
Abstract

Molly was thrilled to be expecting her first child. She knew that there was a chance her child could be born with disabilities due to genetic factors, but this was a very much wanted pregnancy. When her son James was born prematurely, a few months later, he had complex medical needs and spent the first year of his life in the hospital. While James was hospitalized, he began receiving services through early intervention. Although he had access to the related services he needed, once he had been home for a bit, Molly wanted him to have the opportunity to socialize with his same-aged peers in a typical early childhood environment. She was also looking to get back into the workforce, having taken an extended leave of absence after James was born. She began making phone calls to child care programs around town, starting with places that her friends and family recommended. She wanted to be transparent about James’s needs, and in each phone call, she shared his age, the things she delighted in about him, and his diagnosis. In phone call after phone call, she was told that enrollment would not be possible due to the program’s inability to “meet his needs,” citing the lack of an on-site nurse, funding, or staff. Molly tried to explain that she was not asking for one-on-one support. In fact, she felt that would potentially stigmatize him. But she was still told “no.” She kept searching online and finally found a program that advertised itself as “inclusive” and was accredited through the National Association for the Education of Young Children (NAEYC). She was shocked at how welcome she felt, with the program even updating their marketing materials with James’s picture. However, after a few months, she got a phone call that she had to leave work and come to the center immediately. Staff were concerned that James might be in respiratory distress. When she arrived at the center, Molly realized that James was not in distress but was having typical two-year-old “big feelings.” While Molly had been en route, the center had called an ambulance and insisted that he needed medical intervention. Molly pleaded for a few minutes, tried to soothe James herself, and was able to settle him. She was advised to take him home for the rest of the day. She complied, not wanting to argue further. However, in the coming days and weeks, she came to recognize this event as a turning point in her relationship with child care staff.
Despite the well-recognized benefits of early care and education and the critical importance of access for children with disabilities (DEC & Start Early, 2024), access to care continues to remain elusive for those that need it most (Center for Law and Social Policy [CLASP], 2024; National Academies of Sciences, Engineering, and Medicine, 2023; Weglarz-Ward et al., 2019). Among child care providers, Costanzo and Magnuson (2024) identified potential factors that may influence a lack of access to care for children with disabilities, including the high cost of care, perceived discrimination against children with disabilities, and a lack of staff training or professional development. Weglarz-Ward and colleagues (2019) found similar results when surveying child care providers about their experiences serving young children with disabilities and also noted that providers reported high staff-to-child ratios, lack of planning time, and limited access to services as barriers.

In addition to provider-level challenges, there are also systemic barriers. Even publicly funded programs do not necessarily have sufficient funding and other necessary supports to serve all eligible children. Furthermore, children from historically marginalized backgrounds, such as children of color and children with disabilities, are even less likely to have access (CLASP, 2024; National Academies of Sciences, Engineering, and Medicine, 2023). There are also disparities in access to subsidies to support access to care, further compounding racial and economic disparities in accessing early childhood special education screening, identification, and referral for service delivery (ECTA, 2023). The U.S. Department of Health and Human Services and U.S. Department of Education’s (2023) policy statement on the inclusion of children with disabilities in early childhood programs highlights the need for child care programs to understand legal requirements to serve children with disabilities and adequately train and support child care staff. Furthermore, a recent report on building inclusive state child care systems from the Division for Early Childhood and Start Early (2024) calls for increased collection and reporting of data on children with disabilities accessing child care.
