
Abstract

Tanya is an infant toddler developmental specialist who has been working in the field for 5 years. She recently was asked to work with a Filipino-American family, the Capunos, to provide weekly early intervention (EI) services for their son David. David is a 27-month-old boy whose Individualized Family Service Plan indicates the need for support in the areas of communication and social interaction. David is the youngest child of the three Capuno children and the only son. At the first visit, Tanya asks the family about David’s favorite activities, the family’s typical day and week, and what their concerns are for David. Mrs. Capuno shares that she stays home with David and Chesa, her younger daughter, whereas her older daughter Angel attends first grade. Mr. Capuno works 6 days per week with a rotating day off at a local office supply store. Mrs. Capuno, David, and Chesa walk Angel to school each morning and pick her up each afternoon. David enjoys riding in a stroller during these walks and often jabbers and points at people and cars along the way. Mr. Capuno smiles when he describes how absorbed David becomes in rolling his toy trucks around the kitchen. He also tells Tanya that he would like for David to talk more because he only says the words Mama and no. Mrs. Capuno says that she would like for David to play more nicely with his sisters, and Tanya observes David hitting and biting his sisters and parents when he is frustrated. Both parents tell Tanya that they have noticed that David is often more aggressive in the morning and when he is tired. When Tanya asks about David’s sleeping habits, Mrs. Capuno shares that David sleeps in the bed with them because he does not fall asleep well by himself.
Tanya asks the Capuno family which concerns they feel are the most important and should be addressed first. Mr. and Mrs. Capuno agree that they would like David to be less aggressive and use more words to communicate with them. Tanya thinks about strategies that have worked with other families experiencing similar concerns. She suggests to the Capunos that they make it difficult for David to access his juice cup and a favorite toy truck, to provide opportunities for him to ask for it. She also suggests that because David is more aggressive when tired, the family could develop a set bedtime and nightly routine for David and be firm in enforcing it. One other recommendation that Tanya makes is to remove David to a quiet location when he hits or bites and praise appropriate interactions with his sisters. The Capunos thank Tanya for her suggestion, and Tanya leaves the family feeling pleased with the visit. When Tanya calls to confirm the next visit, Mrs. Capuno says that they are very busy and she would like to reschedule. For the next few weeks, the same thing happens. Tanya is puzzled. What went wrong?
In the above vignette, Tanya is trying to implement family-centered EI services with the Capuno family. Family-centered practice has long been recognized as the preferred method of delivery for EI services for infants and toddlers who have or are at risk of having disabilities. These services stress the importance of the family in service provision; emphasize the family as decision makers regarding EI services; respect the culture, beliefs, customs, and values of families; and encourage service provision in the natural environment (Crais, Roy, & Free, 2006; Sylva, 2005). The natural environment includes any setting and activities in which a child would participate if they did not have disabilities, including the homes of family members, day care, faith-based settings, and parks or other leisure settings (Sylva, 2005). While Tanya met with the family in their home, she engaged in a discussion of the family’s routines and desired needs to identify the areas in which the family perceived they needed support. She offered recommendations to the family that she believed addressed the concerns they had shared with her. However, as can be seen by the Capuno family response, Tanya’s visit was not perceived as positively by the family as she believed it to be. Tanya failed to consider the cultural context of the family, which may have led to her difficulties in being invited back to the Capuno home.
The population of children and families receiving EI services is increasingly diverse, making it likely that service providers will work with families from cultures other than their own (Durand, 2010; Withrow, 2008). Culture has been defined as beliefs, traditions, activities, and practices that may be shared by members of a community (Rogoff, 2003) and more simply, as a worldview that helps us make sense of what we know (Kalyanpur & Harry, 1997). As culture often guides or influences the activities, routines, beliefs, and expectations of families, it is critical that EI service providers demonstrate cultural responsiveness when working with families to provide effective EI services. Culturally responsive professionals are able to facilitate positive interactions and provide effective services for these culturally diverse children and families (Sareen, Russ, Visencio, and Halfon (2004). However, as demonstrated in the opening vignette, providers can sometimes not recognize the importance of, or feel unsure about, how to provide culturally responsive services to families from cultures different from their own (Lee, Ostrosky, Bennett, & Fowler, 2003).
