
Abstract
Background:
This retrospective analysis investigated the role of serum IL-6 and IL-10 in distinguishing among pathological types of acute appendicitis and in preoperatively predicting perforation.
Methods:
The data from 376 patients were categorized into three groups on the basis of the definitive postoperative histopathological diagnosis: acute simple appendicitis (SIA), acute suppurative appendicitis (SA), and acute gangrenous appendicitis (GA). According to whether acute appendicitis is accompanied by perforation, the subjects are further stratified into two groups: non-perforated and perforated.
Results:
A statistically significant difference in IL-6 levels was observed among the groups (SIA vs. SA, p < 0.0001; SIA vs. GA, p < 0.0001; SA vs. GA, p < 0.0001). The IL-6 independently predicted a types of appendicitis pathology [SIA vs. SA: odds ratio (OR) 1.059, 95% confidence interval (CI) (1.039–1.079), p < 0.0001; SIA vs. GA: OR 1.080, 95% confidence interval (CI) (1.049–1.113), p < 0.0001; SA vs. GA: OR 1.000, 95% confidence interval (CI) (1.000–1.000), p = 0.05]. The optimum cut-off for the initial IL-6 was 23.54 [area under the curve (AUC) 0.8512, SIA vs. SA)], 39.36 (AUC 0.9844, SIA vs. GA), and 90.88 (AUC 0.8433, SA vs. GA). The IL-6 was significantly higher in the perforated group than in the non-perforated group (29.86 vs. 453.50, p < 0.001). The IL-6 independently predicted acute perforated appendicitis in multi-variable logistic regression analysis [OR 1.000, 95% confidence interval (CI) (1.000–1.000), p < 0.042]. The optimum cut-off for acute perforated appendicitis was 331.3 (AUC 0.8074). The diagnostic performance of IL-10 in differentiating acute appendicitis pathology types was fair (AUC 0.7322 for SIA vs. SA; 0.92263 for SIA vs. GA; 0.7738 for SA vs. GA) but consistently lower than IL-6, and its predictive value for acute perforated appendicitis remained limited (AUC 0.7875), further underscoring the superior discriminative capacity of IL-6.
Conclusions:
Preoperative evaluation of IL-6 and IL-10 can be useful in distinguishing pathological subtypes of acute appendicitis and predicting associated perforation.
Keywords
Introduction
Acute appendicitis is one of the most common acute abdominal conditions. The incidence of appendicitis is about 7%, while the rate of appendiceal perforation is as high as 20%. 1 There are various clinical scoring systems used to evaluate the severity of appendiceal inflammation. A definitive diagnosis of appendicitis can be difficult to establish, as the condition may present with atypical or masked clinical features, creating a diagnostic conundrum. 2 The increased risks of perforation, postoperative morbidity, mortality, and extended hospital stay associated with delayed management of severe appendicitis drive the urgent need for accurate predictors of disease severity.
Laboratory parameters such as white blood cell (WBC) count and C-reactive protein (CRP) levels help predict perforation in appendicitis.3–6 The diagnostic efficacy of these two tests is moderate individually, but the sensitivity increases significantly when they are used together. 7 However, neither the WBC count nor CRP level can definitively confirm or rule out a diagnosis of acute appendicitis with sufficient reliability. 8 The neutrophil-to-lymphocyte ratio (NLR) demonstrates acceptable diagnostic performance, serving as a useful marker for both confirming the diagnosis and assessing the severity of appendicitis. 9 Although mildly elevated serum bilirubin (total bilirubin > 1.0 mg/dL) has been found to be a marker for appendiceal perforation, with a sensitivity of 70% and specificity of 86%, it has no discriminatory role and is usually unhelpful in assessing suspected acute appendicitis. Bilirubin elevation has auxiliary diagnostic value in perforated appendicitis. 10
We believe that IL-6, a potent proinflammatory mediator, and IL-10, a proinflammatory and suppressor cytokine, may be useful for diagnosing acute appendicitis because they are important in immune defense and in immune-mediated disease. Recent studies have shown that different cytokine profiles could be associated with infectious conditions.11–13 However, the utility of cytokines in discriminating acute appendicitis was rarely reported. In the present study, we assessed serum levels of cytokines to investigate their predictive role in the pathogenesis of acute appendicitis.
Material and Methods
The study population comprises adults aged 18 years or older who were surgically treated under a clinical suspicion of acute appendicitis during the period spanning September 2023 to September 2024 in this retrospective observational analysis. Patients were enrolled from the Shanxi Bethune Hospital. The inclusion process began with the identification of all adults (≥18 yrs) seeking care in the emergency department who had received a surgical appendectomy during our study period. Participants were excluded based on the following criteria: (1) age below 18 years, (2) the type of operation is not laparotomy, (3) pregnant, (4) a documented immunological deficiency, (5) patients who use immunosuppressive agents such as hormones, and (6) the patient’s postoperative pathology suggested an appendiceal tumor. This study was conducted after approval from the Institutional Review Board at our hospital. To ensure confidentiality, all personally identifiable information was deleted after replacing it with an anonymized study code. The data were obtained through a retrospective chart review.