In addition to difficulties in securing initial access to child care, families of children with disabilities may not have access to sustained enrollment due to exclusionary practices (e.g., suspension and expulsion). Exclusionary practices in early childhood education prevent equitable and inclusive experiences for young children and their families. Particularly in early childhood, these practices are often done both explicitly (i.e., hard) and implicitly (i.e., soft). For example, a family may be told that their child can no longer continue to be enrolled in care (hard expulsion), or a program may implement policies and practices, such as requiring parents to pick their children up early, which makes sustained enrollment infeasible (soft expulsion) (Children’s Equity Project [CEP], 2020). Families may also be forced into placements that they would not otherwise choose. For example, families with young children with disabilities enrolled in a community-based setting may be told that they cannot receive services in that setting and must enroll in a public program, or forego services (Illinois State Board of Education [ISBE], 2022). It is important to note that discussions around suspension and expulsion often frame these practices as ‘exclusionary discipline,’ focusing mainly on children’s behavior, when in fact exclusions happen for other reasons, such as staff feeling illprepared to accommodate children’s needs, or apprehension regarding their disability status (O’Grady et. al, 2025).

The purpose of this article is to provide guidance and support for families with a young child with a disability in gaining sustained access to child care and to remind practitioners of the professional and legal responsibilities to serve these families. This paper is rooted in extant research and policy, and several of our authors’ lived experiences as mothers who experienced the early exclusions of their children with disabilities. Although we cannot change what happened to our own families, it is our fervent hope to prevent other families from experiencing the same. The vignette represents a composite of the experiences of 10 mothers whose young children with disabilities were expelled from child care settings, often because of their disability status (O’Grady, et.al, 2025). One of these mothers is also on the authorship team. We firmly believe that it is a collective responsibility of the entire early childhood system to ensure that all families have access to inclusive child care.
Barriers to Sustained Enrollment
Soon after Molly noticed the shift in her relationship with staff, she was called in for a meeting with the center director to “discuss James’s continued enrollment.” As she drove to the school, she had a sinking feeling in her stomach. The director, Pat, started the meeting by sharing that the center “loved” James and he was a “wonderful” child. However, the staff were concerned that James’ needs were “placing the program at risk.” Pat suggested that James might be “better off” in another setting, rather than staying enrolled at this center. Molly tried to press for a reason “why,” but through Pat’s tone and body language, it was clear that James would not be allowed back. Molly did not feel she could persuade Pat into keeping him and realized she did not want to. Why would she fight to keep her precious boy somewhere he was not wanted? She was also afraid of being labeled a “problem parent” or of the staff retaliating against James.
Expulsion of Young Children with Disabilities
Molly’s experience is all too common, as young children with disabilities are disproportionately suspended and expelled. Edge et al. (2018) found that approximately 43% of young children for whom teachers requested behavioral assistance qualified for or were receiving special education services. In addition, Zeng et al. (2021) reported that approximately 5.4% of preschool students with disabilities were excluded annually, compared to 1.5% of preschoolers without disabilities. Most research has been conducted in public preschool settings; exclusionary rates are predicted to be significantly higher in child care settings, although accurate and comprehensive data are often unavailable (Buell et al., 2022; Giordano et al., 2022). Expulsions occur early, even with infants and toddlers. In Illinois, 42% of child care programs disclosed having expelled an infant or toddler, due to a perception of being unable to meet that child’s needs (Cutler & Gilkerson, 2002). This number is most likely higher, as reliable statistics about infant and toddler expulsions are hard to attain.
It is important to note that in the expulsion discourse, there is much focus on teachers’ perceptions of, and responses to, children’s behavior. For young children with disabilities, these perceptions and responses are rooted in ableism, compounded with a deficit or negative mindset toward disability (O’Grady et al., 2024). For example, in a study examining teachers’ perceptions of “challenging” behaviors, participants noted feeling more frustrated with the behaviors of children with disabilities, specifically struggling with children who were non-speaking (O’Grady & Ostrosky, 2024). Programs may have strict policies to enroll or advance to an age-appropriate classroom around mobility or toileting. For children from multiple marginalized backgrounds, ableism intersects with other biases to sustain a system that disproportionally excludes and “others” these children (Cruz et al., 2021).
Pat told Molly that the center would be “happy” to keep James enrolled for two more weeks. Pat offered no further assistance in finding an alternative setting. Molly felt there was something terribly wrong with this whole situation. She sensed that James was being discriminated against because of his disability, and she began looking into her rights. She contacted the Parent Training and Information Center in her state, but they said they focused on special education rights for school-age students, not parent rights in child care settings. She contacted the Protection and Advocacy Agency in her state and, after answering dozens of questions, was connected with an attorney for a free consultation.
