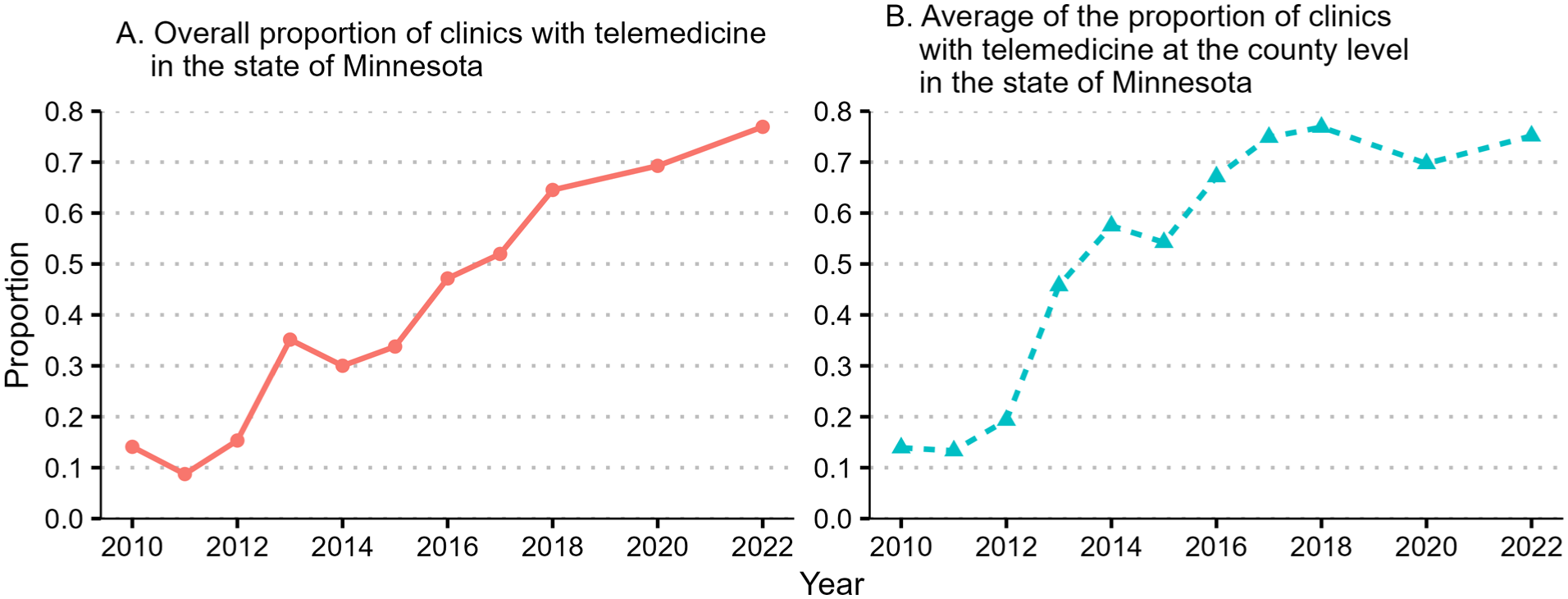
Trends in the availability of telemedicine services in the state of Minnesota.
Moderating Variables
We acquire data from CHR (socioeconomic status); Federal Communications Commission (FCC) (internet speed); Indiana Business Research Center (IBRC) (innovation index); and US Census (race, gender, and age). Specifically, CHR provides the measure for socioeconomic status, which is a composite measure reflecting the level of income, education, employment, safety, and social support in a county. This measure captures the percentage of population with high school degree and some college education, unemployment rate, children in poverty and income inequality, children in single-parent households and access to social opportunities, as well as violent crime and deaths. CHR provides reverse coded z-scores for this measure among all counties in a state, so higher values represent undesirable outcomes.
Digital infrastructure is measured by internet speed of a county reported by FCC. Specifically, internet speed is based on the value reported for residential fixed broadband connections with a downstream speed of at least 10 Mbps (number of housing units with connections per 1,000 housing units).
To study the moderating effect of innovation capacity, we acquire county-level innovation index data from IBRC at the Indiana University Kelley School of Business (https://www.statsamerica.org/innovation/). The data include the 2023 Headline Innovation Index which aggregates underlying core indexes for innovation inputs and outputs. The index reflects a region’s capacity for innovation, considering human capital, knowledge creation, business dynamics, employment, productivity, and overall economic well-being.
Data on county demographics is collected from US Census annual reports. The unit of observation is county-year. Race reflects the proportion of selected racial sub-populations (classifications that include Black community members). Here, we focus on the proportion of: (i) Black or African American alone or in combination; (ii) Black or African American alone; (iii) Hispanic, Black, or African American alone or in combination; and (iv) Hispanic, Black, or African American alone. These race category designations are reported in the US Census data. Gender reflects the proportion of females in the total population of a county. Age reflects the proportion of a county’s population who are 65 years and older.
For ease of interpretation for the moderation effect analysis, the measures of internet speed, innovation index, race, gender, and age are all calculated by removing the mean values over all counties in a year to obtain a relative measure (similar to the treatment of socioeconomic status in CHR). In line with the study setting, we include a suitable set of both time-variant and time-invariant control variables in our analysis. Details regarding the control variables are provided in Supplemental Appendix Section A.3, while descriptive statistics and correlations are presented in Supplemental Appendix Table A2.
Empirical Analysis
Testing Hypothesis 1
Panel Data Analysis
We estimate the effect of availability of telemedicine services on county-level health outcomes using the following panel data analysis with random effect model specification (Equation 1):

where Wit is the proportion of availability of telemedicine services for county i in year t, and the estimation of
The random effect model estimation results are presented in Table 1. The results indicate that increased availability of telemedicine services is negatively associated with overall health outcomes (M1: b = −.122; p < .05). Since this outcome variable is reverse coded, an increase in availability of telemedicine services is associated with improved overall health outcomes. Based on the marginal effect, one standard deviation increase in availability of telemedicine services is associated with 2.0% improvement in overall health outcomes. Increased availability of telemedicine services is also associated with reduced premature death rate (M2: b = −.048; p < .01) and preventable hospital stays (M3: b = −.073; p < .01). In addition, the results show that increased availability of telemedicine services is associated with reduced low birthweight rate (M4: b = −.042; p < .001), smoking rate (M5: b = −.068; p < .01), and need for diabetes monitoring (M6: b = −.105; p < .001). We repeat the panel data analysis with a fixed effect model specification and find the estimation results are largely consistent (see Table 2). In sum, we find empirical support for Hypothesis 1.
Random Effect Model Estimation Results For The Effect Of Availability Of Telemedicine Services On County-Level Health Outcomes.