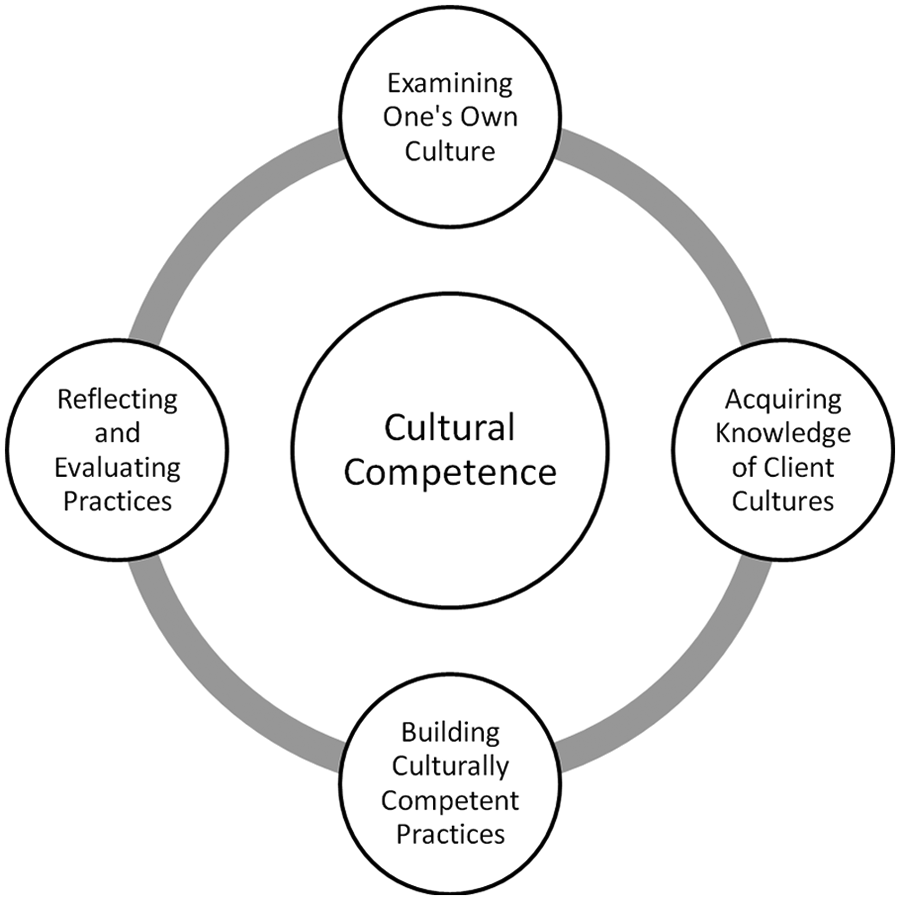
The purpose of this article is to provide a framework that offers a way for EI service providers to better meet the needs of the culturally diverse children and families they serve. This framework was created to organize existing research and literature on cultural responsiveness in a way that fit the unique context of EI. The framework draws from multiple fields of study, including early childhood, multicultural, and special education, as well as psychology and speech-language pathology, and synthesizes knowledge and best practices into four guiding principles (Figure 1). Each principle ties together correspondent themes and ideas from multiple fields, and suggests knowledge and best practices that can be utilized to increase one’s cultural responsiveness when working with families. For example, the first principle, Examining One’s Own Culture, is grounded in findings and recommendations from experts in the fields of early childhood and special education who have all emphasized the importance of self-study in development of cultural responsiveness. The opening vignette will be used to illustrate each of the principles and how they tie into Tanya’s practice.
Framework for Providing Culturally Responsive Early Intervention Services
The first principle, Examining One’s Own Culture, encourages EI providers to take an in-depth look at their own cultural values and beliefs. The second principle, Acquiring Knowledge of Family Cultures, highlights the importance of finding out about the cultures of the families that they serve. These first two principles are foundations for the third, Building Culturally Responsive Practices. This principle actively engages the provider in developing and implementing culturally responsive practices that respond to the unique strengths, needs, and desires of families. Finally, the fourth principle, Reflecting and Evaluating Practices, encourages EI service providers to reflect often on their practices to identify their most and least effective practices with families of cultures different from their own.
Examining One’s Own Culture
Everyone views the world through a cultural lens, often without realizing that they are doing so (Kalyanpur & Harry, 1997). This has been likened to a fish being unaware of the water in which it swims (Rogoff, 2003). Often, members of the dominant culture find it difficult to identify their culture because it is so pervasive that it is considered the “norm” (Durand, 2010; Rogoff, 2003). Many providers assume their beliefs and practices are correct and applicable to all children. Thus, examination of one’s own culture is a critical component of providing culturally responsive services through recognition of how his or her own culture plays into his or her professional perceptions and practices (Durand, 2010; Rogoff, 2003).
