
Abstract
Introduction
Palliative care (PC) is defined by its holistic and multidisciplinary approach to supporting the quality of life and well-being (physical, psychosocial, emotional, and spiritual) of people living with life-limiting illness.1,2 Ageing populations, the prevalence of chronic progressive diseases, and advances in diagnosis and treatment combine to mean that the need for PC is increasing worldwide.3-5 The World Health Organization has encouraged its member states to actively address “this global challenge,” and multiple countries have responded to this call through both policy development and practical and innovative strategies.6-8
Massage is a broad descriptor of practices incorporating numerous methods of manipulation of the soft tissues of the body. 9 Within mainstream (Western) health care, massage is applied as a restorative or rehabilitative technique within physical therapy (physiotherapy) and, traditionally, within nursing practice as a means of fostering comfort for hospitalized patients.10,11 In parallel, massage has sustained a presence outside conventional or mainstream health care, and from this domain a subset of massage practice, defined and known throughout the Western world as massage therapy (MT), has emerged. Conceptualized as a professional, multidimensional health care discipline, MT applies therapeutic skills of touch to address a wide spectrum of conditions for both specific and general benefit. 9 With a growing body of evidence of benefit, evidence-informed practices, and discipline knowledge located within a strengthening educational and regulatory environment, MT is increasingly being recognized as a safe, efficacious, non-pharmacological intervention or treatment that warrants “wider integration into the community of health care professions.”12,13 This shift in the perception and role of MT is illustrated by recently published guidelines of the National Consensus Project for Palliative Care (NCP) in the United States and the American Society of Clinical Oncology (ASCO) that recommend MT as a pain relief and well-being measure in the context of advanced cancer and PC.14,15
For the most part, however, massage retains its characterization as a nonmainstream, complementary therapy. 16 Complementary or integrative therapies, practices, or medicine (initialized as Complementary Therapies, Complementary and Alternative Medicine (CAM), or Complementary and Integrative Medicine (CIM), with the latter acronym applied here) are defined as patient-centered, holistic, evidence-informed health care approaches applied alongside conventional treatments to promote health, healing, and well-being.17,18 In the Western world, the use of CIM therapies is highly prevalent outside mainstream health care. 19 This is most apparent in the context of cancer, where patients utilize CIM practices, including massage, to augment conventional treatments, to relieve symptoms of disease and the effects of treatments, or to enhance quality of life and well-being.13,19,20
Integration of CIM practices (including MT) within conventional settings is a current topic of interest and research activity concerned with establishing evidentiary justification and feasibility, and identification of both barriers and facilitators to their integration and implementation within mainstream health care.21B22 -24 As both an emerging and complementary health care professional discipline, MT sits within this dynamic, evolving environment.
Previous systematic, narrative, and scoping reviews that have investigated the role of massage in the context of PC have predominately focused on investigating and describing its effectiveness and potential benefits, most often as one of a group of CIM approaches, and less often as massage alone.25B26 -29
To our knowledge, no previous reviews have comprehensively explored or mapped the evidence related to characteristics of massage service delivery in mainstream palliative health care settings, whether hospital, hospice, or community-based.
For this scoping review, the primary research question was:
What are the characteristics of massage service provision in PC?
Supplementary questions were:
What drives PC organizations to offer massage services? How is massage in PC conceptualized? (What is it?) How is it operationalized? (What is its scope and who provides it?) How is its value determined?
Methods
Study design
The review followed the Johanna Briggs Institute (JBI) methodology for scoping reviews, with additional reference to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) reporting guidelines.30,31
Protocol
A protocol was designed to develop the research question, to select criteria for study and document inclusion, to develop a data search strategy and to determine the methods for collation, charting, and reporting of results. The protocol was registered prospectively at Open Science Framework: https://doi.org/10.17605/OSF.IO/C6Q7Y.
Eligibility criteria
This review followed the Participants, Concept, and Context (PCC) framework recommended by JBI.
The
The
The review included peer-reviewed studies using quantitative, qualitative, or mixed methods, as well as gray literature such as government reports and publications of health care organizations and policy bodies. Only English-language publications from 2013 to 2024 were included, the time range selected to ensure recency, relevance and manageability.
Studies were excluded if they focused on general palliative approaches (rather than specialist care), included therapies similar to massage (like aromatherapy), lacked massage-specific data, or were review articles or meta-analyses.
Search strategy and information sources
A comprehensive three-step literature search was conducted with support from an academic librarian. The initial search in Medline (Ovid) helped identify relevant keywords and index terms, which were then used in broader searches across EMBASE, CINAHL, and PsychINFO. AMED was a post-protocol addition. Reference lists of included studies were also manually reviewed. All citations and full texts were managed using EndNote X8. Major search terms included concepts related to PC and MT, using both keywords and MeSH terms tailored to each database. A similar strategy was applied to searches of ProQuest and relevant organizational websites for reports and unpublished materials between November 1–30, 2024. A repeat search was conducted to include recent publications. Due to the complexity of the topic, the strategy was refined iteratively throughout the process (Supplementary Data S1).
Data extraction
A data extraction chart was developed within Covidence, a customizable online platform, and was modified in an iterative process to better capture relevant data. To further assist in the categorization and examination of data related to the concept of interest, a deductive approach was used, informed by the Donabedian framework. 32
Comprised of structures (S), processes (P), and outcomes (O), the Structure Process Outcome (SPO) Donabedian framework facilitates the identification of a guiding vision or philosophy, and the implementation, provision, and evaluation of a health service. Extracted study and report data included the primary author, date, country of origin, type of study or report, participants included in the study, setting of the study, aims of the study or report, and a summary of findings mapped to the SPO framework as they align with the objectives of the review (Tables 1 and 2).
Parameters of Data Extraction
Characteristics of Included Studies and Reports
MT, massage therapy; PROM, Patient-Reported Outcome Measure.
A narrative description of the results is further elucidated by additional tables and figures.
Results
Search of the identified databases, Medline (Ovid), EMBASE, CINAHL (Ovid), PsychINFO (EBSCO), and AMED, yielded 2893 records after the removal of 1303 duplicates. Titles and abstracts were screened for relevance applying the eligibility criteria. A total of 257 studies progressed to full-text screening. Further screening resulted in 26 studies selected for inclusion in the review. Two studies were subsequently merged at the data extraction stage,42,43 leaving 25. In addition, 6 reports identified as relevant gray literature were included, meaning that a total of 31 studies and reports were available for charting and analysis. The selection process, including reasons for exclusion, is summarized in the PRISMA chart (Fig. 1).
