
Abstract
Background:
At least 42% of nursing home (NH) residents live with cognitive disability, commonly associated with neurocognitive disorders (e.g., dementia), defined as difficulty concentrating, learning new things, remembering, or making decisions. The population of individuals with cognitive disabilities who qualify for hospice (end-of-life [EOL] care that reduces symptoms and promotes quality of life) in NHs is increasing. However, little is known about hospice enrollment for this population. This information is essential to clarify disparities in hospice access and guide efforts to improve EOL care for this population.
Objective:
To systematically review available evidence on hospice enrollment among US NH residents with cognitive disabilities.
Methods:
This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. A comprehensive search of PubMed, CINHAL, Web of Science, and Google Scholar was conducted to identify studies. Peer-reviewed, English-language articles published before February 28, 2025, were included. The Joanna Briggs Institute Analytical Cross-Sectional Studies Appraisal Tool was used to assess study quality.
Results:
We screened 479 titles and abstracts and reviewed 36 full-text articles. Twelve studies met the inclusion criteria. In seven of the 12 studies, a substantial proportion of NH decedents with cognitive disabilities were not enrolled in hospice. Factors associated with increased likelihood of hospice enrollment at the time of death included female sex (n = 2), White race (n = 2), terminal diagnosis other than cognitive disability (n = 1), and increased prevalence of dementia in NH regardless of the individual’s dementia status (n = 1).
Discussion:
This review is the first to systematically examine hospice enrollment among NH residents with cognitive disabilities. Hospice enrollment varied across studies but was consistently lower for NH decedents with cognitive disabilities compared to those without. Future research should include the broader cognitive disability community to assess hospice enrollment and other EOL outcomes, clarify targets for intervention, and address barriers to care.
Introduction
Cognitive disabilities affect approximately 13.9% of adults in the United States. 1 These disabilities—defined as serious difficulty making decisions, learning new things, remembering, or concentrating—can result from a range of conditions, including Alzheimer’s disease and related dementias (ADRDs), traumatic brain injuries, intellectual/developmental disabilities, and strokes.1,2 With the exception of individuals with ADRDs, individuals with cognitive disabilities are underrepresented in end-of-life (EOL) and hospice research.1,3,4
Even among patients with ADRDs, their involvement in research is likely an underrepresentation due to under-detection and/or late diagnosis. 5 In 2022, the Centers for Medicare and Medicaid Services reported 11.1% of decedents in the United States had an official diagnosis of ADRDs, yet estimates suggest that the real percentage of Medicare decedents with ADRDs is 41%.3,6,7 This difference indicates that using official diagnoses of ADRDs in research, via diagnostic codes and electronic health records, may result in unintentionally excluding a large segment of the population of individuals with cognitive disabilities.5,8 The use of the term cognitive disability better captures the population of interest, and therefore improves research on EOL outcomes for a population susceptible to poor/sub-optimal EOL outcomes.4,9,10
Hospice is a covered benefit under Medicare and the Medicaid benefit in many states that provides specialized EOL care to individuals with an anticipated life expectancy of ≤6 months.11,12 Interdisciplinary teams that focus on symptom management, comfort, and quality of life deliver hospice care and services.11–13 These services have reduced unnecessary and burdensome care, improved quality of life for patients and families alike, and reduced health care spending.12,14,15
While hospice enrollment is recommended for all qualifying patients, 67% of all nursing home (NH) residents who die (i.e., 804,000 individuals in 2023) are not enrolled in hospice.12,16,17 It is not known how many of these residents have cognitive disabilities; however, conservative estimates suggest that at least 42% of NH residents in the United States have some form of cognitive disability. 18 Given that hospice is considered best practice for EOL care, because it minimizes unwanted treatments and improves quality of life near EOL, it is essential to understand barriers to enrollment and use of high-quality hospice care for this population.19–21
Given the high prevalence of residents with cognitive disabilities in NHs and the well-known benefits of hospice care,16–19 it is critical to understand the multilevel factors that influence access in this population. However, little is known about specific resident-level (e.g., diagnosis, race/ethnicity), facility-level (e.g., staffing, ownership), and community-level characteristics (e.g., regional poverty) impacting hospice utilization. This information is essential for clarifying disparities in hospice access and guiding efforts to improve EOL care. In this systematic review, we synthesized the evidence on hospice enrollment for individuals with cognitive disabilities in NHs and the different factors influencing this outcome.