“Many providers assume their beliefs and practices are correct and applicable to all children.”
Several areas in which providers should examine their own beliefs in the context of their service provision have been identified. One area concerns individual beliefs about the range considered “normal” for child development and beliefs about correcting and accepting “abnormal” behaviors (Harry, 1992). Another area on which providers should reflect is their views about what constitutes a family, including roles of family responsibility and how enmeshed or disengaged family members should be with each other (Harry, 1992). Closely related to beliefs about family are provider beliefs about parenting style and what comprises good parenting (Harry, 1992).
Providers need to be aware that their values and beliefs regarding families, child development, and desired outcomes are shaped by their culture (Lynch & Hanson, 2011). By taking time to examine their beliefs about these concepts, providers will be able to more effectively identify how their cultural beliefs impact their professional practice (Kalyanpur & Harry, 1997; Withrow, 2008). One way to accomplish this is through self-questioning (Kalyanpur & Harry, 1997). For example, a provider may ask, “What do I believe are the roles of a father?” or “Why do I believe that children should be making choices about what they want to eat?” These questions can help identify underlying cultural beliefs and assumptions held by providers. Some question prompts are provided in Table 1 that can assist the EI providers in beginning to examine their own culture.
Questions to Consider During Cultural Self-Examination
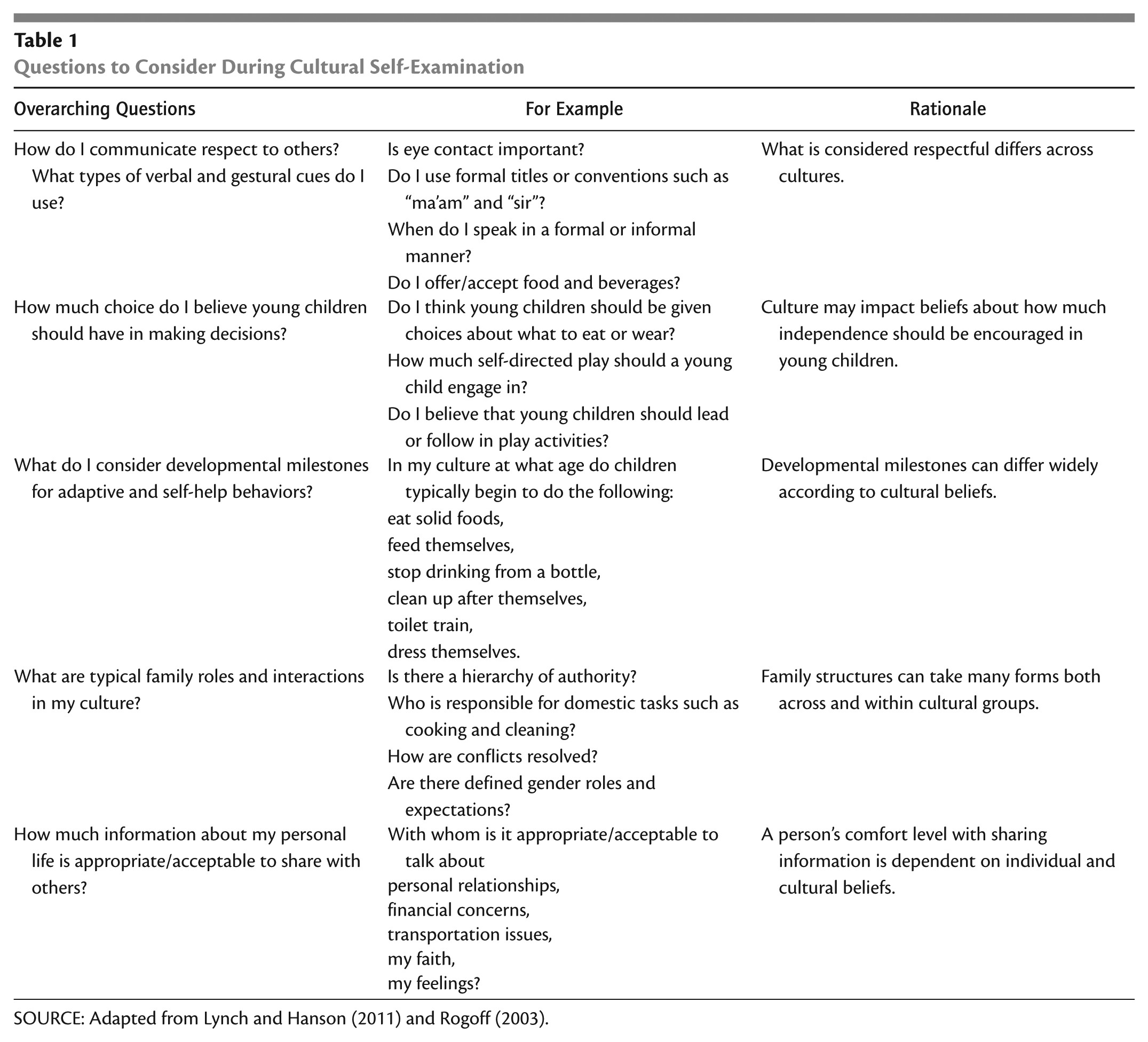
SOURCE: Adapted from Lynch and Hanson (2011) and Rogoff (2003).
