
Abstract
Background:
The consideration of artificial nutrition and hydration (ANH) is recommended for individuals with reduced nutritional intake. However, placing long-term nonoral feeding tubes is not appropriate in those with advanced dementia or if the individual is likely to die imminently—“within hours or days” (GMC, 2010;58). In some instances, the provision of ANH in the weeks leading up to death may be considered a “Non-Beneficial Treatment.”
Objective:
To determine the extent to which “non-beneficial” nasogastric tube (NGT) feeding occurs at the end of life.
Design:
An audit of outcomes for individuals with a Malnutrition Universal Screening Tool (MUST) score of 2 who may be considered for artificial nutrition.
Methods:
All admissions to an acute hospital trust who met the following criteria: ≥65 years old and MUST score (Malnutrition Universal Screening Tool) of ≥2 over a six-month period (September '21–February '22). 1765 individuals met the inclusion criteria. For analysis, individuals were grouped by the presence of an NGT flag and admission survival.
Results:
84 (4.8%) had NGT procedure flags. Of these 84, 28 (33%) died during admission. A further 12 died within six months. In total 40 (47.6%) of 84 NGT-flagged individuals were deceased within six months. Chi-square analysis demonstrated a significant relationship between death during admission and NGT Flag (χ2 = 36.888, df = 1, p = < 0.001). Individuals with NGT flags who passed away were significantly older than peers who survived the admission (t = 2.576, df = 82, p = 0.012).
Conclusions:
NGT insertions in this cohort have a high likelihood of being considered “non-beneficial.” Frailty associated with increasing age may be a factor.
Key Message
A significant proportion of nasogastric tube (NGT) insertions may be considered “non-beneficial” as they are placed in individuals reaching the end of life. Advanced age and dementia are associated with non-beneficial NGT insertion. Furthermore, research is required to identify individuals who will benefit from acute NGT insertion.
Introduction
Nasogastric tube (NGT) feeding is nutritional intake through a thin, flexible tube passed into the stomach through the nose. 1 NGT feeding occurs where an individual has a history of limited nutritional intake 2 or is otherwise unable to meet their nutritional needs orally 1 and has been assessed as requiring artificial nutrition and hydration. 3 The introduction of an NGT to facilitate feeding occurs for several reasons: to avoid or counter malnutrition, prevent prandial aspiration and associated pneumonia, and to prolong survival.3,4 However, NGT feeding is only a temporary installation, utilized where the anticipated length of insertion is <4 weeks, 5 further the risk of aspiration pneumonia is not eliminated by their placement and may occur via other means. 6 Where an individual remains unable to tolerate oral intake after this period, the placement of a permanent feeding tube, 7 or withdrawal of nutritional support 8 must be considered.
NGT insertion is associated with modest costs: £75–158.64,1,9 though these have the potential to “spiral” where multiple staff are involved 1 or where adverse events occur, such as the inadvertent introduction of the tube into the lungs, which is associated with increased morbidity and length of stay (LOS).8,10 This may be particularly costly where ward beds are costed between £351 and 586.59 per day (NHS Digital Figs. cited by Guest 2020 11 ), NGTs may also be placed to manage gastric drainage. 7
Decision-making around NGT feeding initiation is an emotive and ethically complex process. Where an individual is diagnosed with a potentially reversible condition, it is appropriate to initiate NGT feeding,8,12–15 while for irreversible conditions such as progression of dementia, NGT feeding support should not be implemented13,16,17 as it is of little benefit 18 and is associated with agitation, nasal pain, discomfort from gagging, and the use of restraints.17,19–22
Multiple factors influence NGT feeding decision-making, such as past medical history, presenting condition, and prognosis. 1 In addition, there are several clinical and non-clinical decision-makers influencing NGT feeding initiation, including the individual and their family/carers, medical staff, and allied health professionals such as speech & language therapists and dieticians. Due to these various factors and the multiple decision-making participants involved, in practice, NGT feeding decision-making can be heavily impacted by patient and physician preference. 11
NGT feeding, when used in an end-of-life care setting, is considered a non-beneficial treatment. Non-beneficial treatments are interventions that are unlikely to have an effect, 23 do not meet attainable goals, or positively impact an individual’s subjective quality of life (QoL). 24 Where prognosis is poor, NGT feeding may be appropriately withheld, 25 as the intervention may be considered futile or “non-beneficial” if the recipient passes away with the tube in situ or shortly after it is removed.13,26 However, research on the frequency of use and the factors associated with the decision is in its infancy.