Methods
We developed and registered an a priori protocol in PROSPERO (CRD42024593889) and followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. 22 We created a comprehensive search strategy in consultation with a research librarian (see Supplementary Data) and searched four databases (without limits) through February 28, 2025: the Cumulative Index of Nursing and Allied Health Literature (CINAHL), PubMed, Web of Science, and Google Scholar. Studies were eligible for inclusion if they were observational or interventional in design, conducted in the United States, were English language studies published in peer-reviewed journals, included adult (≥18 years) participants receiving care in NH settings, and examined hospice enrollment as an outcome. Eligible studies had to include individuals with cognitive disabilities, which we defined as having a diagnosis of ADRD, stroke, brain injuries, intellectual/developmental disability, or identification of cognitive disability through formal assessment (e.g., cognitive performance scale). Studies were excluded if they were: qualitative; conducted outside the United States; not published in peer-reviewed journals; focused on care settings other than NHs; not inclusive of individuals with cognitive disabilities, or did not assess hospice enrollment.
Article screening
All identified records were uploaded into Covidence 23 for duplicate removal and workflow management. Two reviewers independently screened all titles and abstracts, followed by full-text reviews of potentially eligible studies. Discrepancies were resolved through team discussion.
Critical appraisal of study quality
Study quality was assessed using the Joanna Briggs Institute (JBI) Analytical Cross-Sectional Studies Tool 24 (see Supplementary Data), an 8-item checklist evaluating participant selection, the validity of exposures and reliability of outcome measures, approach to addressing confounders, and appropriateness of statistical analysis. Each criterion was scored as “Yes” (1 point), “No” (0 points), “Unclear” (0 points), or “Not Applicable.”24,25 scores on the tool were summed, and overall quality was calculated as the proportion of “Yes” responses. 24 We established ≤50% as the cutoff for “high risk of bias.” Two reviewers independently assessed each study, the results were compared, and any differences were resolved through team discussion.
Data extraction
Data were extracted using a standardized form that was pilot tested prior to use. Extracted variables included: article citation; study aims and outcomes; NH care setting, defined population meeting review criteria for cognitive disability (e.g., ADRD) inclusion criteria (e.g., the definition of cognitive disability, NH care setting); exclusion criteria (e.g., hospice enrollment was not assessed, not meeting population or setting requirements); data source; sample size; data collection period; study location; statistical approach; study findings, including resident demographics (i.e., race, sex, age, primary hospice diagnoses, and comorbidities) and NH-level characteristics (e.g., geographic location). Two authors independently extracted data using the standardized form, and discrepancies were resolved through team discussion. Study data were synthesized using summary tables and grouped by participant diagnosis, sex, setting, and location to facilitate comparisons.
Results
The initial search yielded 479 records after removing duplicates. Following title and abstract screening, 36 full texts were assessed for eligibility, and 12 studies7,26–35 met all inclusion criteria (Fig. 1). A complete list of excluded studies with reasons for exclusion is provided (See Supplementary Data).
