
Abstract
Background:
Surgical site infection (SSI) after pancreaticoduodenectomy (PD) remains a major cause of post-operative morbidity. Various risk factors for SSI have been identified. This study aimed to investigate the relationship between the C-reactive protein (CRP)–albumin–lymphocyte (CALLY) index, a novel inflammatory biomarker, and SSI following PD.
Methods:
The outcomes of patients who underwent PD between January 2017 and December 2022 were retrospectively analyzed. Patients who underwent laparoscopic surgery, received neoadjuvant therapy for borderline or locally advanced tumors, had metastatic disease, or presented with evident infections requiring treatment at the time of surgery were excluded. Demographic data, post-operative outcomes, and the presence of SSI were recorded. The CALLY index and other potential risk factors for SSI were evaluated.
Results:
The cutoff value for the CALLY index was determined as 5. Patients with a CALLY index <5 had a significantly higher incidence of SSI (p < 0.001). Multi-variate analysis demonstrated risk factors for SSI included CALLY index, elevated pre-operative CRP level, post-operative pancreatic fistula, and pre-operative biliary drainage (p = 0.021, p = 0.003, p < 0.001, and p = 0.037, respectively). Multi-variate analysis demonstrated that the CALLY index was a strong independent predictor of SSI (odds ratio = 5.195; 95% confidence interval: 2.430–11.107).
Conclusions:
The CALLY index is an independent risk factor for SSI after PD. This index reflects inflammation, immune status, and nutritional condition and represents a simple, non-invasive, and easily calculable predictive tool.
Introduction
Radical surgery remains the primary treatment modality worldwide for periampullary tumors. However, despite advances in preventive strategies, surgical site infection (SSI), occurring in approximately 11%–32% of cases, continues to be a significant cause of post-operative morbidity. 1 SSI prolongs hospital stay, increases healthcare costs, and delays the initiation of adjuvant chemotherapy.
To date, several risk factors for SSI following pancreaticoduodenectomy (PD) have been identified, including pre-operative biliary drainage, prolonged operative time, excessive intra-operative blood loss, advanced age, and high body mass index (BMI). 2 The risk factors for superficial SSI differ due to the complex nature of pancreatic surgery. Operative time exceeding 8 h, main pancreatic duct diameter <3 mm, and abdominal wall thickness >10 mm have been identified as independent risk factors for superficial SSI. 3 Other contributing factors include age >70 years, presence of gallstones, pre-operative jaundice, malnutrition, malignant disease, and emergency surgery. 4 Although these factors contribute to SSI development, most are non-modifiable.
The C-reactive protein–albumin–lymphocyte (CALLY) index is a newly introduced inflammatory and nutritional biomarker. First described by Iida et al., this biomarker was shown to be superior to neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) in predicting recurrence-free and overall survival in patients with hepatocellular carcinoma. 5 Subsequent studies have demonstrated the prognostic significance of the CALLY index in periampullary tumors.6,7
However, no study has evaluated the association between the CALLY index and SSI following radical surgery for periampullary tumors. Therefore, this study aimed to investigate the relationship between the CALLY index and SSI, a major post-operative morbidity following PD.
Materials and Methods
This retrospective study reviewed data from patients who underwent PD for periampullary tumors at our surgical clinic. Ethical approval was obtained from the institutional Ethics Committee (approval date: 25 October 2025; approval number: 793), and the study was conducted in accordance with the 2013 revision of the Declaration of Helsinki. Patient records between January 2017 and December 2022 were reviewed.
Patients aged ≥18 years with an Eastern Cooperative Oncology Group performance status ≤2 who underwent elective surgery for periampullary tumors were included. Exclusion criteria comprised laparoscopic surgery, neoadjuvant therapy for borderline or locally advanced tumors, metastatic disease, and clinically apparent infections requiring treatment at the time of surgery.
The CALLY index was calculated preoperatively using routinely measured blood parameters obtained within one week before surgery. Serum albumin (Alb), lymphocyte count, and C-reactive protein (CRP) levels were recorded. The CALLY index score was calculated using the following formula: 5 CALLY index = [albumin (g/dL) × lymphocyte count (×109/L)]/CRP (mg/dL) × 104. To ensure standardization, all blood analyses were performed in a single accredited laboratory.
