
Abstract
To the Editor:
A 13-year-old girl presented to our hospital with a one-month history of swelling on the left side of her neck. Neck examination showed multiple non-tender lymphadenopathies from the left cervical region to the supraclavicular area. Blood tests revealed a WBC count of 4.22 × 109/L, an ESR of 92 mm/h, and a C-reactive protein level of 21.4 mg/L. The HIV test was negative. A contrast-enhanced computed tomography scan of the neck demonstrated an abscess-like mass within the subcutaneous and muscular tissues on the left side of the neck, extending toward the left supraclavicular region and measuring 3.5 cm × 4 cm. The patient was administered intra-venous ampicillin-sulbactam and clindamycin. The ear, nose, and throat (ENT) team drained the abscess, and no growth was detected in the abscess culture. An image-guided fine-needle aspiration biopsy was performed. Because of inadequate clinical improvement despite antibiotic therapy, an interferon-gamma release assay test was performed, which was positive. Repeat abscess drainage was performed by the ENT team, and the specimen tested positive for tuberculosis (TB) by polymerase chain reaction. The pathology report of the cervical lymph node specimen revealed necrotizing granulomatous lymphadenitis. The patient was initiated on standard anti-TB treatment (isoniazid, rifampin, pyrazinamide, and ethambutol).
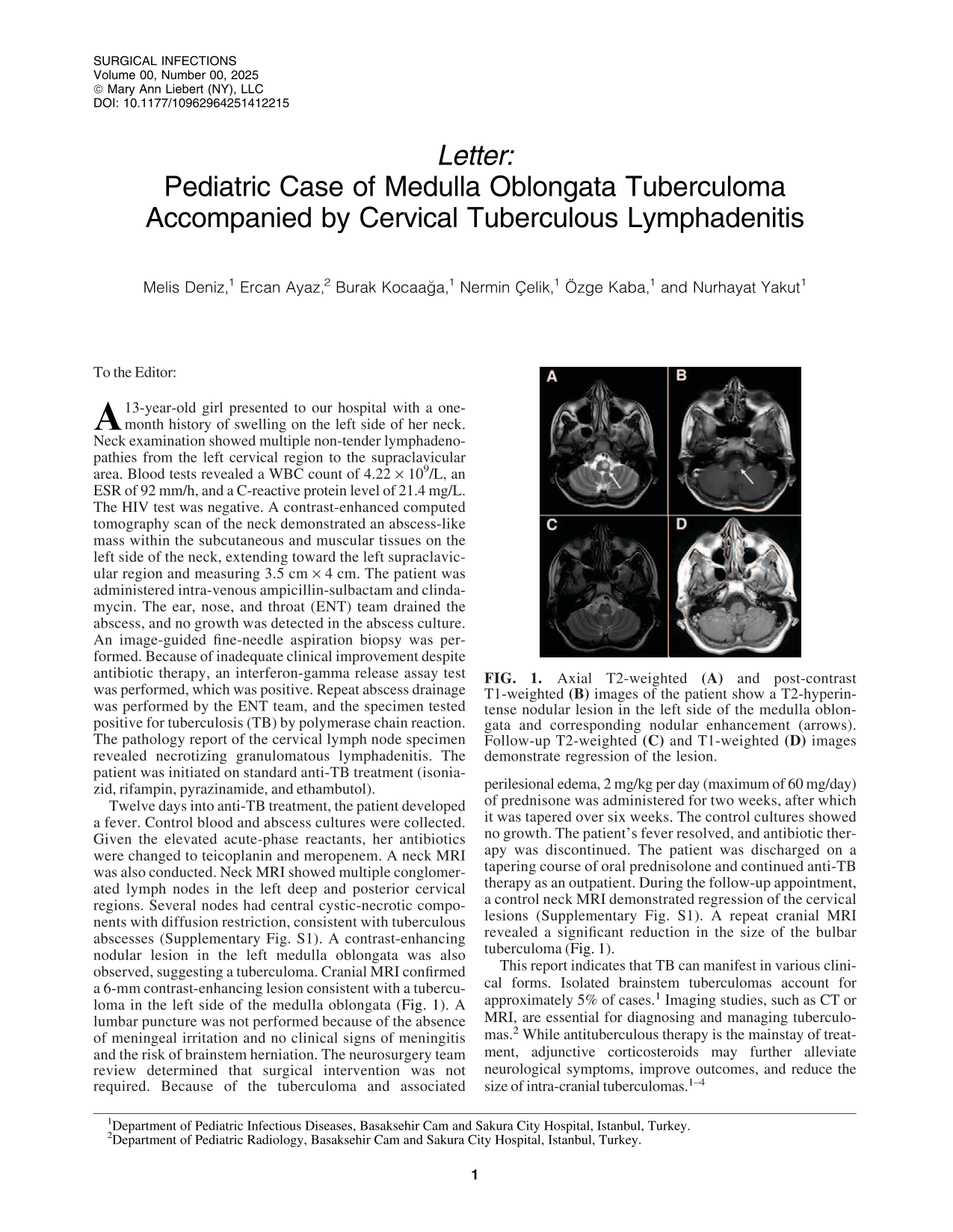
Twelve days into anti-TB treatment, the patient developed a fever. Control blood and abscess cultures were collected. Given the elevated acute-phase reactants, her antibiotics were changed to teicoplanin and meropenem. A neck MRI was also conducted. Neck MRI showed multiple conglomerated lymph nodes in the left deep and posterior cervical regions. Several nodes had central cystic-necrotic components with diffusion restriction, consistent with tuberculous abscesses (Supplementary Fig. S1). A contrast-enhancing nodular lesion in the left medulla oblongata was also observed, suggesting a tuberculoma. Cranial MRI confirmed a 6-mm contrast-enhancing lesion consistent with a tuberculoma in the left side of the medulla oblongata (Fig. 1). A lumbar puncture was not performed because of the absence of meningeal irritation and no clinical signs of meningitis and the risk of brainstem herniation. The neurosurgery team review determined that surgical intervention was not required. Because of the tuberculoma and associated perilesional edema, 2 mg/kg per day (maximum of 60 mg/day) of prednisone was administered for two weeks, after which it was tapered over six weeks. The control cultures showed no growth. The patient’s fever resolved, and antibiotic therapy was discontinued. The patient was discharged on a tapering course of oral prednisolone and continued anti-TB therapy as an outpatient. During the follow-up appointment, a control neck MRI demonstrated regression of the cervical lesions (Supplementary Fig. S1). A repeat cranial MRI revealed a significant reduction in the size of the bulbar tuberculoma (Fig. 1).