“It is critical for child care providers to know their legal responsibilities to serve children with disabilities.”
Expulsion Policies
Although many states require some form of stated exclusionary practice policy for licensed programs and explicit policies for the inclusion of children with disabilities (McCann et al., 2021), it is unclear how this translates into practice because there are no tracking systems for inclusion or exclusion in child care systems (Buell et al., 2022). Most existing legislation prohibiting exclusionary discipline only protects children in publicly funded programs (e.g., subsidized child care, Early/Head Start, public pre-K), leaving children in privately funded programs vulnerable to these practices (Loomis et al., 2021; O’Grady et al., 2024). Related to child care licensing, 31 states allow some in-program or soft suspensions (Buell et al., 2022). Notably, no states explicitly have legislation requiring the inclusion of children with disabilities in child care. However, the Individuals with Disabilities Education Act (IDEA, 2004) encourages services in natural environments and inclusive settings for infants and toddlers with disabilities. It is critical for child care providers to know their legal responsibilities to serve children with disabilities and to understand that children with disabilities cannot be excluded from care based on their disability status. Many early childhood educators want to include children with disabilities but may not feel like they have the knowledge, resources, and supports to do so effectively (Haines, 2023). To shift this mindset, the Division for Early Childhood (DEC) offers a wealth of resources to actualize recommended inclusive practices. It is important to note that the DEC Recommended Practices specifically call for practitioners to help families know their rights and develop advocacy skills (RPF9, RPF10) (DEC, 2014). Additional resources to support inclusive practices are available from partner national professional organizations (c.f., Early Childhood Technical Assistance Center [ECTA] Inclusion Indicators, Head Start Disability Resources).
After consulting with an attorney and joining online groups for moms of young children with disabilities, Molly finally found some helpful resources. She learned that the child care agency was required to follow the Americans with Disabilities Act (ADA). As she discovered more about the ADA, she found a Frequently Asked Questions (FAQs) document that specifically addressed access for children with disabilities in child care settings. In fact, the ADA offers a “FAQ” type document for child care centers (ADA, 2020). Key points are illustrated in Table 1.