The purpose of the current article is to identify the frequency of use of NGT feeding as a non-beneficial treatment and identify factors that may be associated with decision-making in a specific trust.
Methods and Methodology
We aim to identify and quantify instances of “non-beneficial” NGT insertion that may occur as part of regular care and to identify demographic or decision-making factors that influence decisions during or prior to end-of-life Care.
Patient population
An audit and service evaluation was conducted in the National Health Service Hospital Trust. Inclusion criteria were intended to identify any individuals for whom short-term enteral feeding (NGT feeding) may have been discussed and considered—though not necessarily initiated. Participants who met the following inclusion/exclusion criteria were identified by the Trust data team for the purposes of audit. Individuals were included if they had a Malnutrition Universal Screening Tool (MUST) score of 2 (indicating a potential consideration of artificial feeding as per trust policy), were ≥65 years of age, and were acutely admitted to a southeast of England acute hospital trust between September 2021 and February 2022. In 2017 the life expectancy in this area for males was 80.7 years and for females 84.2. 27 This Trust serves an area with a comparatively high average life expectancy, making it appropriate to gather data relating to age related frailty, morbidity, and end-of-life care. 28
Data source and analysis
A complete data set was provided by the Trust following audit approval (Project no. 1653). Ethics approval was provided in accordance with the
Identified participants were coded into four sets depending on whether they survived the admission and whether they received an NGT flag: 1. NGT flag and deceased (NGTDec), 2. NGT flag and discharged (NGTDis), 3. Nil NGT flag and deceased (NILDec), and 4. Nil NGT flag and discharged (NILDis). NGTDec individuals, who received an NGT flag and passed away during admission, could be considered to have received a “non-beneficial” treatment—The insertion of an NGT, which could not meet the aims of insertion due to patient mortality. 4 See Figure 1 for a breakdown of the grouping process.
