
Abstract
Context:
The clinical characteristics of terminal dyspnea, including opioid effects, adverse events, and outcome acquisition rates, remain largely unexplored.
Objectives:
To investigate the clinical characteristics of terminal dyspnea in patients with cancer starting regular systemic opioid therapy, classified by clinician-predicted prognosis (days, weeks, months).
Methods:
This secondary analysis of a multicenter, prospective, observational study included adult patients with cancer who began regular systemic opioid therapy for dyspnea at 12 palliative care sites in Japan. Patients were classified into three prognostic groups: days (1–14 days), weeks (15–56 days), and months (>56 days) according to clinician-predicted survival [CPS]. Dyspnea intensity (numerical rating scale [NRS], Integrated Palliative care Outcome Scale [IPOS]) was assessed every 24 hours for 3 days. Adverse events and outcome acquisition rates were also evaluated.
Results:
A total of 402 patients were enrolled (days: 186, weeks: 174, months: 42). NRS and IPOS scores significantly improved across all groups. At 72 hours, mean NRS decreased from 7.2 to 4.5 in the days group, 6.5 to 3.9 in the weeks group, and 5.8 to 3.2 in the months group (p < 0.001 for all). Mean IPOS showed similar reductions. Somnolence and delirium increased in the days group, whereas such trends were not observed in the other groups. NRS acquisition rates declined in the days group (73.1–55.2%) but remained high in the weeks and months groups. IPOS acquisition rates were consistently high across all groups.
Conclusion:
Opioids alleviate dyspnea in patients with cancer regardless of CPS, but persistent symptoms remain. In imminently dying patients, adverse events were common and NRS was often not assessable. Further research should be conducted to optimize the assessment and management of patients with terminal dyspnea.
Keywords
Key Message
This study examined terminal dyspnea in patients with cancer who began regular systemic opioid therapy, classified by CPS. Opioids alleviated dyspnea regardless of the prognosis. In imminently dying patients, adverse effects were common, and NRS was often unassessable, while IPOS proved useful as a proxy assessment tool.
Introduction
Dyspnea is one of the most common and distressing symptoms in patients with advanced cancer, with prevalence rates ranging from 10% to 70%. 1 Treating the underlying cause of dyspnea is essential for its management. However, as the disease progresses, treatment becomes increasingly challenging and refractoriness often develops, necessitating a more symptom-oriented approach.2,3 In particular, dyspnea can rapidly worsen as death approaches, often becoming resistant to palliative treatments, and sometimes leading to the need for palliative sedation.4–6 Therefore, timely evaluation and proactive symptom management are crucial and necessitate specialized palliative care. Dyspnea in the terminal phase of cancer is referred to as terminal dyspnea, tentatively defined as dyspnea in patients with an estimated life expectancy of days to weeks. 7 Opioids have been shown in randomized controlled trials to be the only effective treatment for alleviating cancer-related dyspnea,8,9 and international guidelines recommend opioids for treating dyspnea in patients with cancer, regardless of the stage.2,3,10 However, much of the existing literature focused on dyspnea in patients who were not yet in the dying phase. Some prospective observational studies included patients with cancer in the dying phase, but they did not classify patients by prognosis and were limited by small sample sizes, short observation periods (1–2 days), and the absence of patient-reported outcomes.11,12 The clinical characteristics of terminal dyspnea, as well as effects and adverse events (AEs) of opioids, remain largely unexplored, and evidence for its management is limited. Given the limited evidence, further investigation into the clinical characteristics and treatment outcomes of terminal dyspnea is warranted. In addition, including patients with a longer prognosis (i.e., months) provides a broader clinical context and helps clarify whether the clinical course and treatment responses of patients with terminal dyspnea differ from those of patients with more stable conditions. Furthermore, as death approaches, the level of consciousness inevitably deteriorates, making subjective assessments increasingly difficult.4,13 Currently, no international consensus exists on how to measure the subjective intensity of dyspnea in patients with impaired communication abilities. In the terminal setting, it remains unclear how many patients can reliably provide patient-reported outcomes.
