
Abstract
Background:
National trends toward earlier onset of diverticulitis combined with more advanced maternal age may converge, making diverticulitis an increasingly important etiology of obstetric abdominal infection. However, there is little data on this topic, and no specific guidelines on how to treat pregnant patients with the disease. The purpose of this study was to identify the frequency of hospitalization for diverticulitis in pregnant patients and the common complications associated with this disease process.
Methods:
We conducted a retrospective cohort study using the National Readmissions Database (NRD) to evaluate maternal and fetal complications among pregnant patients diagnosed with diverticulitis. The NRD was queried for all visits in the first 3 quarters of each year, 2016–2019, that included a patient with an International Classification of Diseases-10 code for diverticulitis and pregnancy. These entries were then further investigated for demographics, gestational age, rates of intervention, readmissions, and maternal and fetal complications.
Results:
A total of 470 patients were identified with a diagnosis of diverticulitis and pregnancy. Most patients (n = 340, 72.3%) were in the third trimester of pregnancy at presentation. 160/470 (34.0%) of admissions led to fetal delivery within 48 h. Of these, 3.8% of patients (n = 18) had complicated diverticulitis on index admission. The 90-day readmission rate for perforation or abscess was 1.3%. There were no reported maternal deaths. The overall rate of maternal complications was 41.3% and fetal complications was 41%, including a 1.9% rate of fetal loss.
Conclusions:
Diverticulitis is associated with significant rates of maternal and fetal complications when it occurs during pregnancy. Further investigation is warranted to better define the outcomes and guide best practices in this population.
Background
Diverticulitis leads to approximately 200,000 people being hospitalized every year in the United States alone. Rates of diverticulosis increase with age, and historically less than 10% of adults under 40 were found to have the condition. 1 However, symptomatic diverticulitis has been increasing in younger populations. One study showed that between the 1980s and 2000s, rates of diverticulitis increased 85% in patients 30–39 years old and 132% in patients 40–49 years old. 2 Treatment of diverticulitis can vary from antibiotics alone, percutaneous drainage, and elective or emergent surgical procedure depending on the patient’s clinical condition. 3 Approximately 40% of patients present with acute diverticulitis, meaning they having a perforation or abscess, and around 80% of these can be managed non-operatively. 4
A recent Centers for Disease Control and Prevention report has stated that the average age of first pregnancy in the United States is steadily rising, reaching 29.6 years in 2023. Over a third of first pregnancies are now occurring in women 30 years or older. 5 Given that rates of diverticulitis are rising in younger patients, and the average age of pregnancy is increasing, the number of pregnant patients experiencing diverticulitis will likely increase over time. The American College of Obstetrics and Gynecology (ACOG) has stated that “A pregnant woman, should never be denied medically necessary surgery or have that surgery delayed regardless of trimester because this can adversely affect the pregnant woman, and her fetus. 6 ” However, in common surgical diseases such as appendicitis and cholecystitis, pregnant women are less likely to receive operative management, even when evidence demonstrates better outcomes with surgical procedure.7,8 The overall reluctance to operate on pregnant patients, or lack of widespread knowledge on treatment recommendations, means that clear, evidence-based guidelines are needed to direct treatment.
Despite the concern for increasing incidence, data on outcomes and evidence-based treatment recommendations for pregnant patients with diverticulitis are lacking. Perhaps because of this, societies for surgeons who perform emergency general surgical procedure, including the American College of Surgeons, the Eastern Association for the Surgery of Trauma, and the American Association for the Surgery of Trauma, do not have any society guidelines specific to the treatment of diverticulitis in pregnancy. The few published studies on the topic are limited to case reports and case series.9–13 The purpose of this study was to identify the frequency of hospitalization of diverticulitis in pregnant patients, as well as the common surgical, maternal, and fetal complications associated with this disease process and any differences in outcomes based on the management strategy. We hypothesized that rates of operative interventions would be low and that rates of maternal and fetal complications would be high, similar to the treatment of pregnant patients with other infectious diagnoses.
