
Abstract
Introduction:
Left upper quadrant (LUQ) drain use after trauma splenectomy varies, with minimal existing data to guide practice. We aimed to investigate the association of LUQ drains with organ space surgical site infection (OS-SSI) after splenectomy. We hypothesized that LUQ drains after trauma splenectomy are associated with increased odds of OS-SSI.
Patients and Methods:
A retrospective study of adult blunt trauma patients who underwent splenectomy from 7/2018 to 6/2024 was performed. We excluded patients who survived <5 days after operation, and those with an intraoperatively identified pancreatic injury. Demographics, surgical details, and drain information were abstracted from the medical record. Inverse probability of treatment weighting (IPTW) was used to balance variables between patients who did and did not receive an LUQ drain after splenectomy. Multivariable logistic regression with IPTW was performed to estimate the association of LUQ drains with OS-SSI.
Results:
Of 179 patients, 68% (n = 121) were male, the median age was 38 years (interquartile range 28, 55), and 27% (n = 48) received an LUQ drain. Patients with a drain were more likely to be male and overweight. Age, injury severity, use of damage control, and bowel injuries and resections were similar in patients with and without drains. LUQ drains were associated with increased adjusted odds of OS-SSIs (aOR 5.6, 95% confidence interval 1.7–18.3, p ≤ 0.01). Seven patients, all with drains, had a pancreatic fistula (7/48 vs. 0/131).
Conclusion:
LUQ drains after splenectomy for blunt trauma were associated with increased odds of OS-SSIs. Given the high likelihood of unmeasured confounders and the inability to capture surgeons’ complex decision-making in this study, randomized controlled trials are needed to assess the risks and benefits of LUQ drains after splenectomy.
Introduction
The spleen is one of the most commonly injured organs after blunt abdominal trauma, 1 with about 15% of patients with a splenic injury receiving immediate operative intervention. 2 Patients who undergo splenectomy after trauma are usually hemodynamically unstable, have higher organ injury scores, and have concurrent injuries compared with those who undergo nonoperative management. 2 Therefore, splenectomy patients are at higher risk for early infectious complications, such as organ space surgical site infection (OS-SSI), compared with patients undergoing abdominal surgery without splenectomy 3 and patients undergoing nonoperative management of blunt splenic injury.4,5
Surgical site infections (SSIs) are known to increase morbidity, mortality, and healthcare costs. 6 SSI rates tend to be high in the trauma setting since there is no time to optimize trauma patients before surgery, with reported rates of SSI ranging from 15% to 36% after trauma laparotomies.7,8 The use of a left upper quadrant drain (LUQ) after splenectomy has been advocated as a window to detect early postoperative bleeding, infection, and missed injuries. 9 However, intra-abdominal drains have also been associated with pain, ascending infection, incisional hernias, malfunctioning requiring additional procedures, and extended hospital length of stay (LOS).10,11 Although randomized trials of drains have been conducted in elective procedures, no randomized controlled trial (RCT) exists comparing the use of an LUQ drain versus no drain following splenectomy after trauma. Observational studies in patients undergoing splenectomy for a variety of reasons, including for trauma and hematological disorders,9,12 as well as animal studies, 13 have produced conflicting results regarding the benefits and potential harms of drains after splenectomy.
Using statistical methods to reduce selection bias that is inherent in observational cohort studies, this study aims to determine if there is an association between LUQ drain placement after blunt trauma splenectomy and OS-SSIs. The secondary aim of this study is to compare the LOS of patients who received an LUQ drain versus those who did not. We hypothesized that LUQ drains after trauma splenectomy are associated with an increased risk of OS-SSIs and longer LOS. Results can be used to inform future randomized trials.
Patients and Methods
A retrospective review of adult blunt trauma patients (≥16 y old) who underwent splenectomy from July 2018 to June 2024 at a level 1 trauma center was performed. The following International Classification of Diseases 10th edition codes were used to identify patients who suffered a blunt splenic injury due to trauma in our trauma laparotomy database: S36.020A, S36.021A, S36.030A, S36.031A, S36.032A, S36.029A, S36.039A, and S36.00XA. Since death is a competing outcome with OS-SSI, and the earliest documented OS-SSI occurred at 5 days, all patients who survived less than 5 days after index laparotomy were excluded. 8 In addition, all patients diagnosed with a pancreatic injury intraoperatively were excluded since they all received an LUQ drain as part of their management.