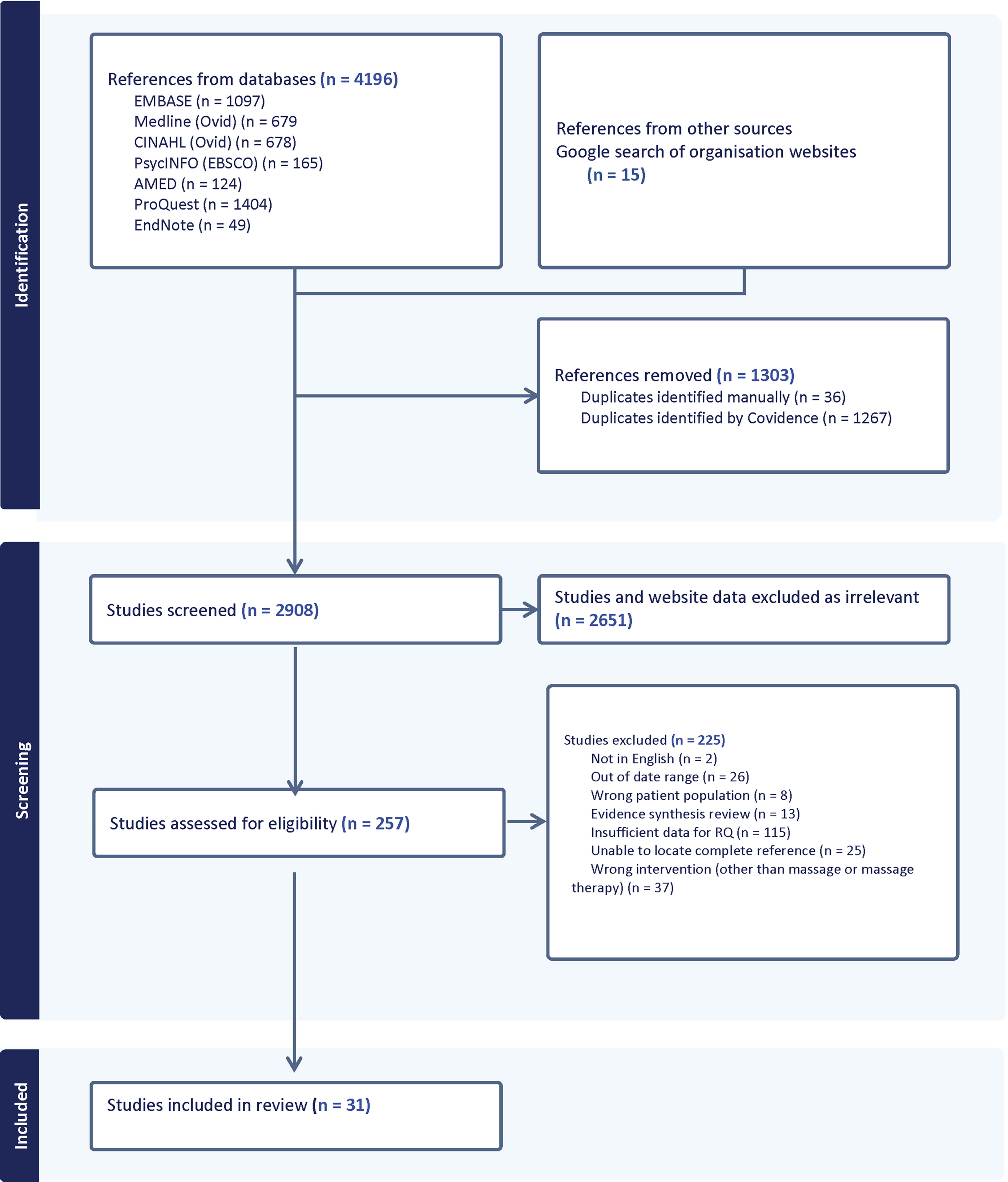
PRISMA study selection flowchart. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study characteristics
The review included 31 studies and reports from 6 countries, with the majority from the United States (n = 17), followed by Australia (n = 4), the United Kingdom (n = 4), Canada (n = 3), Iran (n = 2), and Israel (n = 1). Participant groups across 25 studies (in some studies more than one group was represented48,55,59) included adult (77%) and pediatric (20%) palliative or advanced cancer patients receiving massage; clinicians and health professionals (8%); PC administrators (16%); and researchers (6%). Policy, advocacy, and knowledge resources (gray literature) represented 19% (6/31) of the total studies and reports. Study settings varied and included large (>200 patients) metropolitan public hospitals with dedicated PC units, smaller hospitals, hospices, and mixed PC environments in regional, rural, or metropolitan settings.
All 31 studies and reports, to a greater or lesser extent, contributed data relevant to the review objectives. Of the 25 eligible published studies, 14 (62%) addressed massage as part of a broader group of complementary and integrative medicine (CAM/CIM) practices.25,33-35,39,41,42,46,48,51,53-55,59 Nine studies (36%) focused exclusively on massage,38,40,44,45,47,49,52,60,61 and two studies (12%) examined massage in combination with other therapies, such as music, art, and physical therapy (Table 2).36,37
Types of studies and reports
A diverse range of study designs were included in the review. Among the seven quantitative studies were three randomized controlled trials,44,60,61 three prospective studies,45,46,53 and one pilot study. 36 There were four qualitative studies, including two nested within larger quantitative studies,39,47 one modified Delphi study, 59 and one phenomenological inquiry. 38
Eight studies used mixed methods, including a retrospective outcomes review, 52 an outcome study, 49 an assessment review, 33 three descriptive reports,25,40,43 and two evaluation reports.34,35 The four included surveys gathered quantitative and/or qualitative data from PC provider organizations.37,41,51,55
Additional sources—including gray literature—consisted of a discussion paper, 48 policy recommendations, guidelines and information sources,56,58,62,63 and a blog post. 57 We applied the Donabedian framework to examine the study results (Tables 1 and 2 and Figs. 2–8).