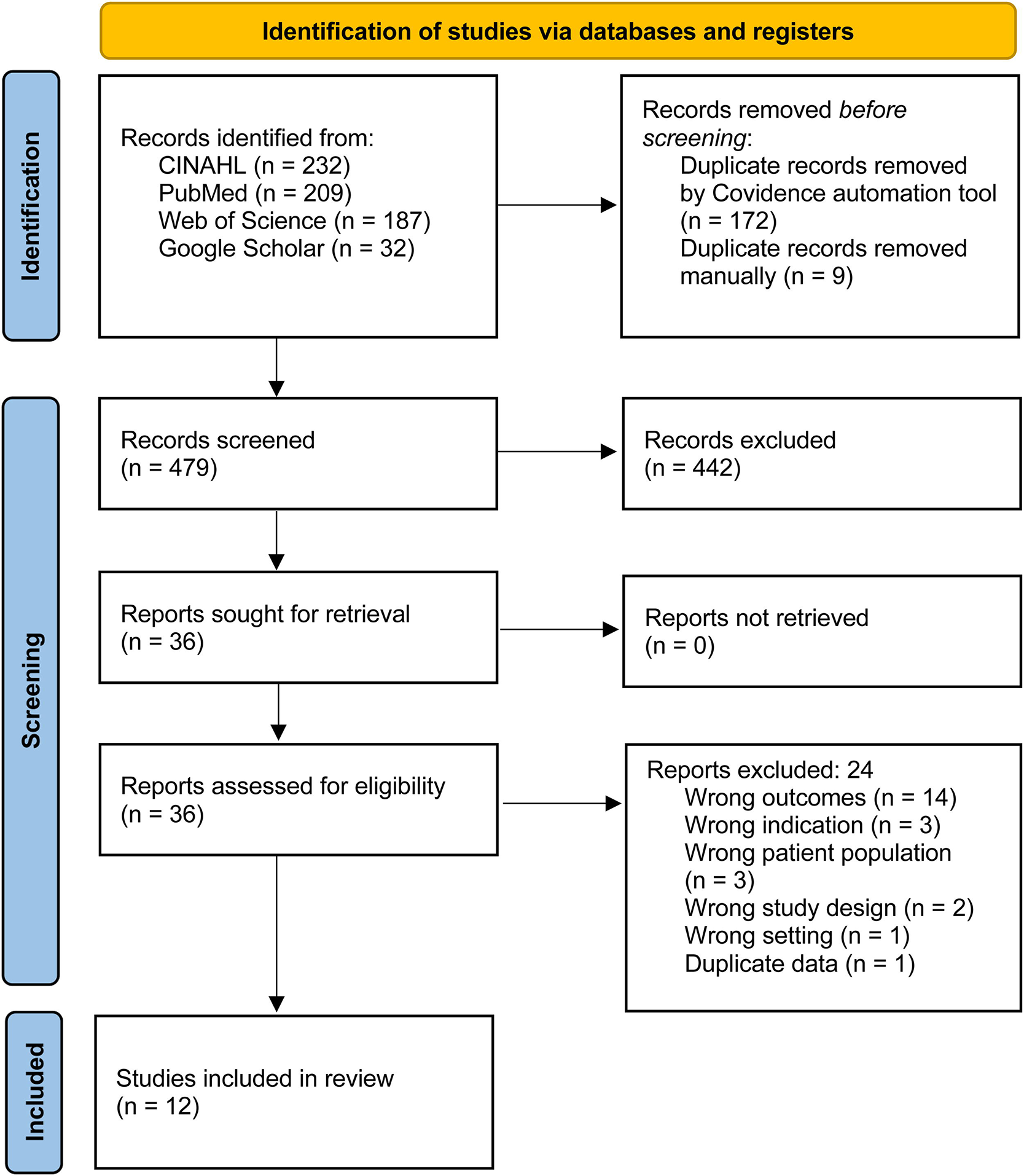
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 flow diagram for new systematic reviews, which included searches of databases and registers only.