The primary outcome of the study was the rate of OS-SSI after blunt trauma splenectomy. OS-SSI was defined based on the criteria set by the Centers for Disease Control and Prevention. 6 We selected OS-SSI as the primary outcome, as these SSIs are linked to significantly higher morbidity and mortality compared with superficial and deep SSIs. 14 In addition, OS-SSIs are well-documented in the medical record and can be more easily identified using multiple sources, including progress notes, imaging studies, procedure notes, and anesthesia records. The secondary outcome of the study was hospital LOS.
Basic demographic information, Injury Severity Scores (ISSs), emergency department (ED) vital signs, administration of preoperative antibiotics, number of units of red blood cells given in the operating room (OR-RBC), intraoperative details, LUQ drain placement, OS-SSI status, and LOS were obtained from the patient’s medical records. Additional information collected included the development of a pancreatic fistula, which was defined by a body fluid amylase level three times that of the serum amylase level. 15 Pancreatic fistulas were also graded based on their severity. Grade A, or a biochemical leak, is diagnosed based on elevated body fluid amylase levels in the absence of a clinical impact on the patient. Grade B refers to a fistula requiring a change in postoperative management, such as leaving a drain in place for >3 weeks or repositioning of the drain. Grade C refers to a pancreatic fistula that required reoperation. 15 One team member (M.O.F.) verified the accuracy of the collected data.
Missing data were minimal, <1%. Preliminary bivariate analysis was performed for categorical variables using Chi-Square or Fisher exact test, Exact Test. We used a two-tailed t-test or Mann-Whitney U test for continuous variables to assess factors associated with OS-SSI after blunt trauma splenectomy.
To balance baseline characteristics and reduce the bias of the estimated treatment effect between patients who received a drain and those who did not, we performed a propensity score analysis 16 with nonparametric generalized boosted models (GBMs) for flexible estimation on all patients who met inclusion criteria. 17 Patients were grouped by drain or no drain placement before the closure of their abdominal fascia after trauma splenectomy, and a GBM was fitted to this treatment variable to estimate the propensity score of the patients. We adjusted the GBM model until the differences between patients who received a drain and those who did not were as small as possible.
The following variables were specified a priori and included in the propensity score model: age, gender, body mass index (BMI), damage control laparotomy (DCL), wound class, ISS, emergency room vitals (pulse and systolic blood pressure), units of OR-RBC, large bowel resection, small bowel resection, full-thickness small bowel injury, and full-thickness large bowel injury.
The baseline characteristics between patients with and without a drain were evaluated using a threshold of 0.2 for standardized mean difference. An inverse probability of treatment weighted (IPTW) adjusted sample was generated from the propensity score model, achieving a balance of baseline variables of interest between patients who received an LUQ drain and those who did not. A multivariable logistic regression model was performed on the IPTW-adjusted sample to estimate the effect of LUQ drain placement after blunt trauma splenectomy on the odds of developing an OS-SSI and the impact on LOS. Statistical significance was defined by a p value <0.05. In addition, the G-computation method 18 was used to calculate the marginal risk difference in OS-SSI between two counterfactual scenarios: one where all patients received a drain versus one where none received a drain. R Studio version 2024.04.1 + 748 was used for the statistical analysis.
UTHealth Houston Institutional Review Board and Memorial Hermann approved this study and waived informed consent. This study was performed in compliance with the Health Insurance Portability and Accountability Act.
Results
A total of 179 patients met the inclusion criteria (Fig. 1); 68% (n = 121) were male, and the median age was 38 years (interquartile range [IQR]: 28, 55). Of the included patients, 27% (n = 48) received an LUQ drain (Table 1).