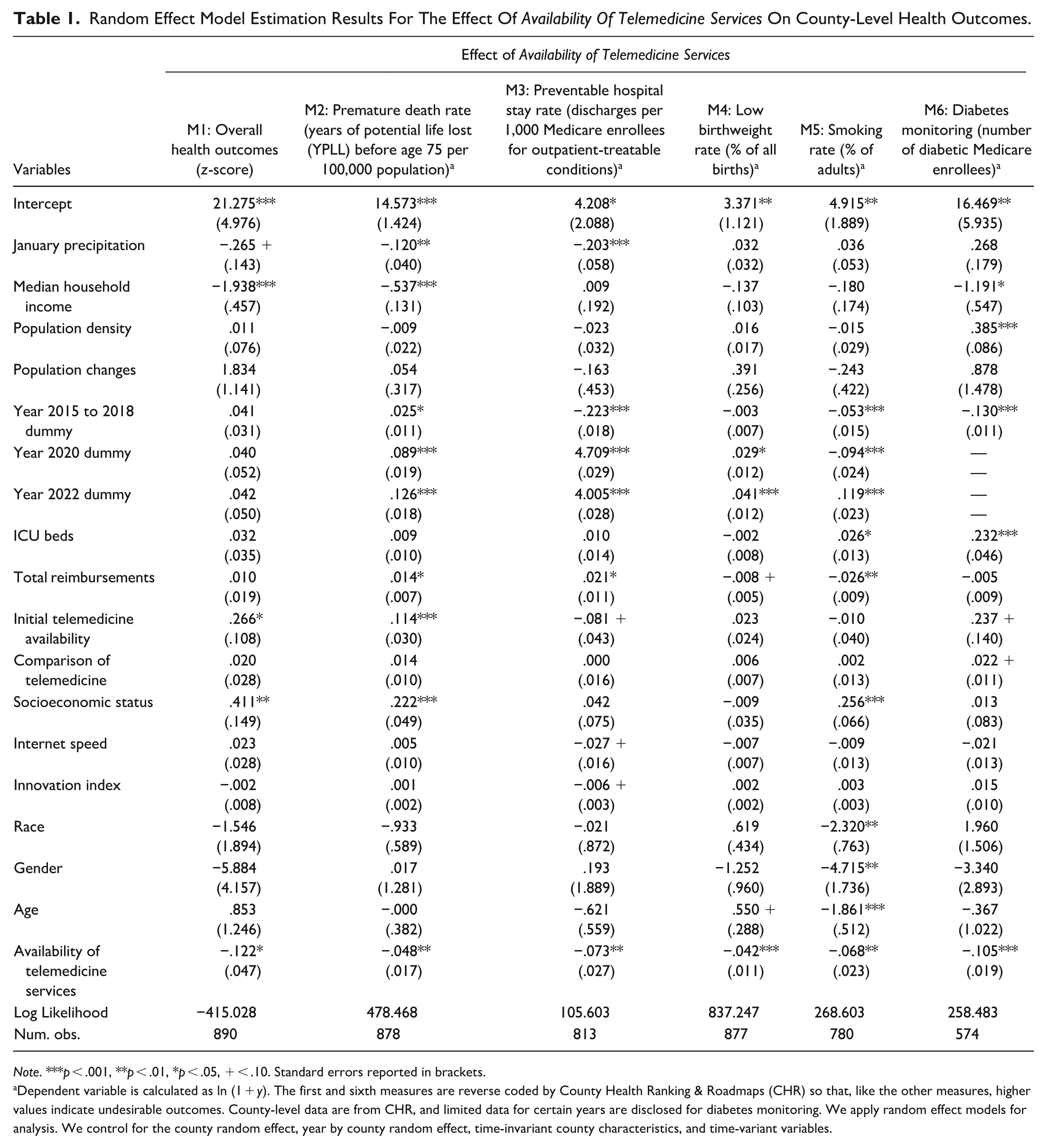
Note. ***p < .001, **p < .01, *p < .05, + < .10. Standard errors reported in brackets.
Dependent variable is calculated as ln (1 + y). The first and sixth measures are reverse coded by County Health Ranking & Roadmaps (CHR) so that, like the other measures, higher values indicate undesirable outcomes. County-level data are from CHR, and limited data for certain years are disclosed for diabetes monitoring. We apply random effect models for analysis. We control for the county random effect, year by county random effect, time-invariant county characteristics, and time-variant variables.
Fixed Effect Model Estimation Results For The Effect of Availability of Telemedicine Services on County-Level Health Outcomes.
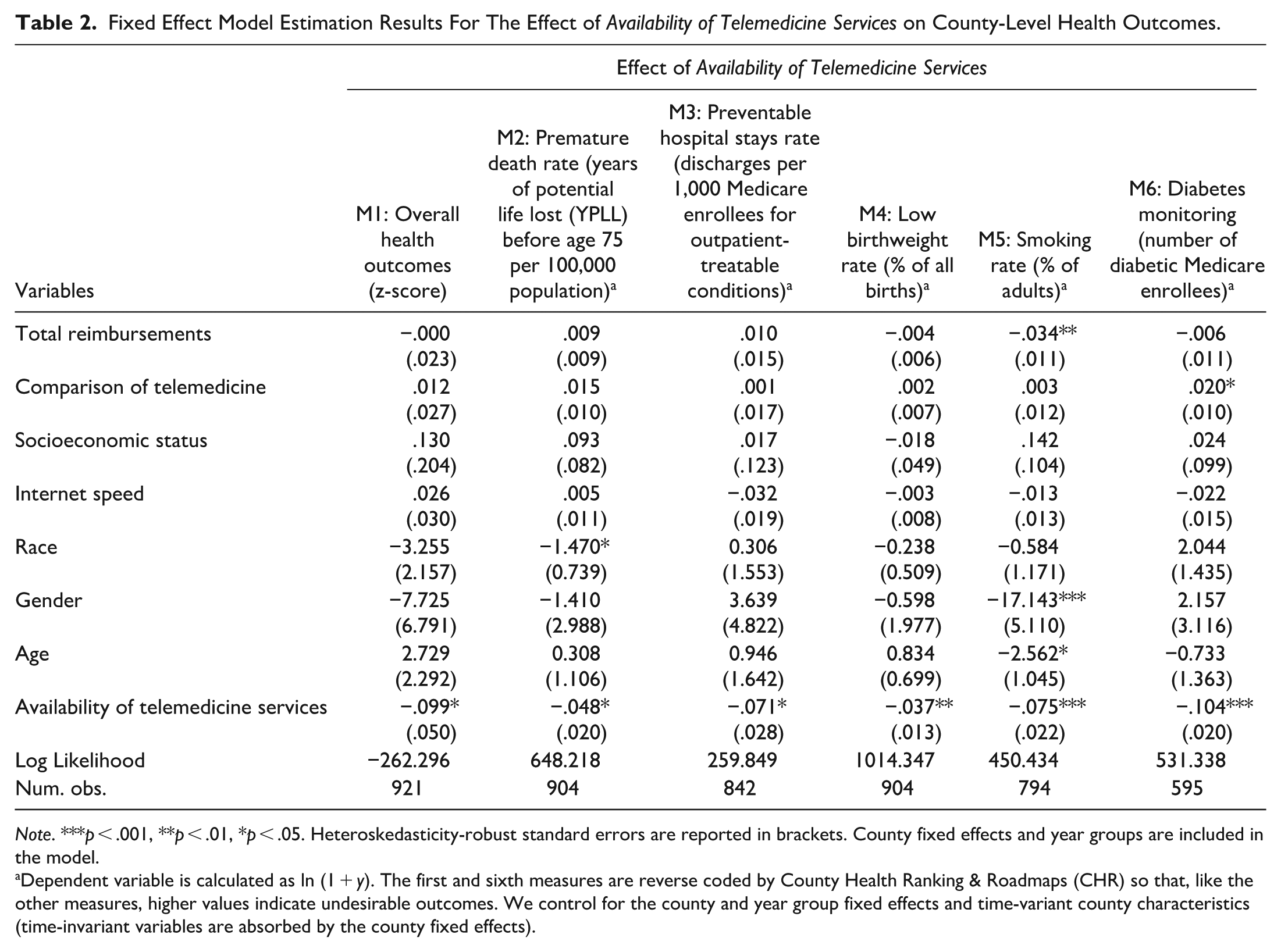
Note. ***p < .001, **p < .01, *p < .05. Heteroskedasticity-robust standard errors are reported in brackets. County fixed effects and year groups are included in the model.