Quality appraisal
All included studies met at least 75% of the JBI quality appraisal criteria as described above and were included in the qualitative synthesis (Table 1). Eleven of the 12 studies met 100% of the criteria.7,27–36 Four studies were descriptive in nature,26,27,31,35 and thus received a “Not Applicable” rating for the criterion related to strategies for confounding. One study was downgraded due to uncertainty around valid/reliable outcome measurement. 26
Joanna Briggs Institute Checklist
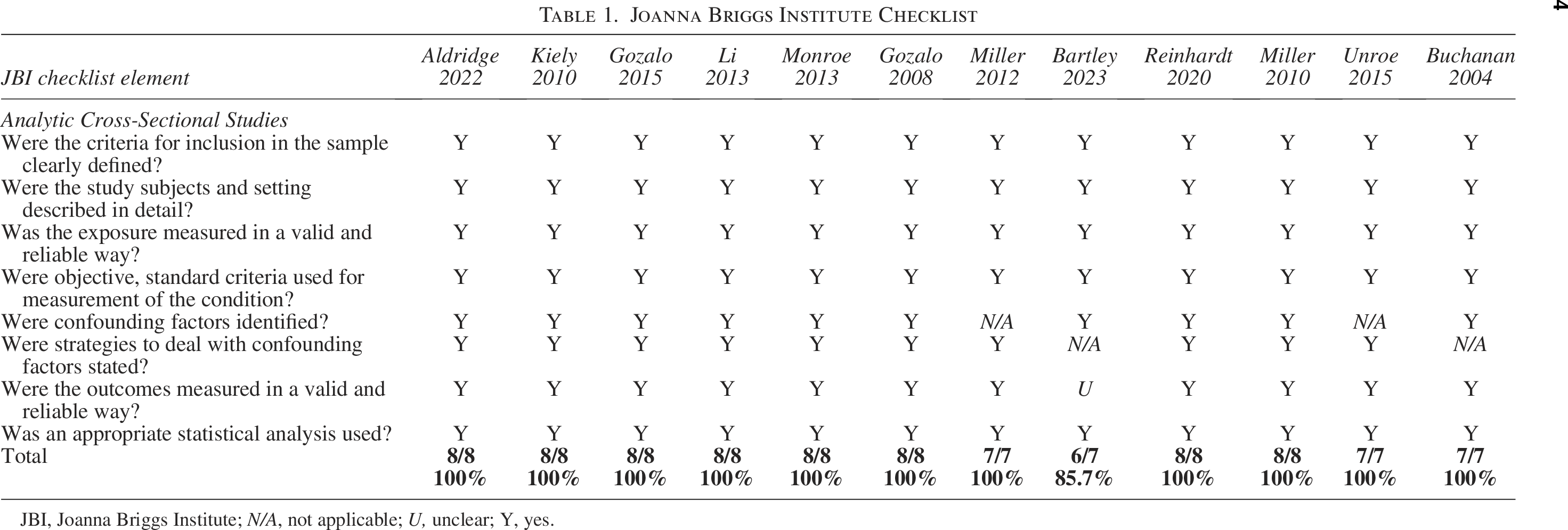
JBI, Joanna Briggs Institute; N/A, not applicable; U, unclear; Y, yes.
Study characteristics
Table 2 reports detailed study characteristics. Studies were published between 2004 27 and 2023 26 and analyzed data from 1998 29 to 2018. 26 Authors from six studies used national datasets (i.e., included NHs across all 50 states),7,27,28,30–32 and of these, the District of Columbia was included in two.31,32 Authors from other studies focused on specific geographic regions, including a single safety-net health care system in Indiana, 35 nine NHs within a 150 mile radius of Nashville, Tennessee, 33 22 NHs within a 60 mile radius of Boston, Massachusetts, 36 11 skilled nursing facilities in Rochester, Minnesota, 26 a single NH in New York State, 34 and an undisclosed number of NHs across the state of Florida. 29 Sample sizes ranged from 55 33 to 3,848,114 32 corresponding to the variation in geographic location (e.g., larger sample sizes for studies of national datasets).7,27,28,30–32
Study Characteristics for Included Studies
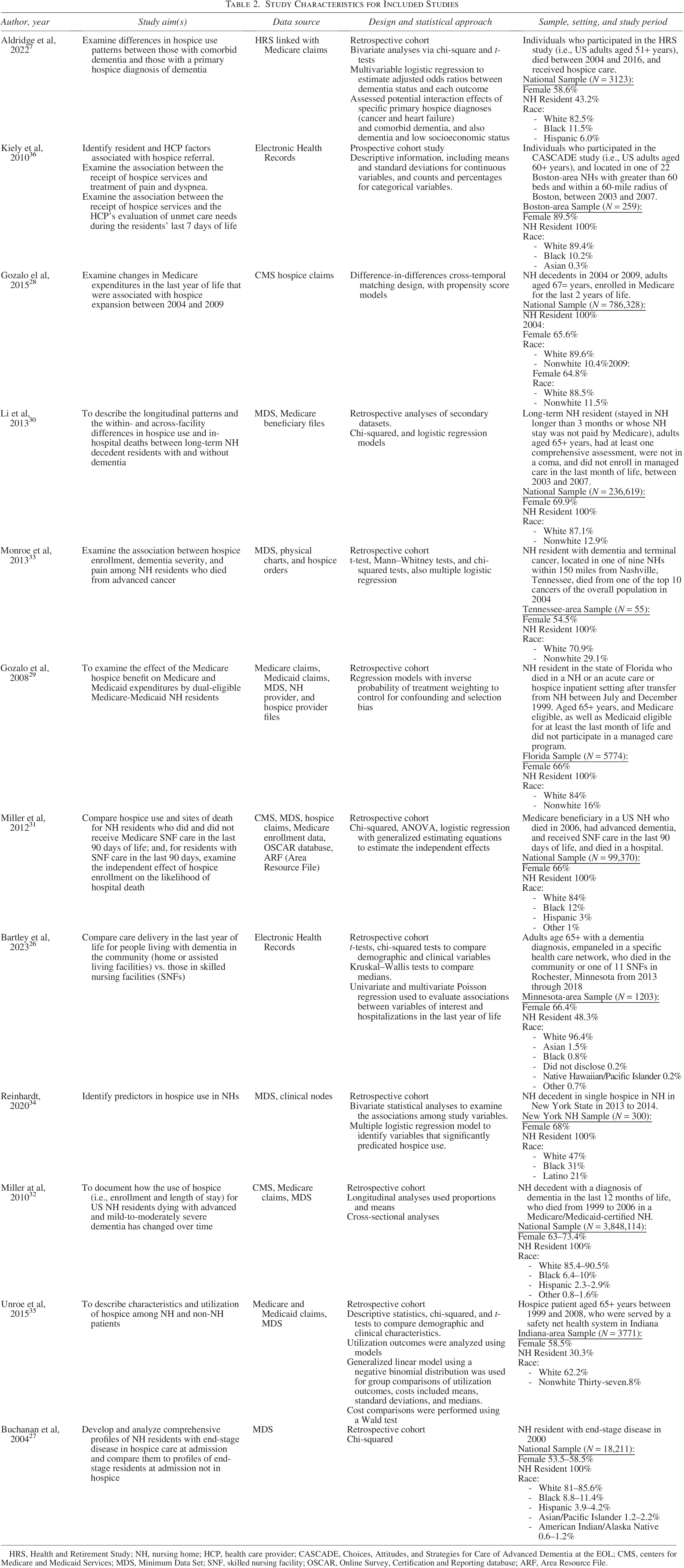
