
Abstract
Background:
Bone metastases cause significant symptom burden, yet patterns of palliative care (PC) utilization in this population remain poorly characterized.
Objectives:
To evaluate trends in PC use, compare inpatient palliative care (IPPC) and outpatient palliative care (OPPC) utilization, identify predictors of PC engagement, and assess the impact on readmissions.
Methods:
Using the PearlDiver database (2011–2021), patients with bone metastases were identified. PC encounters were classified as IPPC or OPPC. Trends were assessed with linear regression; predictors and outcomes were evaluated using multivariate logistic regression.
Results:
Of 471,713 patients, 17.2% received PC. Overall PC use did not increase significantly from 2011 to 2021 (p = 0.14), though OPPC rose from 0.7% to 2.6% (R2 = 0.87). Predictors of PC use included younger age (mean age 64 vs. 66 years, p < 0.001), female gender, higher comorbidity burden, Medicaid insurance, and region (p < 0.01 for all). Receipt of OPPC within six months of hospice was associated with 77% lower odds of readmission (Odds Ratio (OR): 0.23, 95% Confidence Interval (CI): 0.17–0.30, p < 0.001).
Conclusion:
PC utilization remains low in this population. OPPC use has modestly increased and is associated with reduced readmissions prior to hospice referral. Expanding OPPC may reduce hospitalizations and improve care quality.
Key Message
This study examines PC utilization among patients with bone metastases. It finds that overall PC use has modestly increased. Outpatient PC is associated with lower hospital readmission rates in the months preceding hospice. Enhancing early PC education may improve patient outcomes.
Introduction
Bone metastases affect up to 400,000 people annually in the U.S. and are associated with high morbidity and mortality.1–6 Patients often experience severe symptoms, including fractures, pain, mobility issues, and psychological distress.4–8 Given the complexity of these symptoms, comprehensive care, including advanced care planning, is vital.
Palliative care (PC) is uniquely positioned to address these challenges, improving quality of life and reducing distress.9,10 Early integration of PC has been linked to better symptom management and fewer hospital admissions.11–13 Reflecting this evidence, national guidelines—including those from the National Comprehensive Cancer Network (NCCN) and the American Society of Clinical Oncology—recommend early PC involvement for all patients with advanced cancer.14,15 Notwithstanding these guidelines, PC remains underutilized, particularly among underinsured and minority populations.16–20
Despite the substantial symptom burden associated with bone metastases and the proven benefits of PC, patterns of PC utilization in this population remain poorly characterized. This study aims to describe PC utilization among patients with bone metastases, compare inpatient palliative care (IPPC) versus outpatient palliative care (OPPC) usage, identify sociodemographic factors influencing utilization, and assess the impact on readmission rates.
Methods
A retrospective analysis was performed using the PearlDiver Patient Record Database (www.pearldiver.com; PearlDiver, Inc., Warsaw, IN), which includes de-identified billing records from various payer types (Medicare, Medicaid, commercial insurance, and self-pay).
Data collection
Patients diagnosed with bone metastases between 2011 and 2021 were identified using International Classification of Diseases (ICD)-9 and ICD-10 codes (Supplementary Appendix S1). Those without active records within a year of diagnosis were excluded. Extracted demographic and clinical data included age, gender, mean family income, geographic region, insurance status, Charlson Comorbidity Index (CCI)—a validated measure of comorbidity burden that predicts 10-year mortality risk based on weighted comorbid conditions—and hospital length of stay.
PC services were classified as IPPC, OPPC, and “other.” Hospice transitions were also identified. Readmission rates between patients receiving IPPC and OPPC within six months of hospice transition were compared. Only patients with a coded transition to hospice were included in this analysis; individuals who died prior to hospice enrollment or who died during the same admission as their PC consultation without subsequent hospice documentation were excluded. This approach was selected to focus the comparison on patients at a similar stage of illness, just prior to the transition to end-of-life care.