Dependent variable is calculated as ln (1 + y). The first and sixth measures are reverse coded by County Health Ranking & Roadmaps (CHR) so that, like the other measures, higher values indicate undesirable outcomes. We control for the county and year group fixed effects and time-variant county characteristics (time-invariant variables are absorbed by the county fixed effects).
Robustness Checks
Causal estimation using GRF analysis
We conduct GRF analysis to obtain causal evidence in observational studies (Athey and Imbens 2019; Imbens and Rubin 2015). We implement this supervised matching learning method based on causal forest inference to examine the impact of availability of telemedicine services across counties, following Wager and Athey (2018). Extending the idea of a standard random forest (Breiman 2001), GRF estimates the effect based on an average of multiple trees/partitions using a random forest approach. This causal forest employs an “honest” estimation whereby the sample is randomly split into two subsamples, with one used to develop the trees/partitions and the other to make inference regarding the effect. GRF excels in providing estimates that are robust, consistent, and asymptotically normal. Recently, this method has been used to study the effect of information disclosure on payments to physicians in a healthcare setting (Guo, Sriram, and Manchanda 2021). We apply the GRF method to estimate the average partial effect because we have a continuous treatment variable. The effect estimation is derived from the full sample (see Supplemental Appendix B.1.1). As illustrated in Figure 3 and the average treatment effects in Supplemental Appendix Table B1, the GRF analysis supports the panel data analysis findings, showing that increased availability of telemedicine services in a county is positively associated with improved county-level health outcomes, including overall health outcomes, premature death rate, preventable hospital stays, low birthweight rate, smoking rate, and need for diabetes monitoring.
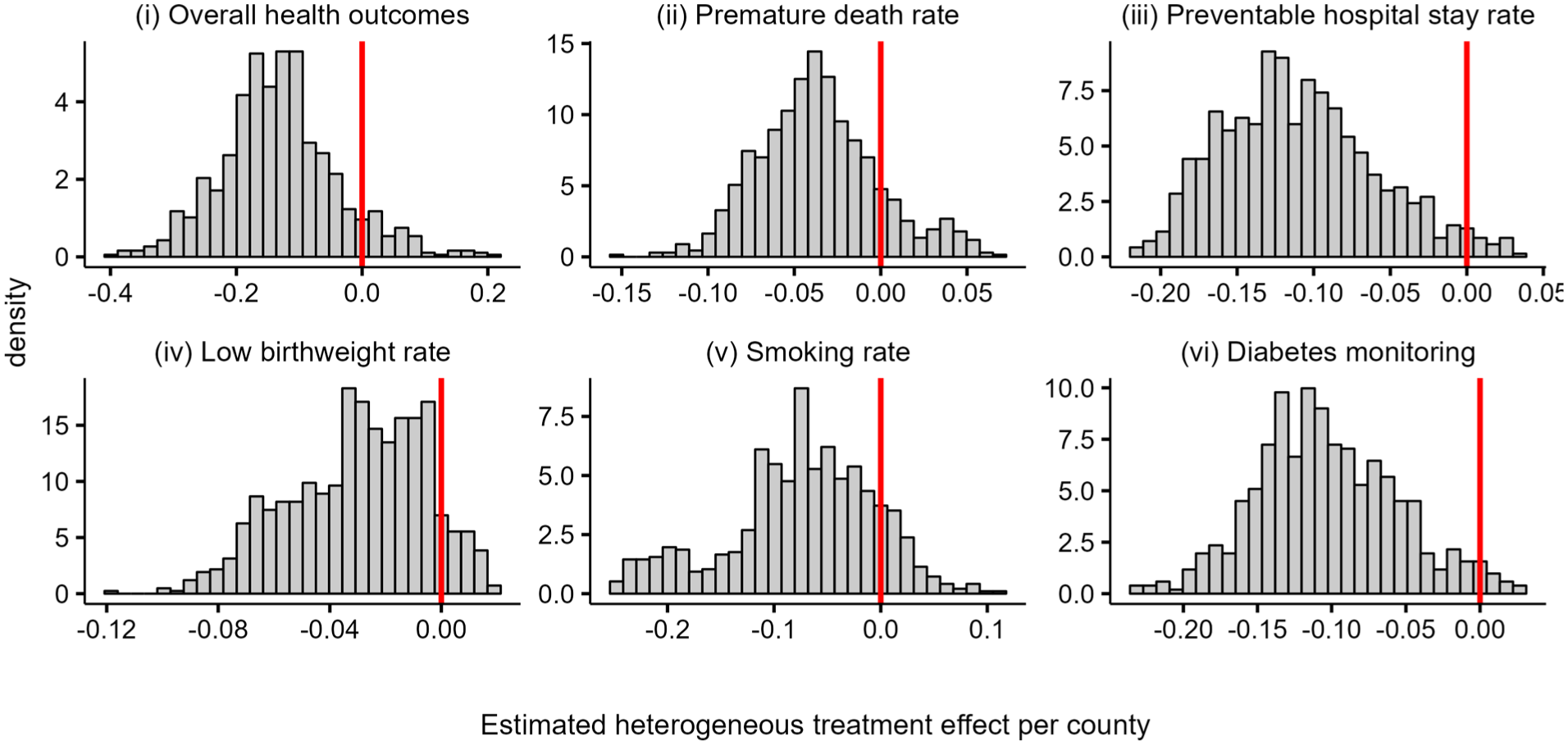
Estimated heterogeneous effects of availability of telemedicine services per county,
Lagged independent variable
The impact of telemedicine services may take time to be realized in community outcomes, so we test the sensitivity of our findings to time effects by replacing telemedicine with its 1-year lagged value. Table 3 presents the results, which indicate that lagged telemedicine remains significantly associated with the outcome variables, supporting the robustness of our findings.
Robustness Check: Lagged Independent Variable Using Random Effect Model Estimation Results For The Effect of Availability of Telemedicine Services on County-Level Health Outcomes.