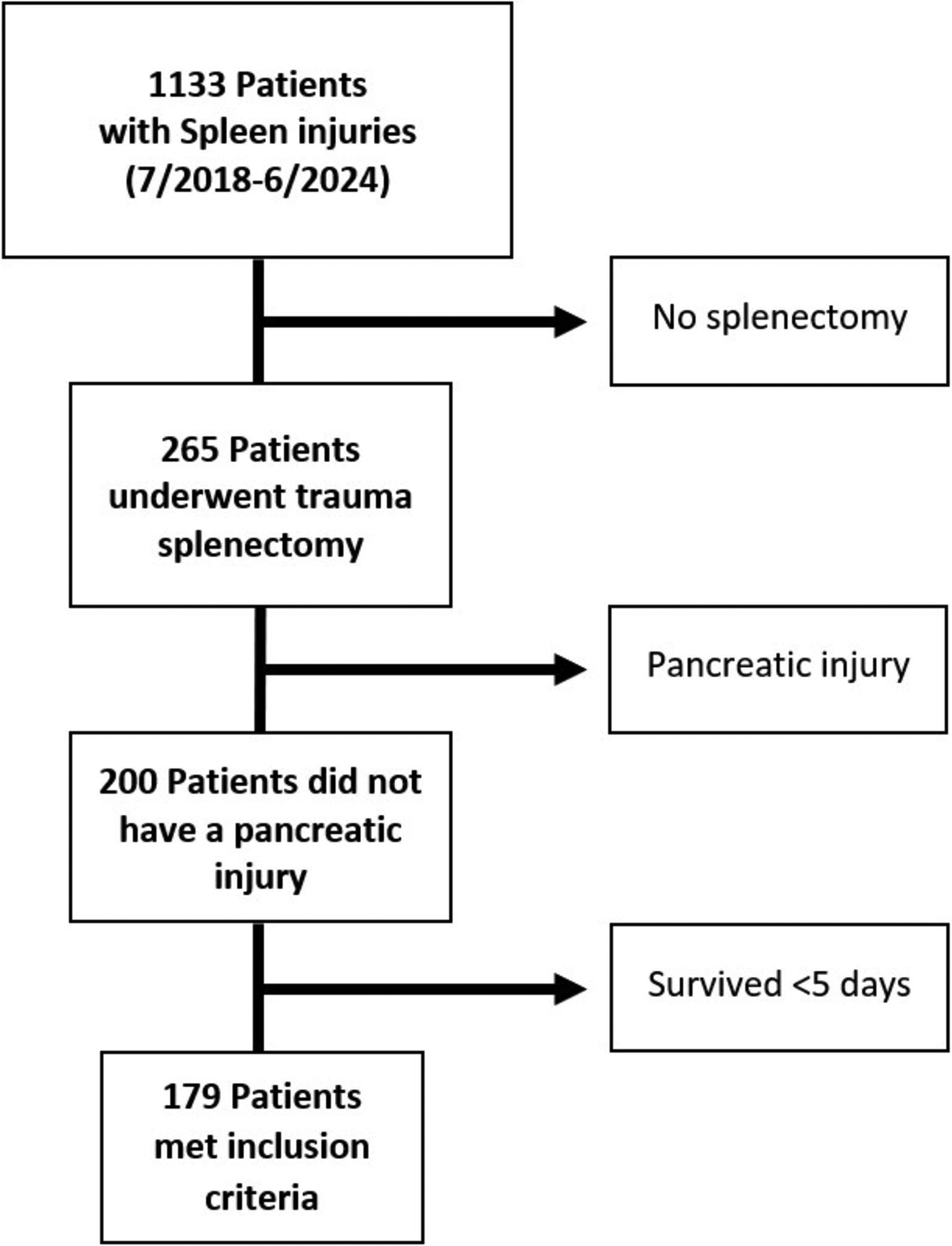
Patient population flowchart. A total of 179 patients underwent trauma splenectomy, had no associated pancreatic injury, and survived for at least five days after the index operation.
Patients’ Characteristic
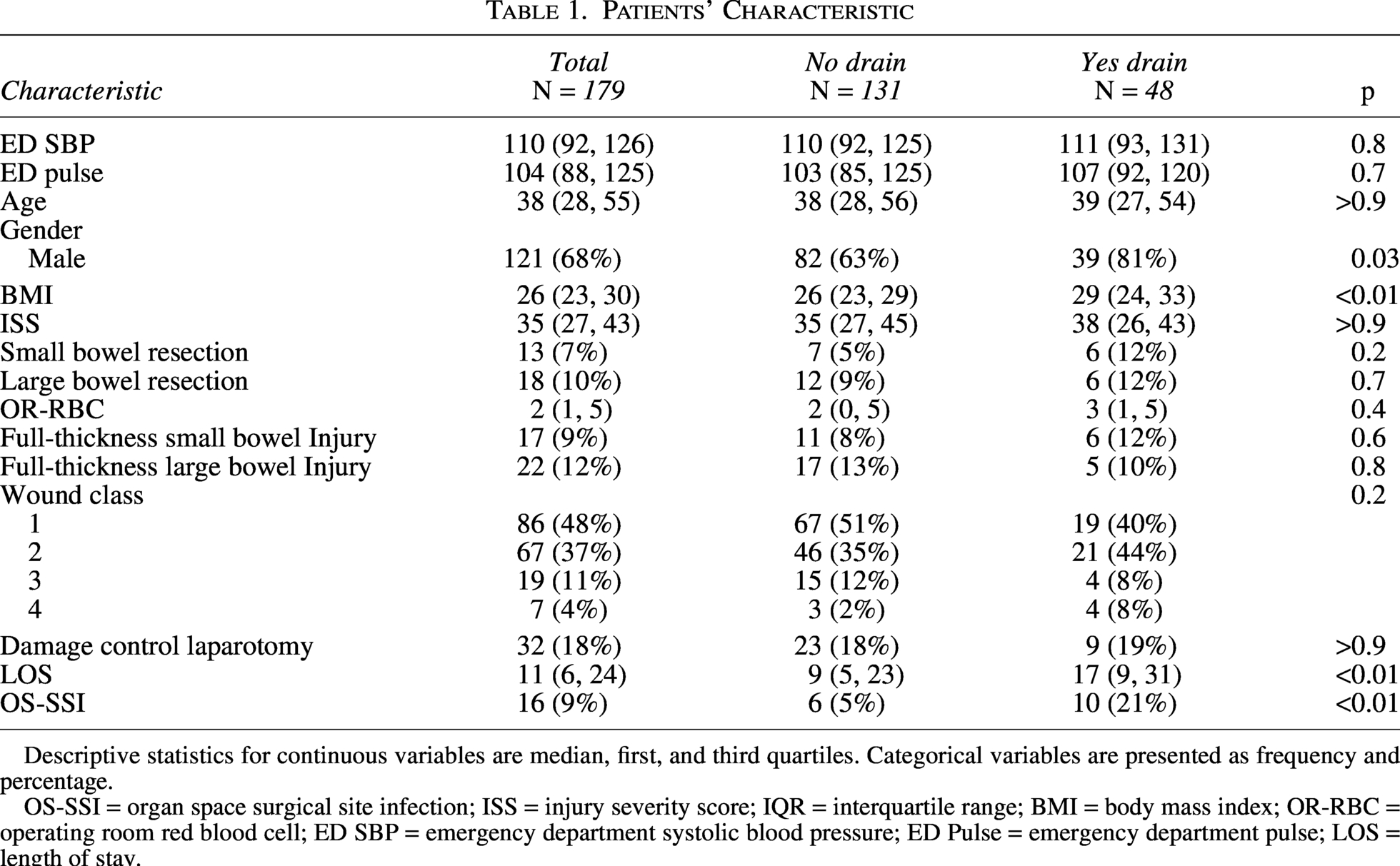
Descriptive statistics for continuous variables are median, first, and third quartiles. Categorical variables are presented as frequency and percentage.
OS-SSI = organ space surgical site infection; ISS = injury severity score; IQR = interquartile range; BMI = body mass index; OR-RBC = operating room red blood cell; ED SBP = emergency department systolic blood pressure; ED Pulse = emergency department pulse; LOS = length of stay.
Patients with a drain versus no drain
Patients with and without a drain were similar in ED vitals, age, ISS, rates of bowel injury and resection, and receipt of DCL (Table 1). Of all the included patients, 98% (176/179) had documented administration of preoperative prophylactic antibiotics. Of the patients with an LUQ drain, 71% (34/48) received cefazolin or cefoxitin as a preoperative antibiotic versus 84% (110/131) of patients without an intraoperative placed drain (p = 0.05). On univariable analysis, patients who received an LUQ drain were more likely to be male and had a higher BMI. There was no difference in wound class between patients with and without a drain. In addition, patients with a drain had a higher rate of OS-SSI (21% [N = 10] vs. 5% [N = 6], p ≤ 0.01) and had a longer LOS (17 [9, 31] vs. 9 [5, 23], p < 0.01) compared with patients without a drain. Of the 48 patients who received an LUQ drain, 41 had their drain in place for a median time of 10 days (IQR: 6, 17) with removal prior to discharge. One patient died before their drain was removed, and six patients were discharged with a drain, but no clinic record of drain removal was found.
A review of patients’ operative notes was performed. Among the 48 patients who received an LUQ drain, documentation cited concern for a missed pancreatic injury as the reason for drain placement in 15% (7/48) of patients. The remaining operative notes did not provide a rationale for drain placement.