Methods
Data source
The Nationwide Readmission Database (NRD) was reviewed using data from Q1 to Q3 during the years 2016–2019. The Q4 entries were excluded because of the increased likelihood that readmissions would occur the following calendar year and therefore not be captured in the database. This database is maintained by the Agency for Healthcare Research and Quality and was developed for the Healthcare Cost and Utilization Project (HCUP). The de-identified dataset contains over 100 variables collected from institutions in 27 states and allows data on initial admissions and readmissions to be collected even if the readmission is at a different hospital, provided the readmission occurs in the same state and within the same calendar year. 14 Readmissions include readmissions for any cause. In 2022 the NRD included 16.5 million discharges. 15 Diagnoses and procedures were identified using International Classification of Diseases (ICD)-10 codes and Current Procedural Technology codes. This study was exempt from Institutional Review Board approval because of the de-identified nature of the national dataset.
Data
The NRD was queried for patients with both ICD-10 codes for pregnant (Z33.1, Z33.3, Z3A.0-Z34.49) and diverticulitis (K57.0, K57.1*, K57.2*, K57.3*, K57.4*, and K57.5*). The database was then queried for demographic data, including age, race, gestational age, and insurance status. They were also reviewed for procedures including exploratory laparotomy (49000), colon resection (44140, 44143-7, and 44160), diagnostic laparoscopy (49320), laparoscopic colon resection (44204 and 44208), and interventional radiology drain (49405). Entries were further reviewed for readmission within 30, 60, and 90 days from initial admission, time to readmission, as well as mortality rates at initial presentation or readmission. For a full list of the ICD-10 codes used to search for fetal, pregnancy-associated, and maternal complications, please see Supplementary Appendix.
Statistical analysis
Means of continuous variables were compared using a student’s t-test or analysis of variance, while continuous variables with nonnormal distributions were compared using the Mann–Whitney U or Kruskal-Wallis test. Proportions were compared using chi-square tests. When individual data points were missing, cases were still included in the analysis of variables for which data were available. Statistical significance was set at p < 0.05. All statistical analysis was performed using SPSS v28 (IBM, Armonk, NY). Per HCUP requirements and our data use agreement, when fewer than 10 patients were included in a given category, the individual number is not reported. Recommendations for reporting observational studies were followed using the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. 16