Patients were divided into high and low CALLY index groups. Demographic data and SSI occurrence were compared between groups. SSI diagnosis and classification were performed according to the Centers for Disease Control and Prevention guidelines. 8 SSI was classified as incisional (skin, subcutaneous tissue, fascia, or muscle) or organ/space SSI. Post-operative pancreatic fistula (POPF) was defined according to the International Study Group of Pancreatic Fistula criteria. 9
Standard PD was performed by experienced surgeons. Drain amylase levels were measured on post-operative days 3 and 5. Drains were removed on post-operative day 5 if values were within normal limits; otherwise, they were retained in patients with pancreatic fistula.
Continuous variables were expressed as median and interquartile range, while categorical variables were expressed as numbers and percentages. Receiver operating characteristic (ROC) analysis was used to determine the optimal cutoff value for the CALLY index. The independent samples t-test or Mann–Whitney U test was used for numerical variables, and Pearson’s chi-square test was used for categorical variables. A p-value <0.05 was considered statistically significant. Statistical analyses were performed using IBM SPSS version 25 (IBM Corp., Armonk, NY).
Results
A total of 194 patients were included. Demographic characteristics are presented in Table 1. Of these, 105 patients (54.1%) were male, and the most common tumor location was the ampulla of vater (37.6%). SSI occurred in 105 patients (54.1%), with organ/space SSI observed in 39 patients (20.1%). Pancreatic fistula was detected in 112 patients (57.7%), including all fistula grades.
Demographic and Clinical Characteristics
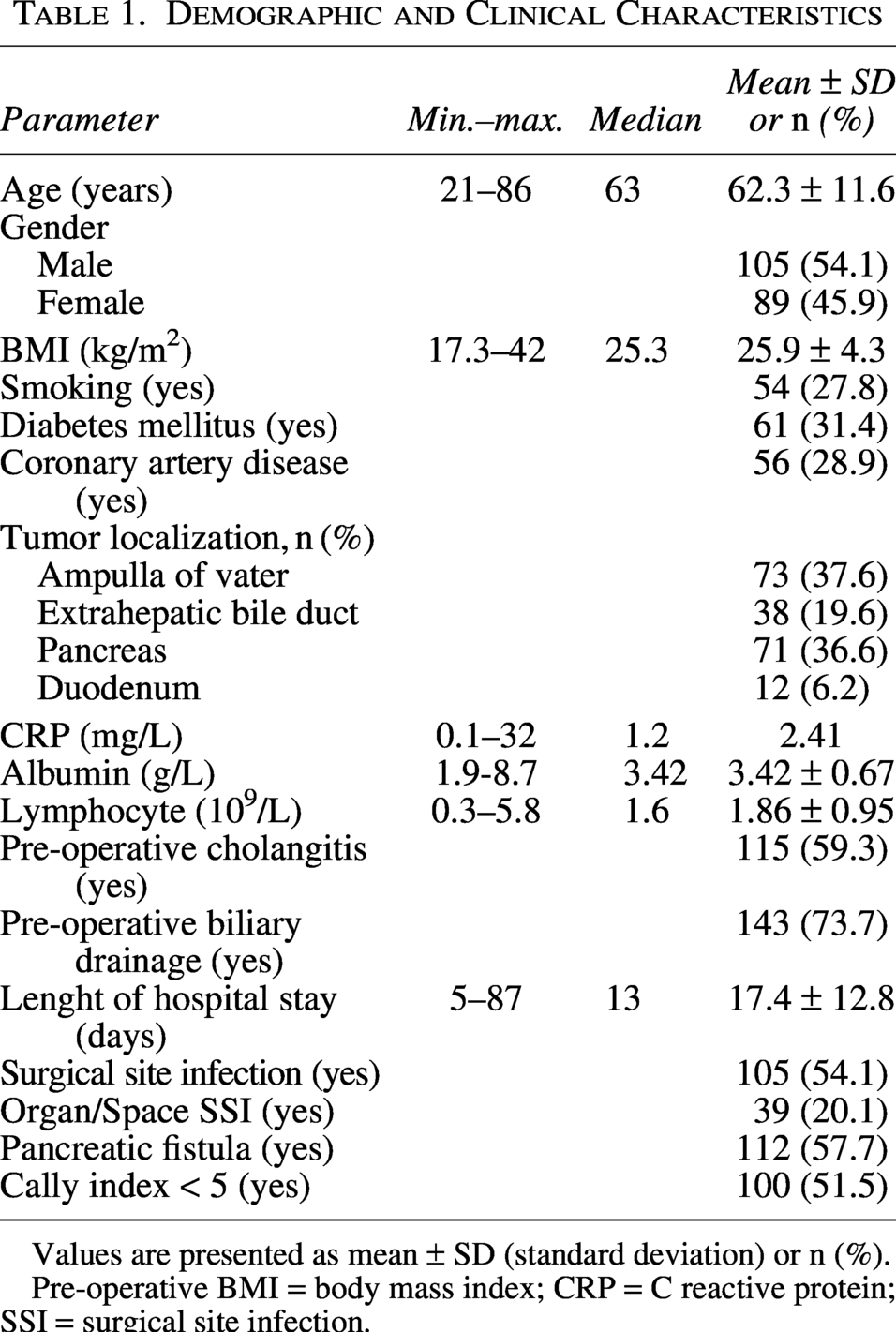
Values are presented as mean ± SD (standard deviation) or n (%).