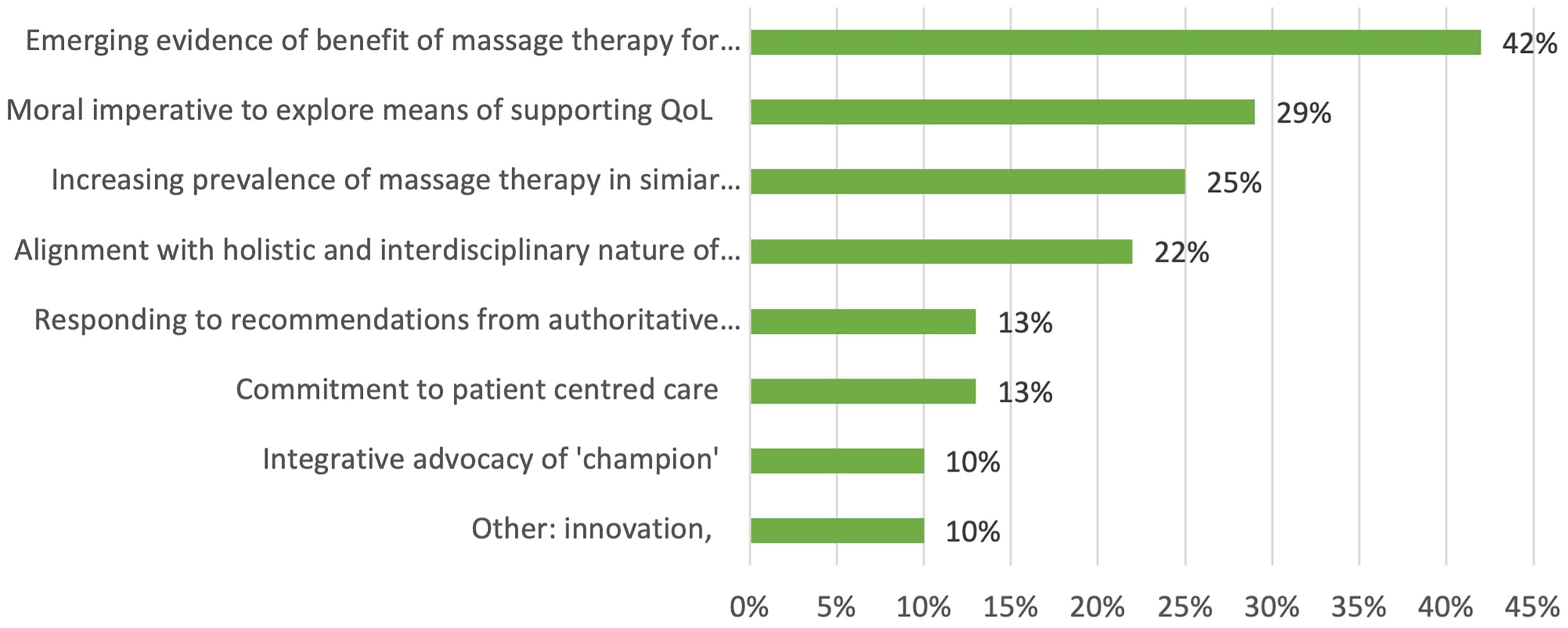
Facilitators: values, philosophies, principles (n = 31 studies).
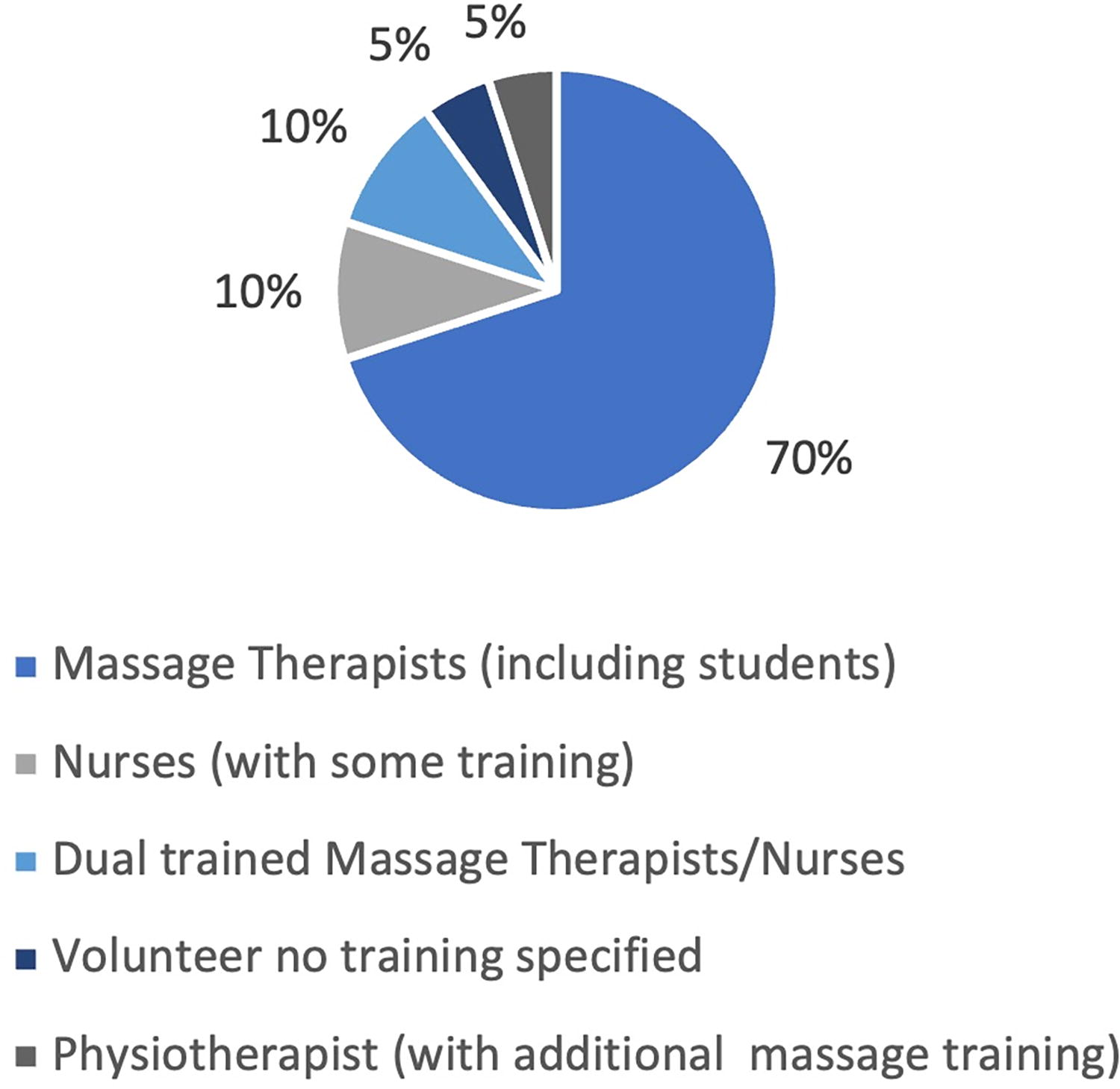
Provider identity percentage reported in studies (n = 20).