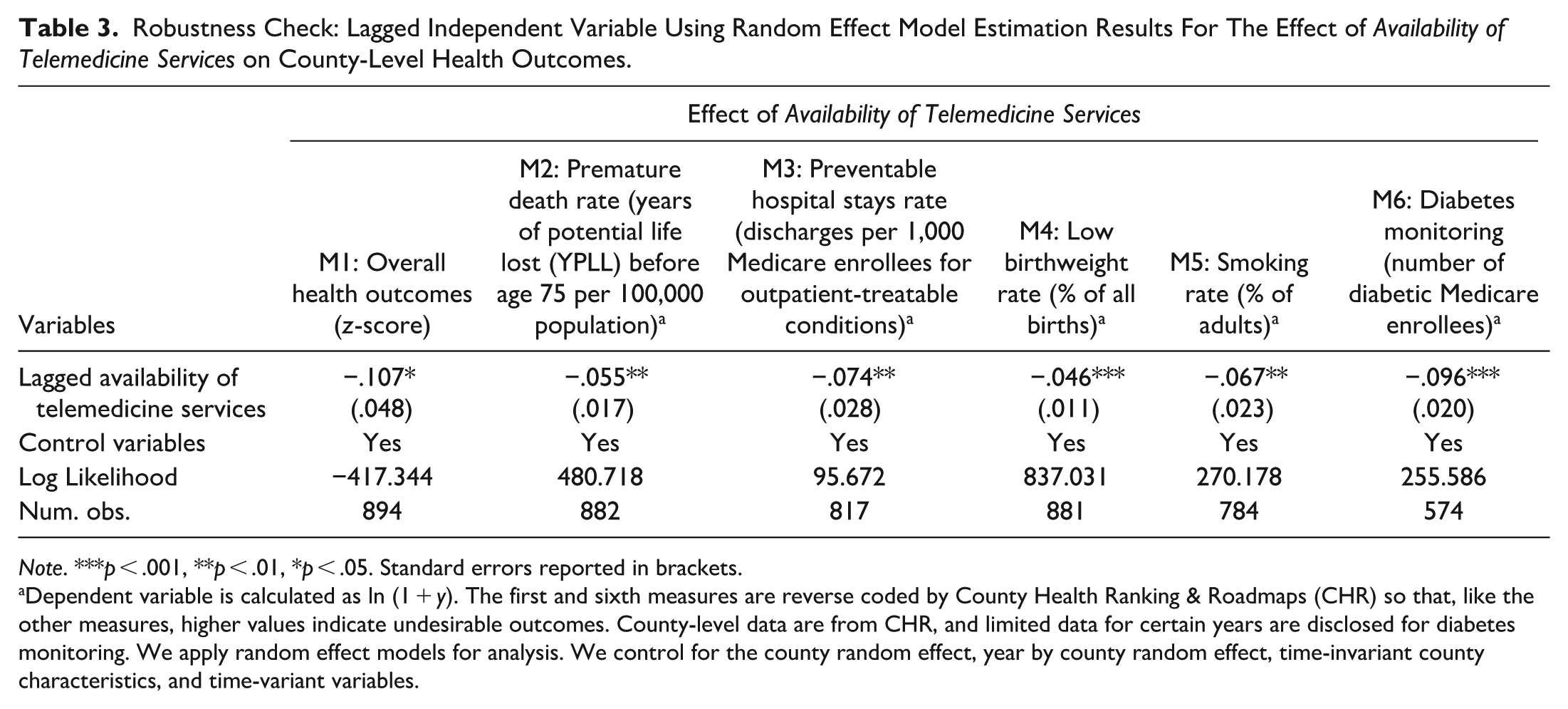
Note. ***p < .001, **p < .01, *p < .05. Standard errors reported in brackets.
Dependent variable is calculated as ln (1 + y). The first and sixth measures are reverse coded by County Health Ranking & Roadmaps (CHR) so that, like the other measures, higher values indicate undesirable outcomes. County-level data are from CHR, and limited data for certain years are disclosed for diabetes monitoring. We apply random effect models for analysis. We control for the county random effect, year by county random effect, time-invariant county characteristics, and time-variant variables.
Clinical care quality
Our estimates could be influenced by existing clinical care quality, as counties with better clinical care infrastructure may experience different telemedicine uptake patterns, or availability of telemedicine could reflect broader variations in local healthcare quality. Overlooking this could bias our results, as we might mistakenly attribute to telemedicine effects that are actually driven by underlying differences in clinical care quality. To address this, we incorporate a lagged county-level measure of clinical care quality obtained from CHR (https://www.countyhealthrankings.org/health-data/community-conditions/health-infrastructure/clinical-care). CHR defines clinical care as “anything relating to the direct medical treatment or testing of patients,” and emphasizes that care should be “accessible, timely, safe, effective and affordable, providing the right care for the right person at the right time.” This measure reflects access to physicians, mental health providers, dentists, insurance, and hospital stays for ambulatory-care sensitive conditions. It is operationalized as a reverse-coded z-score, with higher values indicating poorer quality. As shown in Table 4, controlling for clinical care quality does not materially alter the association between telemedicine services and health outcomes, alleviating concerns regarding the influence of clinical care quality on our results.
Robustness Check: Controlling for Clinical Care Quality Using Random Effect Model Estimation Results For the Effect of Availability of Telemedicine Services on County-Level Health Outcomes.
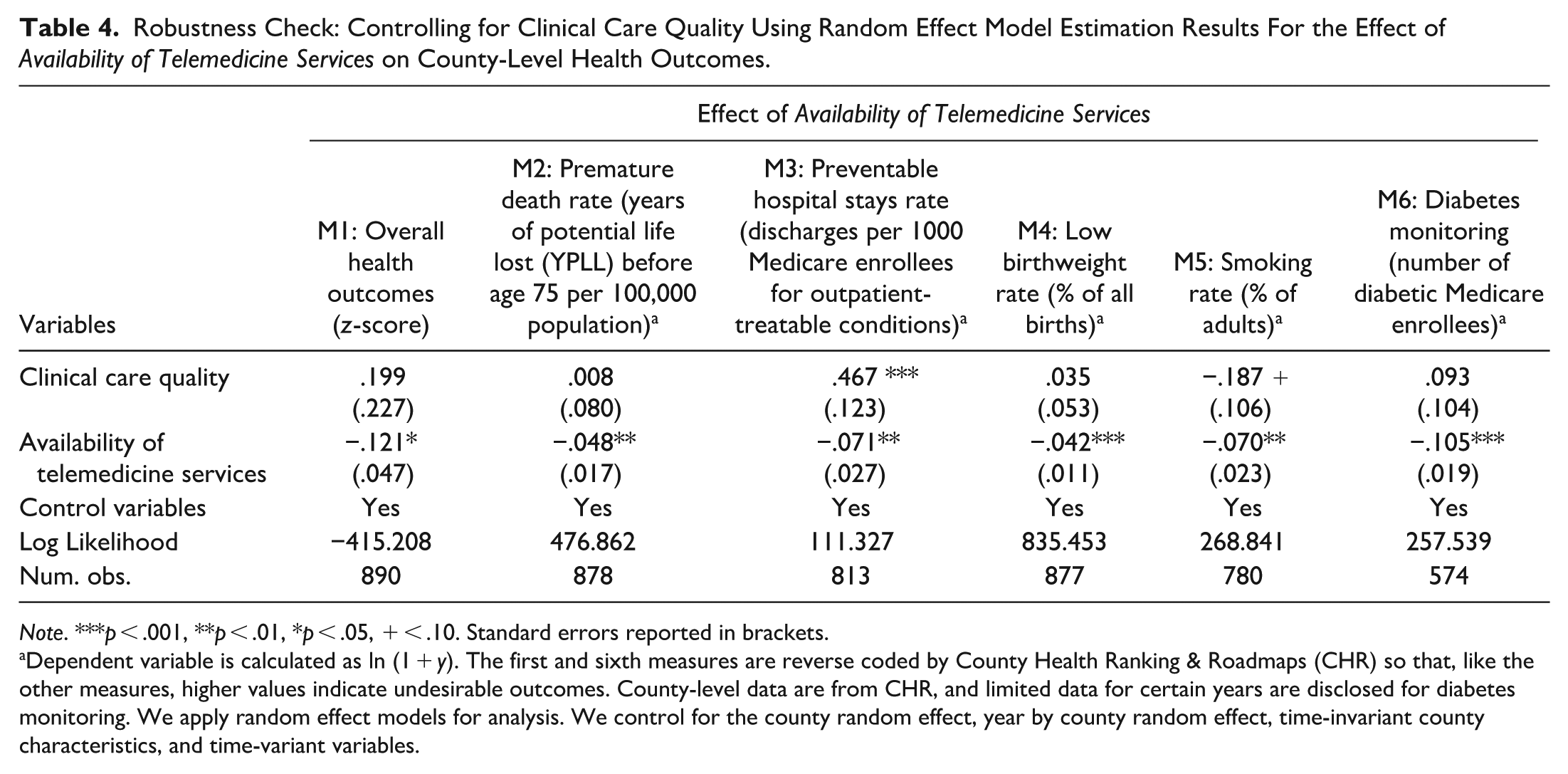
Note. ***p < .001, **p < .01, *p < .05, + < .10. Standard errors reported in brackets.