Pre-operative BMI = body mass index; CRP = C reactive protein; SSI = surgical site infection.
The prognostic value of the CALLY index for predicting SSI was evaluated using ROC analysis, and the optimal cutoff value was determined as <5 (AUC: 0.775; 95% confidence interval [CI]: 0.709–0.840) (Fig. 1). CRP, one of the components of the CALLY index, in predicting SSI was evaluated using ROC analysis. The optimal cut-off value for CRP was determined as >2.5 (AUC: 0.830; 95% CI: 0.772–0.887). These findings indicate that CRP has a good discriminative ability for predicting the development of SSI.
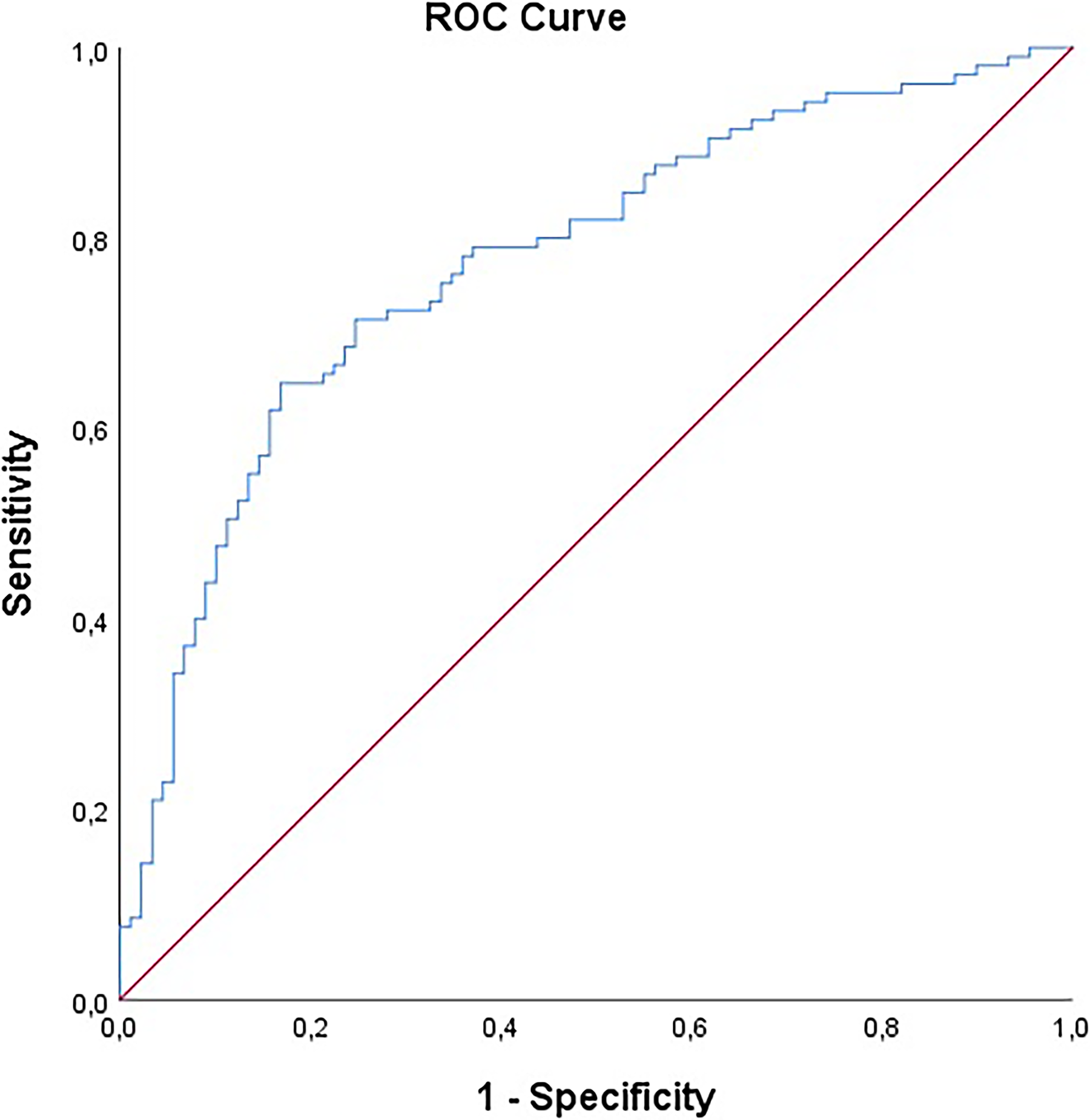
Receiver operating characteristic curve (ROC) Analysis for the CALLY Index in Predicting Surgical Site Infection in Pancreaticoduodenectomy Patients.