We then stratified the enrolled patients into three groups—simple acute appendicitis (SIA), suppurative appendicitis (SA), and gangrenous appendicitis (GA)—according to the operative and histological findings. Among the complicated group (including SA and GA), patients were further stratified into non-perforated and perforated groups based on the presence of perforation.
Data for this retrospective study were extracted from the electronic medical records, including demographic characteristics including gender, age, BMI, length of hospital stay, and post-operative length of stay; medical history including time since, the onset of symptoms until surgical intervention; laboratory characteristics including WBC count, neutrophil count, neutrophil percentage, CRP, prothrombin time, procalcitonin (PCT),
Statistical analysis
Continuous data, expressed as mean ± SD (normal distribution) or median (IQR) (non-normal distribution), and categorical data, presented as frequencies (percentages), were compared between groups using the Mann-Whitney U/Chi-square tests (two groups) or one-way ANOVA/Kruskal-Wallis tests (multiple groups), with results reported as values (95% CIs). Significant uni-variable variables were advanced to a multivariable logistic regression model to define independent predictors; their diagnostic performance was evaluated via ROC curve analysis, yielding an optimal cut-off value with its sensitivity and specificity. Inter-variable correlations were analyzed using Pearson’s test. A two-tailed p < 0.05 was set as the threshold for statistical significance.
Results
Characteristics of the study subjects
Between September 2023 and September 2024, 412 patients with appendicitis who underwent a laparoscopic appendectomy were initially selected for this study. After screening based on inclusion and exclusion criteria, 376 patients with appendicitis were included in final study, out of which 196 (52.1%) were men and 180 (47.9%) were women, with a median age of 41 years (range: 18–91 yrs). Demographic and clinical parameters were summarized in Table 1. There were 94 patients in the SIA group, 77 patients in the acute SA group, and 107 patients in the acute gangrenous group (GA). We observed an older age (35.5 vs. 51.5, p = 0.0012; 40 vs. 51.5, p = 0.0017), a longer time of length of hospital stay (4 vs. 6, p < 0.0001; 4 vs. 6, p < 0.0001), and a longer postoperative period (3 vs. 6, p < 0.0001; 4 vs. 6, p < 0.0001) in group GA as compared with group SIA and group SA (Table 1).
Demographic Characteristics, Hematological Markers and Imaging Characteristics Between the Acute Simple Appendicitis, Acute Suppurative Appendicitis, and Acute Gangrenous Appendicitis Groups

SIA = acute simple appendicitis; SA = acute suppurative appendicitis; GA = acute gangrenous appendicitis; IL-6 = interleukin 6; IL-10 = interleukin 10.
The differences between acute and perforated appendicitis are summarized in Table 4. There were 315 patients in the non-perforated appendicitis group and 61 patients in the perforated appendicitis group. Whether appendicitis was perforated or not shows no gender inclination (48.6% vs. 44.3%, p = 0.5771). Patients with perforation are older in age (40 vs. 51, p = 0.0385) and heavier in weight (64% vs. 70%, p = 0.0466). Furthermore, their hospital stay (4 vs. 6, p < 0.0001) and postoperative hospitalization time (4 vs. 6, p < 0.0001) are also longer.