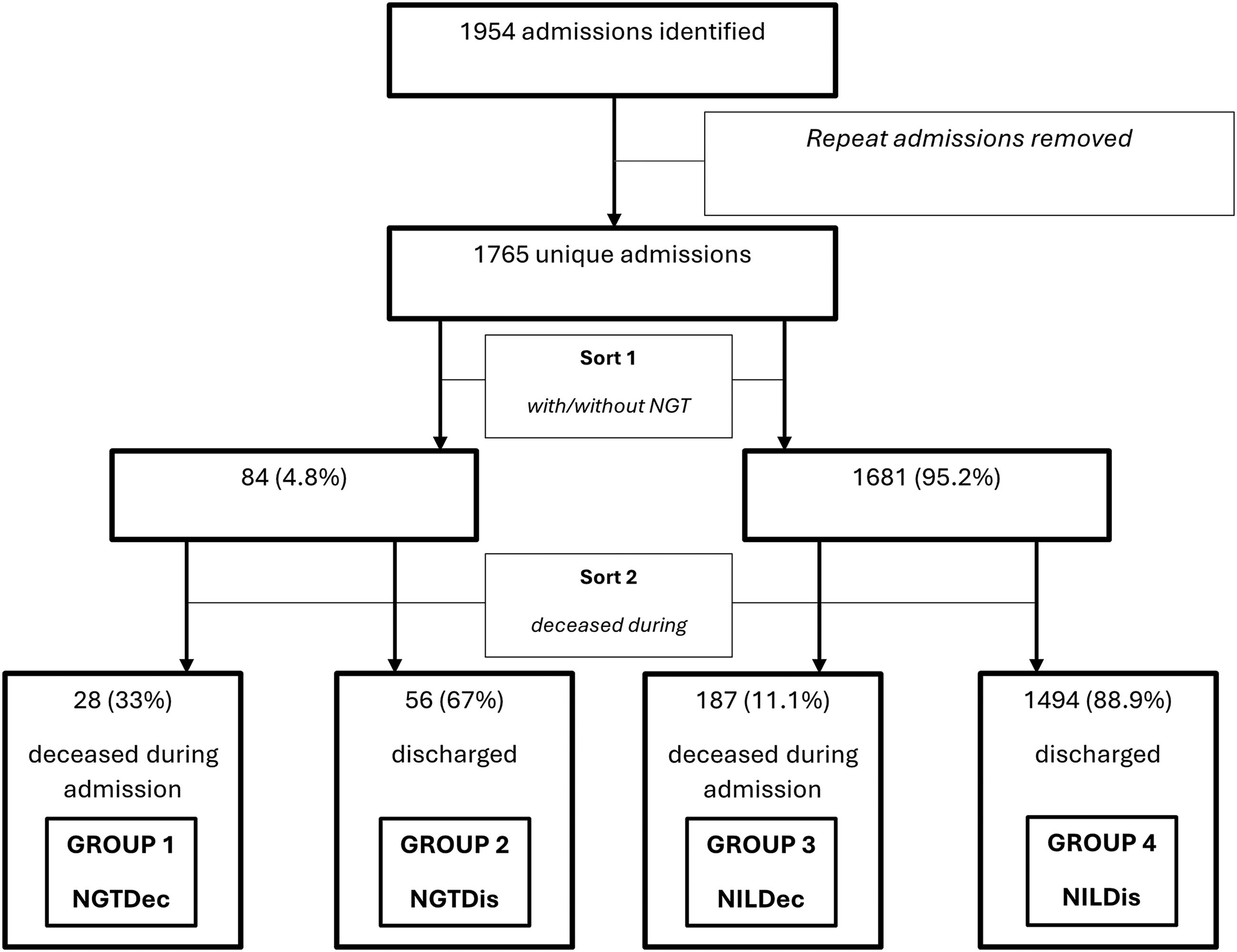
Diagram showing how unique admissions were sorted by “with/without NGT flag” and “deceased during admission/discharged” into four groups. Percentages reflect quantities at the “Sort” level.
Instances of multiple admissions were removed prior to full data analysis. Retaining duplicates would lead to the same discharge outcomes (including death) being analyzed multiple times; i.e., an individual with three admissions who passes away within six months of the initial admission would appear as three separate “deceased within six months” outcomes.
Statistical analysis
Statistical analysis was carried out using JASP 0.16.4. The relationship between categorical variables was explored using chi-square analysis. Nominal data were analyzed via paired t tests ANOVA, or their non-standardized data equivalents.
Results
With duplicate admissions removed, the dataset consisted of 1765 “unique” patients. (female, n = 1002, 56.8%). Mean age 82.8 years (65–105 years). Where applicable, participant data were associated with data flags that indicated the presence of NGT insertion, dementia or progressive neurological disease, etc. 325 (18.4%) had dementia flags; 170 (9.6%) were flagged with progressive neurological illnesses; 215 (12.2%) died during admission (female 44.2%, n = 95). Table 1 shows the total demographics.
Showing Total Demographic Data and by Gender. The Outcomes of Comparative Statistical Analysis Examining the Relationships between Gathered Data and Gender Are Shown in the Left Column
Significant statistical analysis outcomes in bold.
Includes those deceased at three months.
Cumulative total includes those deceased as inpatients.
LOS, length of stay.
Primary diagnosis
The most common primary diagnosis for admission in the data was injury and poisoning (n = 289, 16.4%), followed by diseases of the respiratory system (n = 254, 14.4%), symptoms, signs, and abnormal lab findings (n = 244, 13.8%), and diseases of the circulatory system (n = 238, 13.5%). See Figure 2 for a breakdown of the primary diagnosis of each group.