In contrast, no statistically significant cut-off values were identified for the other components of the CALLY index, namely albumin and lymphocyte levels, in predicting SSI.
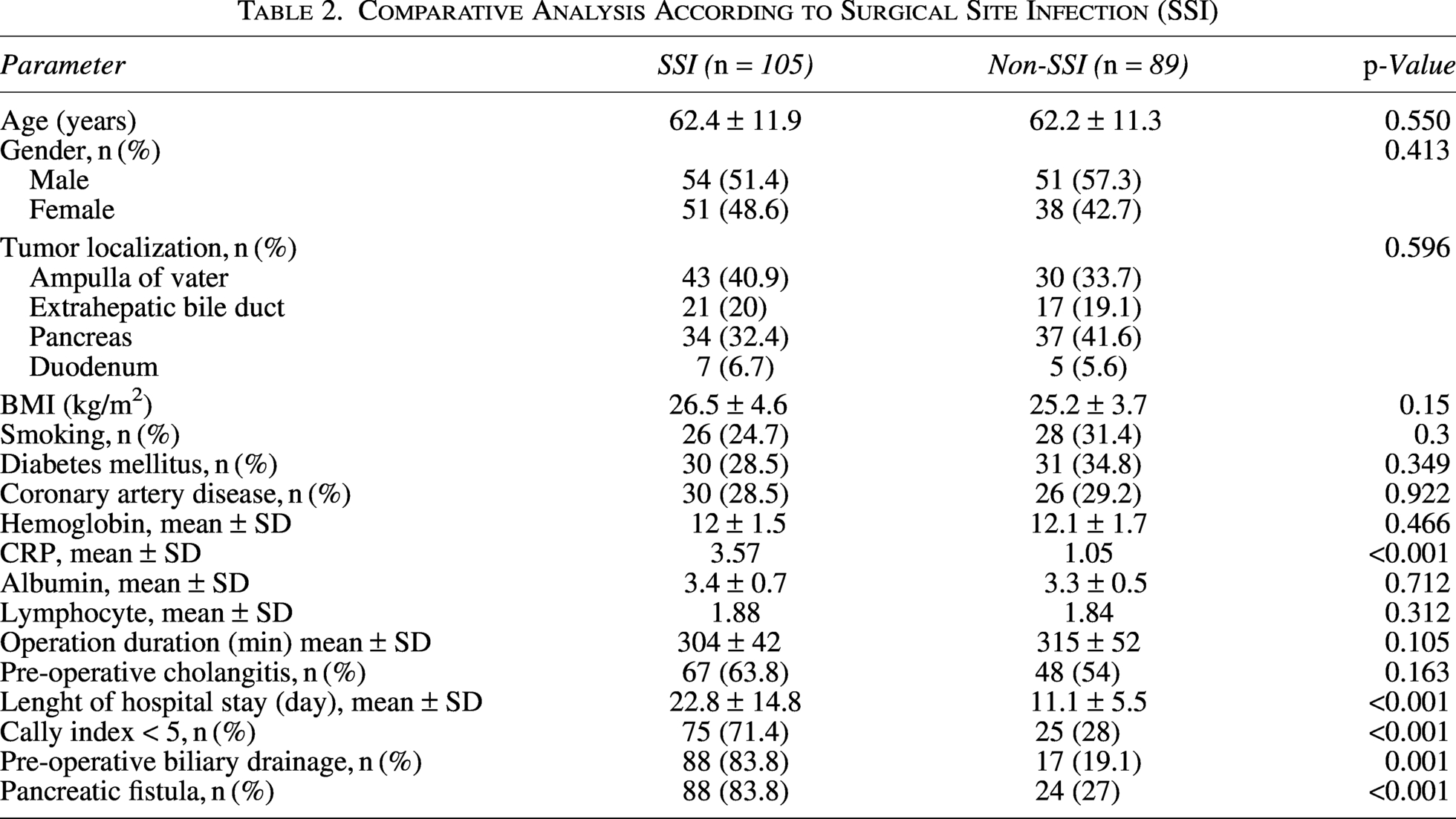
Preoperatively, 100 patients (51.5%) had a CALLY index <5. In these 100 patients with a CALLY index <5, significantly higher CRP levels (3.9 vs. 0.8, p < 0.001), lower lymphocyte counts (1.6 vs. 2.1, p < 0.001), and lower albumin levels (3.2 vs. 3.5, p < 0.001) were observed compared with patients with a CALLY index ≥5. Among patients who developed SSI, 75 (71.4%) had a CALLY index <5, which was significantly higher than in the non-SSI group (p < 0.001). Pre-operative biliary drainage and POPF were also significantly associated with increased SSI incidence (p = 0.001 and p < 0.001, respectively). Comparative data are presented in Table 2.
Comparative Analysis According to Surgical Site Infection (SSI)