Statistical analysis
Patient demographics and clinical characteristics were summarized using counts (percentages) for categorical variables and means (standard deviations) for continuous variables. Chi-squared tests were used for categorical variables and independent samples t-tests for continuous variables. Trends in PC utilization, as well as differences in IPPC and OPPC usage over time, were analyzed using linear regression. Univariate and multivariable binomial logistic regression models were used to assess associations between demographic and clinical variables and the likelihood of utilizing PC. Statistical significance was set at p < 0.05. All analyses were performed using R Studio (version 4.2.2).
Results
A total of 471,713 patients with bone metastases were identified during the study period. Of these 471,713 patients, 81,280 (17.2%) received PC.
Patient demographics
Patients utilizing PC were slightly younger than those who did not (mean age 64 vs. 66 years, p < 0.001). A higher proportion of females (17.9%) accessed PC compared to males (16.6%, p < 0.001). PC users also had a higher mean family income ($79,778.8 ± 21,677.7 vs. $78,432.8 ± 21,671.6, p < 0.001) and longer average length of hospital stay (8.2 ± 8.3 days vs. 7.8 ± 8.6 days, p < 0.001). PC utilization varied by insurance status (p < 0.001). Of those who received PC, 24.3% were covered by Medicare, while 30.0% of patients not receiving PC had Medicare coverage. Medicaid was more common among PC users (7.0%) compared to non-users (4.7%). Private insurance coverage was higher among PC users (62.1%) than non-users (58.6%), indicating potential better access to PC for those with private insurance or Medicaid (Table 1).
Baseline Demographic Characteristics Between Bone Metastases Patients Utilizing PC and Those Not Utilizing PC
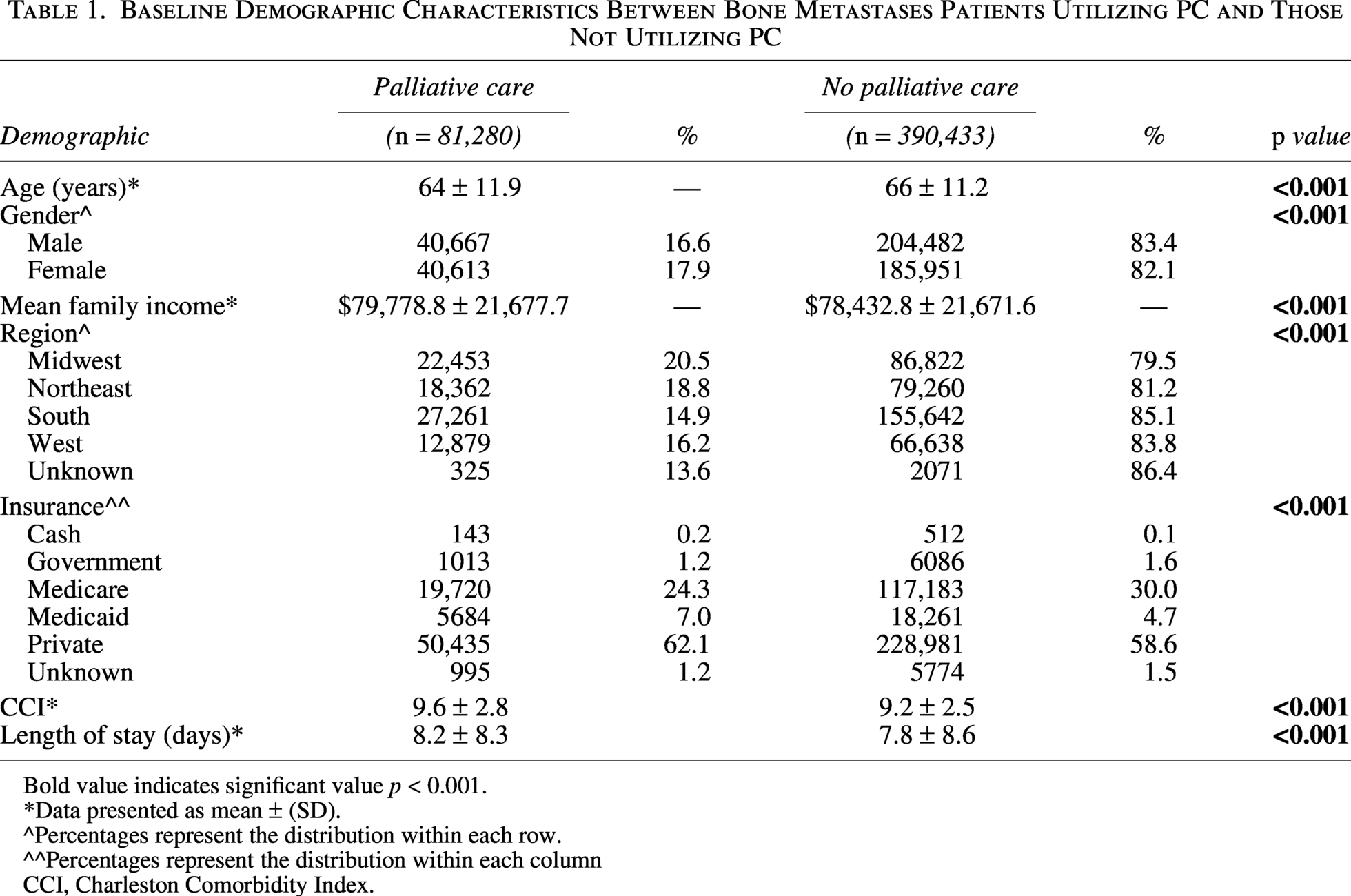
Bold value indicates significant value p < 0.001.
*Data presented as mean ± (SD).
^Percentages represent the distribution within each row.
^^Percentages represent the distribution within each column
CCI, Charleston Comorbidity Index.
Predictive factors associated with palliative care utilization
