
Abstract
Introduction:
Facial fractures account for over 400,000 emergency department visits annually in the United States. They are managed operatively, non-operatively, or via observation with diet and activity modification. Regardless of management, antibiotic agents are commonly prescribed. The Surgical Infection Society (SIS) published the 2020 guidelines limiting antibiotic agent use to the peri-operative period.
Methodology:
We performed a retrospective chart review to evaluate antibiotic agent prescribing practices for patients with isolated facial fractures at an academic level-one trauma center. We assessed potential antibiotic agent days saved by adhering to SIS guidelines. Patients 18 and older presenting to the trauma service with a facial fracture from January 2019 to August 2024 were identified from the trauma registry. Patients with clear antibiotic agent indications (e.g., open fractures) were excluded. Descriptive and chi-square analyses were used.
Results:
The number of potentially saved antibiotic agent days was 495. Of 119 patients, 89.1% received antibiotic agents, 57.6% at least twice. A total of 80.2% of antibiotic agents given were against SIS recommendations. The antibiotic agent administration rate for mandibular fractures was 97%. Operative management accounted for 93.2% of cases. Antibiotic agent use did not significantly differ between operative and non-operative management (p = 0.18) or between open and closed operative cases (p = 0.99). In operative cases, appropriate peri-operative antibiotic agents were used 89.9% of the time, with 47.5% pre-operative and 63.6% post-operative non-guideline use. Segmented logistic regression showed no statistically significant reduction in non-guideline antibiotic agent use after the guidelines were published. The 30-day post-operative surgical site infection rate was 3.4%, with no significant difference between guideline and non-guideline use.
Conclusion:
There is substantial discordance between real-world antibiotic agent prescribing practices and SIS guideline recommendations for facial fractures. Quantifying excess non-guideline antibiotic agent use highlights an important opportunity for antimicrobial agent stewardship and provides a foundation for future quality improvement initiatives.
Keywords
Introduction
Facial fractures are among the most common traumatic injuries worldwide, with an estimated global incidence of 10.7 million cases in 2019. In the United States alone, they account for more than 400,000 emergency department visits annually. 1 These injuries include upper face, mid-face, and mandibular fractures, the latter being the most prevalent. Management strategies range from operative to non-operative approaches; however, antibiotic agents are frequently prescribed regardless of management tactic, often without a clear indication. In the absence of standardized protocols, antibiotic agent prescribing practices for facial fractures vary widely across institutions, contributing to substantial overuse.2–6 This is particularly concerning given that unnecessary antibiotic agent exposure is associated with avoidable complications, including Clostridioides difficile infection, renal toxicity, allergic reactions, and the broader public health threat of antimicrobial agent resistance, which was associated with an estimated 1.27 million deaths worldwide in 2019. 7 These considerations underscore the importance of antibiotic agent stewardship in facial trauma care.
In contrast to facial fractures, open extremity fractures—particularly tibial fractures—have well-established antibiotic agent guidelines because of the high risk of infection, with reported infection rates approaching 18%. 8 Evidence-based recommendations, such as those from the Eastern Association for the Surgery of Trauma, have standardized antibiotic agent timing and duration in these injuries and improved outcomes. 4 Facial fractures, however, have historically lacked uniform guidance because infection risk varies by fracture location, sinus involvement, and whether fractures are open or closed.2–6 To address this gap, the Surgical Infection Society (SIS) published guidelines in 2020 recommending against routine antibiotic agent use in non-operative facial fractures and limiting antibiotic agent administration to the peri-operative period for operative cases. 9 Accordingly, this study evaluates the current antibiotic agent prescribing practices for isolated facial fractures at the Henry Ford Hospital, a quaternary regional academic level-one trauma center, to determine the extent of discordance with SIS guideline recommendations and to quantify the potential reduction in antibiotic agent exposure if these guidelines were followed.
Patients and Methods
Study design
We conducted a retrospective chart review of the patients who presented with isolated facial fractures to the Henry Ford Hospital from January 2019 to August 2024. Data were recorded from the hospital’s trauma registry, and patients were manually screened for the eligibility criteria.
Eligibility criteria
Inclusion criteria consisted of patients aged 18 and older with isolated facial fractures admitted to the trauma service. Exclusion criteria included patients with open fractures and complex lacerations. Facial lacerations and open fractures were identified and excluded using the International Classification of Diseases, Tenth Revision diagnosis codes recorded in the trauma registry.