Demographic Characteristics, Hematological Markers and Imaging Characteristics Between the Non-Perforated and Perforated Appendicitis Groups
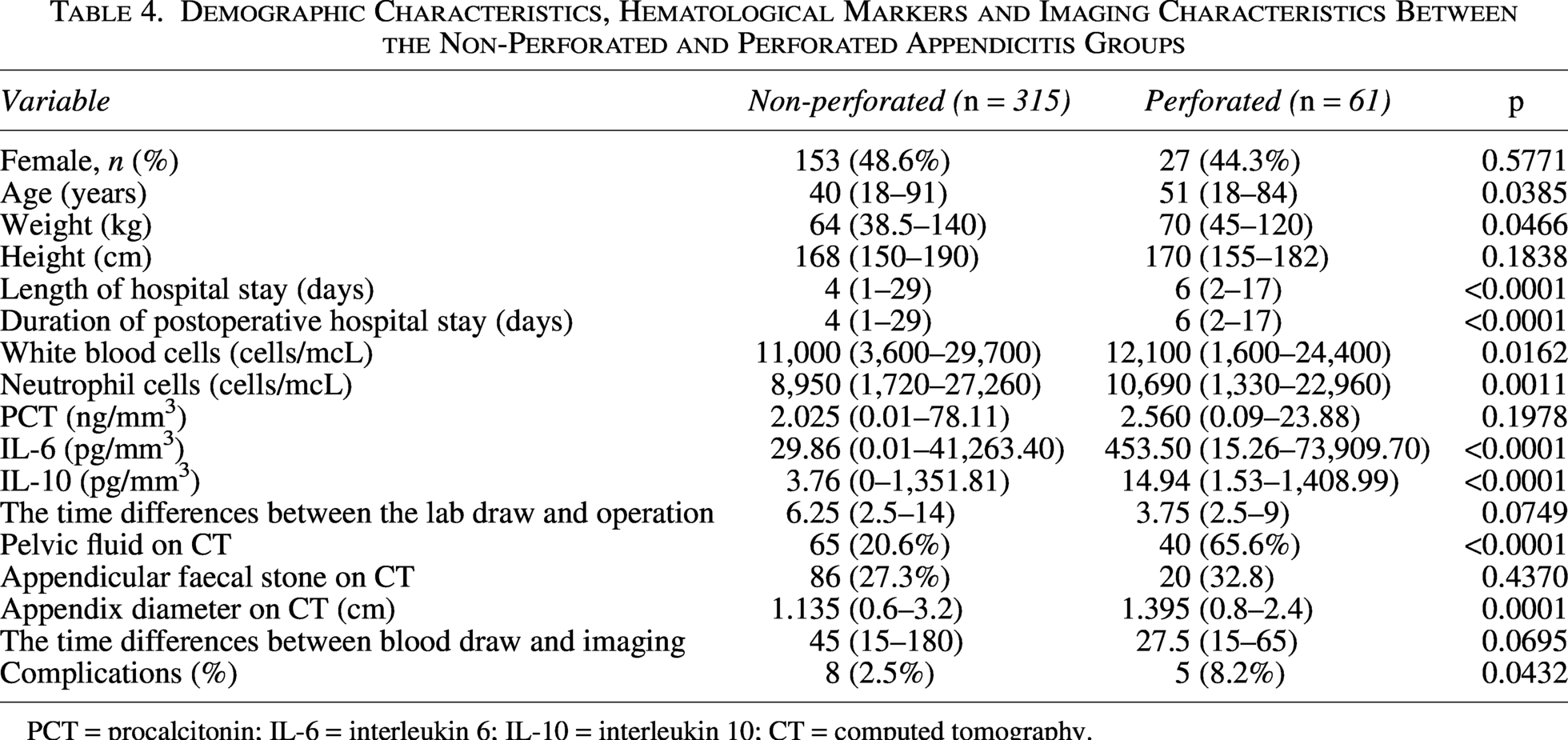
PCT = procalcitonin; IL-6 = interleukin 6; IL-10 = interleukin 10; CT = computed tomography.
IL-6 to predict the type of acute appendicitis pathology
The median IL-6 values were 4.43, 38.58, and 334.20 in the SIA, SA, and GA groups, respectively. Significant differences were noted between groups (SIA vs. SA, p < 0.0001; SIA vs. GA, p < 0.0001; SA vs. GA, p < 0.0001) (Table 1).
Variables with a statistically significant difference between the groups were included for multi-variable logistic analysis. In the multi-variable logistic regression analysis, the IL-6 independently predicted a type of appendicitis pathology [SIA vs. SA: odds ratio (OR) 1.059, 95% confidence interval (CI) (1.039–1.079), p < 0.0001; SIA vs. GA: OR 1.080, 95% confidence interval (CI) (1.049–1.113), p < 0.0001; SA vs. GA: OR 1.000, 95% confidence interval (CI) (1.000–1.000), p = 0.05] (Table 2). The AUC values for IL-6 in predicting the pathological type were 0.8512 (SIA vs. SA), 0.9844 (SIA vs. GA), and 0.8433 (SA vs. GA), respectively. The optimum cut-off for the initial IL-6 was 23.54, 39.36, and 90.88, giving a sensitivity of 69.71%, 91.59%, and 80.37%, and specificity of 85.11%, 94.68%, and 74.86%, in that order (Table 3, Fig. 1). Similarly, there are also significant differences in IL-10 between the pairwise comparisons of the three groups (SIA vs. SA, p < 0.0001; SIA vs. GA, p < 0.0001; SA vs. GA, p < 0.0001). The IL-10 was an independent variable in the multi-variable analysis [SIA vs. SA: OR 1.388, 95% confidence interval (CI) (1.213–1.588), p < 0.0001; SIA vs. GA: OR 1.827, 95% confidence interval (CI) (1.494–2.234), p < 0.0001; SA vs. GA: OR 1.003, 95% confidence interval (CI) (1.001–1.005), p = 0.015] (Table 2), but the predictive value of IL-10 for the type of acute appendicitis pathology was fair [0.7322 (SIA vs. SA), 0.92263 (SIA vs. GA), and 0.7738 (SA vs. GA)] (Table 2, Fig. 1) and lower than that of IL-6.