Therefore, this study investigated the clinical characteristics of terminal dyspnea in patients with cancer who started regular systemic opioid therapy for its management. Specifically, patients were classified into three groups (days, weeks, and months) based on clinician-predicted survival (CPS) and the clinical features, effects, and AEs of opioids, and the rate of outcome acquisition, including patient-reported outcomes, was evaluated over a 72-hour period.
Methods
Design
This was a secondary analysis of a multicenter, prospective, observational study that evaluated the effectiveness of regular systemic opioid therapy for dyspnea in patients with cancer. Methodological details have been reported elsewhere. 14 From December 2019 to August 2021, we consecutively enrolled adult patients with cancer who had started regular systemic opioid therapy for dyspnea at palliative care units or palliative care consultation teams at 12 sites in Japan. The study adhered to the Declaration of Helsinki, and the protocol was approved by the Institutional Review Board (IRB) of NHO Kinki Chuo Chest Medical Center, as well as IRBs of all participating sites. In accordance with the ethical guidelines for human research issued by the Ministry of Health, Labor, and Welfare in Japan, the requirement for informed consent was waived due to the observational nature of the study. 15 The trial was registered at UMIN-CTR (UMIN 000038918).
Participants
Inclusion criteria were as follows: adult patients who were hospitalized and had an Integrated Palliative care Outcome Scale (IPOS) dyspnea score of 2 or higher at the initiation of regular systemic opioid therapy.11,12 Exclusion criteria were patients expected to require therapeutic interventions for dyspnea due to nonmalignant causes within three days of enrollment (e.g., antibiotic therapy for pneumonia, treatment for asthma attacks, or acute exacerbations of chronic obstructive pulmonary disease), as well as those scheduled to undergo procedures that could acutely affect dyspnea symptoms (e.g., pleural fluid drainage or airway obstruction stenting).
Measurements
At the baseline, clinicians recorded various clinical parameters, including patient demographics, primary cancer site, presence of metastases, presence of pleural effusions, underlying causes of dyspnea, CPS (days: 1–14 days; weeks: 15–56 days; and months: >56 days), 16 Eastern Cooperative Oncology Group Performance Status (ECOG PS), coexisting respiratory diseases, smoking history, current medications (benzodiazepines and corticosteroids), blood laboratory results, and anxiety intensity as assessed by IPOS. Opioid therapy for dyspnea was classified into the following categories: initiation of opioids for opioid-naïve patients, opioid switching, dose escalation of baseline opioids, and addition of another opioid to the baseline opioid (opioid combination). Additionally, types of opioids administered for dyspnea (morphine, oxycodone, hydromorphone, and fentanyl) and dosage of regular opioids for dyspnea, calculated as the oral morphine equivalent daily dose (OMEDD), were recorded. Opioid doses were recorded only for scheduled administration, and rescue doses were not included. After enrollment, the intensity of dyspnea was assessed using the numerical rating scale (NRS) and IPOS. Patient-reported effectiveness,17,18 respiratory parameters (respiratory rate, oxygen saturation, and oxygen flow rate, etc.), and AEs were also evaluated. These parameters were measured at the baseline and every 24 hours for up to 3 days following the initiation of regular systemic opioid therapy for dyspnea. The average dyspnea intensity over 24 hours was evaluated using NRS (0–10, with 0 indicating no dyspnea and 10 indicating the worst possible dyspnea) as a patient-reported outcome.19,20 Since a significant percentage of participants were expected to be unable to provide patient-reported outcomes due to cognitive impairment or reduced awareness, dyspnea intensity was also assessed using IPOS for the previous 24 hours as a clinician-rated outcome. The dyspnea item of IPOS was evaluated using a 5-point Likert scale (0 = not at all; 1 = slightly; 2 = moderately; 3 = severely; 4 = overwhelmingly).21,22 Patient-reported effectiveness was assessed using a three-category scale: improved, unchanged, and worsened, to evaluate overall improvement after opioid administration.17,18 Common opioid-related AEs, such as nausea, somnolence, and delirium, were assessed using the Japanese version of the Common Terminology Criteria for Adverse Events version 5.0. 23 Other AEs of grade 3 or higher were also assessed using the same criteria. Treatment-emergent AEs (TEAEs) were defined as new or worsening symptoms that developed after the baseline evaluation. All assessments were performed and recorded by trained investigators at each site. Physicians were permitted to adjust the dosage as needed, taking into account factors such as organ function and the preferences of the patient and family, and to provide concurrent palliative treatments for dyspnea, including rescue opioid use in accordance with routine clinical practice.