Revisiting Tanya and the Capuno Family: What Went Wrong?
Tanya did not recognize that her personal values and beliefs were shaping the way she approached the Capuno family. She made recommendations for David’s sleeping routine based on her beliefs about what constituted “normal” sleep behaviors. Although Tanya spent time asking the family about their areas of concern, she made recommendations for dealing with these concerns that were rooted in her personal beliefs about the capabilities and interactions that should be exhibited by a toddler. She did not consider that strategies that work for some families may not be a good fit with the cultural values and beliefs of others.
Acquiring Knowledge of Family Cultures
Family-centered EI services are rooted in the knowledge that infants and toddlers with disabilities are best helped when their family is empowered to actively participate in decision making (Withrow, 2008). To do so, service providers need to acquire knowledge of the cultural beliefs and practices valued by the families they serve (Lynch & Hanson, 2011; Puig, 2010). This knowledge will contribute to identification and development of services that are in harmony with the beliefs and values of families. However, it is important to realize that cultural beliefs cannot be assumed based on membership in a single cultural category (Harry, 2002). Each family has a different context influenced by many factors that contribute to the unique cultural beliefs of families, including ethnicity, race, social class, nationality, geographical location, language, age, and professional or personal interest group membership (Harry, 2002).
It is particularly important that EI providers consider the context in which families understand disability. Cross-cultural research has shown that beliefs about the causes of disability differ among cultural groups (Harry, 2002; Lynch & Hanson, 2011). For example, some Asian and Hispanic cultural groups believe that disability has supernatural causes and is either a retribution or reward for past actions (Glover & Blankenship, 2007; Harry, 2002). In turn, these beliefs may affect a family’s feelings about intervention services intended to lessen the effects of a disability (Lynch & Hanson, 2011; Puig, 2010).
Culture can also affect the way that families perceive the presence and effect of disabilities (Olivos, Gallagher, & Aguilar, 2010; Rogoff, 2003). The developmental ages at which children are expected to demonstrate specific skills and behaviors vary widely across cultural groups, as does the emphasis placed on specific skills and behaviors (Lynch & Hanson, 2011; Rogoff, 2003). For instance, small children are commonly encouraged to contribute to conversations with adults and peers in European American families, in contrast to the value placed on silence and restraint in children of many Native American cultural communities (Rogoff, 2003). Middle-class European American families often expect young toddlers to follow simple social rules, whereas many traditional Japanese, Native American, and Mayan families believe that following social rules cannot be expected or enforced until a child is ready to comply with them voluntarily (Rogoff, 2003). In addition, in many cultures, children are not expected to sleep alone or follow napping and bedtime routines—instead they fall asleep when they are tired and sleep with their parents or siblings (Rogoff, 2003). Although these areas are commonly addressed in EI service provision, EI providers should be careful not to ascribe behaviors to disability when they are considered developmentally appropriate in the culture of the family.
“EI providers should be careful not to ascribe behaviors to disability when they are considered developmentally appropriate in the culture of the family.”
Acquiring knowledge about the cultures of families receiving EI services increases the ability of the EI provider to match interventions to family needs and desires. However, providers must be cautious not to apply stereotypes to families on the basis of individual cultural factors (Durand, 2010). Multiple influences contribute to the cultural beliefs and values of families. One way for providers to obtain this knowledge is to have open communication with families about what they expect from their children at different ages or stages of development (Durand, 2010). When conducting assessments that ask if children have attained developmental milestones, providers may explore caregiver responses to determine if a milestone is not being reached because it is not developmentally appropriate according to the family culture (Roopnarine & Metindogan, 2006).
