
Abstract
Bella is a 5-year-old girl with autism who attends a reverse inclusive preschool class. She primarily uses gestures and a communication binder to communicate with others. In addition, she is not toilet trained even though her teachers and her parents have tried numerous attempts over a 3-year period to train her. Bella also has gastrointestinal problems that make toilet training even more difficult. Her doctors, teachers, and parents are starting to doubt she will ever be toilet trained. Recently, Bella’s mom was in her preschool class as a volunteer. Her mom was standing by Bella when a few students approached them and said to her mom, “Why does Bella go potty in her pants? She’s too big to go potty in her pants. I don’t want to play with her when she smells.” The students then walked away. Bella’s mom was crushed. She realized that peer acceptance is an integral part of helping her daughter’s social and communication deficits, and that this was going to become an even bigger problem as Bella gets older. It was in that moment that Bella’s mom realized that she needs a plan, a portable potty plan (PPP).
The idea of beginning to toilet train a typically developing child can often produce a sense of anxiety in parents and caregivers. However, for parents, caregivers, teachers, and other related service personnel who work with children diagnosed with autism, toilet training can seem an almost impossible task. Researchers note that compared with their typically developing peers, many children with autism have an increased level of difficulty reaching this milestone (Cicero & Pfadt, 2002; Crowley, 2009). Current measures of how widespread this problem may be within early childhood programs are difficult to locate, but a handful of studies provide some insights into this issue. For instance, Schum et al. (2002) found that in a sample of 267 typically developing children, the median age for boys to achieve toilet training was 35 months (girls = 32.5 months). In a much earlier study, Eaves, Ho, and Eaves (1994) found that in a sample of 166 children with autism spectrum disorders, 81% (deemed the “high-functioning” group) were successfully toilet trained by the age of 42 months, whereas the remaining 19% (deemed the “low-functioning” group) had an average age of 59 months before training with typical methods was successful. In attempting to gauge the possible, current situation suggested by these small-sample findings, one should keep in mind that the number of children with autism in our public schools increased over 500% from 1993 to 2002 (U.S. Government Accountability Office, 2005). Given the fact that the rate of autism has increased over 78% since 2002 (Centers for Disease Control and Prevention, 2012), our public schools are now feeling the impact of this increase.
The acquisition and use of toilet-training skills is a necessary and basic part of the quality of life and independence for children with autism (and for all children, for that matter), and the inability to successfully self-toilet can present for these children barriers to establishing routines, such as successful socialization with peers (Rinald & Mirenda, 2012). In addition to increased social stigma, failure to learn self-care skills such as toileting can result in a comparatively limited number and range of activities in which children are encouraged to participate (as discussed in Kroeger & Sorensen-Burnworth, 2009), as well as the health risks and discomfort associated with poor personal hygiene. Despite the importance of this critical life skill for developing a foundation for greater independence in children with autism, there has been a scarcity of literature that is aimed specifically at assisting parents, caregivers, teachers, and related service personnel with this important undertaking (Kroeger & Sorensen-Burnworth, 2009). This scarcity has led quite a few current researchers to base their toileting interventions for children with autism (e.g., Chang, Lee, Chou, Chen, & Chen, 2011; Chung, 2007; Kroeger & Sorensen, 2010; LeBlanc, Carr, Crossett, Bennett, & Detweiler, 2005; Post & Kirkpatrick, 2004) on a single study conducted more than 40 years ago (i.e., Azrin & Foxx, 1971).
Behavioral Approaches to Toilet Training
Despite the dearth of literature in this area, a few recent studies using behavioral approaches have demonstrated efficacy in assisting children with autism to toilet train quickly and with a high level of maintenance, even those children who have had previous difficulty with acquiring this skill. For example, within a 7- to 11-day training period, Cicero and Pfadt (2002) used a combination of positive reinforcement and systematic instruction to help children with autism completely eliminate urination accidents and spontaneously request bathroom use, gains that were maintained over 6-month and 1-year follow-up periods. Similarly, recent toileting studies have used (a) behavioral approaches to increase in-toilet defecation (Rinald & Mirenda, 2012) and (b) parents as trainers for their children with autism (e.g., Kroeger & Sorensen, 2010; LeBlanc et al., 2005). There is also emerging evidence that behavioral approaches used in conjunction with visual supports may be able to improve gains produced through behavioral approaches alone. For example, Keen, Brannigan, and Cuskelly (2007) implemented a reinforcement-based, video modeling procedure with a treatment group of children with autism and found that the combination of behavioral and visual methods produced a higher frequency of appropriate urination (i.e., within a toilet) than that found within a control group of children who received only the reinforcement procedure.