Results
There were a total of 5,961,283 patients admitted with a pregnancy diagnosis during the study period. A total of 470 of these patients had a diagnosis of diverticulitis, suggesting an incidence of 0.008% among pregnant patients admitted to the hospital. The distribution of maternal age of presentation is shown in Figure 1. Age at admission ranged from 17 to 52 years old, with an average age of 32.8 years and most patients presenting during their 30s (n = 296, 62.9%). Most patients (n = 340, 72.3%) were in the third trimester of pregnancy, and 34.7% of index admissions led to fetal delivery. The distribution of gestational age at initial presentation is shown in Figure 2. Only 3.8% of patients (n = 18) had complicated diverticulitis on index admission, with 14 (3%) having surgical interventions including both diagnostic laparoscopy and exploratory laparotomy. None had a percutaneous drain placed as initial treatment. A 90-day readmission rate for perforation or abscess was 1.3%, while the total 90-day readmission rate was 27.4% for all causes. Due to database design, follow-up time for each patient is limited to the calendar year within which they initially presented.
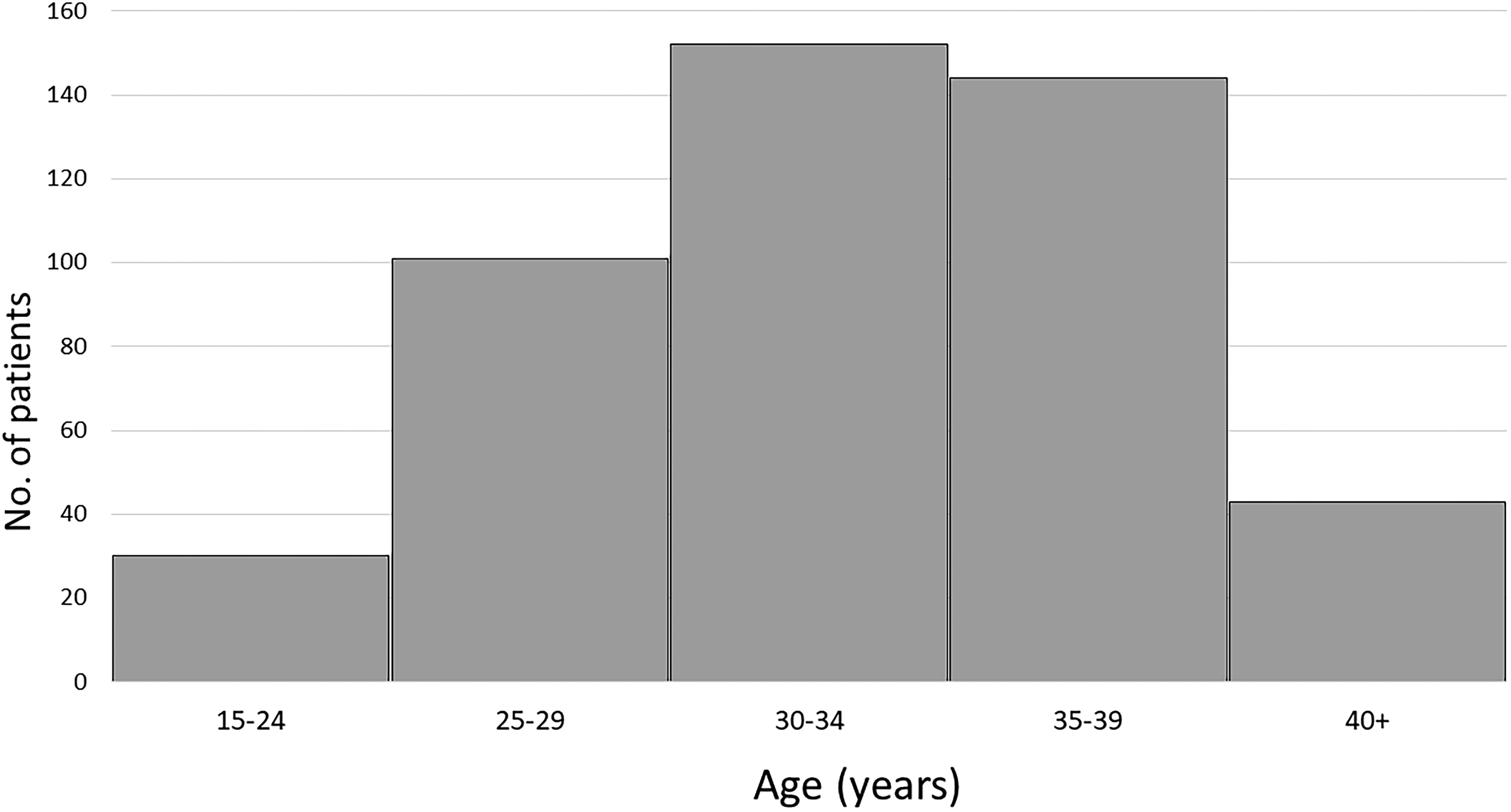
Maternal age distribution at the time of initial admission.
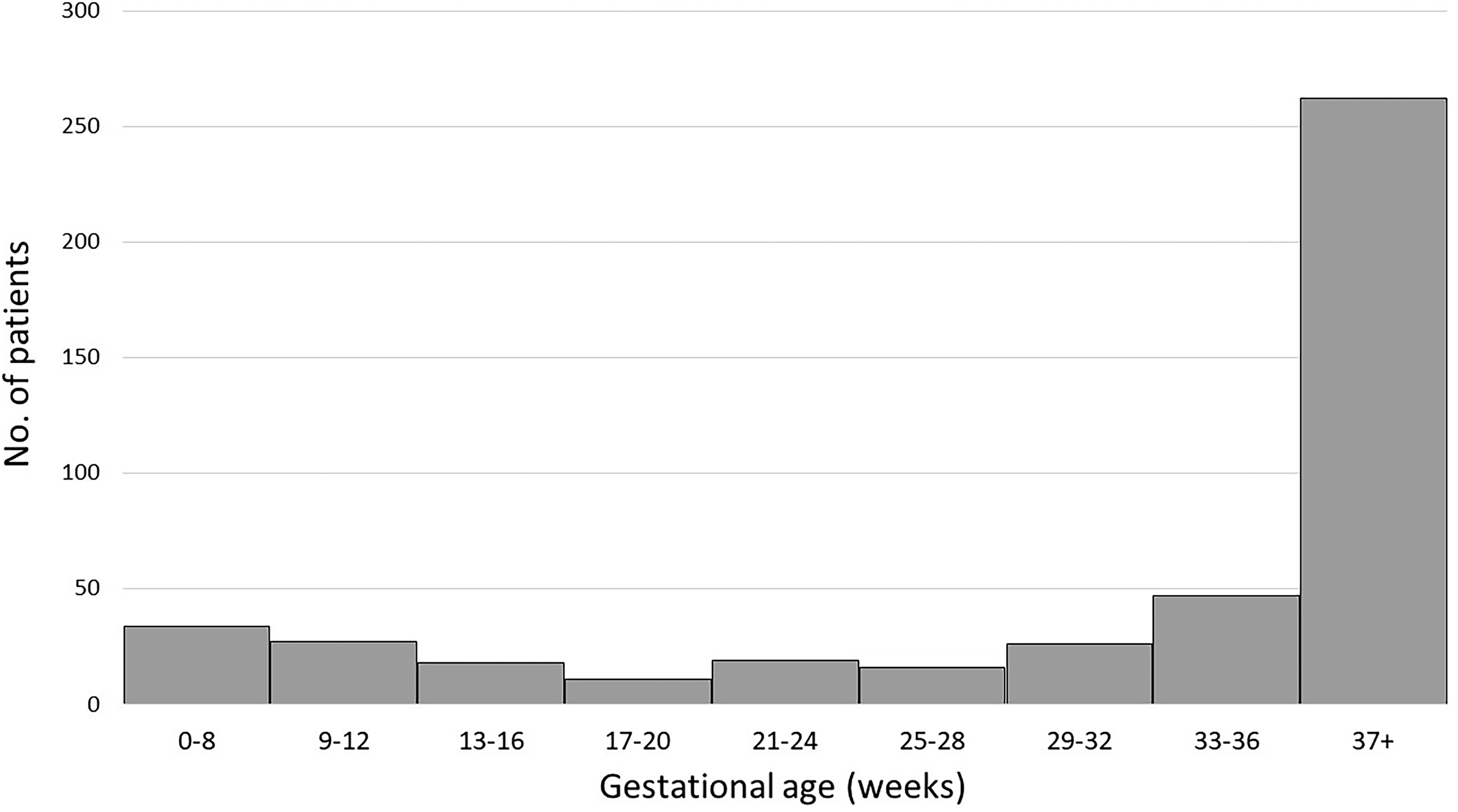
Gestational age at the time of initial admission.
Available demographic data are shown in Table 1. A majority of patients had private insurance, with most of the rest being covered by Medicaid. Included patients were most commonly treated at large hospitals in urban areas. Patient income was evenly distributed across all quartiles.
Insurance, Income, and Hospital Designation for the Study Population
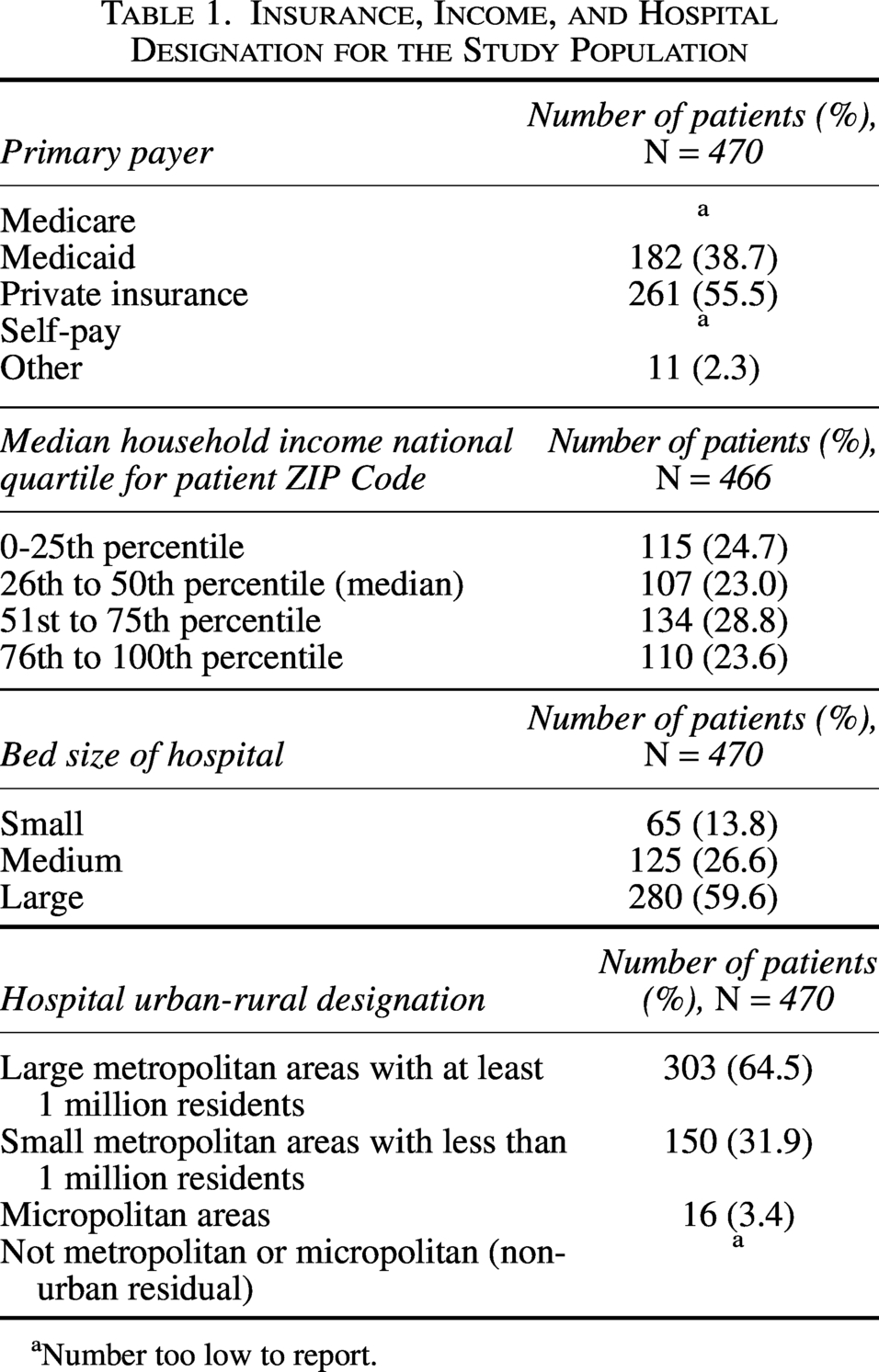
Number too low to report.
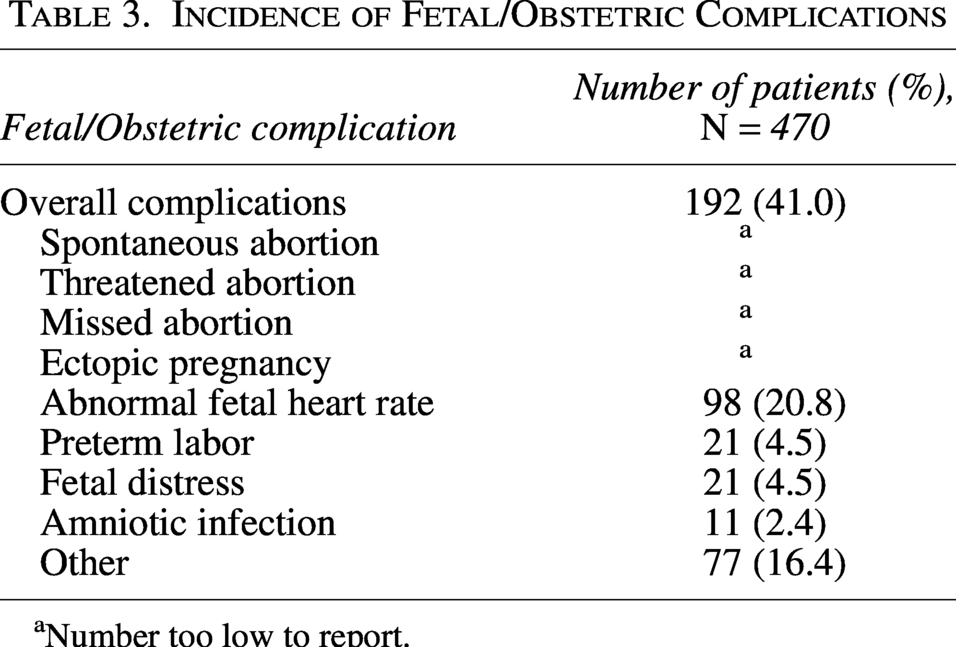
Maternal complications are shown in Table 2. There were no reported maternal deaths, but the overall maternal complication rate was 41.3%, with cardiopulmonary complications being the most common (18.1%) followed by gestational diabetes (15.5%). Table 3 shows obstetric and fetal complications. Preterm labor occurred in 4.5% of patients. The overall rate of fetal loss was 1.9%, and fetal complications were 41%. The most frequent complication events were abnormal fetal heart rate (20.8%), preterm labor (4.5%), and fetal distress (4.5%). There was no significant difference in maternal or fetal outcomes when operative and non-operative treatment groups were compared.