Multivariable logistic regression revealed that female gender (OR: 1.10, 95% CI: 1.04–1.16, p = 0.001), younger age (OR: 0.98, 95% CI: 0.98–0.99, p < 0.001), higher CCI scores (OR: 1.05, 95% CI: 1.04–1.06, p < 0.001), and Medicaid insurance (OR: 1.16, 95% CI: 1.04–1.29, p = 0.009) were associated with increased odds of PC utilization. Regional differences were also noted, with patients in the Midwest showing the highest odds of PC use, while the South had 36% lower odds (OR: 0.64, 95% CI: 0.60–0.69, p < 0.001) (Table 2).
Predictive Factors for Palliative Care
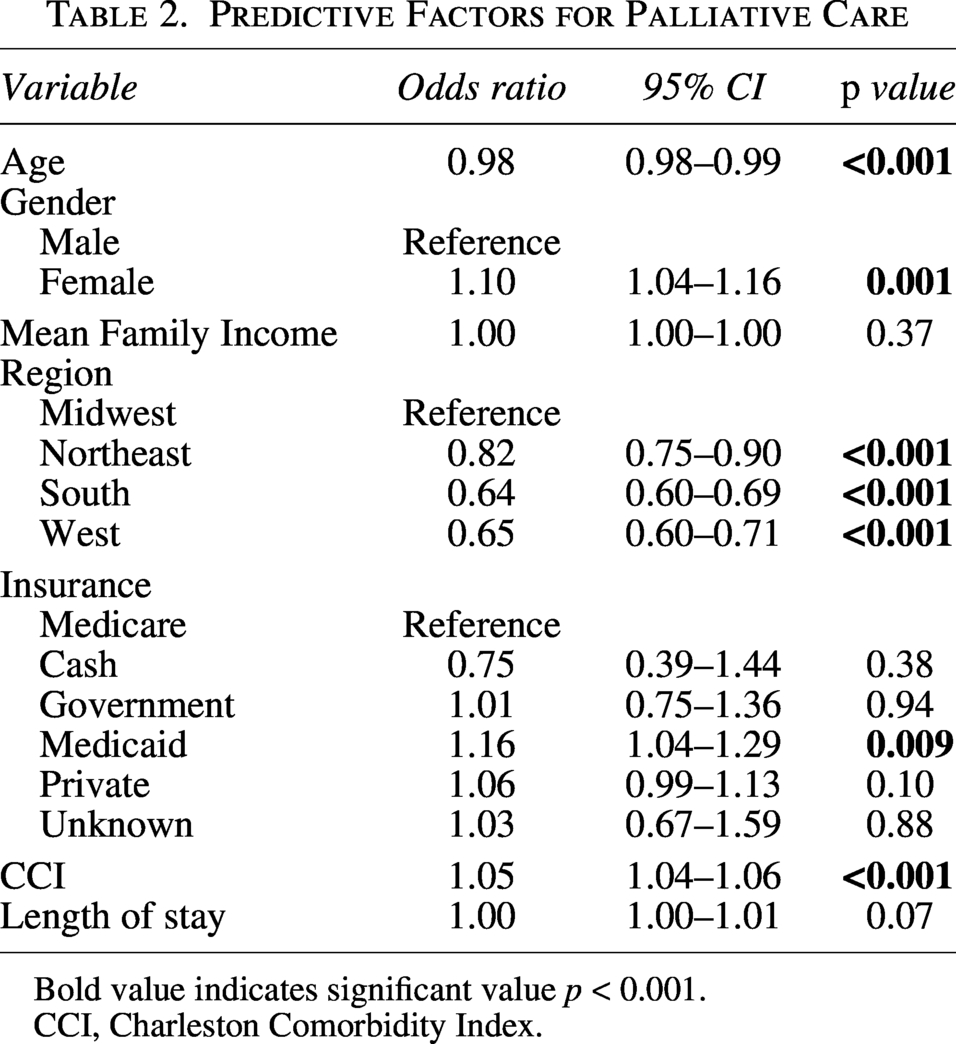
Bold value indicates significant value p < 0.001.
CCI, Charleston Comorbidity Index.
Inpatient versus outpatient palliative care
Patients utilizing OPPC were younger (62 vs. 63 years, p < 0.001) and had higher incomes compared to IPPC users (mean income $81,460.9 ± $22,557.3 vs. $79,067.5 ± $21,298.2, p < 0.001). Females had a higher utilization rate of OPPC (17.8%) compared to males (16.1%, p < 0.001). Insurance representation also varied between OPPC