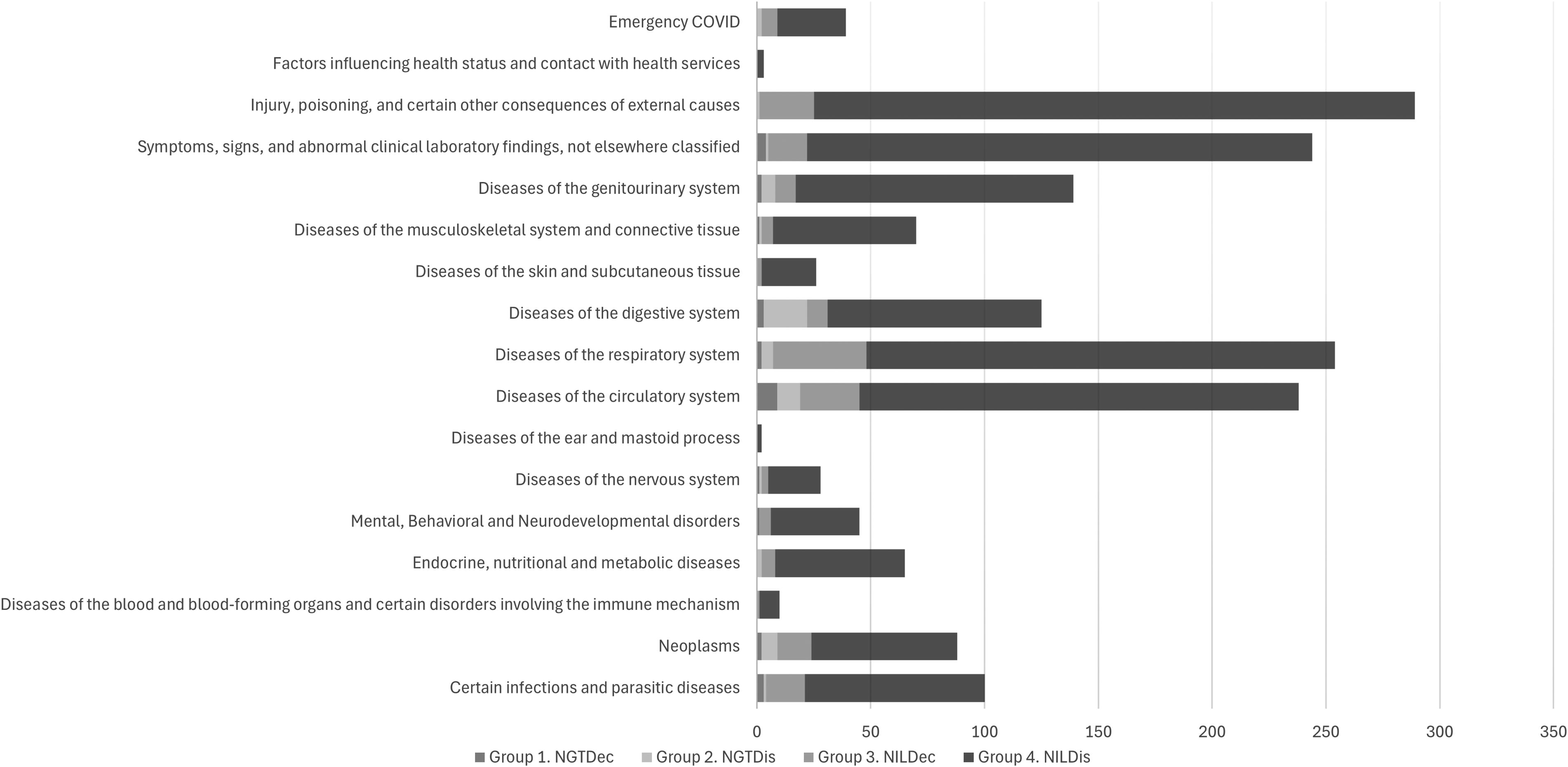
Chart showing the comparative causes of admission by group.
NGT and EOLC
Eighty-four (4.8%) of the 1765 unique admissions were flagged for an NGT procedure (female n = 41, 48.8%). Of the 1002 females identified during the audit, 41 (4.1%) had an NGT flag as opposed to 43 (5.6%) of the 763 male participants identified. Chi-square analysis did not demonstrate a significant relationship between gender and NGT flag (χ2 = 2.278, df = 1, p = 0.131) (See Table 1).
1494 individuals were discharged, of which 56 (3.7%) had an NGT flag. 215 individuals passed away during admission, of which 28 (13%) received an NGT flag. Table 2 shows the end-of-life and admission outcomes by NGT-flag status. Of the NGT flagged individuals, 28 (33.3%) died during admission (female/male = 13/15 [46.4/53.6%]). Of the 56 that were discharged, a further 10 individuals died in three months and two more individuals died within six months. In total 40 (47.6%) of 84 NGT-flagged individuals were deceased within six months. Table 3 shows outcomes by group. Figure 3 shows the relative admission mortality of NGT-flagged individuals compared to those without NGT flags.
