
Abstract
Patients with cancer have a high rate of comorbid psychiatric disorders. While the exact prevalence of comorbid bipolar I disorder and cancer is unknown, given the worse health outcomes associated with siloed specialist care, increased knowledge of the co-management of patients with cancer and bipolar I disorder is needed in palliative care. This case highlights a need for awareness regarding the specific combination of olanzapine and samidorphan (Lybalvi), approved in 2021 for the management of bipolar I disorder. Samidorphan, an opioid antagonist, mitigates the metabolic side effects of olanzapine. Notably, patients with comorbid bipolar I disorder and cancer often have both significant anorexia and pain, making samidorphan less desirable, as, in addition to mitigating metabolic side effects, it can limit the efficacy of analgesia from opioids. A recommendation of transitioning to olanzapine only is discussed.
Introduction
Patients with cancer have a high rate of comorbid psychiatric disorders 1 that palliative care providers are often challenged to co-manage. It is estimated that approximately one-third of patients living with cancer have an underlying mood disorder.1B2 -4 This association is bidirectional in that both patients with cancer are at increased risk of developing psychiatric disorders,2,3,5-7 and patients with preexisting psychiatric disorders, such as bipolar I disorder, are at increased risk of developing certain types of cancer.8-10 As a result, it is estimated that fewer than half of cancer patients living with psychiatric comorbidities receive appropriate care.4,11,12 While the exact prevalence of comorbid bipolar I disorder and cancer is unknown, given the high prevalence of comorbid physical and mental illness and worse health outcomes associated with siloed care, 13 increased knowledge of the co-management of patients with cancer and bipolar I disorder is needed in palliative care.
Bipolar I disorder is a primary psychiatric mood disorder characterized by episode(s) of mania and, frequently, depression. 14 The management of bipolar I disorder typically involves the use of a second-generation antipsychotic, such as olanzapine, for antipsychotic and mood-stabilizing effects. 15 Olanzapine is approved in the United States for the treatment of adults with schizophrenia or bipolar I disorder and has known metabolic side effects, like weight gain and metabolic syndrome, that have traditionally limited its clinical use in psychiatric patients. However, in oncology settings, olanzapine is usually prescribed at lower doses than are typically used for psychiatric patients, to successfully stimulate desired weight gain and address cancer-related and chemotherapy-associated nausea.16B17 -19
The specific combination of olanzapine and samidorphan (Lybalvi) was approved in the United States in 2021 to provide both the well-known antipsychotic efficacy of olanzapine for psychiatric patients while mitigating weight gain from olanzapine with the addition of samidorphan. 20 Samidorphan is an analog of naltrexone that effectively acts as a mu opioid receptor antagonist. Blockade of the mu opioid receptor leads to downstream reduction in hepatic gluconeogenesis and increased insulin sensitivity, regulating glucose and lipid metabolism typically affected by olanzapine. Furthermore, it is thought to target the endogenous opioid system that affects metabolism, thereby reducing cravings for high-calorie foods and attenuating the weight gain typically induced by olanzapine. 21 While samidorphan does not possess properties for the treatment of psychiatric conditions alone, research has highlighted that the addition of samidorphan to olanzapine, compared to olanzapine alone, has been associated with significantly less weight gain in patients with serious mental illness.22,23 However, in patients with cancer, who often have significant anorexia and pain, it is less desirable to mitigate the metabolic side effect of olanzapine with an opioid antagonist that may also contribute to the ineffectiveness of pain-relieving opioid medications.
Here, we present the case of a man with a longstanding diagnosis of bipolar I disorder, pharmacologically managed with olanzapine-samidorphan (Lybalvi), who was diagnosed with metastatic colorectal cancer. Over time, his cancer progressed, and he became increasingly cachectic and developed worsening cancer-related pain. Outpatient supportive oncology/palliative care was consulted for management of symptoms related to cancer.