Dependent variable is calculated as ln (1 + y). The first and sixth measures are reverse coded by County Health Ranking & Roadmaps (CHR) so that, like the other measures, higher values indicate undesirable outcomes. County-level data are from CHR, and limited data for certain years are disclosed for diabetes monitoring. We apply random effect models for analysis. We control for the county random effect, year by county random effect, time-invariant county characteristics, and time-variant variables.
Additional analyses to assess robustness and generalizability
Specifically, we evaluate the results using (i) an alternative measure of availability of telemedicine services; (ii) alternative samples to account for incomplete responses from clinics and missing values; (iii) DID analysis incorporating variations in state telemedicine parity laws; (iv) a control for nearby counties; (v) instrumental variable and control function analysis; (vi) within sample DID analysis; and (vii) matching approaches (see Supplemental Appendix B.1.2). These analyses confirm the robustness of our findings across alternative measures and sample criteria, and support the generalizability and causal interpretation of the positive impact of availability of telemedicine services both within our sample and nationwide.
Testing Hypotheses 2, 3, 4, and 5
While increased availability of telemedicine services improves county-level health outcomes, as shown in our main analysis, we now examine heterogeneity in the impact of telemedicine services on health outcomes as it relates to county-level socioeconomic status, digital infrastructure (i.e., internet speed), innovation capacity, and demographics (i.e., race, gender, and age) as proposed in Hypotheses 2 to 5. The results of the analysis are reported in Table 5.
Contingency Effects: Heterogeneous Effects of Availability of Telemedicine Services on County-Level Health Outcomes Depending on County Socioeconomic Status, Digital Infrastructure, Innovation Capacity, and Demographics.
Panel A. County Socioeconomic Status, Digital Infrastructure, and Innovation Capacity.
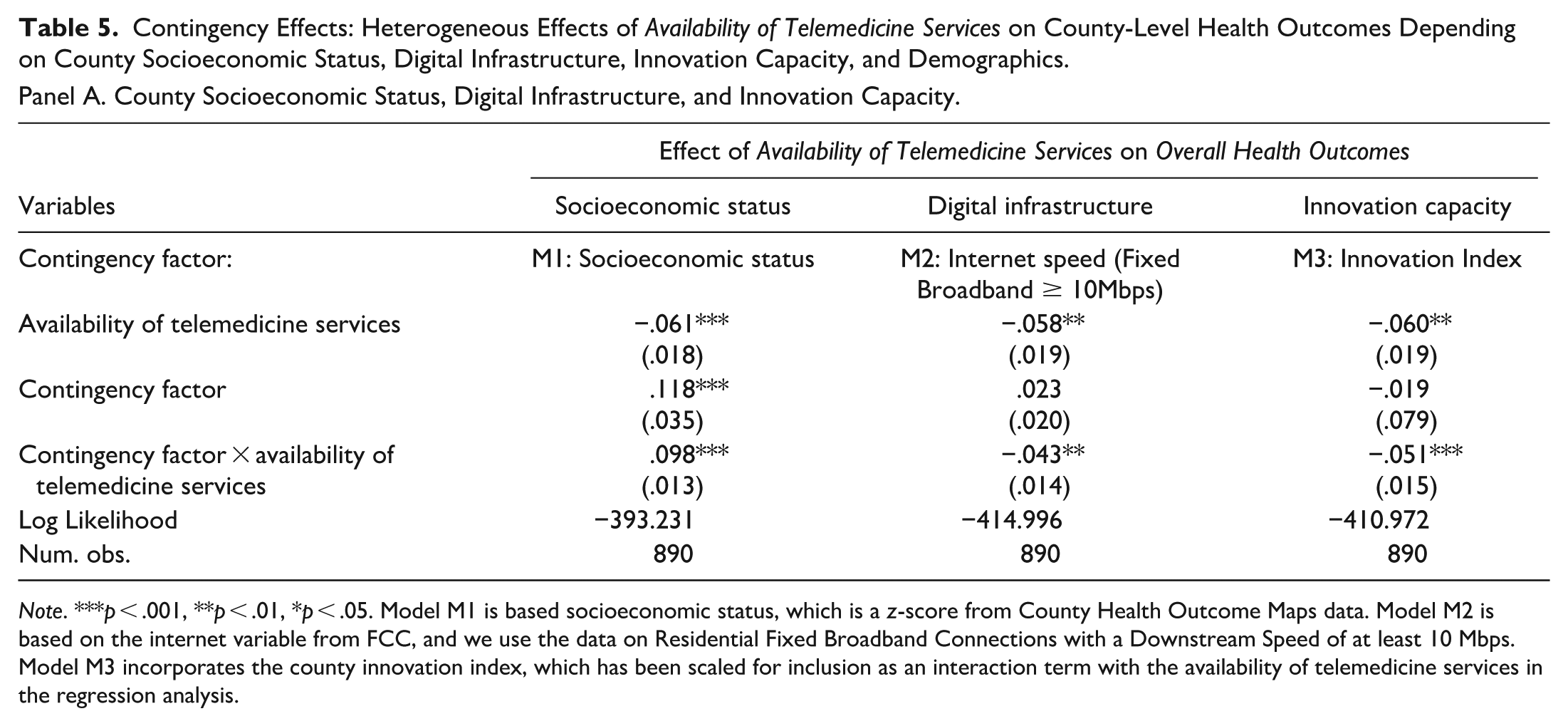
Note. ***p < .001, **p < .01, *p < .05. Model M1 is based socioeconomic status, which is a z-score from County Health Outcome Maps data. Model M2 is based on the internet variable from FCC, and we use the data on Residential Fixed Broadband Connections with a Downstream Speed of at least 10 Mbps. Model M3 incorporates the county innovation index, which has been scaled for inclusion as an interaction term with the availability of telemedicine services in the regression analysis.
Panel B. County Demographic Characteristics.