Revisiting Tanya and the Capuno Family: What Went Wrong?
Tanya did not take time to talk with the Capuno family about their expectations for David in each of the areas in which they expressed concern. Instead, she made recommendations based on her experiences with other families that may not share the same values and beliefs about children as the Capunos. Tanya could have engaged in more in-depth conversation about the Capuno family’s beliefs and expectations for children and their desires for David’s participation and growth to better match potential strategies to the needs of the family.
Building Culturally Responsive Practices
Through recognition and acceptance of the cultural differences between themselves and the families they serve, EI providers can build culturally responsive practices into their professional repertoire. Although it is impractical to develop an encyclopedic knowledge of the cultural beliefs of every family that an EI provider works with, it is possible for providers to become competent in process-oriented practices that bridge the differences between cultures to work effectively with all families receiving EI services (Durand, 2010; Lynch & Hanson, 2011). The foundation for building these practices is openness and willingness on the part of the provider to explore the strengths, needs, and desires of the families they are serving.
EI providers can build their cultural competence through recognition and utilization of culturally protective factors (Withrow, 2008). Culturally protective factors are those factors that are present in a cultural group that can increase the resiliency of the families of children receiving EI services (Mogro-Wilson, 2011; Withrow, 2008). For example, some cultural groups typically provide strong maternal social support through emotionally supportive relationships and assistance in caring for children and completing other required tasks. This support can lessen the stress on the mother of a child with disabilities and positively affect infant social development (Withrow, 2008). By recognizing this culturally protective factor, the EI provider may be able to build this support into services—increasing the likelihood that service provision will be culturally appropriate and successful. Some additional culturally protective factors are listed in Table 2. However, it is important to remember that each family is unique and not make the assumption that a family possesses culturally protective factors just because they belong to a specific cultural group.
Culturally Protective Factors
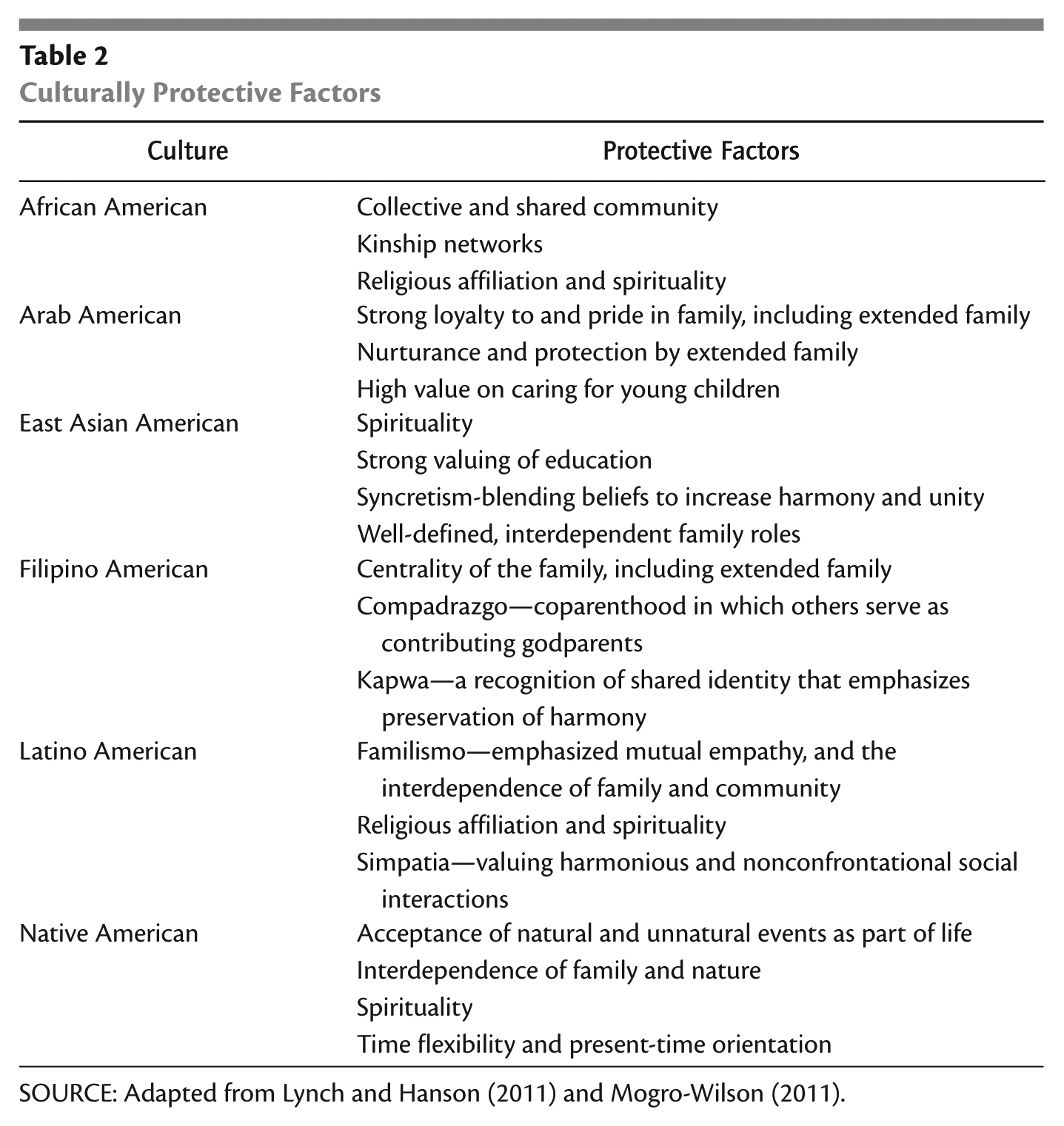
SOURCE: Adapted from Lynch and Hanson (2011) and Mogro-Wilson (2011).
“it is important to remember that each family is unique and not make the assumption that a family possesses culturally protective factors just because they belong to a specific cultural group.”