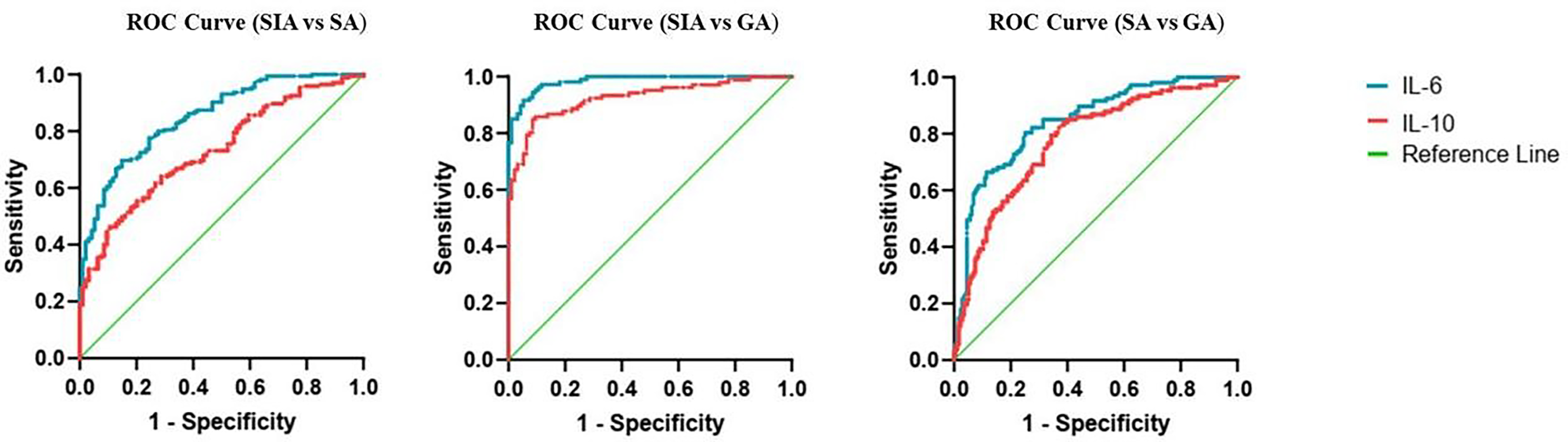
ROC curves showing sensitivity and specificity of the inflammatory biomarkers. IL-6 = interleukin 6; IL-10 = interleukin 10.
Multi-variable Logistic Regression Analysis of Parameters for Predicting the Type of Acute Appendicitis Pathology
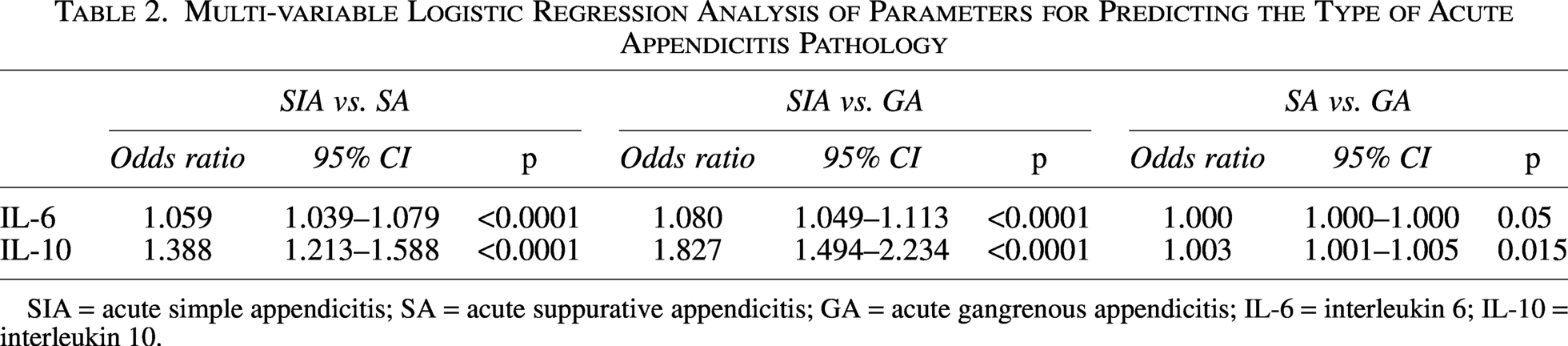
SIA = acute simple appendicitis; SA = acute suppurative appendicitis; GA = acute gangrenous appendicitis; IL-6 = interleukin 6; IL-10 = interleukin 10.