Incidence of Maternal Complications
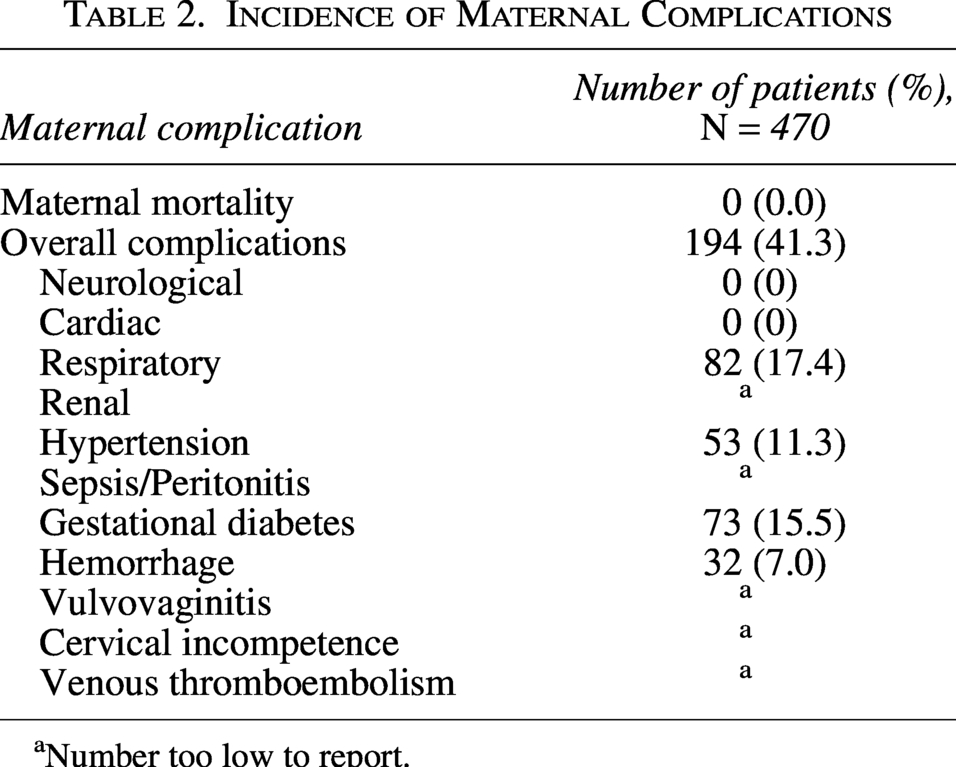
Number too low to report.
Incidence of Fetal/Obstetric Complications
Number too low to report.
The mean cost of the first admission was $29,156 ± 28,705, while the average cost of the first readmission was similar at $29,546 ± 35,573. The cost of readmission was highest when associated with readmissions for renal complications ($88,342 ± 98,683), peritonitis ($86,430 ± 51,462), and fetal malposition ($71,969 ± 82,154).
Discussion
Emergency general surgical procedure in pregnant patients remains a complex problem. Even when there is clear guidance for treatment, providers may be reluctant to intervene either because of the technically difficult aspects of intervention or because of liability concerns. While diverticulitis is most commonly seen in patients over 50 years old, rates among younger patients are rising. 17 As the average age of pregnancy also increases, this will become an increasingly common problem. To our knowledge, this is the first large-scale study examining complications and outcomes associated with treating diverticulitis in pregnant patients.
A meta-analysis looking at complications across multiple countries found an infant mortality rate of 1.7% in elective cesarean sections and 9.8% in emergent cases. 18 The National Vital Statistics Report published in 2015 reports a mortality rate of 5.96 fetal deaths per 1,000 live births in the United States, though this only reports fetal deaths after 20 weeks gestation. 19 However, the risk of fetal complications rises substantially when an intra-abdominal infection is present. For example, risks of fetal loss are 6% and preterm labor are 11% when appendicitis presents with peritonitis, and fetal loss increases to 24–36% once the appendix is perforated.20,21 In cholecystitis, there are reported rates of 6% preterm delivery, 0.6% rate of intra-uterine fetal death, and 0.9% amniotic space infection at the index admission, while 0.8% poor fetal growth is reported on 30-day readmission. 22 In contrast, our findings suggest that diverticulitis is associated with lower rates of preterm labor and fetal loss but higher rates of amniotic space infection.