Case Description
Oncologic history
The patient is a 52-year-old male with asthma and bipolar I disorder, diagnosed with colorectal cancer in 2021 Fig. 1. He underwent a right hemicolectomy at the time of diagnosis, and pathology revealed colonic adenocarcinoma, mucinous type. The following year, he presented with diffuse peritoneal carcinomatosis and was treated with first-line treatment. Over years, his disease progressed, and he became increasingly cachectic. On evaluation in 2024, the extent of his disease precluded further resection. He resumed systemic therapy, now second and third line, and at the time of his presentation to the supportive oncology clinic, imaging showed stable peritoneal carcinomatosis and no intracranial metastasis.
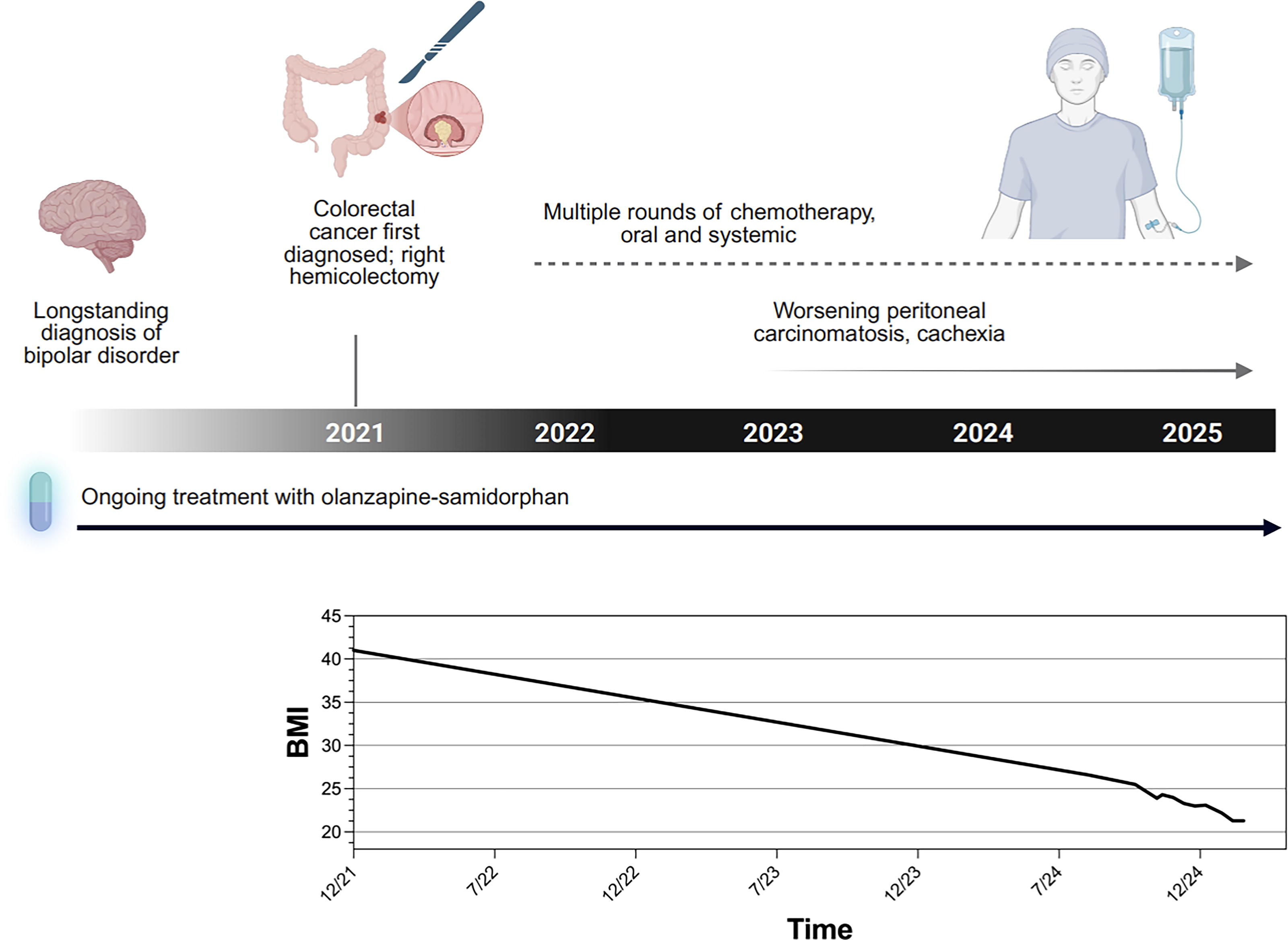
Graphical representation of patient history. The patient was treated for bipolar I disorder by a community provider, who recommended olanzapine-samidorphan as opposed to olanzapine alone in the context of obesity. The patient was later diagnosed with colorectal cancer and, over years, progressed to cachexia. Palliative care recommended transitioning to olanzapine to support appetite.