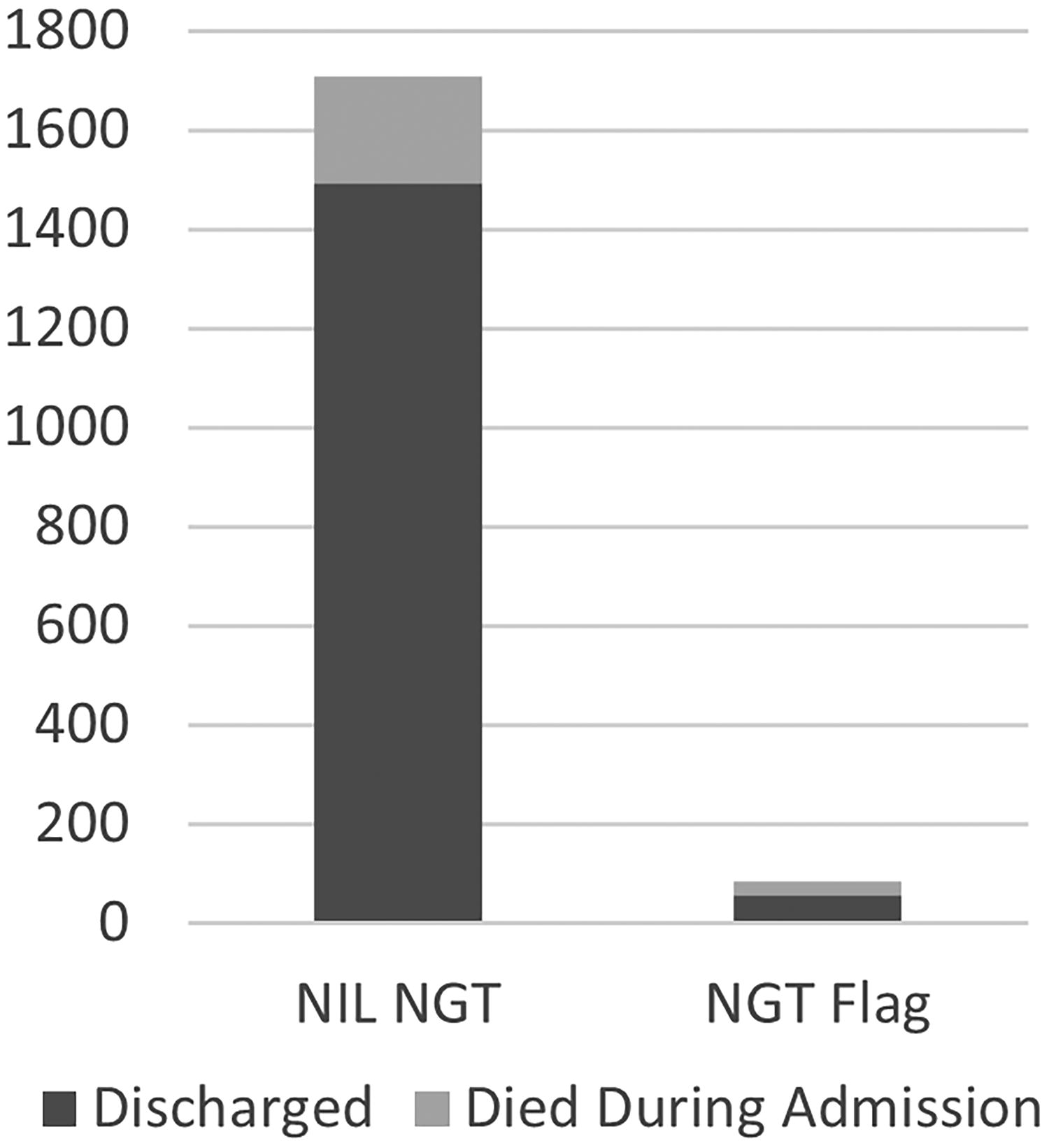
Chart showing relative mortality following an NGT insertion. NGT, nasogastric tube.
Showing Demographic and Admission Data by NGT Flag Status and by Gender. The Outcomes of Comparative Statistical Analysis Examining the Relationships between Gathered Data and the Presence of an NGT Flag Are Shown in the Left Column
Significant statistical analysis outcomes in bold.
Includes those deceased at three months.
Cumulative total includes those deceased as inpatients.
Showing the Demographic and Discharge Data by NGT Flag and Deceased/Discharge Group. The Outcomes of Comparative Statistical Analysis Examining the Relationships between Gathered Data, NGT Flag Status, and Deceased/Discharge Group Are Shown in the Left Column
Bold data represents the significant results.