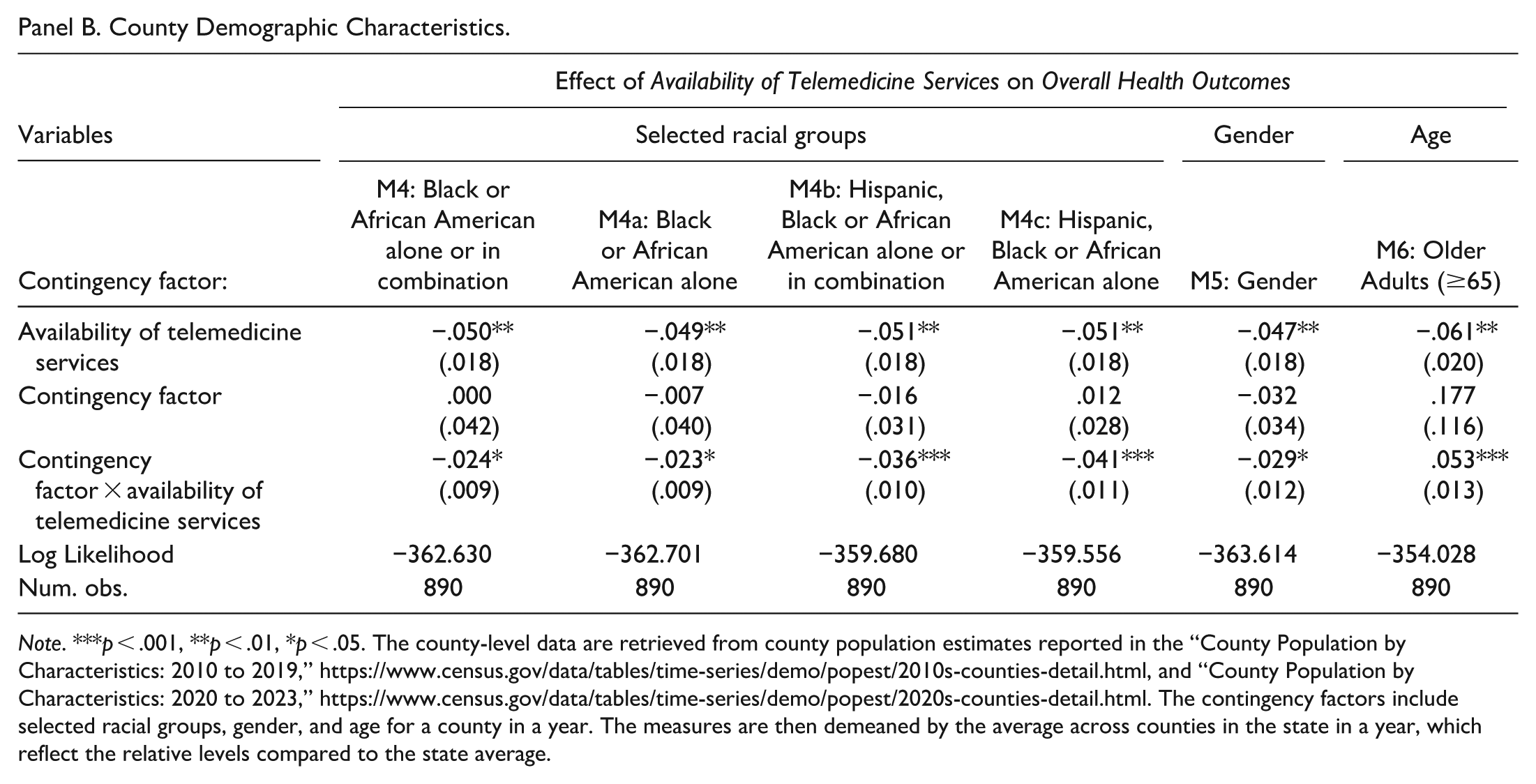
Note. ***p < .001, **p < .01, *p < .05. The county-level data are retrieved from county population estimates reported in the “County Population by Characteristics: 2010 to 2019,” https://www.census.gov/data/tables/time-series/demo/popest/2010s-counties-detail.html, and “County Population by Characteristics: 2020 to 2023,” https://www.census.gov/data/tables/time-series/demo/popest/2020s-counties-detail.html. The contingency factors include selected racial groups, gender, and age for a county in a year. The measures are then demeaned by the average across counties in the state in a year, which reflect the relative levels compared to the state average.
In Panel A of Table 5, the positive coefficient for the interaction term: socioeconomic status × availability of telemedicine services (M1: b = .098, p < .001) shows that lower socioeconomic status weakens the positive impact of increased availability of telemedicine services, lending support to Hypothesis 2. In essence, telemedicine services may not reach their full potential toward improving health outcomes for counties with low socioeconomic status.
In Panel A, negative coefficients for the interaction terms: internet speed × availability of telemedicine services (M2: b = −.043, p < .01), and innovation index × availability of telemedicine services (M3: b = −.051, p < .001) suggest that higher internet speed and greater innovation capacity in a county strengthen the positive impact of increased availability of telemedicine services, lending support to Hypotheses 3 and 4. Thus, superior digital infrastructure, evidenced by high internet speed, and greater innovation capacity enhance the enabling role of telemedicine services in improving county-level health outcomes.
In Panel B of Table 5, we observe that benefits from availability of telemedicine are greater when the proportion of the Black or African American sub-population is higher (M4: b = −.024, p < .05), and these results are robust across various US Census group designations for Black community members (M4a: b = −.023, p < .05; M4b: b = −.036, p < .001; M4c: b = −.041, p < .001). These results support Hypothesis 5a. Furthermore, we observe that counties with a higher proportion of females (gender) have better overall health outcomes as availability of telemedicine services increases (M5: b = −.029, p < .05), lending support to Hypothesis 5b. Finally, we find that counties with a higher proportion of older adults (age) have lower overall health outcomes as availability of telemedicine services increases (M6: b = .053, p < .001). This result lends support to Hypothesis 5c and suggests that telemedicine services are not likely to reach full potential in improving health outcomes in counties with high proportions of older adults. Possible explanations of this result include older adults’ limited adaptability to telemedicine services or the lack of telemedicine services tailored to their needs.
In summary, we find empirical support for heterogeneity in the positive impact of availability of telemedicine services on health outcomes across counties. Furthermore, we find that heterogeneity is explained by the moderating effects of socioeconomic status, digital infrastructure, innovation capacity, and demographics. We do not observe any negative impacts of telemedicine services on the set of studied health outcomes, alleviating concerns of potential unintended harms (Berry et al. 2022; Polonsky et al. 2024). The relationship between availability of telemedicine services and community health, and the moderating effects on this relationship, are captured in an integrated conceptual framework (i.e., Figure 1, shown earlier).
Post-hoc Analyses of Pandemic Timeframe
Pre- and mid-pandemic subgroup analysis
For this post-hoc analysis, we investigate whether the impact of availability of telemedicine services on overall health outcomes across counties changed during the COVID-19 pandemic. We assess the effect of availability of telemedicine services by splitting our sample into two subgroups: (i) pre-pandemic (2010–2018), and (ii) mid-pandemic (2020–2022). As shown in Supplemental Appendix B.1.3, Table B8, the main effects of availability of telemedicine services remain consistent across both subgroups, suggesting consistent impacts on overall health outcomes before and during the pandemic.
Cross-sectional analysis for COVID-19-related deaths
Furthermore, we examine how the availability of telemedicine services may have impacted community health during the COVID-19 pandemic by facilitating better coordination between in-person and remote virtual care. To that end, we construct a cross-sectional sample that incorporates pre-pandemic availability of telemedicine services data and pandemic mortality (i.e., COVID-19-related deaths). We collected data on COVID-19-related deaths compiled by The New York Times (2023) from state and local sources. We use reported daily deaths, which include both confirmed and probable deaths from COVID-19, to calculate the average number of daily deaths in each county 2020 to 2022. For pre-pandemic availability of telemedicine services and other control variables, we compute the average value across the years 2010 to 2018 for each county. For robustness checks, we develop two alternative measures for COVID-19-related deaths: (i) rolling averaged daily deaths, representing county-level daily deaths averaged over a 30-day period, and (ii) rolling averaged daily deaths per 100,000 county residents. We also conduct robustness checks for the time effects of the measure of daily deaths, exploring different time windows, using the year 2020 only, and the years 2020 to 2021.
Table 6 presents the results of post-hoc regression analysis examining the impact of pre-pandemic availability of telemedicine services on COVID-19-related deaths and its implications for contingency factors. In Model 1, the significant and negative coefficient estimation (M1: b = −.052, p < .01) suggests that higher pre-pandemic availability of telemedicine services is associated with a reduction in new daily COVID-19-related deaths. Calculating the corresponding marginal effect reveals that predicted new daily deaths decrease from 0.155 to 0.101 when pre-pandemic availability of telemedicine services increases by one standard deviation (mean + SD = 0.470 + 0.192 = 0.662). This predicted marginal effect indicates a 36.9% reduction in deaths. This finding is robust when considering alternative measures of COVID-19-related deaths (see Models M2 and M3) and different time windows (see Models M4 and M5).