Visual Supports
Visual supports is a very broad term that includes many types of media such as real objects, photographs, and line drawings, as well as many uses, such as schedules, scripts, and task lists (Meadan, Ostrosky, Triplett, Michna, & Fettig, 2011). The use of visual supports is a well-established, evidenced-based approach for helping children with autism acquire new skills and successfully navigate their environments (Odom et al., 2003). Supports such as schedules can assist children with autism to establish meaningful, school-based routines (e.g., Massey & Wheeler, 2000), and other types of visual supports can aid with the development of needed skills, such as making transitions (Dettmer, Simpson, Myles, & Ganz, 2000) and engaging in socially appropriate behaviors with teachers and peers (Schneider & Goldstein, 2010). The use of visual media integrates well with the systematic, data-based approaches to teaching often used for students with developmental disabilities, and it plays to a particular strength of most persons with autism, that of visual-spatial ability (Mitchell & Ropar, 2004).
Portability
Many of the researchers studying toilet training have used highly specialized equipment (e.g., wetness detectors, toileting videos) and techniques (e.g., positive practice, communication training) that make difficult the transfer of the interventions to other environments. By necessity, interventions that are used to assist children with autism to toilet train across, for instance, home and school environments should have portability (or be easily transferable from one environment to another, as well as conveniently usable in all of the places that children will go) so that they can readily use this skill across varying sets of conditions and demands. Going potty at home is not like going potty at school, and visits to shopping malls and outdoor events add even more challenges in making the successful transfer of learned skills. It has been demonstrated that the proper incorporation and use of visual strategies can provide children with autism the support they need for successfully using previously learned skills across persons, places, and changing sets of environmental cues (Laushey, Heflin, Shippen, Alberto, & Fredrick, 2009; Dettmer et al., 2000).
However, to be truly “portable,” an intervention must be physically transferable in addition to being conceptually transferable. The visual materials that provide support for the successful demonstration of a skill should be easy to carry, store, and retrieve, and they should be easy for children, teachers, and parents to organize and use when needed. Ideally, they should also be inexpensive to create, replace, clean, and maintain.
Designing and Implementing a PPP
As experts in education and child development, teachers are encouraged to take the lead in teaming with parents to design and implement a plan that will be used across home and school. In the same way that folders containing student work, screening information, notes to parents about upcoming events, and so on go back and forth with children between school and home, the potty plan should be designed to travel, for who knows when and where the need to go will arise, and a lack of preparedness is the enemy of instruction.
It is also important to note that in their work with parents from diverse cultural backgrounds and their children with autism, it is recommended that teachers use a range of visual symbols specific to a child’s culture (Trembath, Balandin, & Rossi, 2005). Also relevant are the following steps from the National Autism Center (2009) for maximizing the potential of evidence-based interventions to be accepted by families from diverse backgrounds who have children with autism: (a) Target behaviors for intervention that are most relevant and acceptable to the family and their culture; (b) consider the educational needs of the child not from the viewpoint of the dominant culture but from the viewpoint of the child’s culture, and be willing to deliver instruction appropriately; and (c) critically examine personal biases that could lead to artificial, ineffective alterations in educational practices.
What follows is a series of six instructional steps (see Table 1, for a condensed version of steps) for teachers to implement in the design and use of a PPP for a student with autism. To illustrate what implementation might look like, immediately following each instructional step is a corresponding part of the case example, Bella. Last, Bella’s immediate and long-term outcomes are described.