Data collection
Data on patient demographics, fracture location (upper face, mid-face, or mandibular), management type (operative vs. non-operative), and antibiotic agent use were extracted from the hospital’s trauma registry. The timing of antibiotic agent administration was classified as follows:
Pre-operative: Given more than one hour before operation. Peri-operative: Administered within one hour before operation to 24 hours post-operatively. Post-operative: Administered more than 24 hours after operation.
These definitions reflect the 2020 SIS guidelines, which were used as the reference standard for determining guideline concordance in this study.
The primary outcome was the total number of antibiotic agent days used. Secondary outcomes included antibiotic agent use between fracture types, surgical approaches, non-guideline antibiotic agent use, non-guideline antibiotic agent days, surgical site infection, and C. difficile infection rates.
Our follow-up for complications, including surgical site infections and C. difficile infections, was conducted for 30 days post-operatively. Surgical site infections were identified using trauma registry parameters defined according to the National Trauma Data Bank standards, defined as an infection involving the skin or subcutaneous tissue occurring within 30 days of the operative procedure and documented during the index hospitalization.
Statistical analyses
Descriptive statistics were used for quantitative data, and chi-square tests were performed for categorical variables to compare the differences between operative and non-operative groups as well as pre- and post-operative antibiotic agent use. A p value of <0.05 was considered significant. Fisher exact test was used to compare categorical variables when expected cell counts were less than 5.
To evaluate temporal trends in non-guideline antibiotic agent use before and after publication of the SIS guidelines, we conducted a segmented logistic regression analysis. Patients were classified as presenting before or after guideline publication, and a binary outcome variable indicated whether non-guideline antibiotic agent use occurred. Time, defined as the number of days before the start of the study, was included as a continuous covariate to assess overall prescribing trends. An interaction term between time and guideline period was included