Psychiatric history
The patient established psychiatric care through a community provider, separate from the institution coordinating his oncologic and palliative care. He has a long-standing diagnosis of depression, which eventually declared itself a component of underlying bipolar I disorder. His medication regimen consistently included an antidepressant, and he had also been trialed on several mood stabilizers and antipsychotics. Years prior, he gained a substantial amount of weight while taking olanzapine. He was relieved to switch to olanzapine-samidorphan (Lybalvi), to which he attributes a weight loss of approximately 100 pounds. At the time of presentation to supportive oncology, his psychiatric medication regimen consisted of the mood stabilizer divalproex sodium (Depakote), the antidepressant escitalopram (Lexapro), and the antipsychotic olanzapine-samidorphan (Lybalvi). Per patient, his oncology and mental health care have proceeded in parallel, with no changes to his psychiatric medications as he underwent cancer treatment.
Initial presentation to supportive oncology
The patient presented to the Supportive Oncology clinic in 2025 alert and oriented, mildly dysphoric in mood, and grossly cachectic with bitemporal wasting. He had a large, palpable, tender mass in his left upper quadrant. Chart review revealed he weighed 175 lbs (79 kg) in 8/2024, decreased to a nadir of 140 lbs (64 kg) in 2/2025, and 143 lbs at time of presentation. His comprehensive metabolic panel was unremarkable except for low total protein, at 5.7 g/dL (nl = 6.7–8.6 g/dL), consistent with malnutrition. The patient endorsed anorexia, describing that his tumor negatively impacted his satiety. He had no complaints of nausea, vomiting, or diarrhea but endorsed pain with eating. He reported meeting with a dietician who recommended protein and nutrition supplements, which he only tolerated temporarily. Notably, olanzapine precluded the use of a second dopaminergic agent such as metoclopramide as a promotility agent for early satiety given the risk of extrapyramidal symptoms. 24 Furthermore, though opioid antagonists are frequently simultaneously administered with opioid agonists to mitigate opioid-related side effects,25B26 -28 reduce long-term abuse potential in medication-assisted treatment (MAT) for opioid use disorder (OUD), 29 and for simultaneous treatment of pain in patients on MAT for OUD,30-32 the specific manufacturer warning against using olanzapine-samidorphan (Lybalvi) together with opioids, partly due to the lack of efficacy of opioids, limited traditional analgesic options for this patient.
Recommendations
Attempts were made to reach out to the patient’s community psychiatrist for collaboration. However, the patient strongly preferred to remain on his current psychiatric regimen of escitalopram, divalproex sodium, and olanzapine-samidorphan, as he felt good control of his psychiatric symptoms with these medications. We shared our concern regarding his cachexia, malnutrition, and the appetite suppression from samidorphan and introduced the anticipated concern of escalating pain that would not be possible to treat with opioids while on olanzapine-samidorphan. The recommendation was made to transition to olanzapine only and consider metformin for management of metabolic syndrome if needed. While this was not explicitly recommended by his community psychiatrist, we fostered comfort and collaboration with the patient to emphasize that increasing weight and pain control better supported his long-term goals for ongoing cancer-directed therapy. The patient’s psychiatric regimen was transitioned to olanzapine alone, together with escitalopram and divalproex sodium.
Discussion
This case highlights the importance of thorough and ongoing medication reconciliation for patients with cancer and comorbid serious mental illness to improve overall quality of care. Palliative care providers, who are experts in symptom pharmacology, must be acutely aware of the complexities posed by new medications, specifically novel psychotropics. Psychiatrists, as well, must recognize when it may be appropriate to transition from managing long-term side effects of psychotropics to a more short-term palliative treatment approach.