HRS, Health and Retirement Study; NH, nursing home; HCP, health care provider; CASCADE, Choices, Attitudes, and Strategies for Care of Advanced Dementia at the EOL; CMS, centers for Medicare and Medicaid Services; MDS, Minimum Data Set; SNF, skilled nursing facility; OSCAR, Online Survey, Certification and Reporting database; ARF, Area Resource File.
In nine studies, investigators reported the mean age of participants,7,26,28,30,33,34,36 which ranged from 71.8 27 to 87.5 years. 26 Investigators of all studies reported sex and race; in all studies, females outnumbered males, ranging from 54.5% 33 to 85.4%. 36 Reporting of race varied across studies (e.g., multiple racial groups, White vs. nonwhite). White decedents were the majority in all studies, ranging from 47% 34 to 97.7%. 26
With regards to diagnoses/conditions, in five studies, researchers focused on NH residents with dementia;7,26,31,32,36 in one study, researchers focused on NH residents with dementia and terminal cancer. 33 In the remaining six studies, researchers looked at decedents in general.27–30,34,35
Variables measurement
In four studies, investigators used cognitive performance scale scores to determine the presence of, and severity of, cognitive disabilities.27,28,32,33 Investigators of one study used the global deterioration scale scores to determine the presence of, and severity of, cognitive disabilities. 36 In one study, investigators used a clinically validated algorithm based on cognitive and functional assessment scores to determine the severity of cognitive disabilities. 7 In addition to these assessments, in all 12 studies, investigators used diagnoses via medical charts (i.e., ADRDs) to determine the presence of cognitive disabilities.