to evaluate whether the slope of non-guideline antibiotic agent use changed following guideline publication. No formal guideline implementation strategies, educational interventions, or provider-level feedback mechanisms were undertaken during the study period; therefore, guideline publication itself was treated as the sole intervention in the analysis.
Results
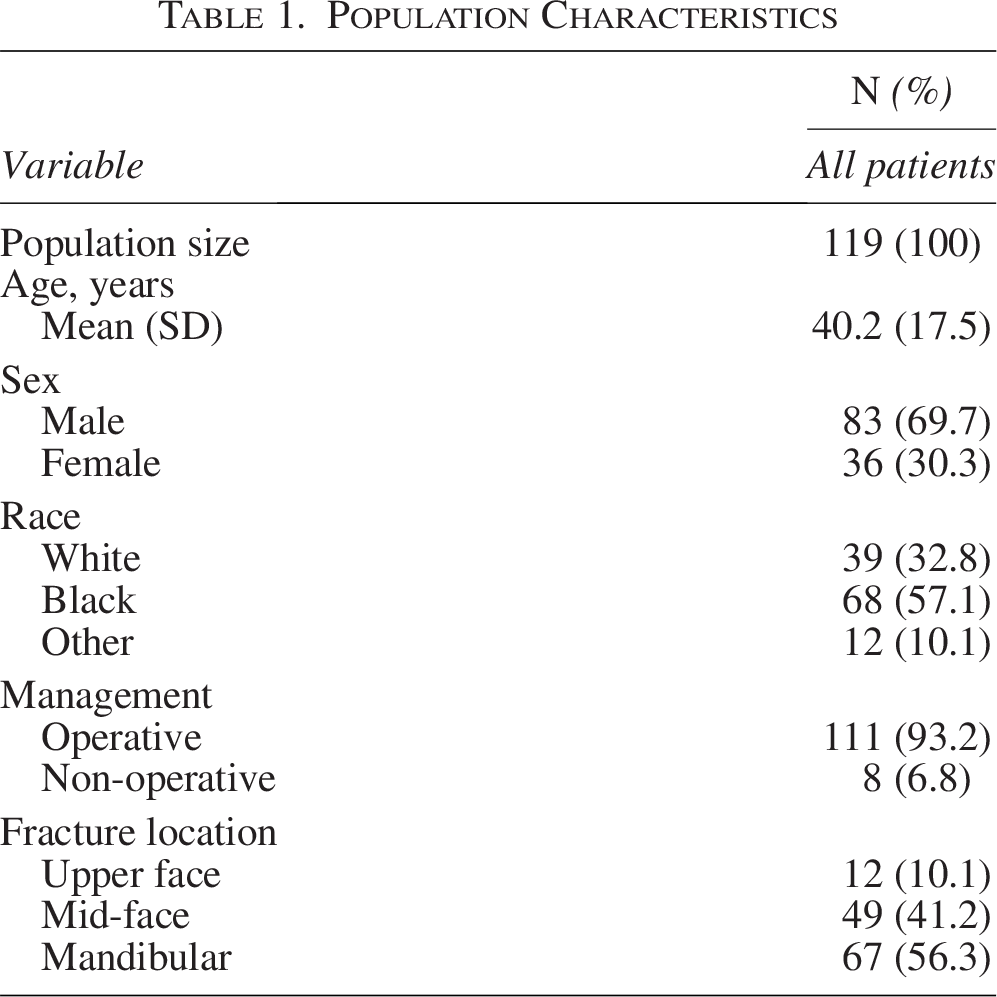
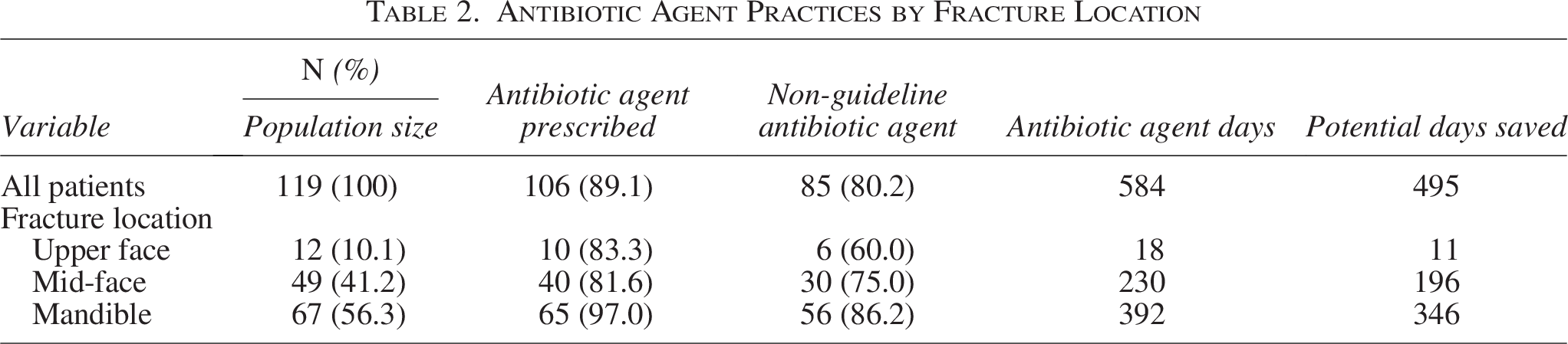
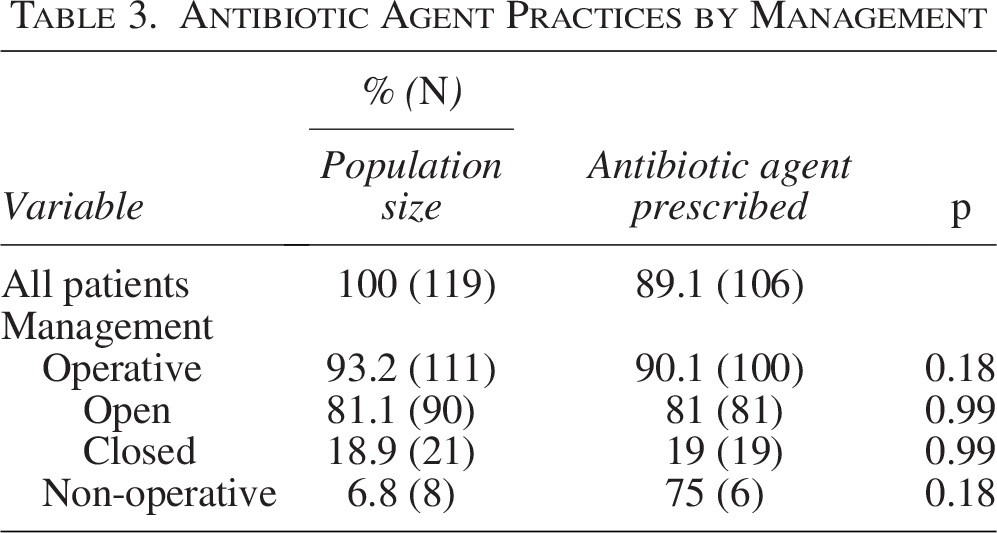
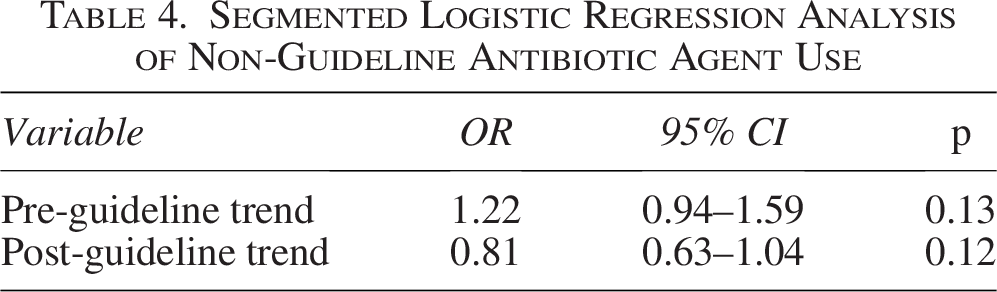
A total of 119 patients met the eligibility criteria (Fig. 1). The mean age of our cohort was 40.2 (17.5) years, with 69.7% being male (Table 1). The most prevalent fracture locations were the mandible (49.6%) and the mid-face (41.2%) (Table 1). The total number of antibiotic agent days given was 584, with a mean of 4.9 days per patient (Table 2). Non-guideline antibiotic agents were administered in 495 antibiotic agent days. A total of 89.1% of our patients received antibiotic agents, with 57.6% receiving at least two (Table 2). The majority of these prescriptions were given against the SIS recommendations (80.2%) (Table 2). The antibiotic agent