Patients with an OS-SSIs
A total of 16 (9%) patients developed an OS-SSI. Ten of these patients had a surgically placed LUQ drain, of whom 4 underwent an additional operation and 6 required an additional drain placed by interventional radiology to treat their OS-SSI. Of the 131 patients without an LUQ drain, 6 (5%) developed an OS-SSI, of whom 2 required a return to the operating room, and 4 patients had an LUQ drain placed by interventional radiology. Among patients with OS-SSIs, 50% of patients in both the drain (5/10) and no drain groups (3/6) underwent procedures categorized as wound class 3 or 4.
The IPTW model achieved a balance between covariates with a threshold of 0.2 on standardized mean differences, except for gender (Fig. 2). Therefore, this variable was incorporated into our multivariable regression model, making the model double robust. On multivariable logistic regression analysis incorporating the IPTW, patients with an LUQ drain were associated with 5.6 times higher odds of developing an OS-SSI compared with patients without an LUQ drain (OR: 5.6, 95% confidence interval [CI]: 1.7–18.3, P ≤ 0.01) (Table 2). Using G-computation, the marginal average probability of developing an OS-SSI was 19.5% when all patients received a drain, as compared with 4.5% when none of the patients received a drain, resulting in a risk difference of 15% (Standard Error [SE] = 6.56%, 95% CI = 2.1%-27.8%, p = 0.02).
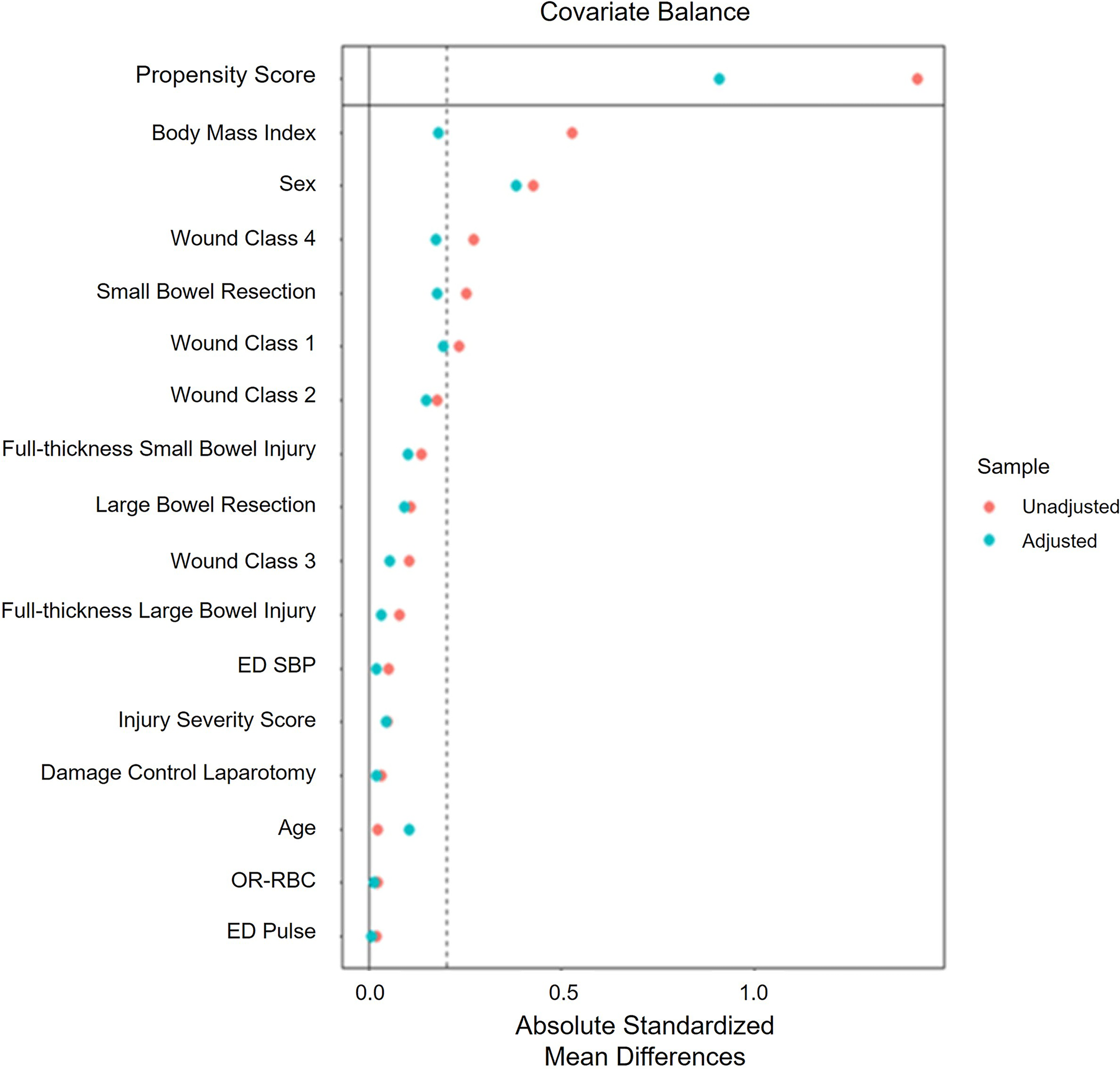
An inverse probability of treatment weighting (IPTW) model achieved a balance between covariates with the threshold of 0.2 on standardized mean differences except for gender. ED SBP = emergency department systolic blood pressure; OR-RBC = operating room red blood cell; ED Pulse = emergency department pulse.