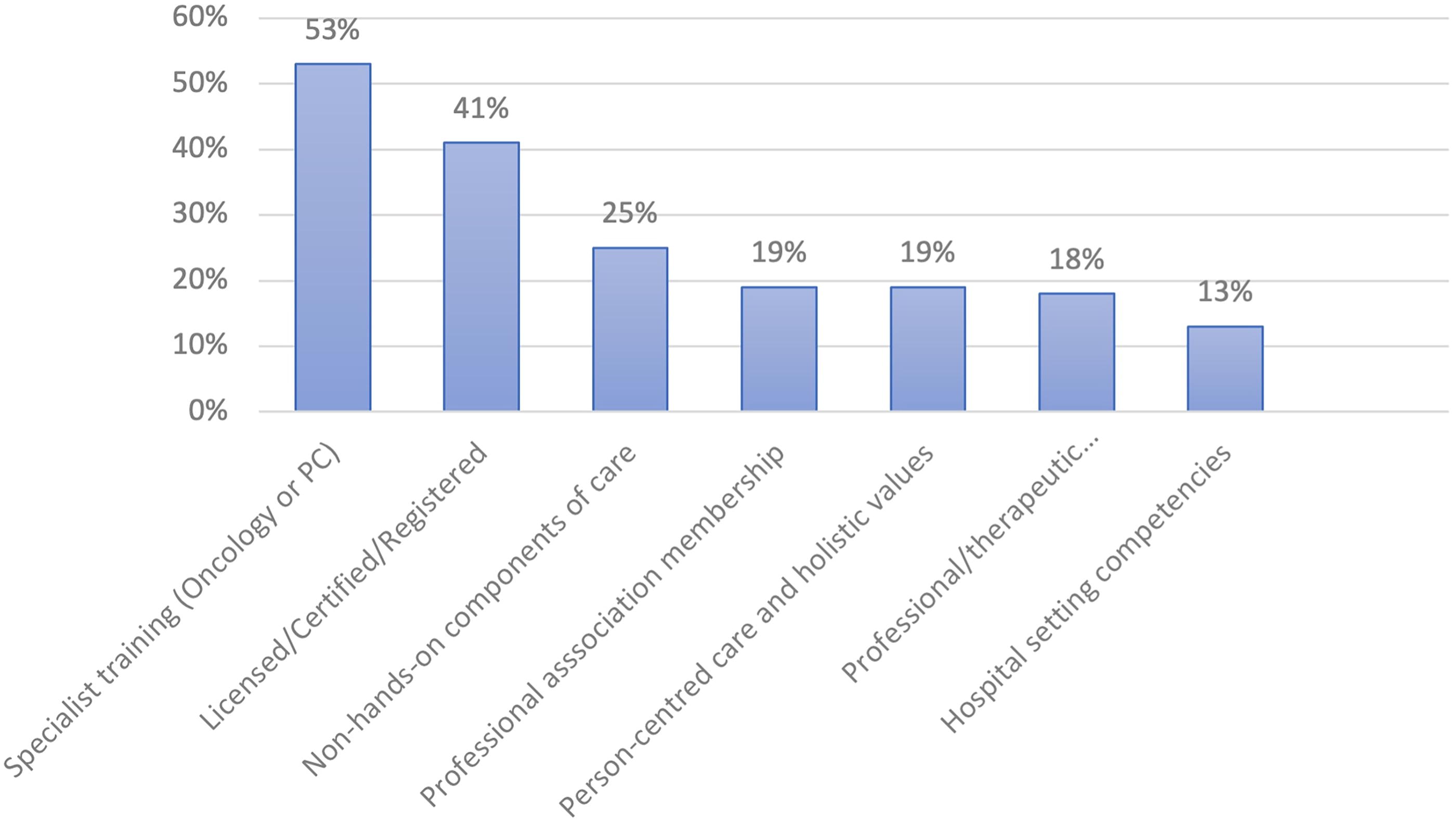
Percentage of studies (n = 15) reporting massage provider characteristics.
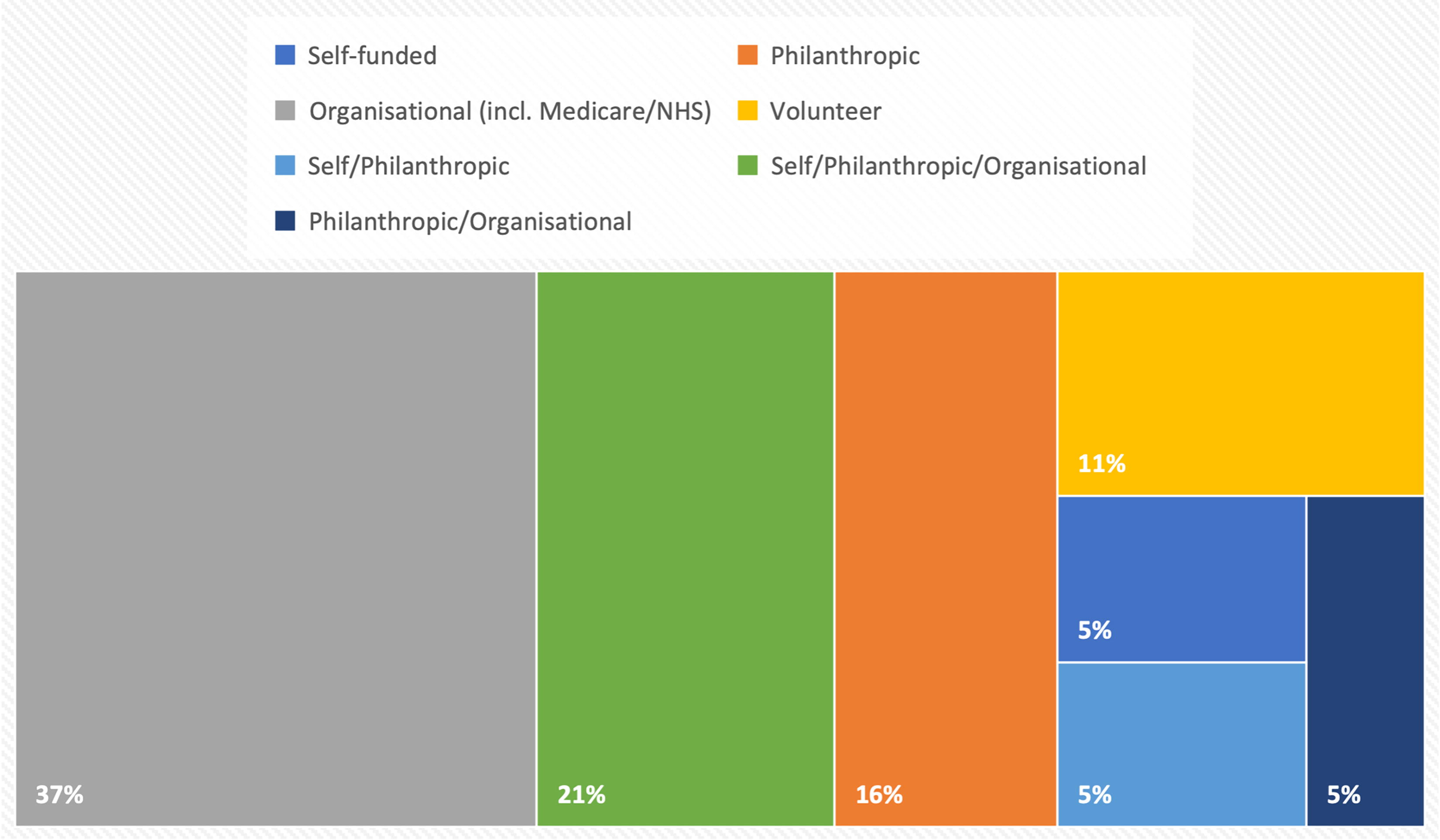
Funding models of studies, expressed as percentage.