Statistical analyses
In the secondary analysis, patients were classified into three groups based on CPS. The primary outcome was the change from baseline in the mean dyspnea NRS score at 72 hours after the initiation of regular systemic opioid therapy in each group. Secondary outcomes included: changes in the dyspnea NRS score at each assessment time point, changes in the dyspnea IPOS score, percentage of patients with at least a 1-point decrease in the NRS score, percentage of patients with an IPOS score of lower than 1, percentage of patients reporting improvement in patient-rated effectiveness, and TEAEs in each group. Descriptive statistics were used to summarize baseline data and outcomes over time. Differences in NRS and IPOS scores between the baseline and each assessment time point were evaluated using a paired t test. The mean difference in NRS scores from the baseline at each assessment time point is reported with 95% confidence intervals. A sensitivity analysis (last observation carried forward) was conducted to address missing data. The acquisition rates of NRS and IPOS were calculated as the number of evaluable patients as a proportion of surviving patients at each time point. For all statistical analyses, a two-sided p value of below 0.05 was considered significant. Although patients were classified based on CPS, no direct comparisons were made between groups due to markedly different patient backgrounds. Statistical analysis was performed using SPSS for Windows software (version 25.0, IBM Japan Institute, Tokyo, Japan).
Results
A total of 402 patients with cancer who began regular systemic opioid therapy for the management of dyspnea were enrolled (Table 1). The mean age of patients was 70.4 years (standard deviation [SD]: 12.6), with 45.3% being female. The most common primary cancer type was lung cancer, and more than half of the patients had lung metastases (51.5%) or pleural effusion (63.2%). The underlying causes of dyspnea were lung tumors (31.1%), pleural effusion (29.4%), and lymphangitis carcinomatosa (11.4%). Patients were classified according to CPS, with 186 patients in the days group, 174 patients in the weeks group, and 42 patients in the months group. ECOG PS of 3–4 was observed in 99.5% of patients in the days group and 89.1% in the weeks group, whereas 47.6% of patients in the