Multi-Variable Logistic Regression Analysis for Organ Space Surgical Site Infection Incorporating the Inverse Probability of Treatment Weighting Model
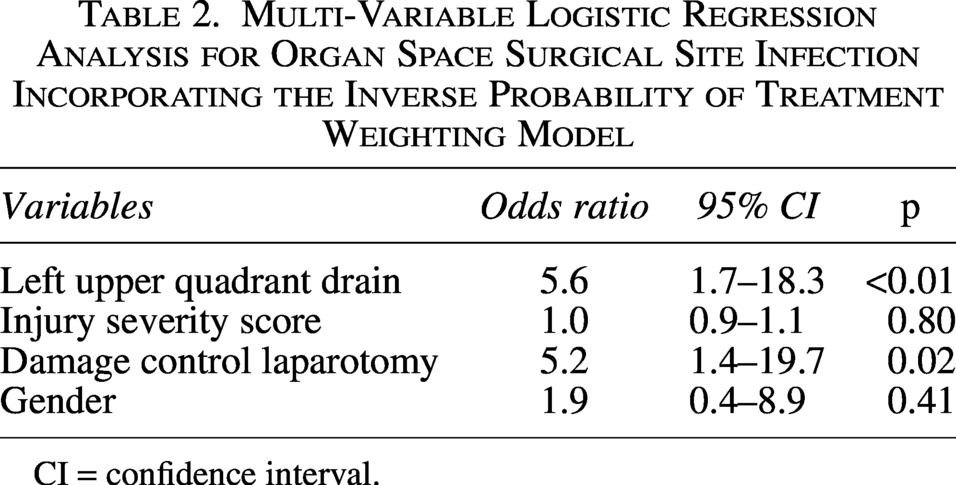
CI = confidence interval.
Culture data
Of the 16 patients that developed an OS-SSI, at least one organism was isolated from 10 (63%) patients with positive cultures, and 3 patients grew more than one organism. There was 1 gram-positive bacterium, Enterococcus species. There were 8 different gram-negative bacterial species: Klebsiella pneumoniae, Acinetobacter baumannii, Enterobacter cloacae, Pseudomonas aeruginosa, Enterobacter aerogenes, Serratia marcescens, Proteus mirabilis, and Escherichia coli, which was the most commonly isolated organism. In addition, 4 (25%) patients did not have a good window to drain their abscess, 1 (6%) patient did not grow anything in their culture, and 1 (6%) patient did not have cultures taken.
Pancreatic fistulas
A total of 25 of the 48 patients (52%) who had an LUQ drain also had a drain amylase level obtained before drain removal. On the basis of the drain amylase to body fluid level, 7 patients were diagnosed with a pancreatic fistula (4% of the overall cohort). Two patients had a Grade A fistula (biochemical leak), 3 had a Grade B fistula, and 2 patients were sent home with their initial drain in place, but no clinic record of drain removal was found. In addition, 3 out of 7 (43%) patients with a pancreatic fistula were also found to have an OS-SSI, for which they required an additional drain placement by interventional radiology for its treatment. No patients in our cohort required an invasive procedure to treat their pancreatic fistula.