Investigators of five studies focused on hospice enrollment for decedents with dementia.7,26,31,32,36 In five studies, investigators looked at hospice enrollment for all decedents (i.e., those with and without dementia, as well as other diagnoses).28–30,34,35 In one study, investigators examined hospice enrollment for all decedents diagnosed with end-stage diseases, including dementia. 27 And in the final study, investigators examined hospice enrollment for individuals with cancer and dementia diagnoses. 33
Study findings
Hospice enrollment
Table 3 reports detailed study findings. In 11 studies, investigators reported the percentage of NH decedents with cognitive disabilities who were enrolled in hospice care;7,26–33,35,36 of those, researchers from seven found that fewer than half were enrolled in hospice at the time of death.7,29–33,36 Investigators from two studies concluded that only a minority of residents with severe cognitive disability received hospice care,31,36 and researchers from one study found that hospice-enrolled decedents were less likely to have severe cognitive disability. 33 One study 34 found a significant association between dementia diagnosis and hospice enrollment, but did not report a specific enrollment percentage. Researchers from all the included studies found that a significant percentage of NH decedents with cognitive disabilities were not enrolled in hospice at the time of their deaths.
Key Findings
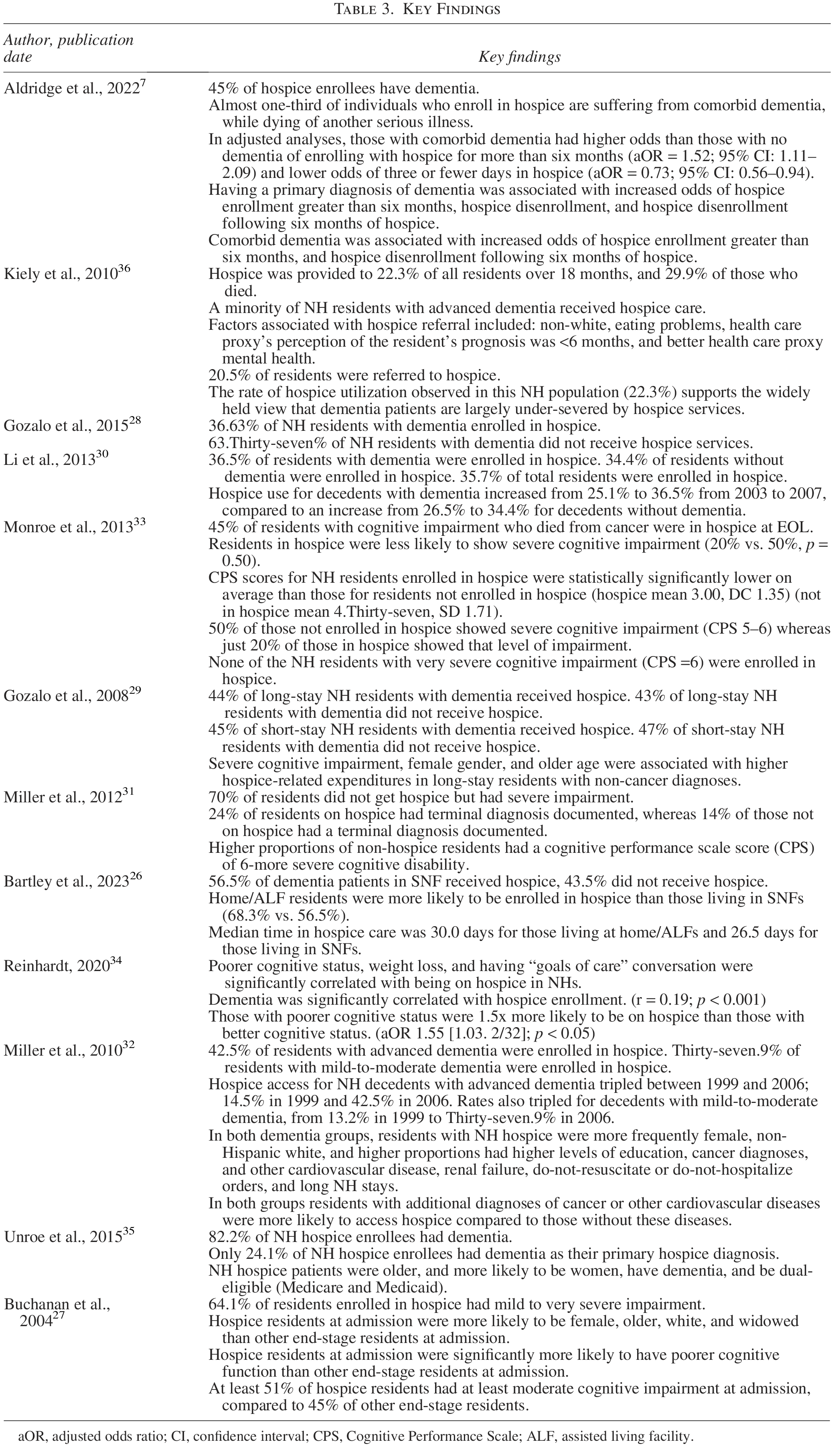
aOR, adjusted odds ratio; CI, confidence interval; CPS, Cognitive Performance Scale; ALF, assisted living facility.
Growth in hospice enrollment
Investigators from three studies examined changes in hospice enrollment over time among NH decedents with dementia.28,30,32 Gozalo et al. (2015) reported a 5.2% increase in hospice use from 2004 to 2009 for NH decedents with dementia, reporting a decline in enrollment for decedents without dementia. Li et al. (2013) also found an increase in hospice enrollment from 2003 to 2007 for NH decedents with dementia (11.4%), compared to those without dementia (7.9%). Miller, Lima, & Mitchell (2010) reported that hospice use tripled from 1999 to 2006 for residents with mild-to-moderate dementia.
Factors associated with hospice enrollment
Findings reported across studies focused mainly on patient-level factors associated with hospice enrollment. Investigators of two studies identified significant associations between hospice enrollment and specific demographic characteristics; in both, White race and female sex were positively associated with hospice use.27,32 Investigators of one study found that NH decedents with additional diagnoses of cancer or cardiovascular disease were more likely to enroll in hospice compared to those without these comorbidities. 