Six PPP Steps Condensed
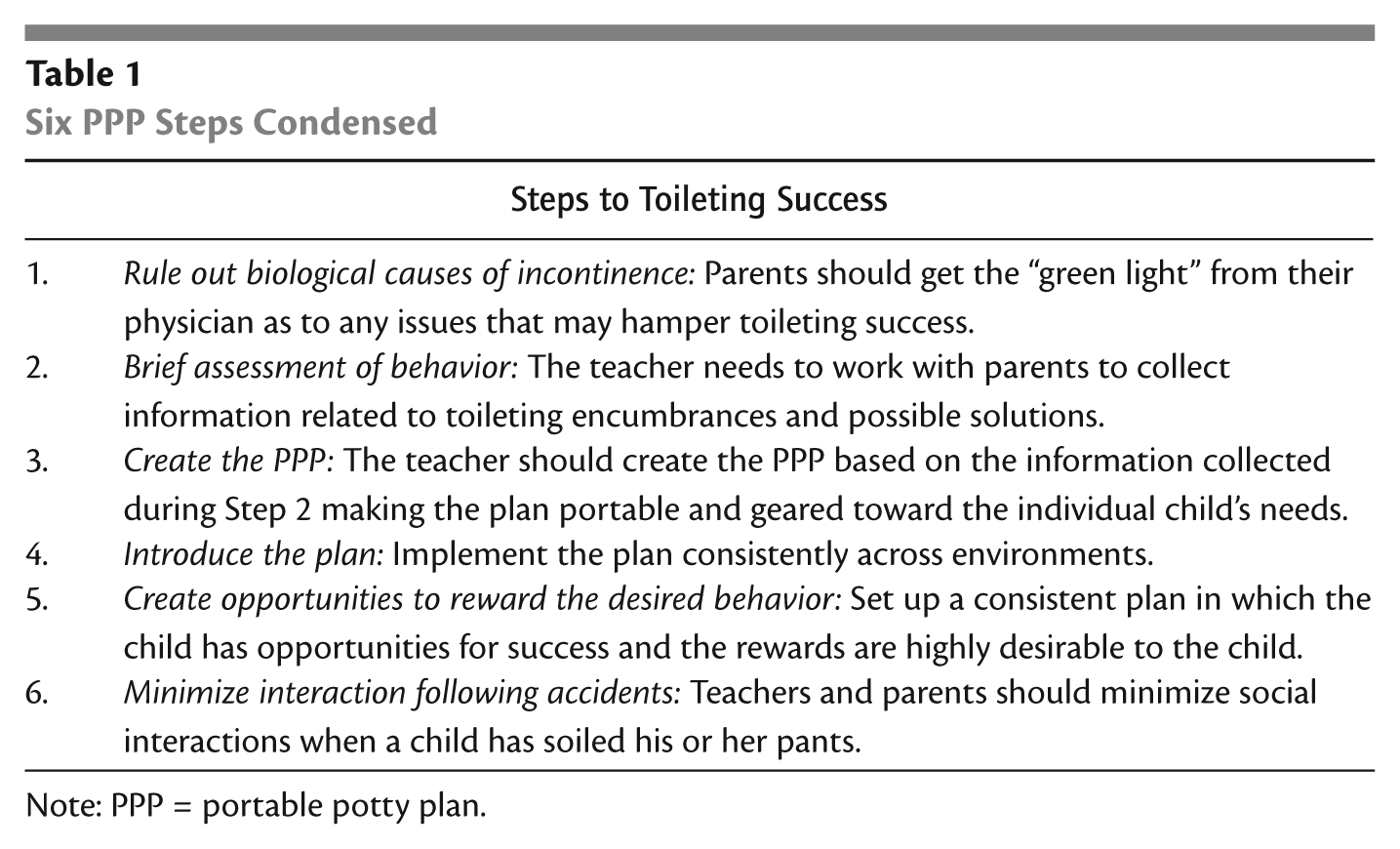
Note: PPP = portable potty plan.
Step 1: Rule Out Biological Causes of Incontinence
In this step, teachers should encourage parents to check with their pediatricians to ensure there are no biological causes for incontinence that might make toilet training difficult or less effective for their child (Rinald & Mirenda, 2012). This is not to say that parents should be encouraged to give up on the idea of toilet training if problems are discovered. Rather, parents should be equipped with the “big picture” by knowing the obstacles and working with their pediatrician to make a plan that will be more likely to work for their child and family.
Bella is under the care of an internist for gastrointestinal problems. Her internist and family physician agree that, although her health issues might make learning to self-toilet a little more difficult, her current diet and medication were being monitored and controlled closely enough that they feel comfortable with giving Bella’s parents the green light to address toileting issues.
Step 2: Brief Assessment of Behavior
Once all health concerns have been carefully considered, the next step is for the teacher and parents to conduct a brief assessment of the child’s current voiding behavior (i.e., urinating and bowel movements) across school and home (Keen et al., 2007). Assessment should consist of two steps: (a) recording the child’s void times and (b) interviews with other teachers, paraeducators, and family members (including the child, if possible).