Length of hospital stay
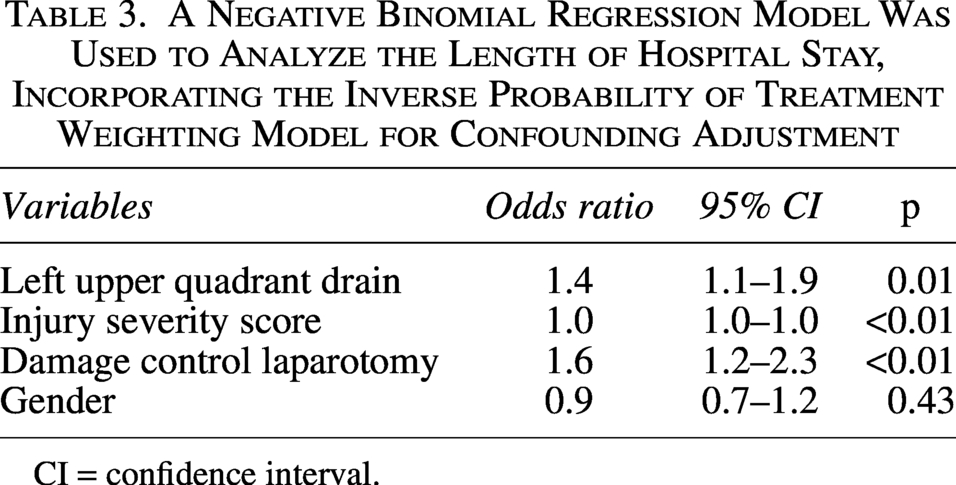
A negative binomial regression model was used to analyze the length of hospital stay, incorporating the IPTW model for confounding adjustment. LUQ drains were associated with a 40% increase in LOS compared with no drains (risk ratio 1.4, CI: 1.1–1.9, p = 0.01) (Table 3). Using G-computation, the average estimated LOS was 22 days if all patients received an LUQ drain, compared with 15 days if no patients received an LUQ drain. The yielded marginal average treatment effect was 7 days (SE = 2.9 d, 95% CI: 1 d–12 d, p = 0.02).
A Negative Binomial Regression Model Was Used to Analyze the Length of Hospital Stay, Incorporating the Inverse Probability of Treatment Weighting Model for Confounding Adjustment
CI = confidence interval.
Discussion
In a single institutional analysis, LUQ drains were placed after splenectomy for blunt trauma in one out of every four cases. After adjusting for known potential confounders, LUQ drains were associated with increased OS-SSIs and longer LOS. Although the use of advanced statistical methods such as IPTW can decrease bias related to known confounders, unknown confounders may still bias the results. Observational cohort studies can only determine association, while randomized trials are required to evaluate for causation. This study was unable to account for complex surgical decision-making, which likely incorporated clinical suspicion for a pancreatic injury, as noted from the review of operative notes and the identification of pancreatic fistulas only in patients with drains. Out of the entire cohort, a total of 4% of patients (n = 7) were diagnosed with a pancreatic fistula, but none of them required an invasive procedure for its treatment, such as endoscopic retrograde cholangiopancreatography (ERCP) or reoperation.
The literature is conflicting regarding whether LUQ drains after splenectomy are associated with OS-SSIs. In some clinical and animal studies, LUQ drains have been associated with an increased risk of OS-SSIs.12,13 Cohn et al. performed a study on patients undergoing splenectomy due to trauma, hematological disorders, and portal hypertension. They reported a higher rate of subphrenic abscesses (18.5% vs. 0%) in patients who received a drain after splenectomy versus those who did not receive a drain. 12 Other studies have not found an increased risk of SSI with drains. For example, Mohseni et al. performed a study on patients undergoing emergency trauma laparotomy for isolated solid organ injury, including the spleen. They found that intraabdominal drains were not associated with SSIs. However, only 50% (n = 62) of the included patients underwent splenectomy, of whom 58% received a drain. Therefore, the study might have been underpowered to detect a difference. 19 The inclusion of polytrauma patients in our study population, rather than just isolated splenic injury patients, increases the generalizability of our findings compared with this study. In another study, Vecchio et al. 9 reported that drain placement after elective open and laparoscopic splenectomy was not associated with infectious complications. Notably, their study excluded emergency and trauma operations, and 90% of the splenectomy drains were removed within 3 days of surgery compared with our patient population, which had their drains for a median time of 10 days (IQR: 6, 17). While we found no studies comparing early versus late removal of LUQ drains after splenectomy, a RCT by Bassi et al. investigating this topic after pancreatic resection showed a decreased rate of pancreatic fistulas (2% vs. 26%, p ≤ 0.001) and abdominal complications (12% vs. 53%, p = 0.001) with early drain removal (postoperative day 3 vs. 5 or later). 20
Several mechanisms have been proposed for why drains may be associated with a higher rate of OS-SSIs. Drains may increase the risk of infection by allowing retrograde bacterial migration; for example, pathogenic bacteria may migrate up the drain track into the peritoneal cavity. 13 Bacteria can adhere to the surface of a drain and form a biofilm, which makes bacteria resistant to antibiotics. 21 Drains can also cause a foreign body reaction, altering local immune activity. 22 In addition, drains can become clogged, providing ideal conditions for bacteria to grow. 23