ADA Guidance for Child Care Settings
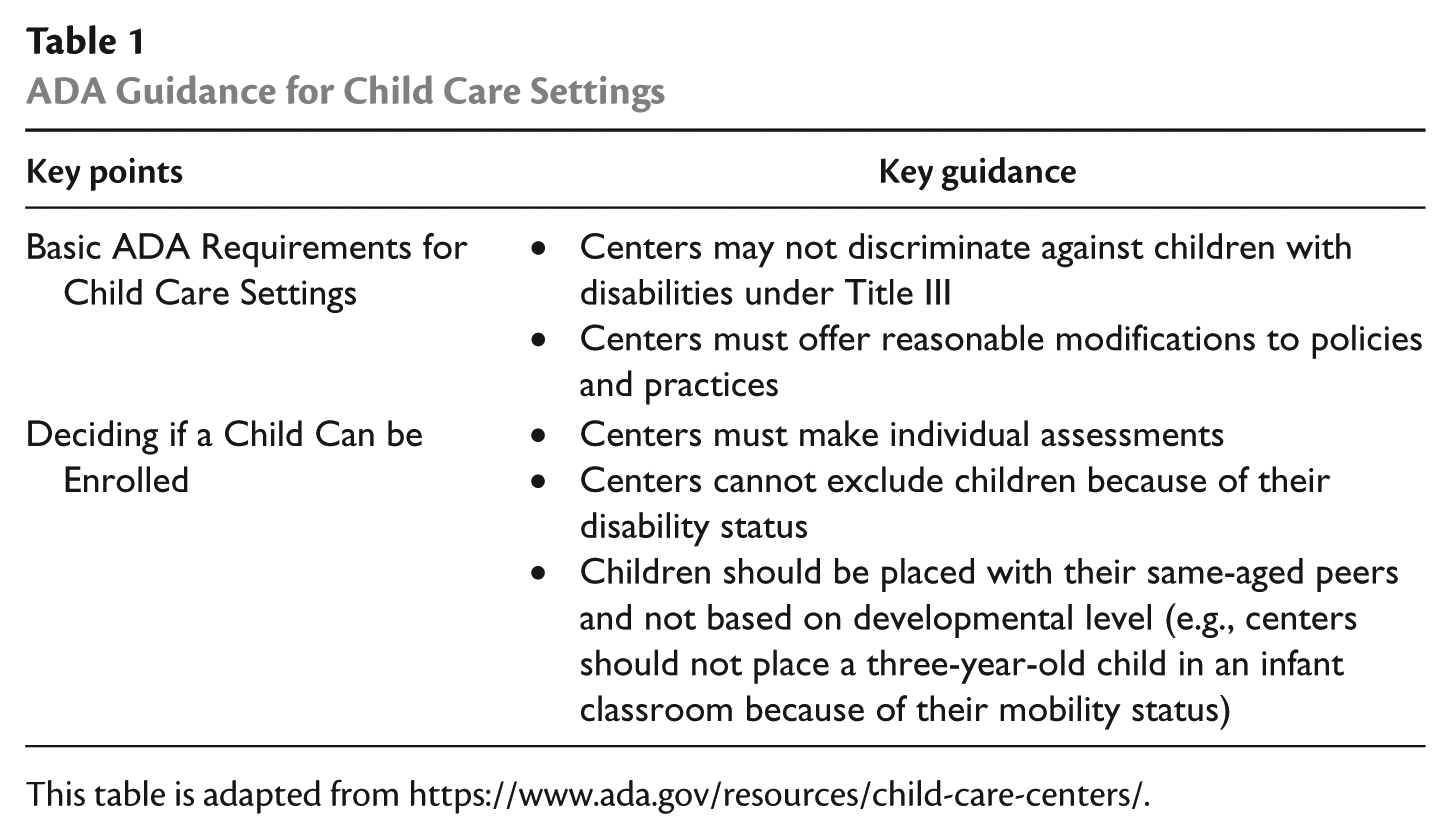
This table is adapted from https://www.ada.gov/resources/child-care-centers/.
Molly was determined to help other families avoid the heartbreaking situation she had found herself in. She questioned why the child care system was so resistant to children with disabilities. Shouldn’t caregivers of children with disabilities be able to work, with access to child care? She used her resolve to connect with other families in her online “moms of children with disabilities” group to create advocacy resources. When she shared her story and what she was struggling with, many moms commented and private messaged her to say this had happened to their family too. Together, they drafted an infographic outlining families’ rights and links to local resources to be highlighted and saved on their group’s page. She decided to file formal complaints through NAEYC and the Department of Justice against the child care James had left, and at the same time, seek an alternative child care program for a fresh start. Through the online group, Molly learned of a “mom’s morning out” style child care program that families reported having a positive experience with. She arranged a meeting with the director to discuss James’s potential enrollment. She was pleasantly surprised when the director also suggested including a member of James’s early intervention team in the meeting to learn how the staff could best support James. Molly was cautiously optimistic and also felt prepared to advocate if needed.
Family Advocacy
In addition to the complexities of navigating and accessing child care, families of young children with disabilities must also learn to navigate the special education system and assert their rights to gain access to the appropriate services and supports for their child (Burke, 2013; Trainor, 2010). Even with very young children, families often engage in advocacy (c.f., Burke et al., 2025; Schraml-Block & Ostrosky, 2022). Such advocacy often reflects three forms: individual advocacy (i.e., advocating for one’s child), peer advocacy (i.e., advocating for another family of a child with a disability), and systemic advocacy (i.e., advocating for systemic change for all children with disabilities) (Li et al., 2024). In this section, we give tangible strategies for families to advocate at each of these levels.