Includes those deceased at three months. Percentages refer to totals at the top of their respective columns.
Males appeared more likely to pass away during admission—15.7% (n = 120) of 763 admissions passed away in hospital compared to 9.5% (n = 95) of females. Chi-square analysis demonstrated a significant relationship between gender and death during admission (χ2 = 15.799, df = 1, p = < 0.001). Similarly, males were deceased in significantly greater numbers at three months and six months.
Chi-square analysis demonstrated a significant relationship between death during admission and NGT Flag (χ2 = 36.888, df = 1, p = < 0.001). Similarly, chi-square analysis demonstrated a significant relationship between NGT flag and death within three months and six months (see Table 2).
Age on admission
The NGT flag group was slightly younger (mean = 78.7 years) than the non-NGT flag group (mean = 83.0 years). An independent samples t test demonstrated that this was a significant difference (t = 4.568, df = 1763, p = < .001), two-tailed. When considered by group (see Fig. 4), group 2 was the youngest (77.2 years), whereas group 3 was the oldest (these groups are inverted when considering LOS—see below). Between-subjects ANOVA demonstrated a significant effect of group on age (F [3,1761] = 10.390, p = <.001). An independent samples t test also demonstrated a significant difference in age on admission between groups 1 and 2 (t = 2.576, df = 82, p = 0.012).
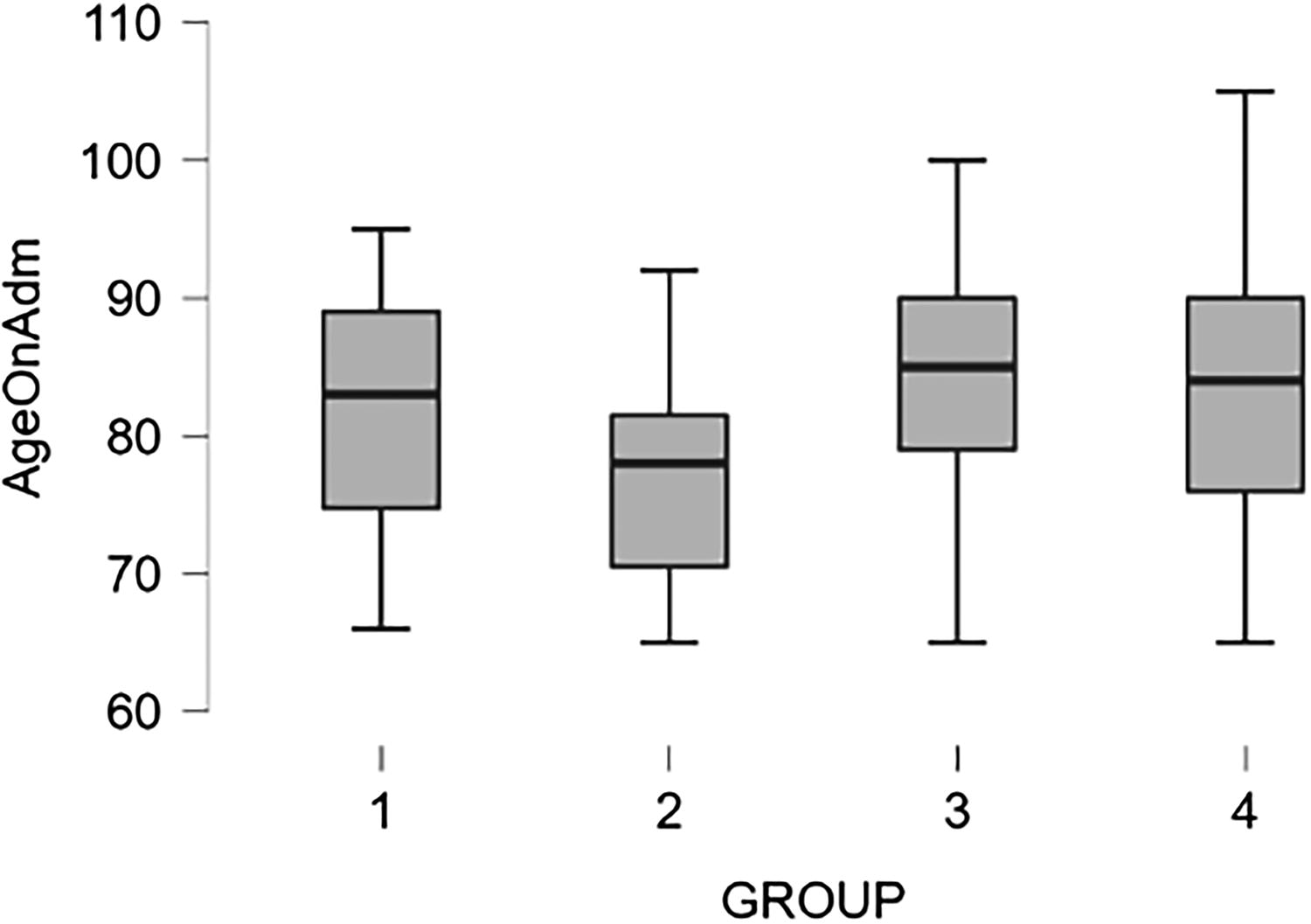
Boxplot showing age on admission by group (inc. Outliers).