and IPPC groups (p = 0.02). Medicare and Medicaid utilization were similar across groups, while a slightly higher proportion of OPPC patients had private insurance compared to IPPC patients (64.7% vs. 63.2%). OPPC users also had lower CCI scores (9.4 ± 2.6 vs. 9.8 ± 2.8 for IPPC, p < 0.001) (Table 3).
Baseline Demographic Characteristics Between Patients Utilizing OPPC and IPPC
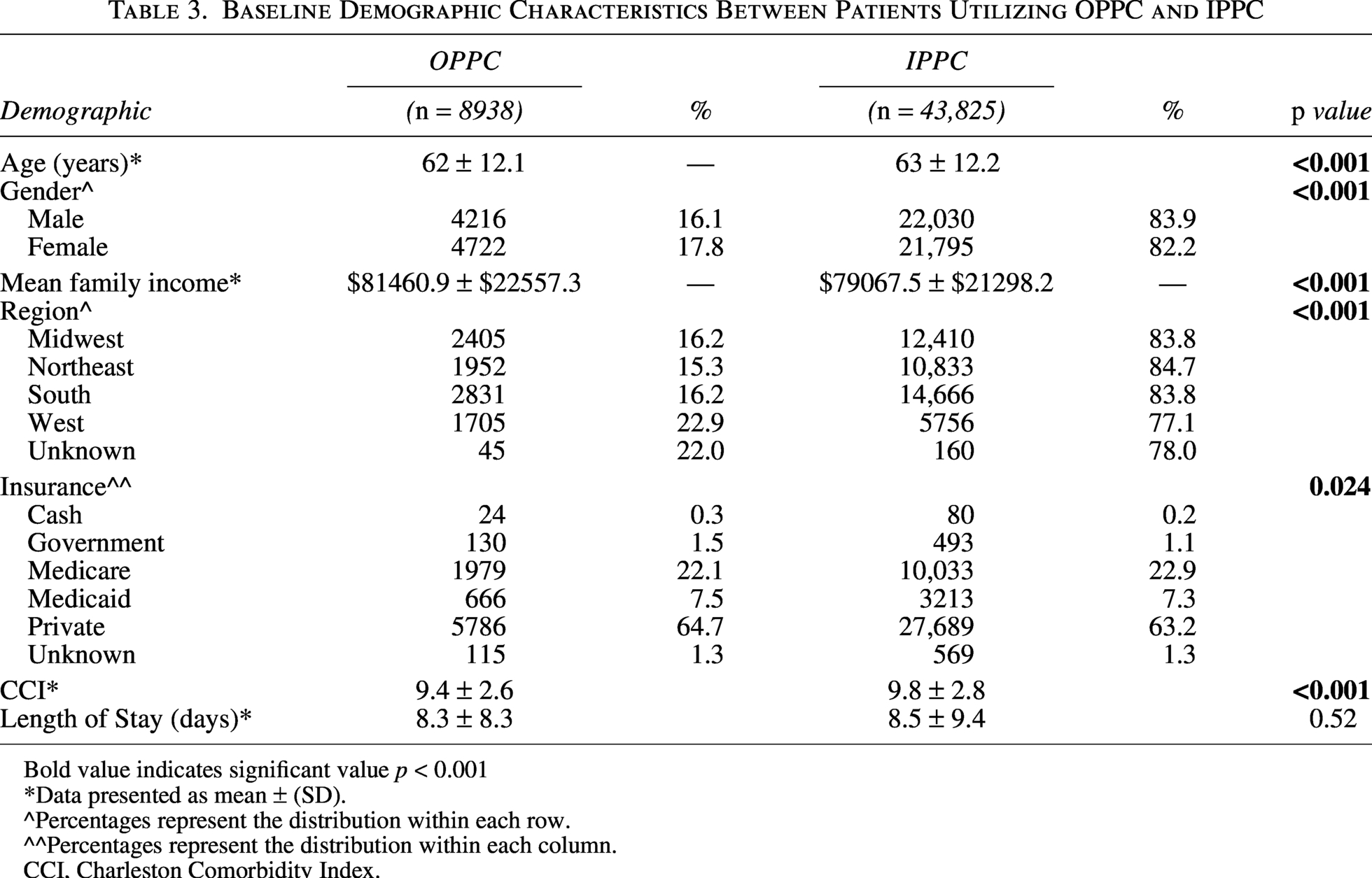
Bold value indicates significant value p < 0.001
*Data presented as mean ± (SD).
^Percentages represent the distribution within each row.
^^Percentages represent the distribution within each column.
CCI, Charleston Comorbidity Index.
Trends in palliative care utilization over time
No significant increase in overall PC utilization was observed over the study period (p = 0.14) (Fig. 1). 14 However, over the study period, the proportion of patients receiving OPPC steadily increased, rising from 0.7% in 2011 to 2.6% in 2021 (p < 0.001, R2 = 0.89). In contrast, IPPC utilization did not change significantly over the study period (p = 0.65) (Fig. 2A).