Uni-variate analysis revealed that a CALLY index <5 (odds ratio [OR] = 6.4; 95% CI: 3.419–11.979; p < 0.001), CRP > 2.5 mg/L (OR = 15.328; 95% CI: 5.231–44.915; p < 0.001), pre-operative biliary drainage (OR = 3.2; 95% CI: 1.633–6.270; p < 0.001), and pancreatic fistula (OR = 14.02; 95% CI: 6.968–28.207; p < 0.001) were significantly associated with the development of SSI. Multi-variate analysis confirmed that a CALLY index < 5 (OR = 2.742; 95% CI: 1.161–6.472; p = 0.021), CRP > 2.5 mg/L (OR = 7.302; 95% CI: 1.928–27.654; p = 0.003), pre-operative biliary drainage (OR = 2.51; 95% CI: 1.055–5.975; p = 0.037), and pancreatic fistula (OR = 13.011; 95% CI: 5.791–29.232; p < 0.001) were identified as independent risk factors for SSI (Table 3).
Uni-variate and Multi-variate Analysis of Risc Factors for SSI
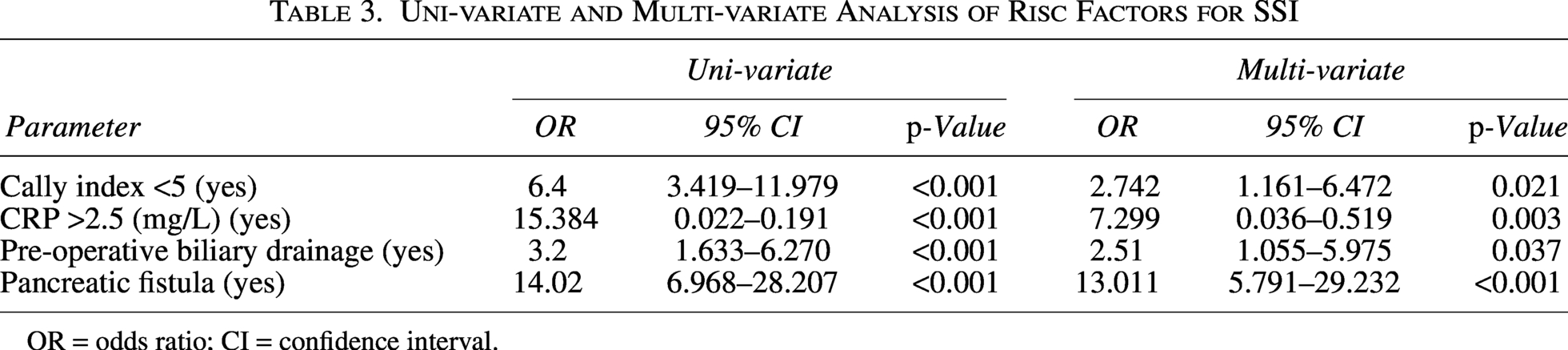
OR = odds ratio; CI = confidence interval.