First, the teacher and parents should begin to record when the child voids so that any events or situations occurring around the time of the incontinence can be examined to see whether they (a) somehow are contributing to the occurrence or (b) present barriers to toileting (see Figure 1 for an example void chart). This information will also be used in the next step of the plan in which times are set to take the child to the bathroom. This information should be recorded for approximately 2 to 4 weeks, even if the child has never voided in the toilet, to establish common dry and void times. However, if after the period of 2 weeks, a consistent trend emerges (e.g., the child is found to be consistently dry from 7 a.m. to 9 a.m., voids in pants around 9:30 a.m., etc.), then the teacher and parent may make a mutual decision to move on to Step 3. Teachers and parents must be consistent in recording the data throughout planning and implementing the toileting intervention for the child to achieve toileting success.
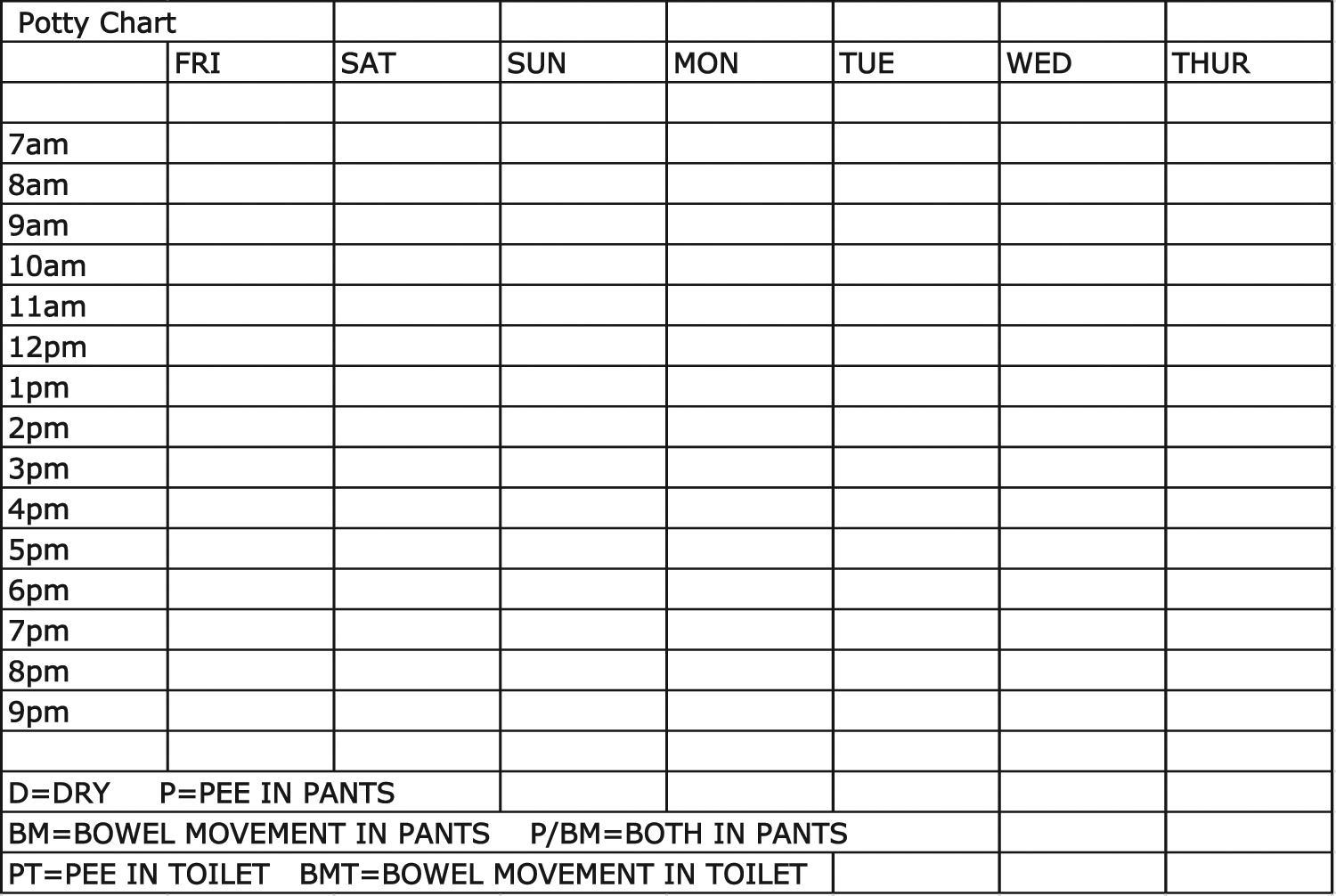
Sample void chart
During the period that voiding information is being recorded, teachers should conduct the interviews by asking other teachers, paraeducators, and family members about (a) any possible barriers to toileting success (e.g., inconsistent daily schedules or communication difficulties), (b) the presence of any signs of toilet readiness (e.g., separating self from others when voiding in pants, dry periods of several hours, and/or showing interest in bathroom behaviors such as flushing), and (c) the child’s current ability to perform behaviors closely involved with toileting (e.g., the ability to independently dress, and wash and dry hands). Furthermore, the teacher needs to determine the child’s special, preferred interests, such as favorite television or movie characters and favorite toys or snacks.