Individual Advocacy
At the most basic level, parents often have to advocate for their own children with disabilities to access child care. Although not specific to child care settings, Trainor (2010) characterized several individual advocacy strategies that may be relevant to child care settings: intuitive, disability expert, and strategist. Regarding intuitive, this suggests that families should trust their own instincts. Just as Molly felt in her gut that James was being discriminated against, intuitive advocacy reinforces the notion that families know their children best. Even without knowing their rights, families should trust their instincts. If something does not “seem right,” it probably is not. Disability expert reflects having intimate expertise of the type of disability of one’s child. Molly was familiar with James’ needs, recognizing that he needed some health support but not an individual aide. Using one’s knowledge of the type of disability and its implications can help inform what types of supports a child does (and does not) need in child care settings. Strategist advocacy means having knowledge of one’s rights. Molly’s perusal of the internet and her use of the ADA FAQ document reflect how Molly learned her rights under the ADA. This knowledge can help inform advocacy, including potential ways to resolve conflict.
Peer Advocacy
When families encounter resistance to including their child in a child care program, be it public or private, one of the most helpful resources can be the disability community (Goscicki et al., 2023). Indeed, parents often learn from one another about which organizations, schools, or programs not only meet compliance indicators for inclusion but also embrace the spirit of inclusion in their settings. Accordingly, as families try to identify the appropriate child care program for their children, they may consider reaching out to other families. To do this, families may attend parent support groups, join Facebook groups for families of children with disabilities in their geographic areas, follow disability influencers and family members of individuals with disabilities on Instagram, and read blog posts from families of children with disabilities. Like Molly, most families of children with disabilities want to help other families. As such, upon joining a group, families should consider asking to speak directly with other families to share their experiences and ask questions. For families navigating a complex system for the first time, they may feel as though they are supposed to assume and accept that nothing is available for their children. Peer advocacy can help to spread awareness, educate new parents or parents of newly identified children with disabilities, share resources, direct them to sources of support, and connect them to information regarding their children’s rights.
Systemic Advocacy
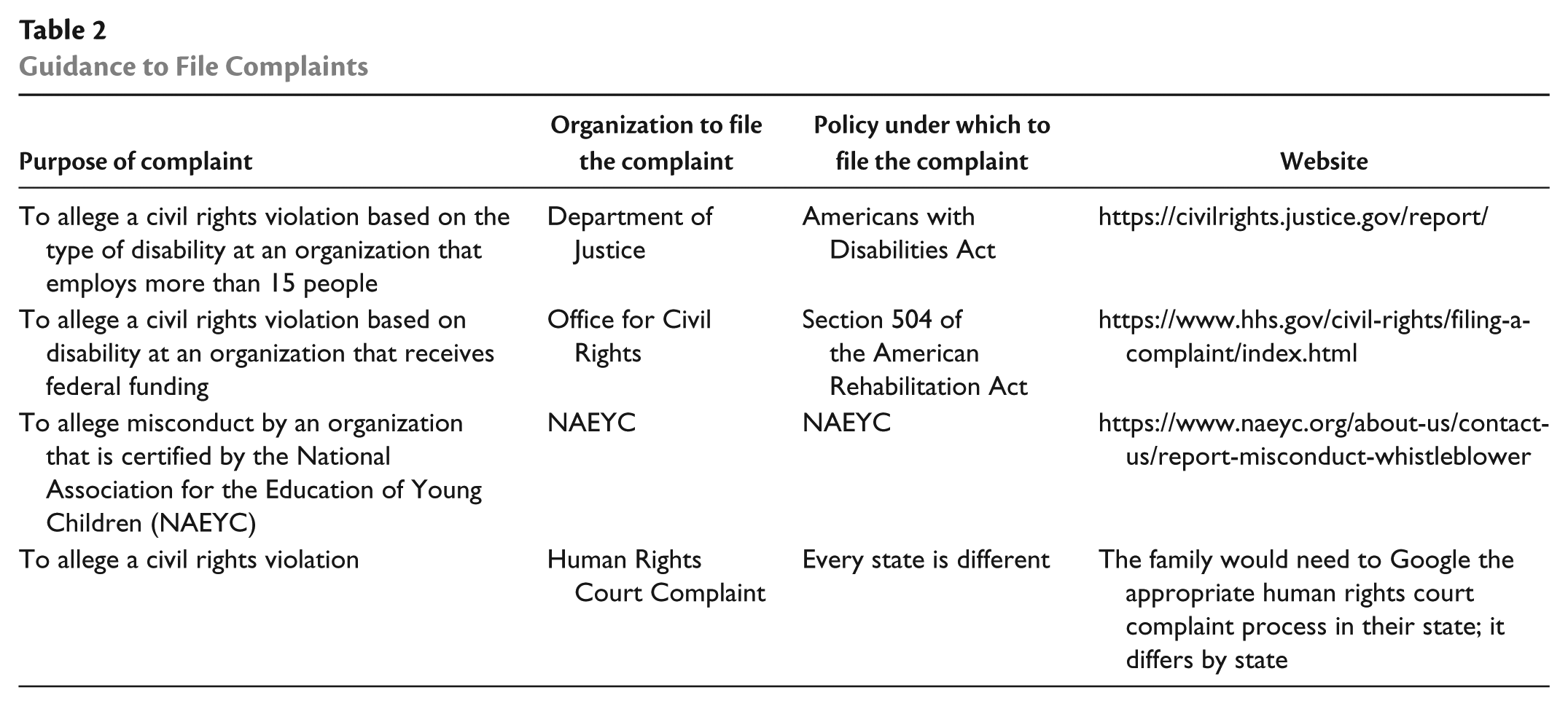