months group had ECOG PS of 3–4. Regarding the number of deaths within 72 hours, 79 patients (42.5%) in the days group, 22 patients (12.6%) in the weeks group, and 3 patients (7.1%) in the months group had died. Opioid-naïve patients comprised 98 (52.7%) of those in the days group, 96 (55.2%) in the weeks group, and 30 (71.4%) in the months group. The mean OMEDD among opioid-tolerant patients was 58.3 mg (75.8) in the days group, 54.1 mg (SD: 60.4) in the weeks group, and 46.7 mg (37.8) in the months group.
Patients’ Characteristics
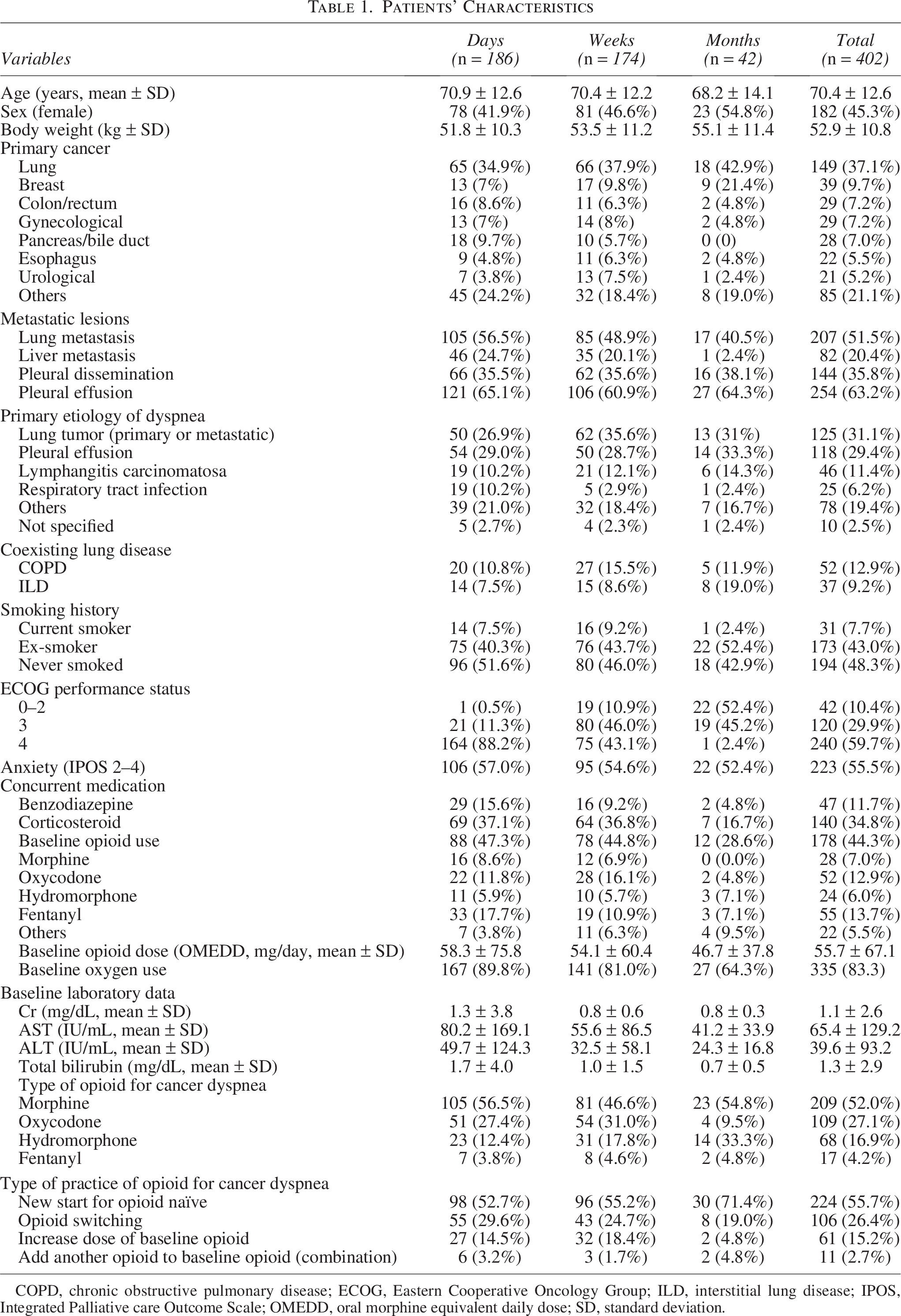
COPD, chronic obstructive pulmonary disease; ECOG, Eastern Cooperative Oncology Group; ILD, interstitial lung disease; IPOS, Integrated Palliative care Outcome Scale; OMEDD, oral morphine equivalent daily dose; SD, standard deviation.
Change in intensity of dyspnea
Figure 1 shows changes in dyspnea intensity at the baseline and 24-hour intervals following the initiation of regular systemic opioid therapy for dyspnea. In the days group, the mean NRS score significantly decreased from 7.2 (SD: 2.0) at the baseline to 4.5 (2.8) at 72 hours, with a mean difference of 2.7 (95% confidence interval [CI]: 1.9–3.5; p < 0.001). Similarly, the mean IPOS score in the days group declined from 2.9 (0.6) at the baseline to 1.4 (1.0) at 72 hours, demonstrating a significant reduction (mean difference: 1.5; 95% CI: 1.3–1.7; p < 0.001). Significant reductions in both NRS and IPOS scores were also observed in the weeks and months groups. Furthermore, reductions in both scores were evident across all three groups at 24 and 48 hours. These findings were consistent with sensitivity analysis (Table 2 and Supplement Table S1). The percentage of patients showing a decrease of at least 1 point in the dyspnea NRS score at 72 hours after initiating regular systemic opioid therapy was 44 patients (77.2%) in the days group, 90 patients (84.1%) in the weeks group, and 27 patients (84.4%) in the months group. Similarly, 63 patients (60.0%) in the days group, 86 patients (58.5%) in the weeks group, and 15 patients (44.1%) in the months group achieved a dyspnea IPOS score of 1 or lower at 72 hours. Patient-reported effectiveness indicated improvement in 74 patients (70.5%) in the days group, 104 patients (70.7%) in the weeks group, and 19 patients (55.9%) in the months group.