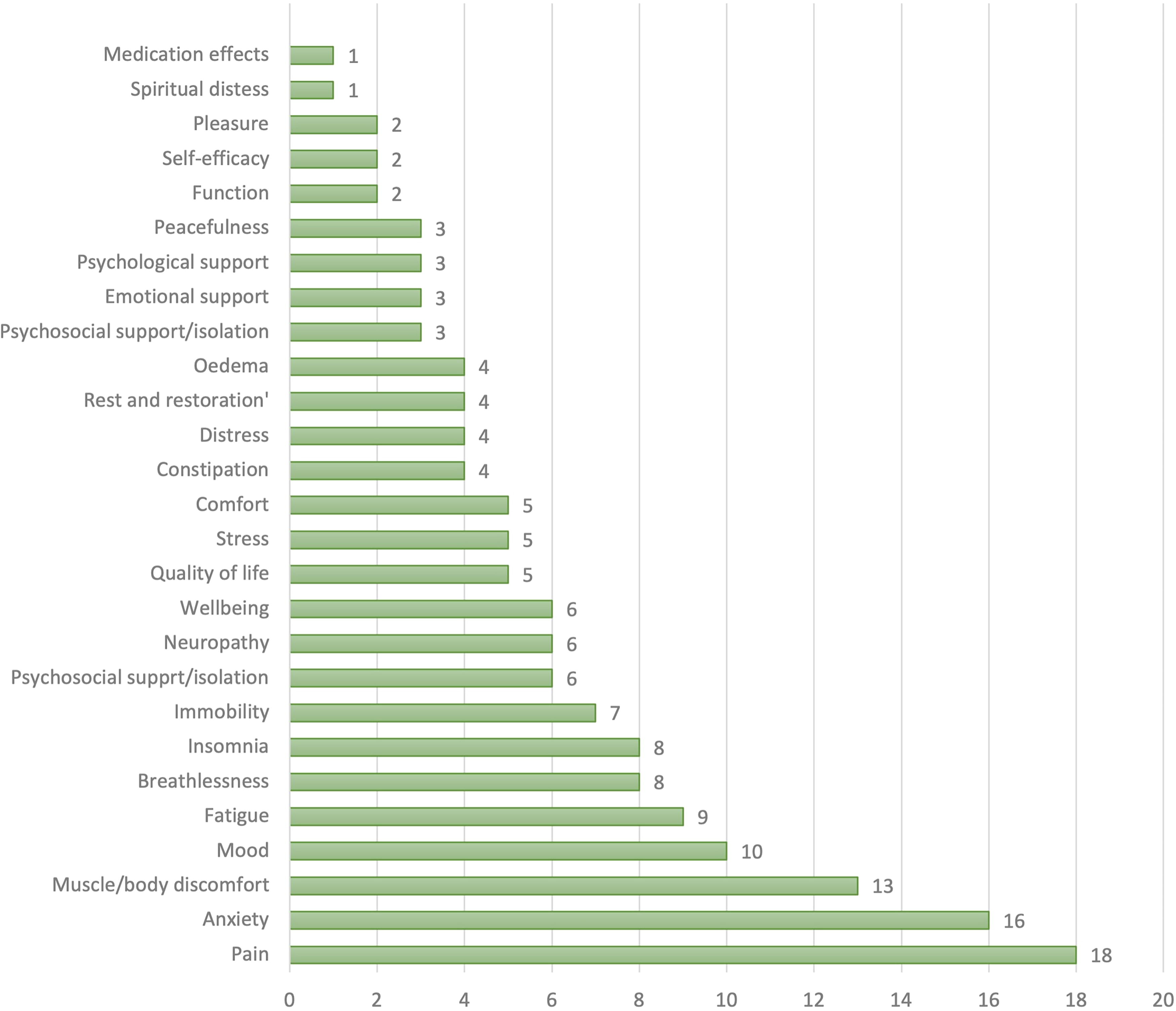
Frequencies of reasons, referral indicators, and outcomes reported across all (n = 31) reports and studies.

Outcomes assessment instruments reported in n = 14 studies.