32 Additionally, investigators in one study found that decedents enrolled in hospice were more likely to have a formal terminal diagnosis documented in their medical records than those who were not enrolled in hospice. 31 These individuals had “terminal” documented in their medical charts, rather than alternative options for hospice enrollment like “estimated less than 6 months life-expectancy.” Only one study team (Li et al., 2013) reported factors associated with hospice enrollment at the NH facility level (i.e., prevalence of dementia among residents; positive association with enrollment).
Discussion
To our knowledge, this is the first systematic review to examine hospice use among US NH decedents with cognitive disabilities. While this population extends beyond those with formally diagnosed ADRDs, we found no studies assessing hospice use among NH residents with other important cognitive disability subtypes (e.g., intellectual or developmental disabilities, and acquired brain injuries). Notably, none of the studies included in this review used the term cognitive disability. Given the heightened risk of poor EOL outcomes among this population,4,9 future research should aim to include a wider range of cognitive conditions to ensure more inclusive and representative findings.
We expanded upon prior research by synthesizing findings related to factors associated with hospice enrollment in NH settings. A few of the studies included in this review identified/reported the association of facility-level factors (e.g., size, ownership, and rurality) with hospice use, warranting further investigation in this area. The literature we synthesized was limited to NH residents with dementia and is thus limited in its generalizability across NH residents with other cognitive disabilities. However, our findings show that hospice enrollment was consistently lower for NH decedents with cognitive disabilities compared to those without, underscoring the critical need for exploration of the barriers and facilitators affecting access/utilization for this population.7,26–36
As of 2010, data show that only 6% of NH decedents were enrolled in hospice care, despite 24% being eligible. 37 While this statistic does not specify cognitive disability status, or the multiple factors that impede access, it highlights a wider gap between eligibility and enrollment observed nationally among NH decedents. Public awareness and perceptions of hospice have evolved since this time; by 2017, 70% of Americans had heard of hospice, and 85% of those endorsed a positive view. 38 Given that the studies in this review span from 2004 to 2023, it is possible that hospice enrollment patterns for individuals with cognitive disabilities have shifted over time, and this may be influenced by multiple factors (e.g., evolving NH resident demographics).