The most common reason why surgeons left a drain after blunt trauma splenectomy in our cohort was for splenic fossa drainage and due to concern for a missed pancreatic injury. The Eastern Association for the Surgery of Trauma (EAST) has no recommendations for or against intraoperatively placed drains to treat Grade I/II pancreatic injuries. 24 Furthermore, studies have suggested that drains near the pancreas may irritate it and cause a fistula. 25 An RCT of drain versus no drain after pancreatoduodenectomy and distal pancreatectomy showed that patients who received a drain had an increased incidence of intra-abdominal abscess and pancreatic fistula formation. 25 In our study, 4% (7/179) of patients were diagnosed with a pancreatic fistula, all Grade A or B. Patients with Grade A fistulas have been shown to have similar outcomes to those without a fistula,16,26 and those patients with a Grade B fistula, in our cohort, experienced persistent drainage for more than 3 weeks. 16 However, none of the patients with a pancreatic fistula required invasive procedures such as ERCP or surgery. In addition, since all of the patients with a pancreatic fistula had a drain, it is unknown whether these fistulas would have been diagnosed in the absence of a drain.
Currently, there is no protocol for the placement or management of drains after trauma splenectomy at our institution, and both are currently based on surgeon preference. The criteria for drain removal vary; some surgeons rule out biochemical leaks before drain removal, while others decide based on volume output. It remains unclear whether the presence of a drain or late removal of a drain is associated with the increased risk of OS-SSI and pancreatic fistulas in our population. In addition, all 7 pancreatic fistulas occurred in patients who had LUQ drains; this might indicate that surgeons were correctly identifying high-risk cases for drain placement based on intra-operative judgment not captured in statistical models.
The limitations of this study are those associated with its sample size, retrospective design, data availability, and accuracy. Due to the small sample size, the estimates of association between drains and OS-SSIs had wide confidence intervals and were imprecise. To account for multiple confounders and the small sample size, we used propensity scores and IPTW to adjust for differences between patients who received an LUQ drain and those who did not. However, as with any observational study, there may be residual confounding and selection bias. Statistical methods cannot capture the complexity of surgeon decision-making. In addition, patients with pancreatic injuries were identified and excluded based on the postoperative diagnosis or procedure list dictated in the operative note. Therefore, if a surgeon failed to list pancreatic injury as part of their postoperative diagnosis, that patient might have been included in this study. We do not have details regarding the sterility and frequency of drain care, which could have affected the drain’s risk of clogging and bacterial migration.
Conclusion
This single-center study showed that leaving an LUQ drain after splenectomy for blunt trauma is associated with an increased risk of OS-SSI and LOS. Although leaving a drain may identify patients with previously unsuspected pancreatic injury, these injuries were few and minor in severity in this study. They may not have been diagnosed if a drain had not been in place. However, even though we used IPTW to balance variables between patients who did and did not receive an LUQ drain after splenectomy, there still are variables that we did not account for that might have influenced the surgeon’s decision to leave a drain. Therefore, a RCT comparing LUQ drain versus no drain is needed to quantify the risks and benefits of splenic fossa drainage after splenectomy for blunt trauma.
Authors’ Contributions
S.M.U.: Conceptualization, methodology, investigation, data curation, formal analysis, validation, writing original draft, and writing—reviewing and editing; M.O.F.: Data curation, investigation, and writing—reviewing and editing; W.D.R.: Data curation, investigation, and writing—reviewing and editing; R.W.G.: Data curation, investigation, and writing—reviewing and editing; S.K.: Data curation, formal analysis, validation, visualization, and writing—reviewing and editing; G.E.H.: Data curation, formal analysis, validation, visualization, and writing—reviewing and editing; L.S.K.: Conceptualization, methodology, investigation, supervision, writing-original draft, and writing—reviewing and editing.
Footnotes
Author Disclosure Statement
No authors declare any other conflicts of interest.
Funding Information
This work was supported by the National Institutes of Health (T32GM008792). The sponsor had no role in the study design, collection, analysis, data interpretation, report writing, or the decision to submit the article for publication.
Data Availability Statement
Data will be available upon request and in compliance with institutional policy.