Receiver Operating Characteristics Analysis of Parameters for the Prediction of the Type of Acute Appendicitis Pathology

SIA = acute simple appendicitis; SA = acute suppurative appendicitis; GA = acute gangrenous appendicitis; IL-6 = interleukin 6; IL-10 = interleukin 10.
IL-6 to predict acute perforated appendicitis
The median IL-6 levels were significantly higher in the perforated group compared with the non-perforated group (29.86 vs. 453.50, p < 0.001) (Table 4). Variables with a statistically significant difference between the groups were included in a multi-variable logistic analysis. In the multi-variable logistic regression analysis, the IL-6 independently predicted acute perforated appendicitis [OR 1.000, 95% confidence interval (CI) (1.000–1.000), p < 0.042] (Table 5). The AUC for the ability of the IL-6 to predict the presence of an acute perforated appendicitis was 0.8074. The optimum cut-off for the initial IL-6 was 331.3, giving a sensitivity of 55.74% and specificity of 90.16% (Table 6).
Multi-variable Logistic Regression Analysis of Clinical Parameters for Predicting Perforated Appendicitis
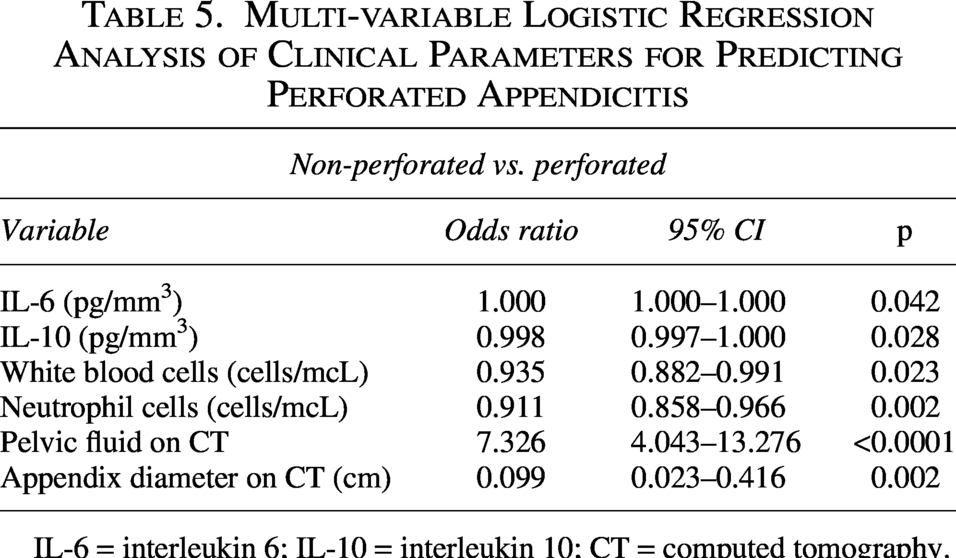
IL-6 = interleukin 6; IL-10 = interleukin 10; CT = computed tomography.
Receiver Operating Characteristics Analysis of Parameters for the Prediction of Complicated Appendicitis
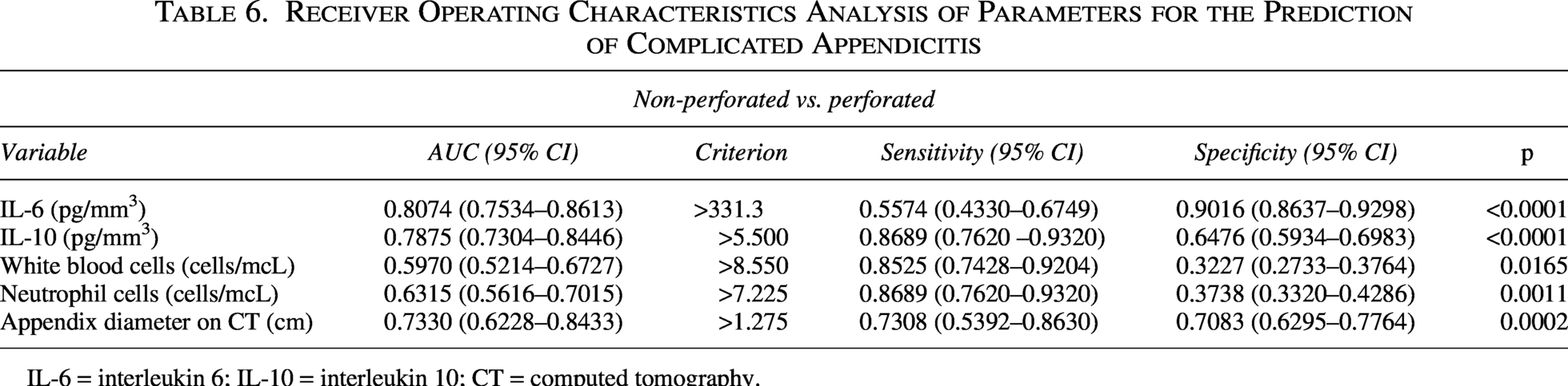
IL-6 = interleukin 6; IL-10 = interleukin 10; CT = computed tomography.