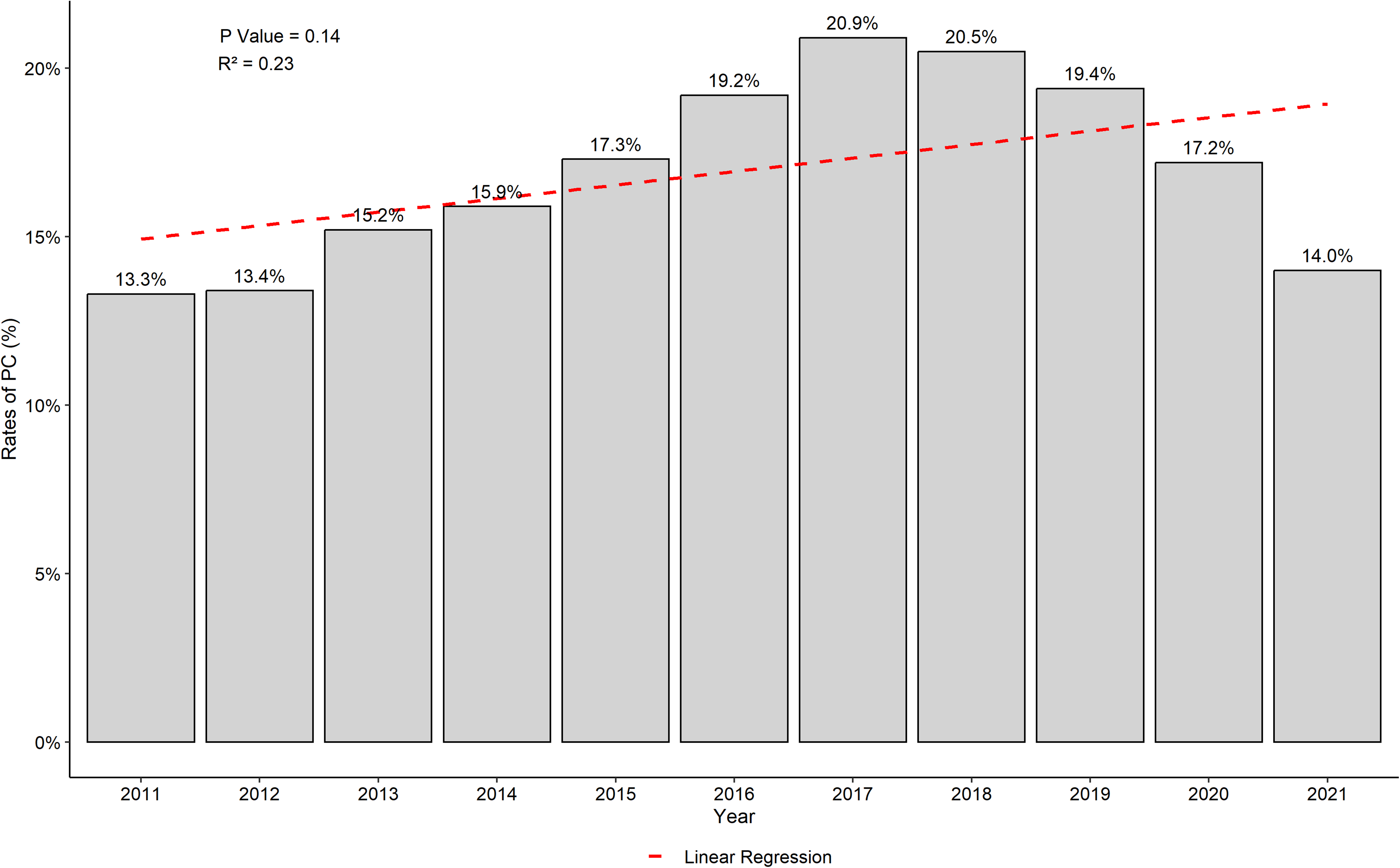
Rates of palliative care utilization by year in patients with bone metastases, 2011–2021.