After Bella’s parents checked with the doctor, they met with her teacher to devise a plan that can be successfully implemented at school, home, and in the community. During the information gathering process, certain barriers that might prevent toileting success are apparent. First, Bella has difficulty communicating her needs and is using a communication binder and gestures to functionally communicate with others. Through the teacher and parent discussion, both parties realize that Bella has some prerequisite skills to toilet training that they will consider while making her PPP (e.g., Bella can wash and dry her hands, and she can sit on and flush the toilet, when verbally prompted). Bella’s teacher makes a note to consider these skills when creating her visual schedule that will be on the PPP. For example, Bella will not need the task of washing her hands broken down into many steps; instead, her parents and teacher believe that a picture card showing a child washing her hands will suffice for this step of the potty plan. Her parents disclose that the family’s hectic schedule makes it difficult to be consistent with checking to see whether she is dry and taking her to the bathroom. Bella’s family reports that once every 1 to 2 weeks, they catch her before she voids in her pants and will take her to the bathroom where she will then void in the toilet. Moreover, Bella’s family states that she occasionally separates herself from others when she has a bowel movement in her pants. Finally, Bella’s parents also relayed that changing her soiled underpants is a fun time for her and that she giggles and laughs with her parents, who sometimes encourage this type of interaction.
Step 3: Create the PPP
The teacher will now create the PPP, which is an intentional play on words (because humor must be injected into this plan to keep one’s sanity during potty training!). The first step is for the teacher to acquire a container that is portable (e.g., a plastic storage clipboard or plastic accordion folder), able to enclose small items such as laminated pictures, and easily wiped off, which is important because this is going into bathrooms.
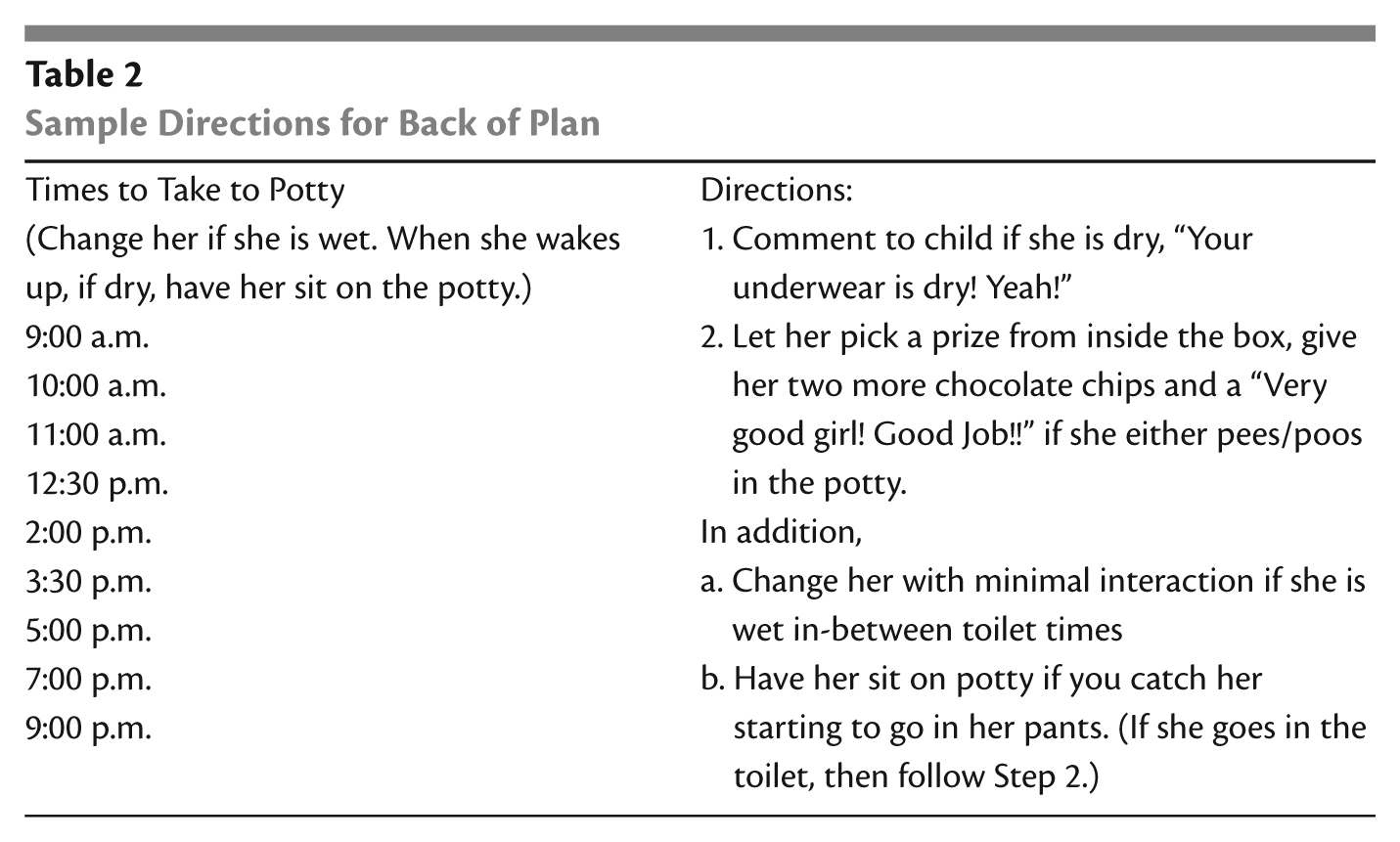
Brief directions for the plan should be placed on the back of the container, to make it easy for anyone to use with the child (see Table 2 for example directions). The directions need to include the times selected to take the child to the restroom, based on the initial information recorded on dry and void times. The times are selected by finding when she is most likely to be found dry, not wet. Once a child is wet or soiled, there is a reduction in the likelihood he or she will then void in the toilet. The goal is for the teacher and parents to try to discover the period(s) of time right before a child is likely to void in his or her underpants. Therefore, when implementing the plan, if the teacher or parent finds that the child tends to have already voided at a previously chosen time, then the target time needs to be reduced by about 15 min. This is to insure that the child is found dry at a time when voiding is most likely to occur. Once the picture task list and the directions for use are determined, they are then placed on the portable clipboard and held in place by a self-adhesive laminated sheet, which allows the plan to be wiped off without water damage.
Sample Directions for Back of Plan