Other hematological and imaging parameters such as the WBCs, neutrophil cells, IL-10, pelvic fluid on CT, and appendix diameter on CT were also significantly different between the non-perforated group and perforated group. Also, theseparameters were included as independent variables in the multivariable analysis; however, WBCs and neutrophil cells showed poor reliability for predicting acute perforated appendicitis (AUC = 0.5970, AUC = 0.6315, respectively). The predictive performance of IL 10,, pelvic fluid detected on CT, and maximal appendiceal diameter on CT for acute perforated appendicitis was moderate to low (AUC = 0.7875, AUC = 0.6315, AUC = 0.7330, respectively) (Table 6, Fig. 2), all inferior to IL-6.
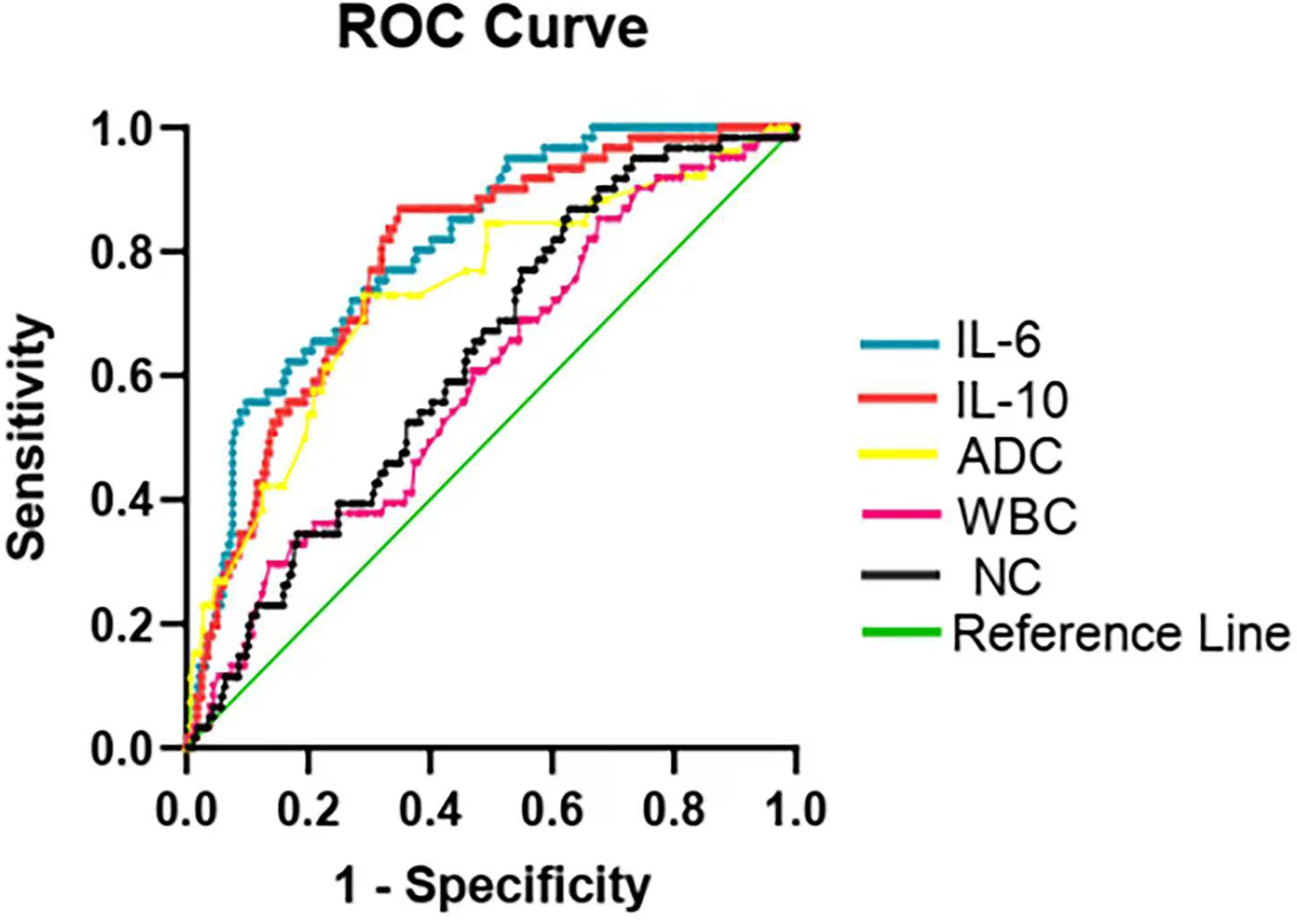
ROC curves showing sensitivity and specificity of the inflammatory biomarkers. IL-6 = interleukin 6; IL-10 = interleukin 10; WBC = white blood cells; NC = neutrophil cells; ADC = appendix diameter on CT.