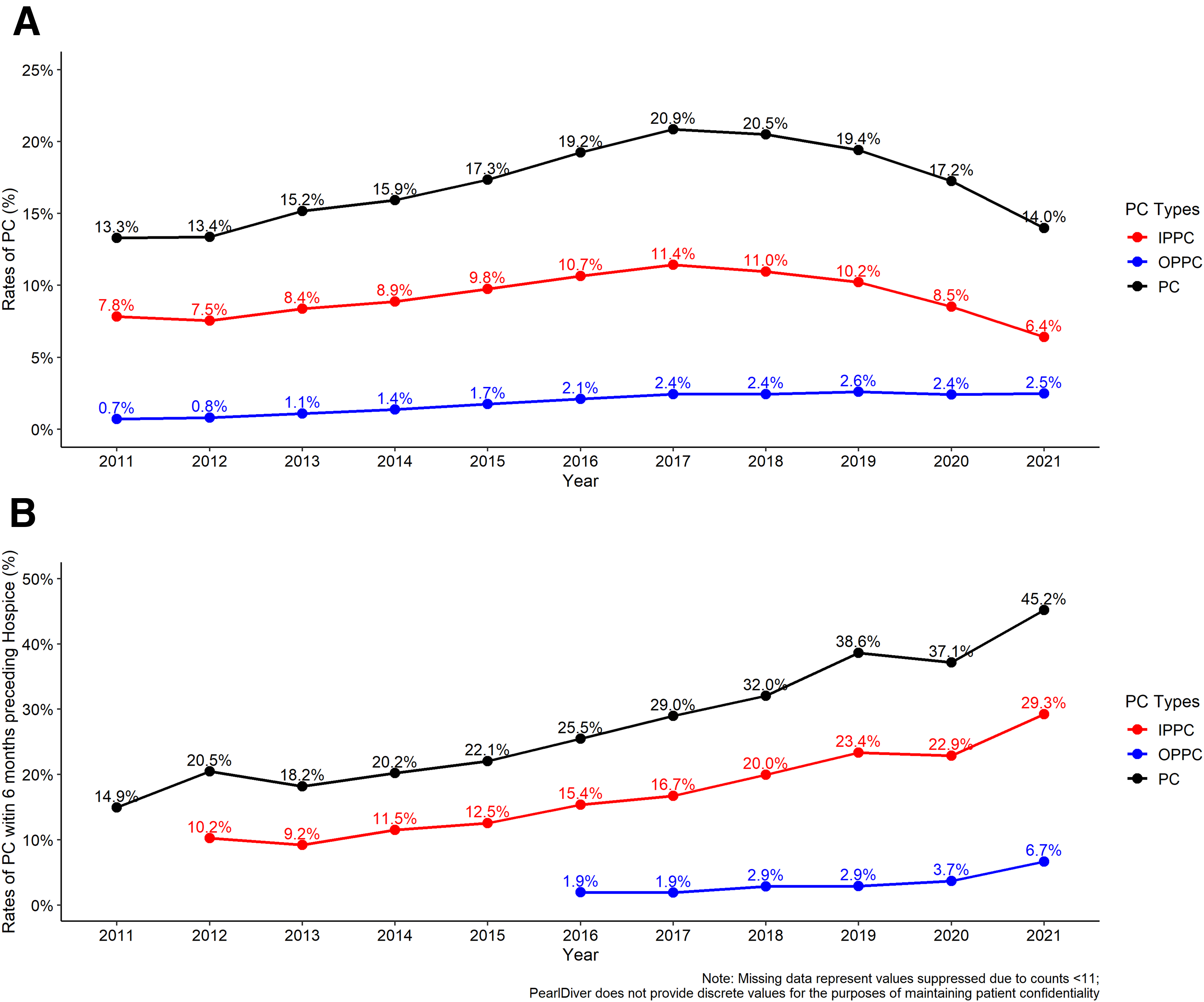
Within six months of hospice transition, there was an increasing trend in PC utilization (β = 2.82, 95% CI: 2.26–3.38; p < 0.001). Rates of both IPPC and OPPC similarly increased over this time period (β = 2.12, 95% CI: 1.70–2.55; p < 0.001 and β = 0.83, 95% CI: 0.20–1.46; p = 0.02, respectively) (Fig. 2B).
Palliative care utilization and readmission rates
Patients who received OPPC within six months prior to hospice transition had significantly lower hospital readmission rates (31.7%) compared to those receiving IPPC (66.8%, p < 0.001). OPPC was associated with a 77% reduction in the odds of readmission (OR: 0.23, 95% CI: 0.17–0.30, p < 0.001).
Discussion
To the authors’ knowledge, this study is the first study to characterize national trends in PC utilization among patients with bone metastases. Despite national guidelines from the NCCN recommending early PC integration for all patients with advanced cancer, 14 this study found that overall PC use in this population remains low and has not significantly increased over the past decade. OPPC use has modestly increased, rising from 0.7% in 2011 to 2.6% in 2021. Nevertheless, OPPC still represents a small fraction of care. Notably, OPPC was associated with lower hospital readmission rates in the six months prior to hospice enrollment, highlighting its potential to improve outcomes near the end of life.