Discussion
This retrospective cohort study aimed to identify risk factors for SSI following PD and to evaluate the association between SSI and the novel CALLY index. The findings demonstrate that pre-operative biliary drainage and POPF are significant risk factors for SSI and that the CALLY index represents a novel independent predictor.
Although mortality following PD has decreased with advances in surgical techniques, post-operative morbidity remains a major concern. SSI prolongs hospital stay, increases healthcare costs, and delays adjuvant therapy. Reported SSI rates following PD range widely, reaching up to 50% in some studies.3,10,11 In the present study, the SSI rate was 54.1%, consistent with existing literature, and was associated with a twofold increase in hospital stay duration.
POPF remains a critical complication after PD, associated with mortality rates up to 39%.12,13 In our study, POPF was present in 83.8% of patients with SSI and emerged as a strong independent risk factor in multi-variate analysis (OR = 13.01).
Pre-operative biliary drainage has also been frequently implicated as a risk factor for SSI. Bacterial contamination of bile has been reported in 69%–100% of cases and is associated with post-operative infectious complications.14,15 Modified surgical techniques aimed at reducing biliary contamination have demonstrated lower SSI rates. 16 Consistent with previous studies, pre-operative biliary drainage was identified as an independent risk factor for SSI in our cohort.
The CALLY index, which reflects inflammatory, immune, and nutritional status, has emerged as an important prognostic biomarker in various malignancies, including esophageal, gastric, and pancreatic cancers.7,17,18 Its advantages include low cost, accessibility, and ease of calculation. In this study, the CALLY index was shown for the first time to be associated with an increased risk of SSI following PD. Although the exact mechanism remains unclear, low albumin and lymphocyte levels and elevated CRP likely reflect impaired immune response and systemic inflammation, predisposing patients to infection.19–21
CRP is synthesized in the liver in response to interleukin-6 and is used as a non-specific marker of inflammation. It has been demonstrated that an imbalance between pro-inflammatory and anti-inflammatory responses in patients undergoing surgical stress may lead to immunosuppression and other complications. 20 The significantly elevated pre-operative CRP levels observed in patients who develop SSI may be considered indicative of acute inflammation and tissue injury. Furthermore, multi-variate analysis identified elevated pre-operative CRP levels as a strong independent predictor of SSI.
Albumin is a marker of nutritional status and also functions as a negative acute-phase reactant in the presence of inflammation. The adverse effects of hypoalbuminemia can be mitigated by correcting pre-operative malnutrition. Low pre-operative lymphocyte levels are likewise associated with an impaired immune system and an increased risk of SSI. 22
The concurrent derangement of these three factors may ultimately lead to a vicious cycle of malnutrition, chronic inflammation, and immunosuppression, thereby adversely affecting post-operative outcomes.
This study has limitations, including its retrospective design, single-center setting, and relatively small sample size. Other inflammatory and nutritional parameters that may affect post-operative outcomes were not included. Prospective, multi-center studies are warranted to validate these findings.
Conclusion
The CALLY index is an independent risk factor for SSI following PD. As a simple, non-invasive biomarker reflecting inflammatory, immune, and nutritional status, the CALLY index may help identify high-risk patients and enable the implementation of proactive strategies to reduce SSI.
Authors’ Contributions
T.O.: Conceptualization, methodology, investigation, data curation, writing—original draft preparation, writing—review and editing, and supervision. G.O.: Writing—original draft preparation and writing—review and editing. K.I.: Conceptualization, methodology, analyzing, writing—review and editing. A.S.: Conceptualization, methodology, data curation, writing—original draft preparation, writing—review and editing, and supervision.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.