Discussion
The most frequent cause of severe abdominal pain is acute appendicitis, and the most common emergency operation performed globally is an appendectomy. Delayed diagnosis and treatment can result in increased perforation rates, surgical morbidity, mortality, and prolonged hospital stays. Despite advanced laboratory and imaging diagnostic modalities, timely and accurate diagnosis remains challenging.
A number of variables, including WBCs, NLR, lymphocyte-to-monocyte ratio, lymphocyte ratio, CRP, erythrocyte sedimentation rate, high serum total bilirubin levels, and decreased serum sodium levels, have been found to be possible predictors of perforated appendicitis in previous studies on serum biomarkers.14–19 Literature studies have found significant differences in other hematological parameters among the groups of gangrenous, suppurative, and simple appendicitis, including WBCs, NLR, lymphocyte-to-monocyte ratio, and platelet-to-lymphocyte ratio. However, there was no difference between the suppurative appendicitis group and the gangrenous group. This result might be consistent with the observation that following appendiceal perforation, the level of WBCs in the blood initially drops in certain patients. 20
Acute appendicitis mortality rates range from 0.09% to 0.24% in wealthy nations and from 1% to 4% in developing nations. The mortality rate for perforation in the elderly might range from 15% to 20%.21,22 In a study involving 77 individuals, Gurleyik et al. found that serum IL-6 levels by themselves did not increase diagnosis accuracy. 23 Similar findings were reached by Goodwin et al., who discovered no statistically significant difference between the IL-6 level in acute appendicitis and an uninflamed appendix. 24
Contrary to these findings, our study demonstrated that IL-6 can serve as a valuable biomarker for not only detecting the pathological type of appendicitis but also distinguishing whether it is complicated by perforation. IL-6 statistically outperformed IL-10 as an independent predictor of appendicitis pathology. Levels of both IL-6 and IL-10 were significantly elevated in the acute perforated appendicitis group compared with the non-perforated group. Moreover, IL-6 demonstrated superior predictive performance over IL-10 as an independent predictor for perforation. These findings suggest that IL-6 can aid clinicians in distinguishing pathological types and identifying perforated appendicitis early in the diagnostic workflow.
The anti-inflammatory cytokine interleukin 10 (IL-10) is mostly generated by Th2-cells and activated macrophages. Its function is to block the Th1 immune response and decrease the ability of cells to deliver antigens. In addition, IL-10 increases the Th2 response, which boosts B-cell proliferation and antibody production. 25 According to the findings of this study, IL-10 showed potential in predicting the pathological type of appendicitis and whether it is perforated. However, IL-10 is less predictive than IL-6.
Some publications propose using IL-6 as a marker in a pediatric acute appendicitis early diagnosis method. Of these, only serum IL-6 was statistically greater in both difficult and not complicated acute appendicitis groups as compared with the control group, with a sensitivity of 77.4% and a specificity of 58.1% (p < 0.01), according to Kakar et al. 26 Haghy et al. showed that including blood levels of IL-6 and PCT in the diagnostic work-up contributed to a statistically significant decrease in needless appendectomies. Sensitivity and specificity levels on PCT were 65% and 80%, respectively, indicating a potential contribution to the diagnosis of acute appendicitis. 27
Significantly higher PCT levels were found in patients with acute complicated appendicitis compared with those with the uncomplicated form, as reported by Vikrant Dharwal and colleagues. 28 However, Kaya et al. claimed that PCT and D-dimer are not superior markers to CRP for the diagnosis of acute appendicitis because of their low sensitivity and diagnostic usefulness. 28 Our study also showed no statistically significant difference in early PCT levels between the groups.
CT has been established as the imaging modality of choice, boasting a superior diagnostic performance with sensitivity and specificity reported at 94% and 95%, respectively. 29 We found appendix diameter on CT can be used to determine whether the appendix has ruptured (AUC 0.7330) (Table 4), but it cannot classify appendicitis type. In addition, of the two cytokines mentioned above, IL-6 correlated positively with appendix diameter on CT (r = 0.2360, p = 0.0019), whereas both IL-10 did not (r = 0.0827, p = 0.2850) (Fig. 3). This coincides with our aforementioned research finding that the diameter of the appendix can predict the severity of inflammation to a certain extent.