As noted in Molly’s vignette, families often want to seek change not only for their own children with disabilities but also for all families of children with disabilities. Under the ADA, families have the right to file a complaint with the Department of Justice if they feel their child has been discriminated against. Such a complaint could result not only in a fair result for the child (James) but also in system changes at the child care program and within state agencies that regulate child care. Notably, depending on the child care program, there may be other ways to engage in systemic advocacy. For example, if the child care center is housed within a university, the family could also file a complaint at the university. In Table 2, we present other ways for families to file formal complaints, supporting not only individual change but also systemic changes.
Guidance to File Complaints
In addition, at a systems level, teacher preparation programs can also help providers to be prepared to support families’ advocacy skills (Strassfeld, 2019). At a minimum, all within the system can engage in everyday advocacy to “demystify disability” through simple acts, such as language changes (e.g., saying “children with disabilities” instead of “children with special needs”), to help advance a collective shift toward a more inclusive mindset (Ladau, 2021).
Conclusion
It is our hope that families can use the information provided here to advocate to ensure their children and others have access to high-quality child care, regardless of disability status. However, this work should not fall only to families. It is imperative that all members of the early childhood community share the collective responsibility to increase sustained access to inclusive child care. It will take a collective effort to break down silos and work together to “demystify” disability, disrupt deficit narratives and assumptions, and build the competence and confidence of the early childhood workforce in working with young children with disabilities and their families. Ultimately, families of young children with disabilities have the right to access high-quality, inclusive care for their children. All of us in the system must ensure that families are not misinformed, feel defeated or discouraged, or forced to navigate a system that feels as though it is designed to work against them. As our mother participant/author shared:
An additional barrier to new parents or first-time parents of children with disabilities at this young age is simply not knowing where to start with advocacy or what resources are available in general. Early intervention and early childhood services and inclusion are so important, and yet there’s such a narrow window of time, much less time to educate yourself as an advocate.
By working together and advocating for systemic change, we can help improve the early care and education experiences of young children and their families.
Footnotes
Authors’ Note
You may reach Courtney E. O’Grady by email at
Declaration of Conflicting Interests
Jasmine Jones was deceased at the time of of acceptance of the article and the Journal was unable to confirm details of any conflict of interest related to this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.