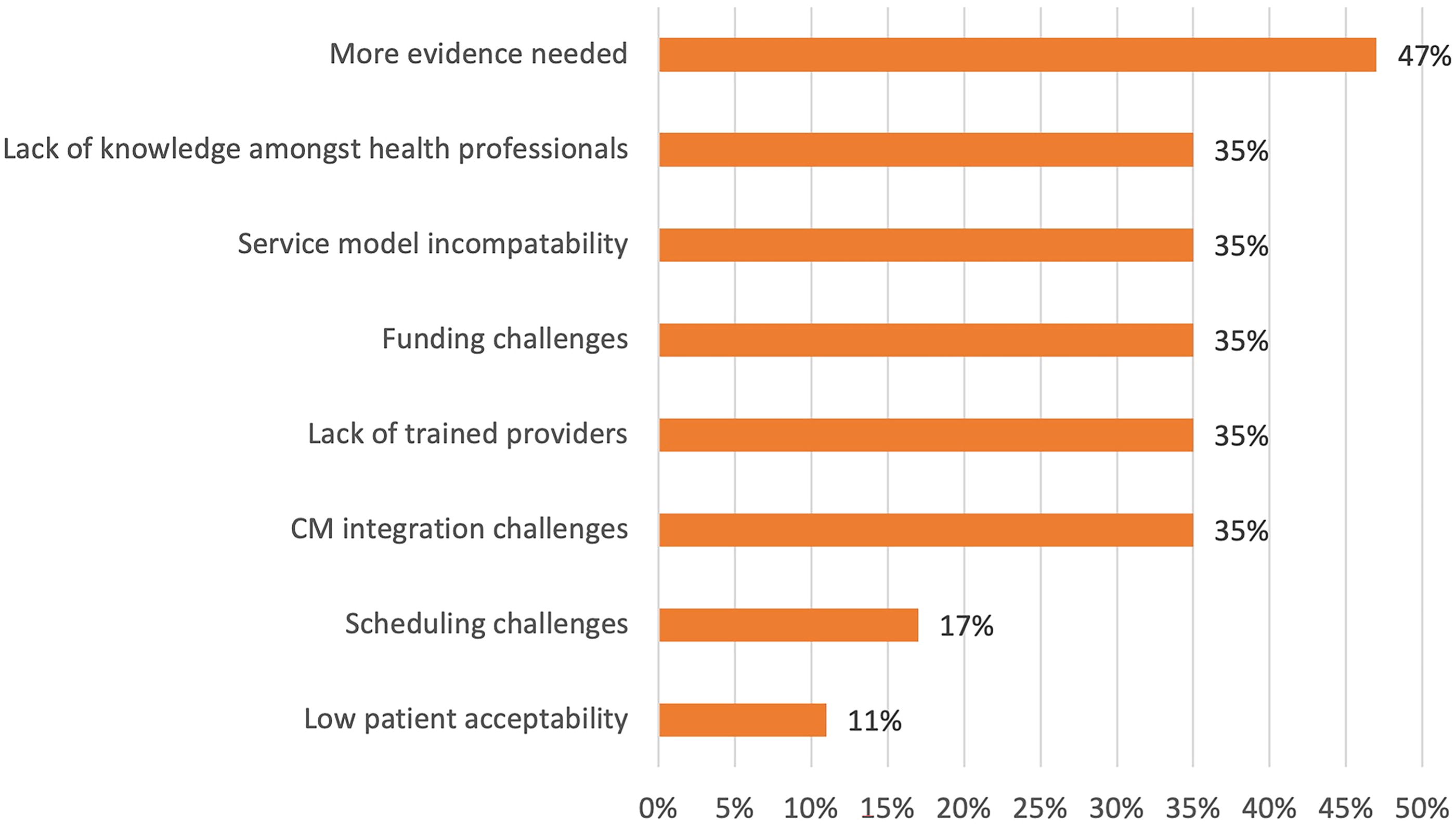
Barriers and limiting factors identified in n = 17 studies or reports.
What Is It? Definitions
Massage
With a deep and wide historical and cultural background, massage is a broad descriptor of practices incorporating numerous methods of manipulation of the soft (muscle and connective) tissues of the body.
(Adapted from Kennedy 2016 and Mao 2022).
Massage therapy
MT is characterized by its holistic, multidimensional, skilled application of numerous modalities of touch and massage to address specific and general physical issues. It includes non-hands-on components of care, such as health promotion and self-care education. MT, and its outcomes, can be influenced by therapeutic relationships and communication; therapist education, skill level, and experience; and the therapeutic setting.
(Abridged Kennedy 2016).
Palliative and oncology massage therapy
A person-centered care approach, grounded in compassion and therapeutic relationship, oncology and palliative massage is the application of modified techniques of MT. It prioritizes comfort and well-being, alleviates symptoms, reduces suffering (physical, emotional, or psychological), and is provided as a supportive, complementary component of care within a broader team of health professionals.
(Adapted from Dain 2015, Berger 2013, and Society for Oncology for Massage https://www.s4om.org/)
Structure
Organization vision, values, or rationale
All studies and reports identified values, philosophies, or rationales underpinning the provision of massage in PC. The existence of evidence or emerging evidence of the benefit of MT for palliative patients was cited in 13 studies (13/31, 42%). Nine (9/31, 29%) studies referenced the moral imperative to explore means of improving quality of life and symptom management, seven (7/31, 22%) studies noted the natural alignment of MT with the holistic and interdisciplinary nature of PC as a value, and eight (8/31, 25%) referred to the increasing prevalence of MT in similar settings as a rationale for exploring its application in a PC setting. The integrative philosophy or vision of an individual “champion” within an institution or organization was mentioned in three studies (3/31, 10%), and responding to recommendations from authoritative bodies was reported in a further four (4/31, 13%). In four studies (4/31, 13%), other values expressed were a commitment to patient-centered care and the fundamental desirability of responding to expressed patient needs or preferences. In a further three (3/31, 10%), innovation was asserted as an intrinsic value in health care (Table 2 and Fig. 2).
Provider personnel and provider credentials
Data related to identification of the personnel providing massage were available from 20 studies (20/25, 80%). Fourteen reported professional massage therapists.36,37,39,40,43B44 -47,49,52,53 This included senior-level student massage therapists in two studies.34,38 Two studies reported dual-trained nurse/massage therapists,33,54 and one study identified physiotherapy (with additional massage training) as the provider discipline. 25 Volunteers, with unspecified training, were reported in one study, 55 and in two studies the providers were nurses with “some” massage training (Fig. 3).60,61
Advanced or specialized training for massage therapists that included PC, oncology,25,43,47,49 or pediatric massage training36,52 was referred to in several studies and reports. The Hospital-Based Massage Therapy Competencies for Optimal Practice in Integrated Environments and training providers recognized by the Society for Oncology Massage were cited as sources or pathways for training, education, and credentialing of massage therapists working in PC settings.43,44,47,64 Communication, interpersonal, or psychosocial skills training were also indicated in three studies.39,44,45,52 Berger 34 reported that in those Canadian provinces where MT is formally recognized as a health care profession, end-of-life education was mandatory for massage therapists. Other qualification-related factors reported were professional association membership (inclusive of codes of ethics, standards of practice, and insurance provisions) and commitment to person-centered care and holistic values. Attention was drawn to the need for advanced education, including non-hands-on components of care, 52 such as coaching and caregiver education. 45 Recommendations for specialized training were also advanced by the Society for Integrative Oncology (SIO/NCCIH), 63 ASCO, 15 Palliative Care Australia (PCA), and Cancer Research United Kingdom (Fig. 4).