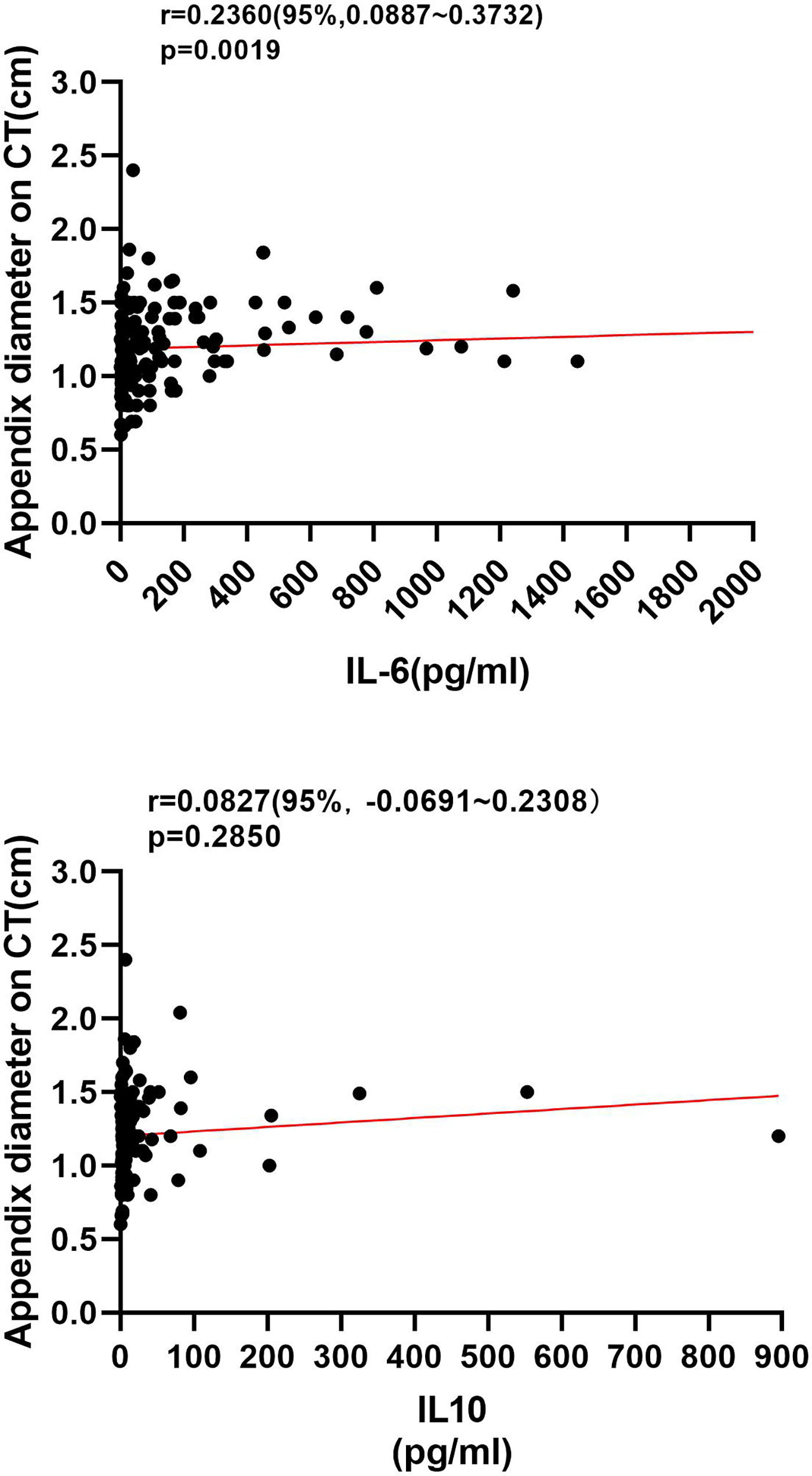
Association between IL-6, IL10 and appendix diameter on CT in patients with acute appendicitis. Correlation analysis of IL-6 and appendix diameter on CT (r = 0.2360). Correlation analysis of IL-10 and appendix diameter on CT (r = 0.0827).
In our study, we performed statistical analyses of the interval from blood sampling to surgery and identified no statistically significant intergroup differences (Tables 1 and 4). However, the present study failed to incorporate the time from symptom onset to blood testing into the analysis, a limitation we recommend be addressed in future investigations. Second, the pathophysiological mechanisms responsible for elevated IL 10 levels remain incompletely characterized and poorly elucidated. But we believe that this problem is outside the purview of our clinical investigation.
Conclusion
The surgeon’s clinical examination remains critical in diagnosing acute appendicitis. Differentiating appendicitis types preoperatively via serum cytokine levels could enhance clinical practice. Our findings suggest that IL-6 and IL-10 could contribute to this goal. When combined with clinical examination, laboratory tests, and CT scan, these markers may assist clinicians in evaluating and managing suspected acute appendicitis effectively.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Consent to Publish
Individual or identifiable participant information has not been used in this study.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Footnotes
Author Disclosure Statement
The authors declare that they have no conflicts of interest.
Funding Information
The authors received no specific funding for this work.