Inside the portable storage container, there should be from three to six small, nontranslucent bags containing a “surprise” that a child will get to choose from when he or she has successfully used the toilet. The bags should contain items that the specific child is likely to find highly desirable. (This list of highly desirable items is obtained during Step 2.) Examples of some items that can be used are small board books, bubbles, jellybeans, a lollipop, a picture of a favorite toy, or movie. The intent of using a picture of a favorite toy or movie is that the child will get to play with the actual toy or watch the movie immediately afterward. Almost any highly desirable item can be used, but, ideally, the items used inside the PPP case should not be ones freely available at other times. In addition, keep a small bag of a highly desirable item (e.g., small candies) to reward the child when he or she is dry, as further detailed in Step 4.
Teachers and parents can also keep a data collection sheet and pen inside the case to collect ongoing data. PPP users will hopefully want to collect data to see whether the plan is working, know when and whether any details of the plan need to be tweaked, inform other plan users how the child did throughout the day, and perhaps gauge the extent of completion of associated Individual Education Plan goals or objectives. Data collection need not be complicated. Making daily tally marks to count instances of “voids in pants” and “voids in potty” will work just fine.
Bella is found to void frequently around 9:15 a.m. Therefore, 9:00 a.m. is included as one of the times to take her to the bathroom (see Table 2 for all of the times during the day that Bella is taken to the bathroom by a teacher, parent, or caregiver). Bella’s plan is contained in a portable storage clipboard (see Figure 2 for an example of how to set up the portable clipboard). The outside of the clipboard uses a visual support showing the step-by-step details of the toileting process paired with high-interest pictures to gain her attention (information on a child’s favorite character or high-interest subjects are obtained during Step 2). Bella loves princesses and mermaids, and so above each step in her plan is a favorite princess character.

Portable clipboard
Step 4: Introduce the Plan
This is the implementation stage of the intervention. First, begin taking the child to the restroom according to the predetermined times (Keen et al., 2007), as listed in the directions. The teacher and parents who are implementing the plan will pair taking the child to the restroom with a visual toileting card every time they go. The toileting card should be placed in multiple locations (e.g., in the child’s communication binder, by his or her bed, just outside of the bathroom, in his or her cubby at preschool, at the child’s desk) to enable the child to have easy access to it once its purpose is understood: to communicate that the child has to use the restroom. In addition, take the child to the restroom if there are signs that he or she is getting ready to void in pants. On entering the restroom, give the child the card to place on the PPP (e.g., via adhesive Velcro© strip), placed just above the first picture step of the toileting procedure. The teacher and parents must be consistent in their use of the plan for the child to have success across environments.