administration rate for mandibular fractures was the highest (97%) (Table 2). Operative management accounted for 93.2% of cases, mostly commonly managed with open reduction (Table 1). Antibiotic agent use did not differ between operative and non-operative management (p = 0.18) (Table 3). The rate of antibiotic agent use between open and closed operative management did not differ significantly either (p = 0.99) (Table 3). Peri-operative antibiotic agents were used in 89.9% of cases, but non-guideline operative use (pre- and post-operative) rates were 47.5% and 63.6%, respectively (Fig. 2). The segmented logistic regression showed no statistically significant reduction in non-guideline antibiotic agent use before (OR = 1.225, p = 0.135) or after (OR = 0.810, p = 0.124) guideline implementation (Table 4). Surgical site infection and C. difficile complication rates during the admission were 0% (Table 5).
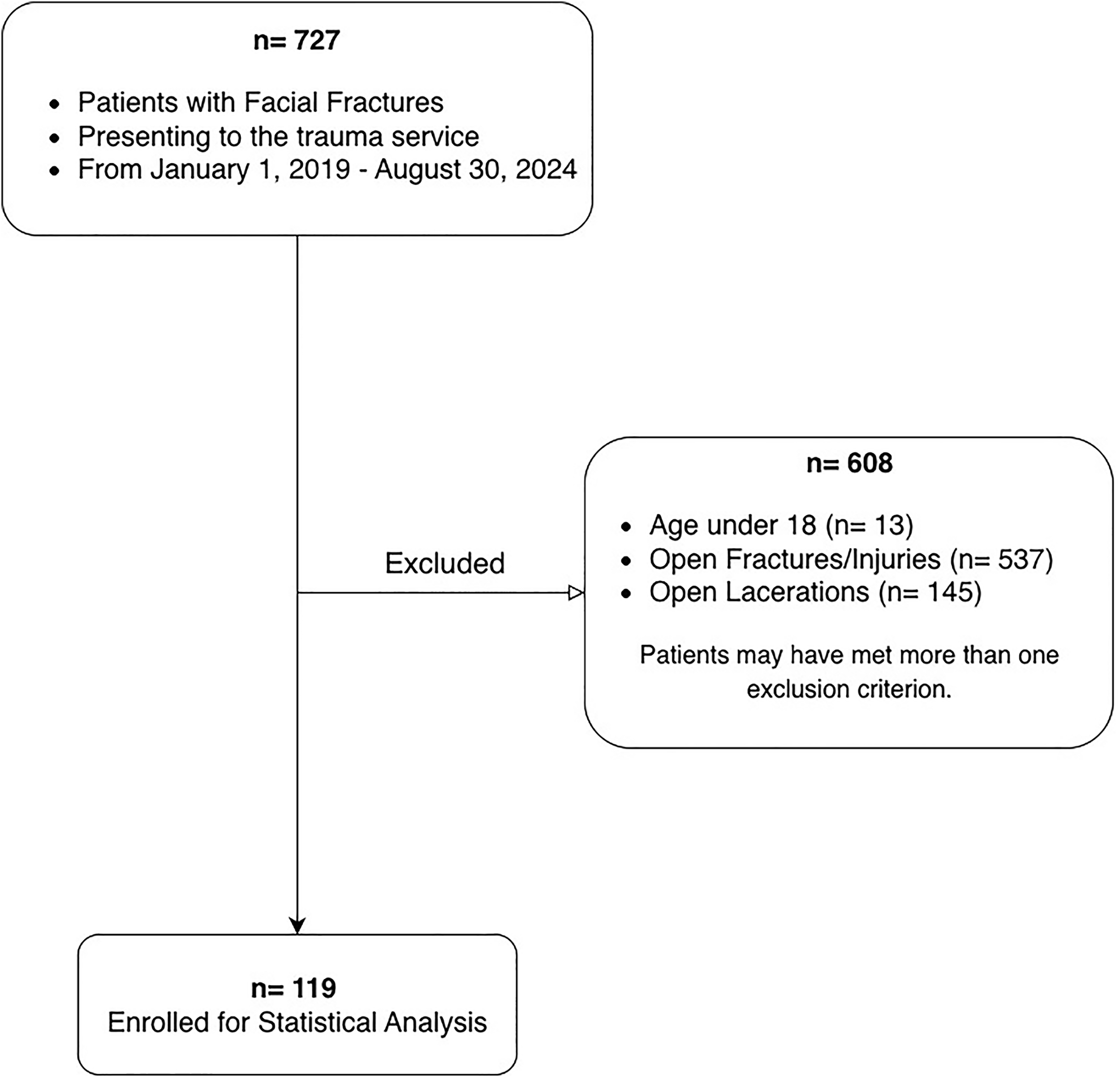
Patient selection and exclusion flowchart.
Population Characteristics
Antibiotic Agent Practices by Fracture Location
Antibiotic Agent Practices by Management
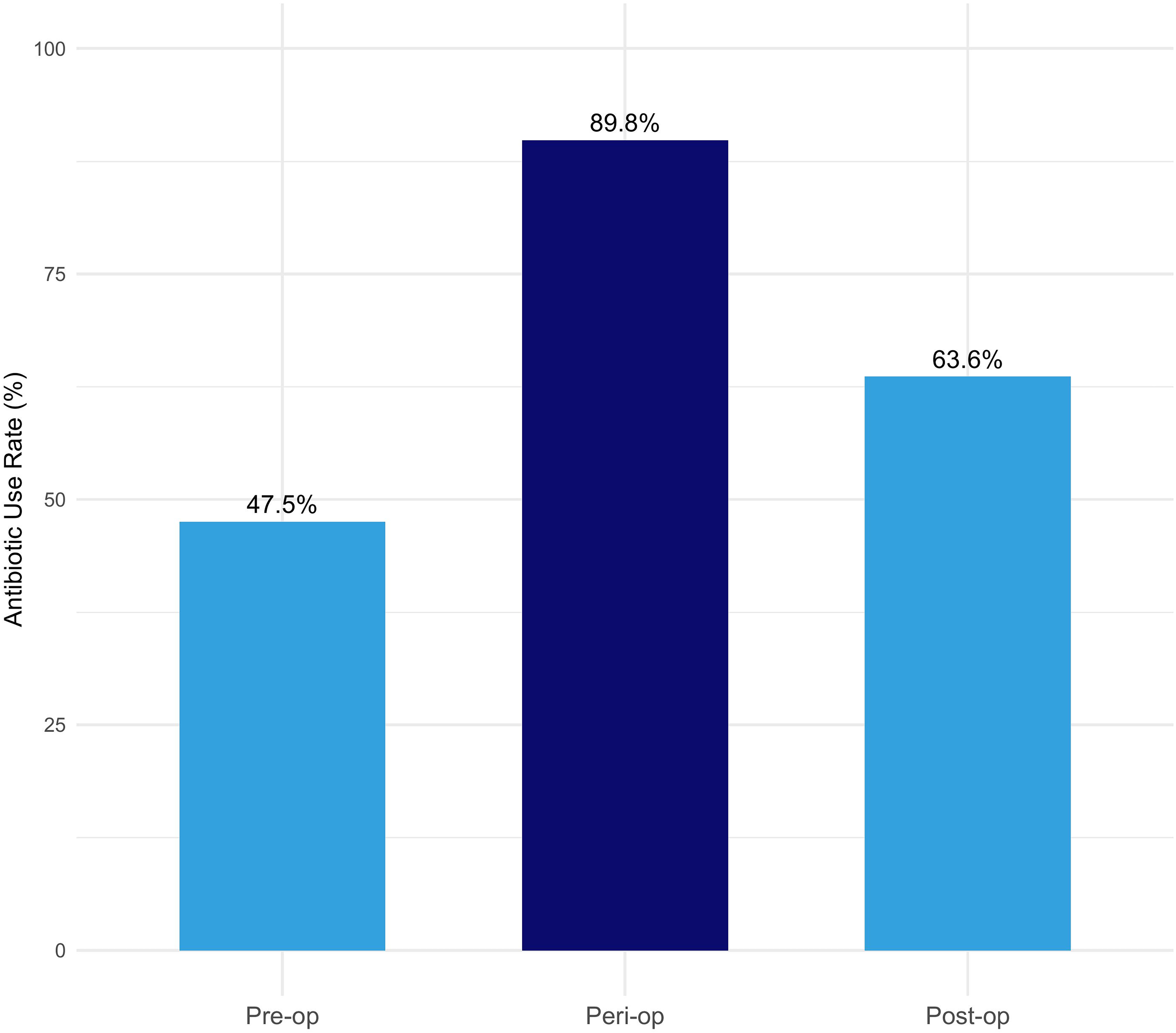
Rate of antibiotic agent use by timing.