Pre-pandemic Telemedicine Services and COVID-19-Related Deaths: Cross Sectional Estimation Results for the Effect of Availability of Telemedicine Services on County-Level COVID-19-Related Deaths.
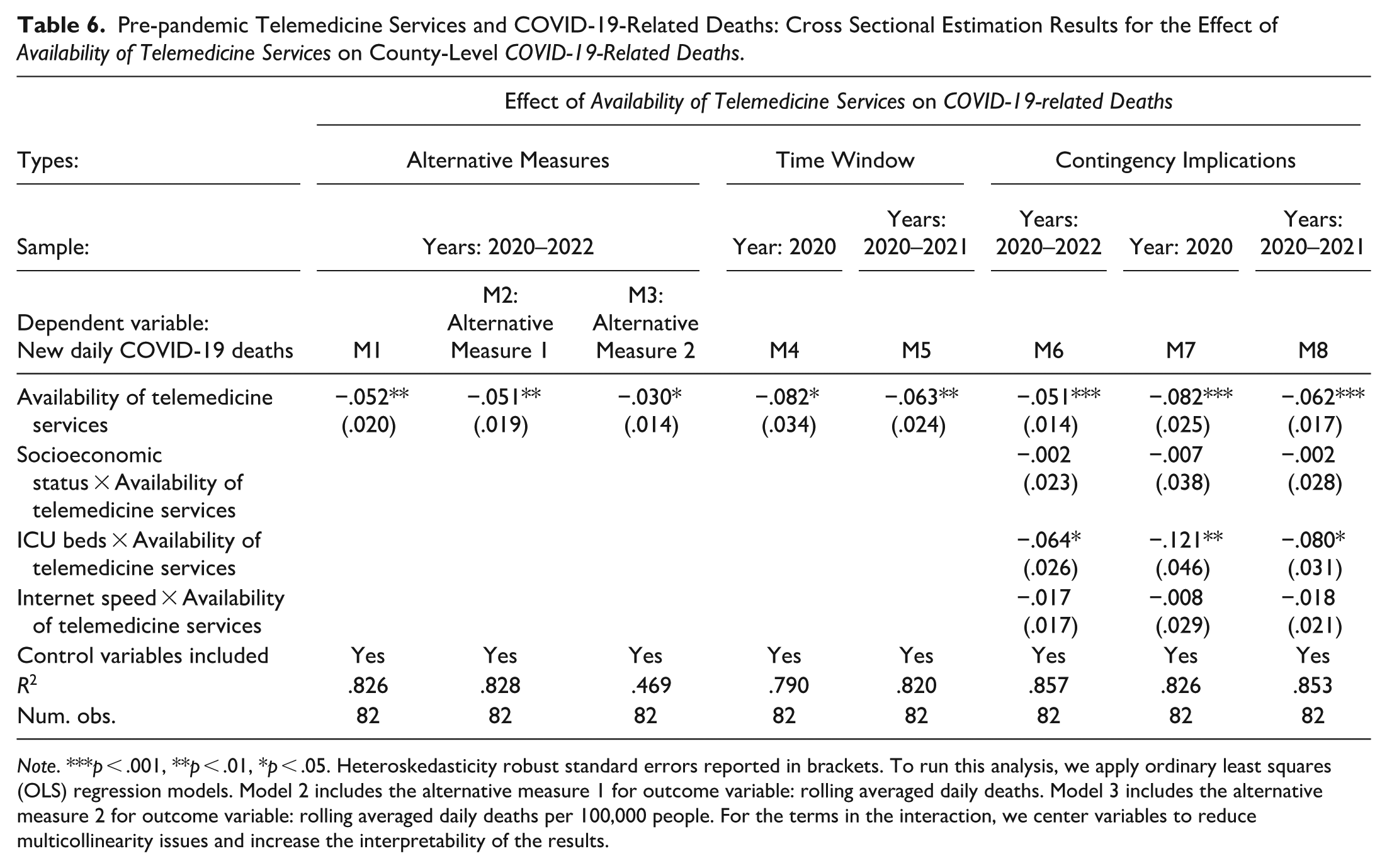
Note. ***p < .001, **p < .01, *p < .05. Heteroskedasticity robust standard errors reported in brackets. To run this analysis, we apply ordinary least squares (OLS) regression models. Model 2 includes the alternative measure 1 for outcome variable: rolling averaged daily deaths. Model 3 includes the alternative measure 2 for outcome variable: rolling averaged daily deaths per 100,000 people. For the terms in the interaction, we center variables to reduce multicollinearity issues and increase the interpretability of the results.
We also assess implications of three contingency factors: (i) socioeconomic status, with higher values indicating worse socioeconomic status; (ii) number of ICU beds, with higher values indicating greater need for hospitalized patient care (Janke et al. 2021); and (iii) internet speed, with higher values indicating superior digital infrastructure. In Model M6, we report the results for these interactions with new daily COVID-19-related deaths from 2020 to 2022. The results show that availability of telemedicine services plays a more substantial role in reducing deaths in counties with more ICU beds (M6: b = −.064, p < .05), while its impact is not significant in counties with lower socioeconomic status or superior digital infrastructure. These results are consistent across different time windows in Models M7 and M8.
Conclusion
Telemedicine services leverage ICTs toward innovating and enabling the delivery of healthcare, overcoming geographical barriers by connecting patients with healthcare providers located at distant sites. Our study is motivated by an acknowledgment in academic and practitioner literature that telemedicine services are a powerful driver of service innovation with the potential to improve community health. While previous studies have explored the drivers of telemedicine adoption and utilization, and associated outcomes at the patient, specialty, or hospital levels, the findings of our theoretically grounded empirical inquiry indicating that availability of telemedicine services improves community health are a significant contribution toward advancing service literature (cf. Berry et al. 2022; Berry, Yadav, and Hole 2024; Ostrom et al. 2015; Ostrom et al. 2021).
Our empirical analysis of county-level panel data indicates that availability of telemedicine services improves health outcomes, reflecting enhanced community health central to the well-being of a community. These improvements are both in aggregate—that is, overall health outcomes—as well as along specific dimensions of reductions in premature death rate, low birthweight rate, preventable hospital stays, smoking rate, and the need for diabetes monitoring. Analysis of relevant data shows that greater availability of telemedicine services was associated with decreased COVID-19-related mortality during the pandemic.
Investigating heterogeneity in the impact of telemedicine services reveals that county contextual factors play a role in the measured health outcomes. Specifically, we find that while lower socioeconomic status reduces the effectiveness of telemedicine services, better digital infrastructure and greater regional innovation capacity enhance effectiveness. Higher proportions of Black and female community members enhance the effectiveness of telemedicine services, whereas a higher proportion of older adults reduces effectiveness. Our study findings, taken together, provide empirical support for the potential of telemedicine services in improving community health while recognizing the importance of the moderating effects of contextual factors in realizing the potential.