Maternal deaths in the United States have increased to 23.6 per 100,000 live births from 2018 to 2021, with rates rising among all race and ethnicity groups, though only 5.8 per 100,000 live births were attributable to direct obstetric causes. 23 While maternal death is rare in appendicitis or cholecystitis, appendicitis increases the risk of antepartum hemorrhage four-fold and doubles rates of abruptio placentae.21,22,24 In acute cholecystitis, rates of maternal complications include 1.8% risk of cardiac complications, 2.4% respiratory complications, 2.2% renal failure, and a 3.0% rate of blood transfusion. 22 In comparison, the maternal complication rates associated with diverticulitis we observed in our study are significantly higher. While the reason for this is unclear, these findings could be because of a delay in diagnosis. Since appendicitis and cholecystitis are the two most common surgical emergencies in pregnancy, 20 they may be higher on the differential when a pregnant patient presents to the emergency room with abdominal pain and thus be recognized more quickly. In addition, cholecystitis is best diagnosed with ultrasound, so physicians may be more willing to order or perform the study since there is no associated radiation, which could lead to a more-rapid diagnosis. These findings demonstrate that diverticulitis is associated with higher maternal morbidity than other common intra-abdominal infections, and providers must remain vigilant in order to rapidly diagnose and treat these patients.
The reason for the observed lower rates of some obstetric and fetal complications but higher rates of most maternal complications when compared with other intra-abdominal infections is unclear. The predominance of late-gestation presentations in this cohort may have contributed to the relatively low rate of fetal loss in this population. Some variation may be because of the fact that diverticulitis can present as a broad range of disease severity, from peri-colonic inflammation and mild pain to perforation with sepsis and peritonitis, 4 and this differentiation is not captured in the current database. Few of the patients in our study received surgical intervention, which could suggest that the disease was typically not advanced at presentation, but this could also be because of surgeons being less likely to intervene on pregnant patients. Such delays or under-treatment could contribute to higher maternal morbidity observed, although one would also expect an associated rise in major fetal complications. Ultimately, the significant overall maternal and fetal complication rates emphasize the need for prompt diagnosis and intervention. Necessary imaging must be ordered, and any procedures necessary to stabilize the pregnant patient should be performed without delay to address this high rate of maternal morbidity.
This study has several limitations. First, as this is a review of a national database, it does not include individual patient clinical information that could be relevant to the patients’ outcomes or the decisions made regarding their treatment. Second, this database is based on ICD-9 and ICD-10 codes, so variations in how different diagnoses or complications are coded at different institutions may introduce variability. Next, we do not have specific data on the severity of diverticulitis and cannot account for patients initially being treated as outpatients, which limits our ability to draw more specific conclusions or make more detailed comparisons to other intra-abdominal infections. Given that some admissions may be for failed outpatient treatment or recurrent disease, the timing of disease onset to delivery may contribute to outcome differences. Finally, the database itself includes data from approximately 30 states and thus may not be applicable to all states or other countries because of regional variations in disease processes or healthcare delivery.
Conclusions
What is clear from this database study is that diverticulitis poses a significant risk to pregnant women and their unborn babies. As rates of diverticulitis in young people rise, this problem will become more common, and physicians need concrete data on which to make treatment recommendations and surgical decisions. Further research is needed on this topic to provide data-driven guidelines. Until those guidelines are available, we recommend that medically necessary surgical procedure should not be delayed in pregnancy as recommended by ACOG, and given the substantial maternal morbidity we observed, we recommend that pregnant patients with suspected diverticulitis receive timely imaging and intervention similar to non-pregnant patients.
Authors’ Contributions
D.C.: Conceptualization, writing—review and editing. A.M.H.: Writing—review and editing. J.S.: Writing—review and editing. A.S.: Formal analysis, writing—review and editing. J.L.W.: Conceptualization, writing—original draft
Footnotes
Author Disclosure Statement
No competing financial interest exist.
Funding Information
No external funding was used to support this study