Another way EI providers can build their cultural competence is through cultural reciprocity (Kalyanpur & Harry, 1997). Cultural reciprocity is a process through which providers frame their interactions with families receiving services and is a way to honor the voices of families (Barrera & Kramer, 2009). Engaging in this process involves attending to cultural beliefs and values of the provider and the family, and respecting the differences that may arise (Barrera & Kramer, 2009; Kalyanpur & Harry, 1997). Furthermore, providers build on this new knowledge by using it to address the individual needs of the family (Kalyanpur & Harry, 1997). Four guidelines for engaging in cultural reciprocity are as follows: (a) recognize cultural values embedded in professional interpretations and suggestions, (b) establish whether the family values these interpretations and suggestions or whether their view differs—and in what ways, (c) acknowledge identified differences and explain the basis of the professional interpretations and suggestions, (d) collaborate with the family to adapt interpretations and suggestions to honor the values of the family (Kalyanpur & Harry, 1997). Engaging in cultural reciprocity makes cultural differences more explicit, decreases miscommunication, and can empower the family and provider by providing space for new options and ideas to be created and considered (Barrera & Kramer, 2009; Kalyanpur & Harry, 1997).
Revisiting Tanya and the Capuno Family: What Went Wrong?
Tanya’s recommendations, although well intended, did not consider culturally protective factors or incorporate the guidelines of cultural reciprocity, which led to a mismatch with the needs of the family. Tanya failed to consider if the Capuno family had protective factors related to their culture that could be incorporated into her support provision. Tanya also did not recognize that her cultural values about discipline and the capacities of children shaped her recommendations, nor did she involve the Capuno family in discussion of their expectations for David. If Tanya had adhered to the first two guidelines of cultural reciprocity, she could have engaged the Capuno family in exploring the differences in their views and jointly built strategies that they felt would work within the context of their family and build on their unique strengths.
Reflecting and Evaluating Practices
The first three components of this framework encourage thoughtful reflection and action on the part of the provider. The last component is a reminder for providers to continuously reflect on their practice and seek feedback from families and colleagues after interactions to evaluate the effectiveness of these interactions and practices. One cannot simply develop cultural competence and move on; it is a recursive process that requires consistent introspection and adjustments (Barrera & Kramer, 2009). Each time a provider begins work with a new family, he or she needs to draw on his or her prior knowledge and experiences in consideration of how to best serve the family in a culturally responsive manner.
Reflective practice, which is used in multiple help-giving fields such as education and infant mental health, is a valuable way for providers to explore and evaluate their experiences in the field (Gatti, Watson, & Siegel, 2011). In reflective practice, providers share specific situations they have encountered and participate in a critical examination of the situation with a facilitator and trusted peers (Gatti et al., 2011). The facilitator, peers, and provider engage in listening and asking questions to more fully understand the dynamics of the situation being reflected on (Gatti et al., 2011).