Contributions
This study is among the very first to expand on the scope of earlier studies showing individual, clinic, or hospital benefits from telemedicine services by investigating their broad-scale impact on health outcomes at the county level. The empirical findings here, taken together, along with the proposed framework (Figure 1), contribute toward advancing the service literature by underscoring the potential for leveraging ICTs—specifically, clinic-based telemedicine services—for improving community health (Anderson and Ostrom 2015; Berry et al. 2022; Berry, Yadav, and Hole 2024; Ostrom et al. 2021). Our study responds to prior calls to revisit and investigate health and safety programs through a CBA (e.g., Aljafari et al. 2024; Bell, Lee, and Gruca 2024; Farmer et al. 2001; Nilsen 2006), and extends stakeholder theory by documenting broad community-wide health benefits from the availability of telemedicine, an ICT-based service innovation (Freeman 1984).
Our study sheds light on an augmented seamless-coordination framework of service innovation by showing how availability of telemedicine services, both directly and indirectly, drive community-wide value configurations and resource integration (Go Jefferies, Bishop, and Hibbert 2021). Telemedicine services amplify the value co-creation through the enhanced connectivity of clinics within healthcare, thus deepening the understanding of frontline service contexts (Makridis and Mishra 2022; Vargo and Lusch 2008). Increased availability of telemedicine services at a clinic facilitates the integration of diverse expertise across providers and incorporates patient-generated inputs through digital platforms, enhancing the application of knowledge in regions. This convergence pushes healthcare closer to a pure service economy, seamlessly merging remote expertise with local delivery to create system-wide synergies, reflecting the idea that “the whole is greater than the sum of its parts” (Antons and Breidbach 2018, p. 17).
By engaging patients as both customers and co-creators, telemedicine services nurture relational, customer-centric exchanges that underpin sustainable community health (Berry, Yadav, and Hole 2024). Patients actively shape care processes in setting goals, managing treatments, and personalizing care routines, especially in chronic care contexts. Their participation also extends to scheduling, self-monitoring, digital communication, and assuming greater autonomy and control over their care. These practices exemplify patient-driven value co-creation and adaptive service innovation, aligning with Go Jefferies, Bishop, and Hibbert (2021).
Moreover, telemedicine acts as a network-of-networks resource integrator (Vargo and Lusch 2008), linking clinics, patients, insurers, and community organizations for value co-creation at individual, organizational, and population levels. As “healthcare is an elementary service that applies to every individual” in a community (Aljafari et al. 2024, p. 1346), our county-level findings demonstrate how seamless ICT-enabled coordination via telemedicine generates, delivers, and disseminates collective health benefits at scale to entire communities.
At a more nuanced level, our findings reveal the heterogeneous impact of telemedicine services on county-level health outcomes, contingent on socioeconomic status, digital infrastructure, innovation capacity, and demographics of counties. Telemedicine alone cannot directly bridge structural disparities; however, we find that it yields greater benefits in counties with robust digital infrastructure, strong innovation capacity, and higher proportions of Black and female residents, whereas lower-resource areas experience diminished or mixed effects. These heterogeneous effects highlight the importance of context in ICT-enabled service innovations (Aljafari et al. 2024; Castrogiovanni 1991), especially in domains like health and safety programs typically assessed at a community level (Nilsen 2006). Strategically adapting telemedicine delivery to local conditions can help address multi-stakeholder needs and ensure sustainable, high-quality care for all community stakeholders (Freeman 1984; Huang et al. 2021; Keiningham, Aksoy, and Malthouse 2024).
Practical Implications
To put the practical implications of this study into perspective, the following background information is relevant. Data on the use of telemedicine services in the United States can be traced back to 2005, starting with 0.02 visits per 1000 persons and rising to 6.57 visits per 1000 persons in 2017 (Barnett et al. 2018). During the COVID-19 pandemic, the use of telemedicine services experienced steep and unanticipated growth, with 40% of surveyed US consumers planning to use telehealth and telemedicine services in the future (Bestsennyy et al. 2021; Dudley and Sung 2020; Hollander and Carr 2020; Rotenstein and Friedman 2020). Specifically, the COVID-19 period demonstrated the potential of telemedicine services to: (i) deliver care at scale— that is, at a community level (Bestsennyy et al. 2021, p. 13)—and (ii) improve equity and access to care (Smith 2022) leading US state governments to seek verification if such potential can indeed be realized during the post-COVID-19 period (cf. MDH 2024). The practical implications of our study include verifying such potential by empirically demonstrating that availability of telemedicine services improve community health, both in aggregate as well as along specific dimensions. By empirically evaluating the moderating effects of socioeconomic status, digital infrastructure (internet speed), innovation capacity, and demographics (race, gender and age), we highlight equity and access to care issues and show that telemedicine’s impact varies across contexts, supporting its potential to reduce health disparities when adapted to local conditions.
These practical implications of our study are both consequential and of contemporary interest. Specifically, health centers in the South region and in rural geographies of the United States have disproportionately fewer telehealth visits (as a percentage of all visits) than their counterparts in the Midwest, Northeast, and West regions and urban geographies, respectively (Demeke et al. 2021). Also, reviewing state-level telemedicine laws and reimbursement policies (pre-COVID-19, to coincide with our data collection period), we find that: (i) all 50 states and Washington DC had some form of Medicaid reimbursement for telemedicine services; and (ii) Minnesota and 39 other states had regulation governing telemedicine service reimbursement by private payers (CCHP 2019, p. 2,19). Thus, our study findings have practical implications by way of being relevant and generalizable to other states and regions because the regulatory context of telemedicine services in Minnesota is comparable to many other US states.
Limitations and Directions of Future Research
Our study has several limitations that provide avenues for future research. First, using more granular data, such as medical specialties, patient conditions, and cost and quality of care, could clarify contextual factors, reduce confounding, and enable our understanding of telemedicine’s dynamic, long-term effects. Second, future research should examine how telemedicine services evolve with ICTs and artificial intelligence, incorporating the role of personal technologies like smartphones and wearables, as well as the dynamics of human versus automated social presence for healthcare communication. Third, additional perspectives on health outcomes, such as patient satisfaction and affordability, are necessary to fully understand the impact of the enabling role of ICTs in improving the delivery of telemedicine services to communities. While our study focused on community health, examining the behavior of individual patients in using telemedicine services can provide a complementary perspective. Fourth, as we primarily rely on geographic units based on counties to define community, future research could analyze non‑geographic communities, such as professional networks or groups formed around shared interests or activities, for additional insights. Deeper theoretical work is needed to bridge gaps between access and quality in healthcare, and between health outcomes and overall well-being, while extending community and stakeholder perspectives. Fifth, with healthcare being a bundle of services, goods, and experiences involving many stakeholders, more research is warranted to further uncover the interactions among the development, adoption, and implementation of ICTs, along with care provider knowledge and equity in care delivery. Finally, given that when it comes to “leveraging technology to advance services” (Ostrom et al. 2015, pp. 143-44), similarities have been acknowledged between telemedicine services for non-urgent care and online banking services (Carenet Health 2020); hence, the generalizability of the conceptual framework proposed in this study should be examined in the context of other service sectors such as to evaluate the community implications of online banking services.
Supplemental Material
sj-docx-1-jsr-10.1177_10946705261417849 – Supplemental material for Evaluating the Impact of Telemedicine Services on Community Health: A County-Level Analysis
Supplemental material, sj-docx-1-jsr-10.1177_10946705261417849 for Evaluating the Impact of Telemedicine Services on Community Health: A County-Level Analysis by Xiaojin Liu, Susan Meyer Goldstein, Kingshuk K. Sinha and Karen Soderberg in Journal of Service Research
Footnotes
Acknowledgements
We gratefully acknowledge the constructive, clear, and insightful developmental comments from the Editor-in-Chief, Co-Editors, anonymous Associate Editor, and three anonymous reviewers, which substantially improved this manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.