Bella’s toileting card is a picture of a mermaid using the restroom and is kept on her communication binder. Her plan consists of the following steps: pull down pants, sit on potty, void in potty, wipe, flush, and wash hands. Each of her steps is paired with a highly preferred favorite princess character to attract her interest and attention to the case (see Figure 3). Bella’s toileting procedure is kept as simple as possible by choosing the number of steps and level of detail within each step according to her level of functioning.

Sample communication binder and PPP
Step 5: Create Opportunities to Reward the Desired Behavior
When the child is taken to the restroom and has not voided in his or her pants, the teacher will open the case and give the child the highly desirable item previously selected for this purpose (e.g., the reward chosen to give the child for having dry underpants). At this time, the teacher will also verbally praise the child for being dry. Next, the teacher will prompt the child to perform the toileting procedure by giving the least amount of support for the child to successfully complete each step (Cicero & Pfadt, 2002). Begin with a verbal direction paired with pointing to the picture step, and, if necessary (i.e., the child fails to perform the step), proceed progressively by pairing verbal direction and pointing to the picture step with (a) gesturing, for instance, to the potty (for “sit on potty”); (b) physically guiding the child through the step and then resetting the situation for him or her to try independently; and (c) physically guiding the child through the step (without resetting the situation).
The child should sit on the toilet for a designated amount of time. The time will be adjusted according to the individual child’s ability to sit on the toilet. For some children, sitting time could be as little as 10 s, but from there the child will work toward gradually increasing the amount of time. In addition, the plan could be altered to include first giving the child the highly desirable item when dry and giving it again for sitting the desired amount of time. To increase the amount of sitting time, the amount of time between a child initiating sitting on the toilet and the child subsequently being given the highly desirable item could gradually be increased (e.g., from an initial time of 10-s to a 15-s sit time). If adding this to the plan, the teacher should consider including on the data sheet a place to write down the amount of time for each try at sitting on the toilet.
When the child has his or her first use of the toilet, as soon as it begins, celebrate with jubilant verbal praise. Simultaneously open the PPP and have the child pick one of the nontranslucent bags with the “prize” inside, and give the child another of the chosen highly desirable items that they also received for having dry underpants (e.g., the “successful void reward” paired with the “dry reward”). For the first few times, place items in the bag that can immediately reward the child for using the toilet. These items are to be rotated frequently and delivered immediately. For example, if a child is at the mall, then the PPP would not contain a picture card of a movie because the movie could not be delivered immediately. Try to stock the box according to location and keep adding fresh surprises. Only permit the child to choose one bag, and do not allow the child to look through all available bags.
When Bella is found to have dry pull-ups, she is given one chocolate chip from the PPP container while the teacher or parent simultaneously says, “Good dry underpants, Bella!” In the beginning when Bella was learning the toileting steps, the adult pointed to the first picture step on the front of the case (which was pulling down pants) while saying, “Pull down pants, Bella,” and then helped Bella to pull down her pants. For Bella, the amount of time chosen for sitting on the toilet was 15 min because, through previous attempts at toilet training, she was found to be able to comfortably sit for that amount of time. Examples of the contents of Bella’s different reward bags during the first few weeks of the toileting plan are skittles, princess stickers, a lollipop, and some jellybeans. Now, after a few weeks, Bella is following the toileting steps on her own, and the nontranslucent bags inside the PPP contain items such as picture cards of favorite books or movies that she receives after toileting success mixed in with other nontranslucent bags that contain aforementioned items (e.g., princess stickers).
Step 6: Minimize Interaction Following Accidents
During this step, teachers and parents should examine their own behavior during PPP implementation. For example, adults should minimize social interaction (talking, play, hugging, etc.) with the child during times when the child has soiled his or her pants (Rinald & Mirenda, 2012). This does not mean showing disapproval or scolding, only withholding “the good stuff” (e.g., making it a fun time by talking, playing, hugging, etc.). Give the child an opportunity to perform each step by (a) providing assistance only when needed, and (b) providing only the amount/type of assistance needed, and make your approval of his or her success readily stand out from times when positive social interaction is withheld.