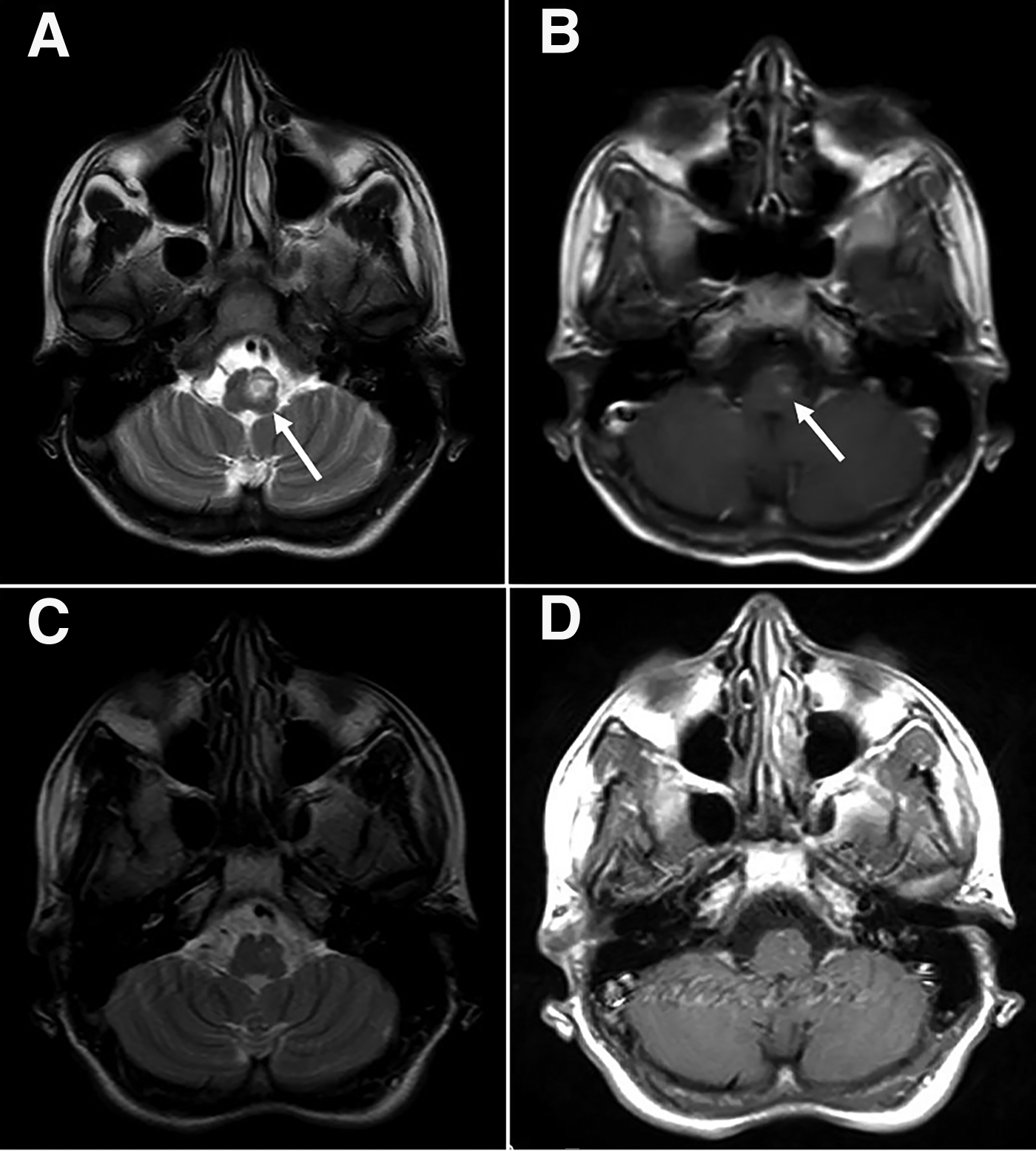
Axial T2-weighted
This report indicates that TB can manifest in various clinical forms. Isolated brainstem tuberculomas account for approximately 5% of cases. 1 Imaging studies, such as CT or MRI, are essential for diagnosing and managing tuberculomas. 2 While antituberculous therapy is the mainstay of treatment, adjunctive corticosteroids may further alleviate neurological symptoms, improve outcomes, and reduce the size of intra-cranial tuberculomas.1–4
Footnotes
Acknowledgments
The authors thank the staff and Basaksehir Cam and Sakura City Hospital for their assistance.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.