A similar way to engage in reflection is through reflective supervision, in which the provider works with a supervisor in a dyadic relationship. The supervisor supports the provider by providing a safe, respectful environment in which to explore experiences and communicate to help the provider develop deeper understanding of these experiences (Eggbeer, Mann, & Seibel, 2007; Stroud, 2010). Sessions should begin with the provider remembering and describing a specific interaction between herself or himself and a family (Foley, 2010; Gatti et al., 2011). After the provider initially describes the interaction, a facilitator or supervisor engages in a conversation about the memory to more fully develop how the experience played out and the provider’s feelings about it. Open-ended questions allow for more depth in reflection and discussion. Some questions that might be asked are listed in Figure 2. By regularly reflecting on and discussing the role culture plays in provider–family interactions, providers may recognize ways to improve their practice, as well as become more comfortable and confident when discussing cultural issues with the families they are serving (Stroud, 2010).
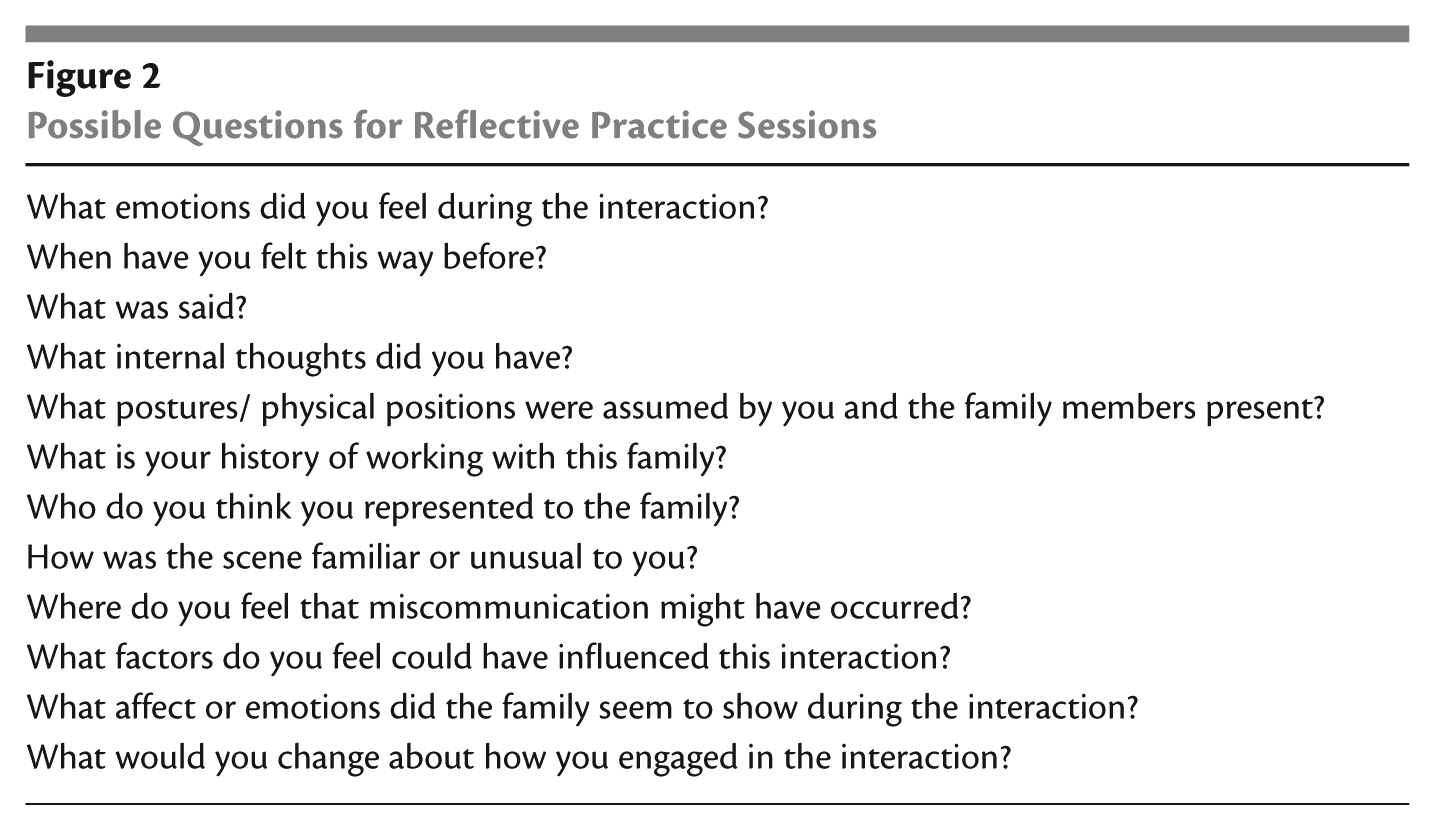
Possible Questions for Reflective Practice Sessions
When engaging in reflective practices, it is critical that providers are mindful of maintaining the confidentiality of families through use of pseudonyms if they do not have consent to share information. To enhance the effectiveness of reflective practice, providers may want to keep a journal of experiences, in which they identify tense or challenging interactions as well as situations that went particularly well. This journal can help providers self-reflect on their own best practices and areas in need of improvement, and serve as a reference when engaging in reflective practice sessions.