Clinical governance
Nine studies reporting on established massage programs provided data related to governance (9/13, 69%). Four described the delivery of MT in formally integrated services or dedicated departments within their respective hospital settings.25,33,43-45,52 Other aspects of governance reported were contractual arrangements, 43 covering scope of practice and regulatory requirements for the conduct of massage services, 54 including policies and procedures for incorporating massage services into existing hospital PC or hospice models of care.35,43,54 Responsibilities of leadership teams and program coordinators were briefly described in three studies (Table 2).35,45,49
Funding
Data related to funding for massage services were provided in 19 studies and reports (19/31, 61%). Three broad classes of revenue sources were described: institutional, philanthropic, or self- or patient funding. Institutional funding included operational revenue, Government, and insurance contributions (such as NHS in the United Kingdom; Medicare or Veteran Affairs in the United States).
Philanthropic funding comprised tied endowments, hospital foundation contributions, and other donations. Seven studies (7/19, 36%) provided massage services through institutional funding alone. Five studies (5/19, 26%) reported funding from patient and philanthropic sources. Two studies reported volunteer provision of massage, and three reported patient funding alone. The remaining study identified the hospital’s operational funding stream combined with contributions from its foundation arm as the source of funding (Table 2).
Processes
Referral sources
Eight studies that reported on established programs (8/13, 61%, 8/25, 32%) identified referrals to massage treatment originating from other health professionals within the PC setting, including from rehabilitation and other inpatient departments 39 or from medical, nursing, or social work personnel.34,36 Several programs included capacity for self- or family-member referrals (Table 2).43,46,54
Reason and referral indicators
All studies, reports, and policy documents referred to symptoms or issues for which massage was or could be applied. In the experimental studies, predetermined sets of referral indicators were evaluated for outcome effectiveness, including a symptom cluster consisting of pain, anxiety, insomnia, and fatigue.60,61 In the controlled trial conducted by Groninger et al., 44 effects of massage in relation to overall quality of life (including physical, emotional, and spiritual domains), and pain, distress, tiredness, drowsiness, peacefulness, depression, and fatigue were investigated. For studies reporting on established programs, either single- or multi-site settings, referral indicators or reported outcomes related to physical and emotional well-being were extensive, as can be seen below (Fig. 6).
Massage treatment descriptions, protocols, or clinical guidelines
Precise treatment protocols, required to meet a randomized controlled design, were described by Miladinia et al.60,61 and comprised technique, duration, and setting specifications. In contrast, the randomized controlled trial conducted by Groninger et al. 44 took a “real-world” approach, and individualized, therapist-devised treatments, informed by patient presentations and input from members of the care team, were applied. Individualized and therapist-tailored treatments were the predominant approaches applied in the remaining studies, with modifications focused on patient health status, need, and preference to pressure, positioning, body site, pacing, and duration.45,47 Non-hands-on components, such as caregiver or psychosocial support or education for self-massage, were also reported. 36 No studies of established programs reported or described the presence of specific clinical guidelines (Table 2).
Interdisciplinary participation
Eleven of the studies of extant massage programs (11/13, 84%) reported massage therapist participation in interdisciplinary or whole-of-care team activities. This included collaboration with other team members in planning patient care and co-treating with other disciplines, such as psychologists, physical therapists, nurses, music therapists, and social workers.36,40,52 Participation in interdisciplinary meetings, case discussions, and rounds were reported as examples of team-oriented approaches incorporating MT contributions.43,49,54 Inclusion by all care providers including massage providers in team-oriented approaches to care was a recommendation in the NICE Cancer Service 62 and National Center for Complementary and Integrative Health guidelines 63 and was further advocated by Cates 57 and Havyer. 45
Documentation of massage treatments
Five of the studies of extant programs (5/13, 38%) provided data related to documentation practices of massage providers, including “read and write” access to medical records. Routine entering of clinical notes (subjective, objective, assessment, and plan—SOAP) in electronic medical records and Patient-Reported Outcome Measure (PROM) data was reported (Table 2). 43
Outcomes and evaluation
To identify the tools and instruments applied to measure outcomes of massage provided in the included studies, data were extracted from those studies that investigated effectiveness of massage in controlled trials or outcome studies, and from those that reported on established programs where outcome measures were routinely applied. Fourteen studies (14/25, 56%) reported data relating to assessment instruments and other evaluation strategies (Table 2 and Fig. 7).
Seventeen of the total studies and reports (17/31, 54%), in evaluation of their variable status, identified actual or potential obstacles and challenges to the implementation or provision of MT services in PC settings (Fig. 8).
Discussion
This review examined characteristics of massage services in the context of PC, and we develop below our key findings about the way massage was conceptualized and operationalized in this setting.
A seminal finding of this review was the consensus identified in all studies and reports recognizing the benefit of massage in ameliorating symptoms and enhancing the physical and emotional well-being of people with life-limiting illness. This position accords with guidelines advanced by the NCP (USA), the SIO, and the ASCO.13-15
Equally robust findings in the review related to the characteristics of massage providers and the processes involved in massage service delivery. Where specified, the dominant providers of massage were identified as professional massage therapists (including a small representation of senior-level student massage therapists). Nurses, dual-trained nurse/massage therapists, physiotherapists, and volunteers with or without formal training were also identified as providers. Diversity of provider identity is consistent with earlier reviews and studies, indicative of uncertainty or lack of clarity about to whom the role “belongs.”65-67 While massage training has retreated from the curricula as a routine or required nursing competency, there are segments of the nursing profession that maintain a role for nurses as massage providers.11,68 However, the prevalence of massage therapists (described in the review studies as licensed, registered, or qualified, depending on jurisdiction) reported as massage providers was significant, as it illustrated a decline during the most recent decade in the provision of massage in hospital PC and hospice settings by both nursing staff (unless dual-trained) and by volunteers.
Amplifying this significance, attention was drawn in several studies to the need for specialist or advanced education and training for massage therapists attending palliative populations.25,42,44,52,56 Citing the need to equip therapists with extended knowledge and skills to address the range and complexity of symptoms and psychosocial issues encountered in seriously ill patients, training beyond that required for foundational MT qualification was advocated throughout this review.25,42,44,45,47,52,56-58 Advanced or specialized training was also recommended by SIO/NCCIH and ASCO. 15
Mirroring the changes in provider identity, training, and qualification were procedural elements (the “what and how”) of established massage programs that featured in this review. Factors indicative of a widening scope of practice and an evolving role for MT in PC included the symptoms and issues for which massage was applied,33,34,45 massage treatments that incorporated non-hands-on components of care, “shared knowledge” documentation practices,43,46 and the level of interdisciplinary engagement such as referral processes and collaborative care planning.36,37,39,40,43,44,54 These elements are consistent with measures of levels of integration of MT in other conventional or mainstream health care settings. 24
Changing perceptions concerning, first, the nature of the massage provided to palliative patients and second, the expected or recommended qualifications of providers of massage to this population, have implications for the governance of massage programs in relation to accountability, risk management, and quality control. This may explain the decline, noted above, in volunteer representation during the time frame of the studies included in this review. Earlier studies reported volunteers, both trained and untrained, as providers,34,35,55 whereas later studies were more likely to report employed professional massage therapists. While volunteerism may function as an avenue for financial sustainability of massage services,55,65 it may be constrained in the future by changing governance or legal considerations.