Segmented Logistic Regression Analysis of Non-Guideline Antibiotic Agent Use
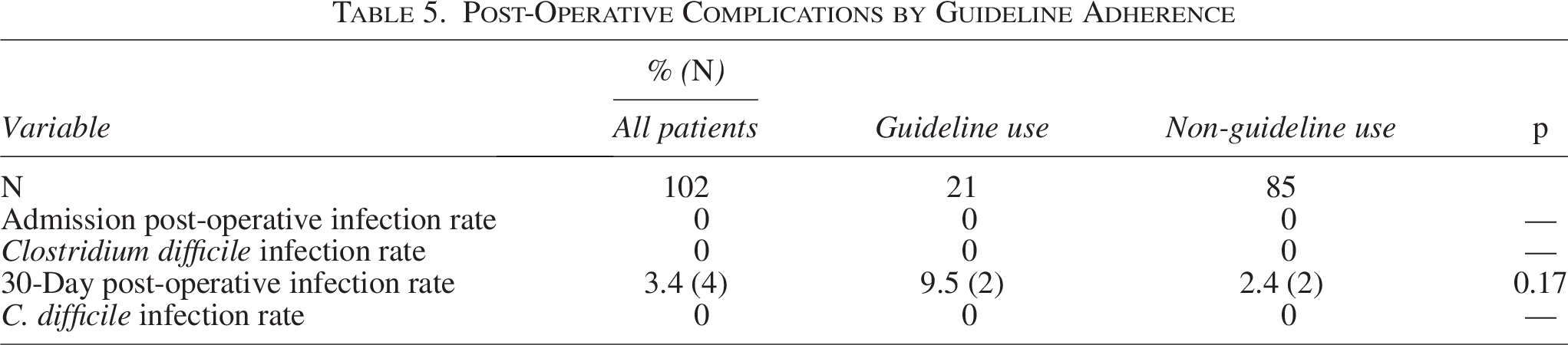
Post-Operative Complications by Guideline Adherence
Discussion
The approach to antibiotic agent use in fracture management has evolved over the years. Before antibiotic agents were widespread, open fractures led to disastrous complications, including severe infections, sepsis, and even death. Management focused on extensive and meticulous debridement to prevent infections such as gas gangrene. 10 The introduction of antibiotic agents, especially penicillin, in World War II, represented a turning point that reduced those complications to all-time lows. In the years to come, research refined the antibiotic agent guidelines, restricting use to specific cases. 11 These efforts have come forth because of the observance of antibiotic agent resistance with an aim to preserve the effectiveness of a powerful weapon in our arsenal.
Our findings demonstrate that antibiotic agent use remains high despite the SIS recommendation against them. This has been highlighted by the fact that 80.2% of prescriptions were non-guideline compliant (Table 2). In addition, the lack of difference between operative and non-operative cases suggests an indiscriminate prescription pattern, emphasizing a significant opportunity for improvement in antibiotic agent stewardship. The 584 days of antibiotic agents administered in five years to just 119 patients represent a substantial area for intervention, where reducing prescriptions could significantly decrease unnecessary antibiotic agent use (Table 2). Given that antibiotic agent-resistant organisms are responsible for over 35,000 deaths annually in the United States, optimizing our practices could have a major impact on resistance rates. 12
When examining non-guideline antibiotic agent use over time, segmented logistic regression did not demonstrate a statistically significant change in prescribing practices following publication of the SIS guidelines. Before guideline publication, non-guideline antibiotic agent use did not change significantly over time (OR = 1.225, p = 0.135). Following guideline publication, the post-guideline time trend also did not reach statistical significance (OR = 0.810, p = 0.124), and no statistically significant immediate change in prescribing was observed. These findings indicate that guideline publication alone was not associated with a measurable change in antibiotic agent prescribing during the study period (Table 4, Fig. 3).