Conclusion
Cultural competence is an important component of providing effective family-centered EI services in the natural environment. However, cultural competence is not a discrete skill that can be learned once and considered accomplished—it requires a constant commitment by the EI provider (Barrera & Kramer, 2009; Kalyanpur & Harry, 1997). The framework presented in this article is intended to assist EI providers in working toward more culturally responsive practice by providing a broad overview of the current literature and recommended best practices in this area. By using the framework, EI service providers can more effectively serve families in ways that respect their culture and individuality. The vignette below demonstrates how Tanya incorporated the framework into her practice, with positive results.
Tanya begins to reflect on her recommendations to the Capuno family. She questions why she recommended a set bedtime routine for David, when the family did not specifically ask for help with David’s sleeping habits. Tanya realizes that her personal beliefs about children’s bedtimes and routines may not be the same as those held by the Capunos. Tanya’s recognition that the Capuno family may have different cultural beliefs and values for their children’s development encourages her to try a different approach with the Capuno family. The next time she calls Mrs. Capuno, Tanya says that she is not sure if her prior recommendations were a good match for the family and apologizes to Mrs. Capuno. Tanya suggests that she would like to learn more about their family, and what they think David should be doing at his age. Mrs. Capuno seems pleased and schedules a date for the following week.
At the next visit, Tanya listens carefully to Mr. and Mrs. Capuno as they explain that they would like David to use more words in his daily activities, but they feel that it is not appropriate to frustrate him by withholding desired items. They also share that they believe that children as young as David are not yet capable of controlling emotions and that isolating him would scare him. Mrs. Capuno hesitantly says that their family has always spanked and scolded the children for misbehavior, but she does not feel that this is appropriate for David. They are most interested in him playing well with his sisters and getting along better with all the family members, including his godparents who spend time with him often. They feel that if he could talk more, he would not be so aggressive. Tanya realizes that her prior suggestions were not in harmony with the beliefs and values of the Capuno family.
Tanya and the Capuno family discuss David’s daily routine and decide that a structured family playtime everyday is one way to teach David more acceptable ways to communicate and interact with his family members. Tanya suggests playing a game where family members hide toys and David must find who has them, embedding gestures and questions (e.g., “Where is the ball? Does Papa have the ball?). She also suggests redirecting aggressive behavior by saying “No, nice touches” and stroking the skin of the person toward whom he was aggressive. She explains that these strategies can encourage David to use more language and teach him appropriate ways to interact with his family members. She asks the Capuno family whether they feel these ideas will work for their family, and they seem excited to try out the strategies.
Tanya begins to keep a journal of her interactions with the families she serves, including the Capuno family. She writes about her experiences and then reviews them after a day or two, highlighting meaningful or puzzling exchanges for further thought. Tanya shares her experiences with a reflective practice group she formed with the other service providers in her organization, with whom she has consent from the family to share information. During these reflective sessions, Tanya is able to ask questions and share challenges that she is not sure how to address independently. She feels more supported in her practice and has found that she learns a lot in helping the others reflect on their experiences. Through these reflective activities, Tanya sees that she often assumed the families she worked had the same beliefs and values as she did, and that she often provided suggestions without considering the cultural context of the family. She consciously works to engage in cultural reciprocity so that she can provide support that is in harmony with the beliefs and values of each family, and tries to engage families more fully in developing strategies.
Footnotes
Author’s Note
You may reach Wendy Bradshaw by e-mail at