In patients with anorexia-cachexia syndrome and cancer-related pain, the limitations of the samidorphan component in olanzapine-samidorphan appear to outweigh the benefits compared to patients with psychiatric illness alone. Because samidorphan is an opioid receptor antagonist, the co-administration of opioids, as often needed for cancer-related pain, can interfere with effective pain management. 20 The Federal Drug Administration warns that olanzapine-samidorphan is “contraindicated in patient using opioids” partly for this reason, since attempting to overcome the opioid blockade by administering high or repeated doses of opioids could result in life-threatening opioid intoxication, including respiratory arrest and circulatory collapse. 33 Though to our knowledge, there are no known cases of ineffective opioids or of opioid overdose while on olanzapine-samidorphan, the manufacturer warns that this risk is increased over time, as the blocking effect of samidorphan slowly decreases and eventually completely goes away, resulting in heightened sensitivity to opioids and increased potential risk of overdose. Conversely, though not commonly encountered in palliative care settings, it is known that starting olanzapine-samidorphan on an opioid-dependent patient poses a risk of precipitated withdrawal.34B35 -37 The manufacturer recommendation is for there to be a 7-day opioid-free interval from the last use of short-acting opioids and a 14-day opioid-free interval from the last use of long-acting opioids before initiation olanzapine-samidorphan. 33 Both palliative care and psychiatry professionals should be aware of these risks when prescribing and reconciling medications for patients with comorbid diagnoses of cancer and psychiatric disorders.
Importantly, samidorphan does not provide additional psychiatric stability, 20 which was relevant in addressing the patient’s concerns regarding his psychiatric goals of care. Given his cancer-related symptoms of anorexia and pain, the benefit from samidorphan was limited, and therefore, the recommendation to transition to the same, previously effective dosage of olanzapine alone was made. The only change in medication was to remove the opioid antagonist, samidorphan, which was mitigating the metabolic effects of olanzapine. To address the concern regarding olanzapine’s long-term metabolic side effects, we emphasized the current benefit of these metabolic side effects for treating his cancer-related anorexia.38,39 Though unlikely to provide benefit for this patient, as he was no longer obese by Body Mass Index criteria or experiencing symptoms of metabolic syndrome, we also considered an alternative approach commonly used in psychiatric settings: low-dose metformin to mitigate metabolic side effects of olanzapine alone.38-40 This technique has been noted in palliative care patients experiencing metabolic syndrome with olanzapine. 41
The overall recommendation of deprescribing is an essential skill in both palliative care and psychiatry.42,43 In palliative care, the primary goal is to enhance quality of life by managing current symptoms, rather than focusing on prevention of long-term health conditions. In psychiatry, the primary deprescribing barrier includes fear of psychiatric relapse. 44 When treating medically ill psychiatric patients, concerns about potential adverse medication interactions that would prompt deprescribing are often balanced against fears of destabilizing psychiatric symptoms and contributing to further functional decline during an already challenging time. 45 In this case, challenges arose when a palliative care specialist recommended a change to a regimen that the patient had been instructed to adhere to strictly by a trusted long-term psychiatrist with whom he had a strong therapeutic alliance. However, given his medical condition, through shared decision-making with the patient, the decision was made to adjust his psychiatric regimen at the time of his presentation to supportive oncology, as this clearly seemed to outweigh potential risks. This is why shared decision-making, and collaboration among specialists are essential for the treatment of patients with comorbid psychiatric and physical illness. 46
In conclusion, this case highlights the importance of thorough and ongoing medication reconciliation for patients with cancer and comorbid serious mental illness to improve overall quality of care. In summary, for patients with anorexia-cachexia syndrome and cancer-related pain, the risks of the samidorphan component in olanzapine-samidorphan (Lybalvi) outweigh its potential benefits, and intentional discussion of medication interactions and the benefits of deprescribing, in the context of prognosis and expected health trajectory, needs to occur with patients and collaborating medical specialists.