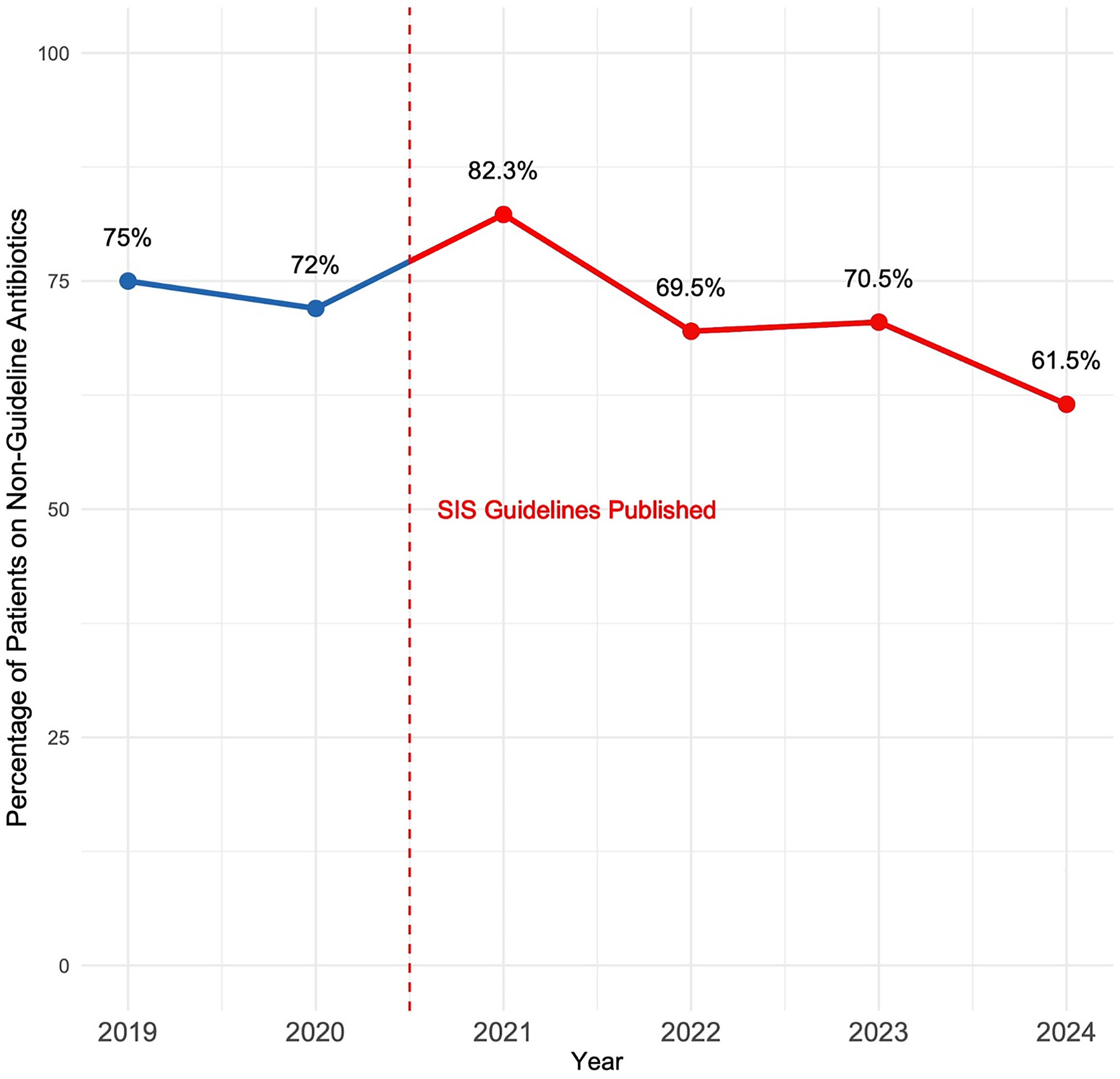
Trends in non-guideline antibiotic agent use in patients with facial fractures. Non-guideline antibiotic agent use in this graph refers to antibiotic agents administered in non-operative cases, as well as pre-operative and post-operative use.