Before PPP implementation, Bella used the time when her parents changed her as fun time to interact with her caregivers. When Bella’s toileting intervention was implemented, her parents changed their behavior. When she was found to have soiled underpants, her parents and teachers took her to the bathroom to change her. However, they minimized eye contact and verbal interactions with Bella to only what was necessary. If she soiled her pants when it was not a scheduled time for her to sit on the toilet, she was changed; she washed her hands, and she was on her way with as little interaction as possible. If this occurred during a predetermined time for her to sit on the toilet, she was directed with a hand gesture to follow her picture schedule on the front of the portable storage clipboard, again, with minimal interaction, except when she voided into the toilet. In addition, when she was found to have soiled her pants during the predetermined toilet times, she was not given the reward for dry underpants. She was only given a chocolate chip for then voiding into the toilet while being simultaneously permitted to choose one of the nontranslucent bags that contained the prize inside (e.g., the “successful void reward” paired with the “dry reward”).
Conclusion
Toileting is a difficult life skill, both to teach and to learn. However, this skill is an integral part of life, and successful mastery can lead to greater independence for the child, parent, and teacher. Although the PPP’s design centers on the use of visual supports and positive reinforcement, its greatest strength may lie within its portability. By being useful to parents and professionals across the environments that children frequent throughout their day, there is an increased functional utility in the procedure for them as well. In addition, it should be noted that although the PPP was conceived for use with children with autism, it could also be useful to children with intellectual disabilities who respond to the use of visual supports.
Bella progressed quickly in learning the skill of independent toileting (see Figure 4). There were several reasons for Bella’s success. First, she was taken to the restroom when there was a high probability of finding her dry, thereby setting her up for success. Second, the rewards chosen for her were highly desirable. Third, when Bella started to demonstrate success with toileting, she was switched from pull-ups to regular underpants, a consequence that became desirable to Bella and therefore led to an even higher rate of success. After she urinated into the potty, she went right for the regular underpants, which her parents had bought in anticipation of success. It also helped that the underpants had her favorite cartoon characters on them. In fact, when her parents then tried to put her in pull-ups at night, she indicated “no pull-up” and would try to put on the regular underpants.
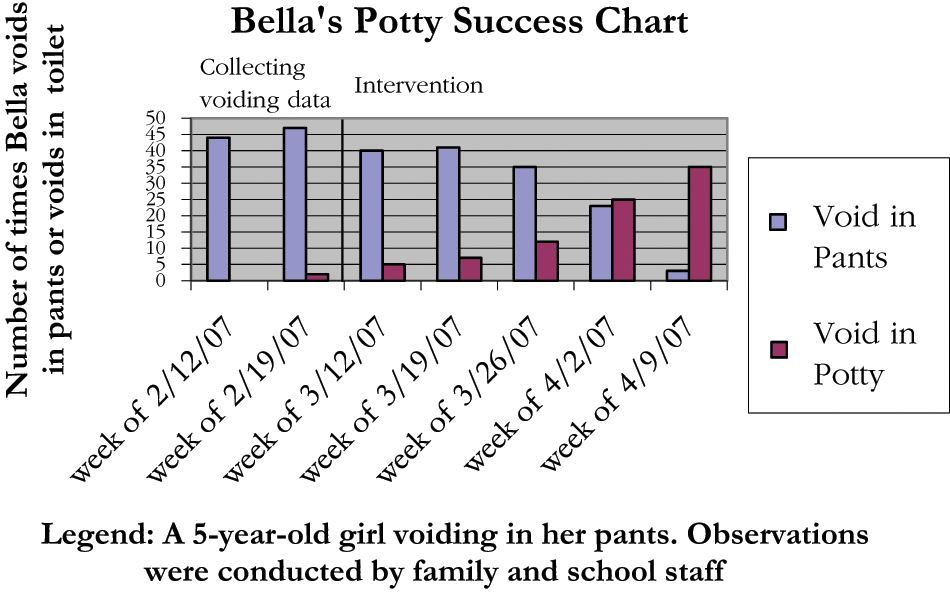
Toileting success chart
By applying the PPP, it became more desirable for Bella to engage in appropriate behavior than to void in her pants. As the plan continued, she found favorite movies and hugging, which were at first delivered as picture cards, more desirable than edible treats. As she continued to experience success with toileting, she even started to independently choose the regular underpants that were kept in a drawer in her bathroom. In the end, it was Bella who decided, all by herself, that she no longer needed to use the PPP. One day, she ran into the bathroom and used the toilet independently, and that was the end of the PPP.