Indeed, taken together, elements highlighted in this review suggest that the practice of massage in PC settings is undergoing a reconceptualization—the surfacing of a new discipline, or at the very least, a specialization within a maturing discipline.
Nilsen 69 describes the emergence of a new discipline in health care as a dynamic process involving the identification of a need (in this case, growing demand for PC), new knowledge (strengthening evidence of efficacy and effectiveness of MT), and policy changes (person-centered-care and patient-experience focus). Predisposing conditions such as these, according to Nilsen, propel development of educational and regulatory pathways in the new discipline, facilitate practice standards and scope, formulate clinical guidelines, consolidate a professional identity, and lead to the recognition, acceptance, and subsequent integration into health care systems. Our findings indicate that MT is immersed in this developmental process.
In countries represented in this review, MT is not a routine presence within hospital or hospice settings, and several studies articulated potential and actual structural and procedural barriers to its introduction or integration.43,44,48
However, with implications for the development and integration of MT services in the future, the review surfaced established massage programs demonstrating that navigation of such obstacles is both desirable and achievable. The Donabedian framework 70 and S.M.A.R.T 54 goals framework were cited in two studies as models for implementation. There were no other attributions to specific implementation models reported. Integration of MT in the balance of extant programs appeared to have been facilitated by customized and context-specific service models developed “from scratch.”43,54 Notable components facilitating integration, encompassing policies and procedures for the operationalization of a PC MT service, were defining the role of massage and its scope of practice within each setting, developing context-driven clinical guidelines, determining the skills, knowledge, and qualifications required of providers, configuring the optimal utilization of service processes, promoting interprofessional and interdisciplinary communication, recognition, and acceptance, and identifying appropriate evaluation strategies.35,39,43 Other key contributors to the integration of massage programs were the active participation in leadership and coordinating roles by senior clinicians with knowledge and training in CIM disciplines as “champions,”33,43 and the formation of dedicated integrative departments or multidisciplinary committees of management to navigate governance requirements.25,45
For the professional discipline of MT (both educators and therapists), the implications flowing from this review concern the work to be done, as proposed by Nilsen, in the development of the identity of MT as a specialization in PC. Further research is needed to clarify scope of practice, to guide content and standardization of optimal training, to explore the impact of specialization on current and future workforce, to consolidate nascent educational pathways (referenced in studies in this review), and to build and disseminate evidence-informed practice guidelines.
Meeting a general requirement to consolidate evidence relating to massage effectiveness and benefit, one study included in this review was concerned with the identification of outcomes of interest for future research. 50 As noted, 44 the use of narrow sets of outcome measures (often selected for research purposes) may limit the identification and understanding of the holistic “hard-to-measure” effects of massage. Several studies in the review confirmed the ongoing need, identified elsewhere,27,71 to attend to less well-documented outcomes of massage, such as transcendence, self-agency, and peace, and to determine how best to measure them in “real-world” practice. The My Concerns and Wellbeing (MYCaW) instrument, nominated in several studies in this review, may offer a pathway to practice “measuring what matters” and capturing the meaningfulness of a massage intervention, but further research is needed to identify appropriate outcome and evaluation strategies.
Our review confirmed a poor level of knowledge among palliative and other health care professionals about the role, scope, and potential benefits of MT for palliative patients.39,43,51 As noted by Nilsen, lack of knowledge and information serve as impediments to the translation of evidence into practice. Furthermore, organizational change and adoption of new practices depend upon health care professionals recognizing the value of a change, particularly its benefits for patients. 69 This review has demonstrated a slow cultural shift toward recognition by medical and nursing staff of the evidence of effectiveness and safety of MT. 42 However, in an evolving environment, it is unsurprising that such recognition may be fragmented or less than universal.39,43,51 More research is needed to substantiate the emerging evidence relating to underlying mechanisms of action of, 72 and the benefits of massage, and to identify how to address knowledge gaps among health professionals and service managers.
Finally, there remains the need for rigorous cost-benefit analyses and testing of funding models.
Strengths and limitations
A review protocol was registered prior to the conduct of the review and is available at Open Science Framework: https://doi.org/10.17605/OSF.IO/C6Q7Y. Minimal amendments to the protocol were applied. The diversity of study designs included in the review contributed valuable contextual and experiential insights. In a research environment where complementary therapies are frequently investigated as a group, the singular focus on massage and MT is a strength of this review.
A primary limitation was the restriction of document selection to those in English. Given that both PC and massage are global phenomena, it is likely that studies in languages other than English have been undertaken and reports about them missed. Additional limitations were the underrepresentation of community-based PC services and that the wider applications of massage to informal and formal caregivers of palliative patients were not explored.
Conclusion
Massage has long provided comfort to people with life-limiting illness, and this review confirms that it continues to be recognized as having that capacity. However, the role of massage and MT in PC is evolving—driven by a shift toward person-centered, integrative care, a deepening understanding of the impacts of massage, growing clinical evidence, and increasing professionalization and specialization of MT. In addition, the review underscores the meaningful contribution to the holistic needs of patients that can be achieved when MT is fully integrated within specialist interdisciplinary PC teams. While barriers and challenges to integration remain, the review highlights that these can be overcome when the core values of PC to provide exemplary high-quality clinical and compassionate care align with leadership commitment and administrative support.
Footnotes
Acknowledgments
The author(s) wish to acknowledge the assistance of Bernadette Gargan, Senior Research Librarian, La Trobe University, Bundoora, Australia.
Research Ethics
As this study represents a scoping review, no formal ethics approval was required.
Authors’ Contributions
R.M.: Conceptualization (lead), writing—original draft (lead), analysis (lead), writing—review and editing (equal), visualization (lead). B.R.: Conceptualization (supporting), writing—review and editing (equal). H.K.: Conceptualization (supporting), analysis—supporting, writing—review and editing (equal).
Author Disclosure Statement
The author(s) have no conflicts of interest to declare.
Funding Information
This study was unfunded.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.