In an era where the broader trend of medicine has been moving from antibiotic agents for all to a more targeted approach, some areas of use are more stubborn than others. The potential morbid complications of facial infections, including osteomyelitis and deep tissue abscesses, incline surgeons to prescribe antibiotic agents as a precautionary measure, even against guidelines, to give them peace of mind. 13 Although their role in open fractures is vital and well-established because of the heightened risk of infection, the high rates of antibiotic agent use in our cohort, which exclusively included closed fractures, are concerning, as they suggest overuse of antibiotic agents despite the lack of clear indications and limited proven benefits in closed fractures. 14
The persistence of non-guideline antibiotic agent use in our cohort highlights a substantial opportunity cost in antimicrobial agent stewardship. Quantifying excess antibiotic agent exposure provides actionable data that can support future implementation efforts, including education, audit-and-feedback, and standardized protocols.
Although institution-specific cost data were not available, published estimates suggest that the direct cost of inpatient antibiotic agent therapy in US hospitals ranges from approximately $50–$150 per antibiotic agent day, depending on agent selection, dosing, and administration requirements.15,16 Applying this conservative estimate to the 495 non-guideline antibiotic agent days observed in our cohort corresponds to an estimated $25,000–$75,000 in direct antibiotic agent costs alone, excluding nursing time, pharmacy overhead, laboratory monitoring, and downstream costs related to adverse events. Although illustrative, this estimate highlights the potential economic impact of excess antibiotic agent prescribing and reinforces the importance of antimicrobial agent stewardship initiatives.
No post-operative surgical site or C. difficile infections were recorded during the admission. However, after following up with patients for 30 days post-discharge, the rate of surgical site infections was highest in the guideline-adherent group (9.5%) compared with the non-adherent group (2.4%) (Table 5). Although the 30-day surgical site infection rate differed numerically between guideline-adherent and non-adherent groups, this difference was not statistically significant and was on the basis of a small number of events. As such, no conclusions can be drawn regarding the relationship between antibiotic agent duration and post-operative infection risk. This observation highlights the need for further investigation with larger sample sizes to better understand the clinical impact of limiting antibiotic agent use in facial fracture management.
Limitations
The most significant limitation of this study is the assumption that publication of national guidelines alone is sufficient to change local prescribing behavior. In practice, meaningful implementation of evidence-based recommendations typically requires local champions, such as surgeon leaders, infection prevention teams, or formal antibiotic agent stewardship programs, to translate national guidelines into institution-specific workflows. Without such local infrastructure, consistent guideline adherence is unlikely to be achieved. Accordingly, our findings should not be interpreted as a failure of individual clinicians to follow SIS recommendations, but rather as evidence of an implementation gap that exists in the absence of targeted local support. Importantly, these data may serve to justify allocation of institutional resources toward education, stewardship oversight, and locally driven implementation tactics aimed at improving adherence to guideline-concordant antibiotic agent use in patients with facial fractures. As with any retrospective, single-institution study, our analysis may be limited by the accuracy of antibiotic agent administration records, potential underascertainment of post-discharge infections if patients sought care outside our health system, lack of insight into individual provider decision-making, and limited generalizability to other institutions with different patient populations, prescribing practices, and protocols.
Conclusion
This institutional audit demonstrates substantial discordance between SIS guideline recommendations and real-world antibiotic agent prescribing practices for isolated facial fractures, resulting in significant excess antibiotic agent exposure. By quantifying non-guideline antibiotic agent use and potential antibiotic agent days saved, this study highlights an important opportunity for antimicrobial agent stewardship and provides a foundation for future guideline implementation and quality improvement efforts.
Authors’ Contributions
A.E.N., H.H., and J.L.J. contributed to the study conception, design, data collection, analysis, and interpretation. A.E.N. drafted the initial article. All critical revisions and final approval were completed by A.E.N., H.H., C.G., and J.L.J. F.A. contributed to data collection. J.L.J. served as the principal investigator. All authors reviewed and approved the final version of the article.
Footnotes
Acknowledgment
The authors thank Sherri M. Minchella, RN, Trauma Program Manager at the Henry Ford Hospital, for her assistance in obtaining data from the trauma registry and supporting the data collection process.
Author Disclosure Statement
No conflicts of interest are reported for any author.
Funding Information
No funding was received for this work.
Data Access Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request. Because of institutional policies and patient confidentiality, some restrictions may apply.
Ethics Statement
The study was approved by the Institutional Review Board of Henry Ford Hospital. Informed consent was waived because of the retrospective nature of the study. All data were handled in compliance with institutional policies and the principles outlined in the Declaration of Helsinki.