Length of stay
Taken as a whole, the NGT flag group had a longer LOS (mean = 31.6 days) than the non-NGT group (mean = 21.2 days). Mann–Whitney tests demonstrated that this was a significant difference (W = 53266.500, df = 1763, p = < .001) two-tailed. Two LOS outliers with LOS >200 days were identified: one male in group 2 and one female in group 4; however, their presence did not impact the statistical significance of this analysis.
When considered by group, group 2 had the longest mean LOS (36.2 days), groups 1 and 4 had similar mean LOSs (22.3 and 21.1 days, respectively), and group 3 had the shortest LOS (16.5 days). This difference in LOS between groups was statistically significant (χ2 = 20.877, df = 3, p = <.001). However, the difference in LOS identified between groups 1 and 2 was not significant (W = 590.500, df = 81, p = 0.067).
Dementia flag
A small proportion (3.1%) of the 324 individuals with a dementia flag also received an NGT flag; no significant relationship between the dementia flag and the NGT flag was identified.
Sixty-one (18.8%) of the 324 Individuals, with a dementia flag identified in the dataset died during admission compared to the 154 (10.7%) of the 1441 who did not have a dementia flag. Chi-square analysis demonstrated a significant relationship between dementia flag and death during admission (χ2 = 16.385, df = 1, p = < 0.001), death within three months (χ2 = 25.514, df = 1, p = < 0.001), and death within six months (χ2 = 20.355, df = 1, p = < 0.001).
When considering only those with NGT flags, a larger proportion of group 1 (NGTDec), who passed away during admission, had a dementia flag (28.6%), compared to the 3.7% in Group 2 (NGTDis) who were discharged. The difference identified was significant (χ2 = 11.124, df = 1, p = < 0.001), suggesting the presence of a dementia flag in those with an NGT placed is associated with death during admission.
Discussion
The aim of this audit was to identify and quantify instances of “non-beneficial” NGT insertion at the end of life. The trust policy recommends that NGT feeding may need to be considered where an individual presents with a MUST score of 2; however, findings from this audit show that a very small percentage of these individuals receive NGT feeding. It is noted that a significant proportion of the individuals that do receive NGT insertion pass away during admission (33%), and almost 50% are deceased within six months. Subsequently, these treatments could be labeled non-beneficial treatments.
The high level of mortality post-NGT insertion is in line with previous similar findings, which demonstrate that approximately 50% of artificially fed dysphagic stroke patients do not survive to six months. 29 Similarly, another poststroke study demonstrated that those who receive temporary enteral feeding (e.g., NGT) have a higher mortality within 30 days post discharge compared to those who receive a permanent enteral feeding (e.g., PEG—percutaneous endoscopic gastrostomy), 30 though the latter group had higher rates of significant disability than NGT-fed peers who survived the admission.
Non-beneficial NGT insertion may occur due to difficulty identifying reliable end-of life-markers, meaning imminent death is not recognized by the medical team,4,31 as a time-limited enteral feeding trial, 13 or secondary to pressure from family members who continue to push for any perceived potential life-sustaining treatment or nutritional sustenance. 32
Though the cost of NGT insertion is minimal, £75–158.64,1,9 this is dwarfed by the cost of an acute hospital stay: £351–586.59 per day (NHS Digital, cited in Guest et al., 2019 11 ) The cost burden of non-beneficial NGT insertion lies in the hospital stay required to maintain the NGT tube. If non-beneficial NGT insertion is avoided, this could facilitate a timely discharge to an appropriate residence for palliative or end-of-life management, thus reducing costs associated with an acute stay, while simultaneously improving quality of life by reducing unnecessary hospital stays and avoiding death in hospital. 33
Beyond hospital admission, NGT insertion itself can have a negative impact on QoL and has been described as uncomfortable and tortuous. 34 Should their presence undermine an individual’s comfort or QoL in their last days, their placement at the end of life, particularly if combined with the use of restraints, may also be considered a non-beneficial treatment 20 and should be avoided.