These findings are consistent with prior research demonstrating similarly low PC uptake, particularly in earlier disease stages.21–23 Multiple barriers likely contribute, including the persistent misconception that PC is appropriate only at the end of life, limited provider awareness, or stigma among patients who do not feel they are in a place to confront end of life or hospice care. Further contributing to the complexity of PC referrals in this population are systemic and structural barriers, including challenges with inconsistent insurance reimbursement and inequitable access across health care systems. 24 The lack of meaningful growth in PC utilization over the past decade is particularly striking given mounting evidence of its benefits in symptom management, quality of life, and health care cost reduction.13,25–27 Moreover, patients with bone metastases (particularly those with spinal involvement) often experience high levels of psychological distress, further underscoring the need for timely, integrated supportive care throughout the disease course.7,8 Addressing these gaps will require focused efforts to improve both provider and patient education, normalize early PC referral, and embed PC specialists within clinical care teams. Clear institutional referral criteria may also support earlier and more consistent integration.
Our finding that OPPC is associated with reduced readmissions near the end of life underscores its broader role in contributing to care in patients with advanced illness. By facilitating proactive symptom management, psychosocial support, and earlier goals-of-care discussions, OPPC may help prevent avoidable hospitalizations while ensuring that care aligns with patient preferences.28–31 Prior studies have similarly shown that OPPC is linked to shorter hospital stays and longer hospice durations among oncology patients, reinforcing its role in facilitating timely and effective advance care planning. Taken together, these findings support efforts to expand OPPC access—not only to reduce health care utilization, but also to promote more coordinated, patient-centered care across the trajectory of serious illness. Additional studies, including those with patient- and caregiver-reported outcomes, should be conducted to further identify the exact mechanism through which OPCC reduces unwanted health care utilization.
This study also sheds light on sociodemographic trends in PC utilization, offering additional context to referral patterns. Although females were more likely to use PC services—consistent with prior research32,33—the gender differences were not clinically meaningful. Similarly, younger patients and those with higher income showed statistically significant, but clinically modest, differences in PC use. Regional disparities were more pronounced, with higher utilization in the Midwest compared to the South, likely reflecting differences in health care infrastructure. Insurance status also played a key role, as patients with private insurance and Medicaid were more likely to receive PC services. The observed regional and insurance trends may be linked to Medicaid expansion, as states that expanded Medicaid have demonstrated increased rates of PC utilization. 34 Recognizing and addressing these disparities is critical for ensuring equitable access.
Future directions
Future research should explore barriers to early PC referrals, including provider attitudes and patient awareness. Studies examining telemedicine’s impact on PC access, particularly in underserved areas, could provide valuable insights. Additionally, examining how socioeconomic factors and regional disparities influence PC utilization will help in developing targeted interventions.
Limitations
This study is limited by the use of administrative data, which does not capture detailed clinical information such as symptom burden or disease progression. The PearlDiver database lacks data on race and ethnicity, restricting our ability to examine potential disparities in PC access across these important demographic factors. Additionally, income was approximated using zip code-level data, which may not accurately reflect individual socioeconomic status. The reliance on ICD codes may also introduce inaccuracies in the form of misclassification bias, as potential errors in billing codes may misrepresent PC utilization. Moreover, survivorship bias is a challenge in many oncologic studies and is present here, especially with regard to those who have lived long enough to experience hospital readmission or transition to hospice care. This bias may influence our findings in the group of patients receiving OPCC.
Conclusion
This study highlights the underutilization of PC among patients with bone metastases, despite its known benefits. PC, especially OPPC, may reduce readmissions, highlighting the need for better utilization. Addressing barriers to early PC referral through provider education and improving access to services could enhance patient care and reduce health care costs.
Footnotes
Author Disclosure Statement
The authors have no disclosures relevant to the current work, nor any true/perceived conflicts of interest.
Funding Information
No funding was received for this article.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.