Researchers from six studies in this review used national datasets,7,27,28,30–32 while others focused on specific regions or health systems.29,33,34 Although geographic variation in hospice referral is well-documented, including disparities both within and across states, 39 none of the studies in this review specifically analyzed regional differences in hospice enrollment. Such variation may reflect differences in the availability of health care resources (i.e., distance to and concentration of health care facilities), NH practices and programs that impact hospice access, racial and ethnic composition, and socioeconomic status. 39 Importantly, none of the studies examined the impact of community-level factors, such as regional poverty. Understanding these and other sources of disparities is essential to improving equitable hospice access for NH residents with cognitive disabilities and should be the focus of future research.
Although all included studies focused on individuals with ADRDs, some researchers used broader cognitive assessments beyond diagnostic codes. Still, no studies specifically addressed important cognitive disability subtypes, such as intellectual/developmental disabilities or acquired brain injuries. While we sought to identify research that included patients with a variety of cognitive disabilities, this proved more difficult than anticipated. All data identified and included in this review focused on individuals with ADRDs. Given the heightened risk of poor EOL outcomes among this population, future research should aim to include a wider range of cognitive conditions to ensure more inclusive and representative findings.
No interventional studies were identified in this review. As the population continues to age and efforts to address health disparities advance, future research should prioritize developing and testing interventions that improve hospice enrollment among individuals with cognitive disabilities. This population already experiences significant disparities in health care access and quality across the care continuum,40–44 yet data on their use of hospice remain scarce. This review highlights the need for a deeper understanding of hospice care disparities affecting individuals with cognitive disabilities and the development of targeted strategies to address them.4,9,40
Additionally, hospice care delivered in other settings (i.e., hospitals, home, assisted living facilities, and group homes) should be examined, as many deaths occur outside of NHs, and many patients with ADRD receive EOL care in assisted living facilities. Furthermore, in the spirit of the principle, “nothing about us, without us,” 45 individuals affected by cognitive disabilities should be meaningfully engaged in the research process, not only as participants but also as stakeholders and collaborators.
Limitations and potential biases
The definition of cognitive disability used in this review was developed by the authors and, while intended to be comprehensive, may have excluded studies of this population using varied definitions. This review was limited to English language, peer-reviewed studies conducted in US NHs, which may have excluded important research from other settings (e.g., those who died in the hospital following hospice care in NHs, participants from other countries). Additionally, all included studies focused on individuals with ADRDs, limiting the generalizability of the findings to the broader population with cognitive disabilities.
Conclusions
Disparities in EOL care exist for individuals with cognitive disabilities, who are less likely to receive hospice services compared to those without such disabilities. This review found that, among US NH residents, individuals with cognitive disabilities are less likely to be enrolled in hospice than their peers without cognitive disabilities. As this population ages and continues to grow, it is vital to understand and address the underlying mechanisms of reduced hospice enrollment and identify novel solutions to address it. Improving hospice access can ensure the delivery of quality EOL care, reduce unnecessary health care utilization and costs, and alleviate distress for both patients and family caregivers.
This review examines hospice enrollment of people with cognitive disabilities. Seven out of 12 articles identified that a significant number of NH residents with cognitive disabilities were not enrolled in hospice at the time of death. Results show that hospice enrollment varied among NH residents with cognitive disabilities, and that race/ethnicity, sex, and facility-level characteristics may influence access to hospice care.
Footnotes
Author Disclosure Statement
The authors listed above have No Interest to disclose.
Funding Information
V.M.W. is supported by the Columbia University School of Nursing Systems Science and Comparative and Cost-Effectiveness Research Training for Nurse Scientists program (S2CER2; T32 NR014205).
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.