Those who could be considered to have received a non-beneficial NGT insertion (group 1/NGTDec) had a shorter LOS than those who received “beneficial” tube feeding (Group 2/NGTDis). Group 1 may represent a previously identified “sub-group” of NGT-fed individuals who demonstrate early mortality in conjunction with a reduced LOS 30 and who may have been treated with an appropriate palliative approach, whereas the requirement for ongoing nutrition increased LOS. It has been suggested that an optimal palliative approach provided by geriatricians may have facilitated admission survival, 35 which may also explain the high proportion of death that occurred post discharge in the NGT-fed group. A multicenter study highlighted that LOS is impacted by age, complexity of care, and length of time enteral feeding is required. 36
Group 1 were significantly older than their NGT-fed peers in Group 2, though younger than the group who were not fed. Being elderly is associated with an increased risk of a variety of comorbidities, including dysphagia, which is also linked with malnutrition.16,37 Elderly individuals are more likely to require a palliative care consultation. 38 Due to the multifactorial nature of malnutrition, evidence is limited that enteral feeding will meet nutritional goals. 1 This suggests that age may play a factor in determining whether an individual is appropriate for NGT insertion, likely through an association with increasing frailty, 37 which may be a more useful indicator of the likelihood that a specific intervention may be required or implemented. 39
The presence of a dementia flag was significantly associated with death during admission, including where an NGT had been inserted. Alverez-Fernandez et al., (2005) 4 found that the presence of an NGT tube was an independent risk factor for a shortened survival in patients with dementia. Individuals with dementia are likely to be impacted by malnutrition; 37 however, guidance exists regarding the appropriateness of enteral feeding, where short-term feeding is only indicated if an individual’s condition is deemed reversable. 13
Advanced age and cognitive decline are here identified as indicators of potential non-beneficial NGT placement. These indicators should factor into decision-making conversations with patients and next of kin, both in the acute setting (the remit of this audit) and as part of advanced care planning, which seeks to manage complex decisions and potentially avoid unnecessary or unwanted hospital admissions and associated interventions. 40
Limitations
Firstly, the sample sizes of the identified groups are underpowered for robust conclusion, yet suggest important data trends. Secondly, as an audit of a single trust, the quantity and proportion of non-beneficial NGT insertions identified may not represent events at other trusts. Future research could replicate the audit to demonstrate consistency of trends. Thirdly, the audit data only cover individuals who receive a MUST of 2 and may exclude those who received NGT insertion in anticipation of a MUST score of 2, which was successfully negated through the provision of nasogastric feeding, Thus potentially excluding those who received both beneficial and non-beneficial NGT insertion while never reaching a MUST of 2. Similarly, the audit data do not distinguish between NGT’s inserted for enteral nutrition or gastric drainage. Finally, individuals with permanent enteral feeding already in situ were not identified or excluded prior to extraction of audit data. These individuals may have been less likely to receive a temporary NGT insertion given they already had an enteral feeding route in situ.
Future research intends to map the decision-making pathway of non-beneficial NGT insertion by reporting the occurrence and timing of key decision-making events that lead to the initiation of NGT insertion.
Conclusion
The act of NGT insertion may be unpleasant and ultimately non-beneficial. Within the current audit data, a significant proportion of individuals who received NGT insertion passed away during admission, and the mortality rate within six months was approximately 50%. Older age at admission appears to be a factor in NGT insertion and in whether those NGTs could be considered non-beneficial. The presence of a dementia flag did not appear associated with NGT insertion, though it was associated with “non-beneficial” NGT insertion. Furthermore, research into the identification of acutely unwell, in-hospital individuals who will benefit from acute NGT insertion is required.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work is supported by Applied Research Collaboration, Kent, Surrey and Sussex, University Hospitals Sussex NHS Foundation Trust, East Sussex Hospitals Trust and the University of Chichester.