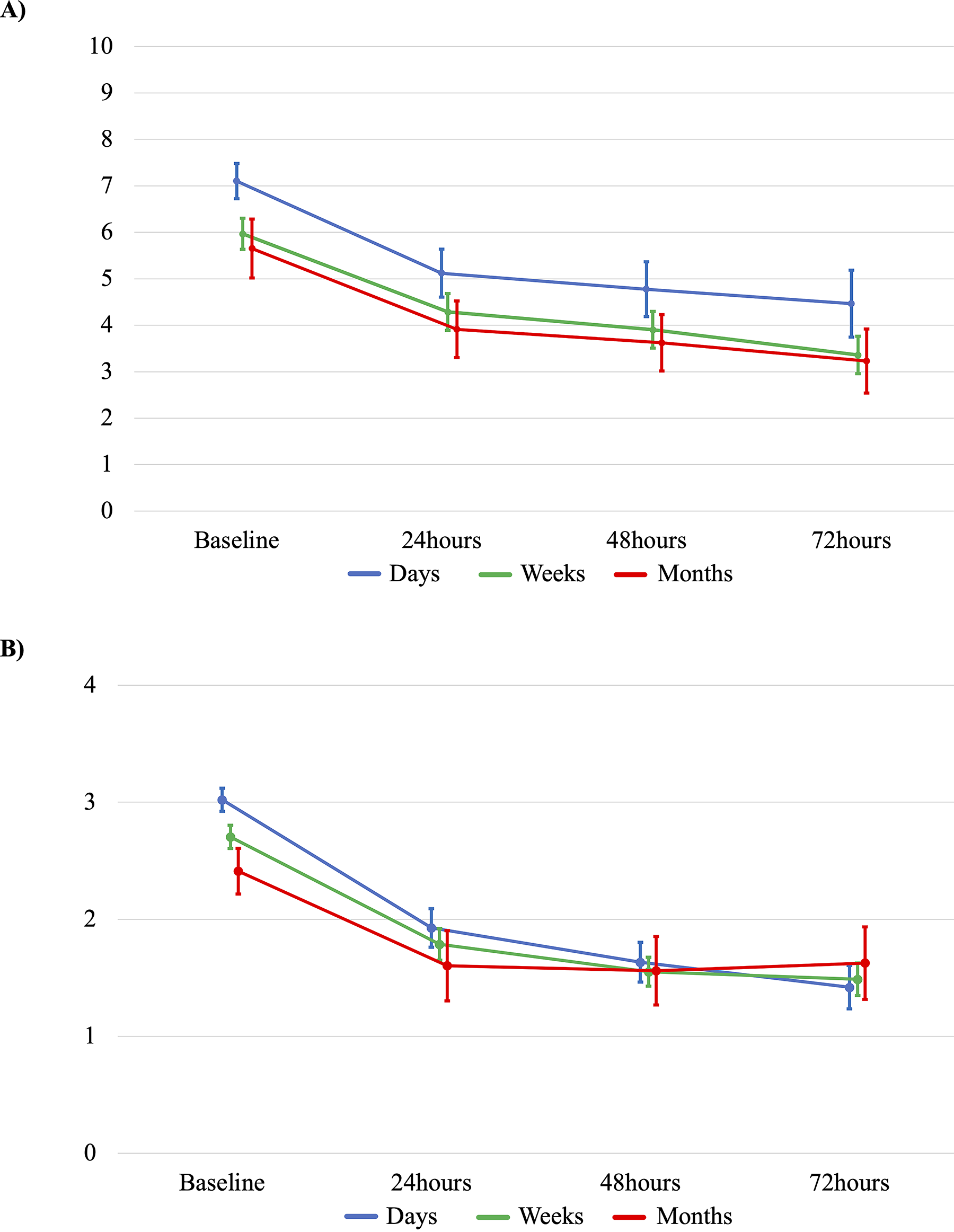
Change in intensity of dyspnea. Bars show 95% confidence intervals.
Distributions of Outcomes Over 72 Hours
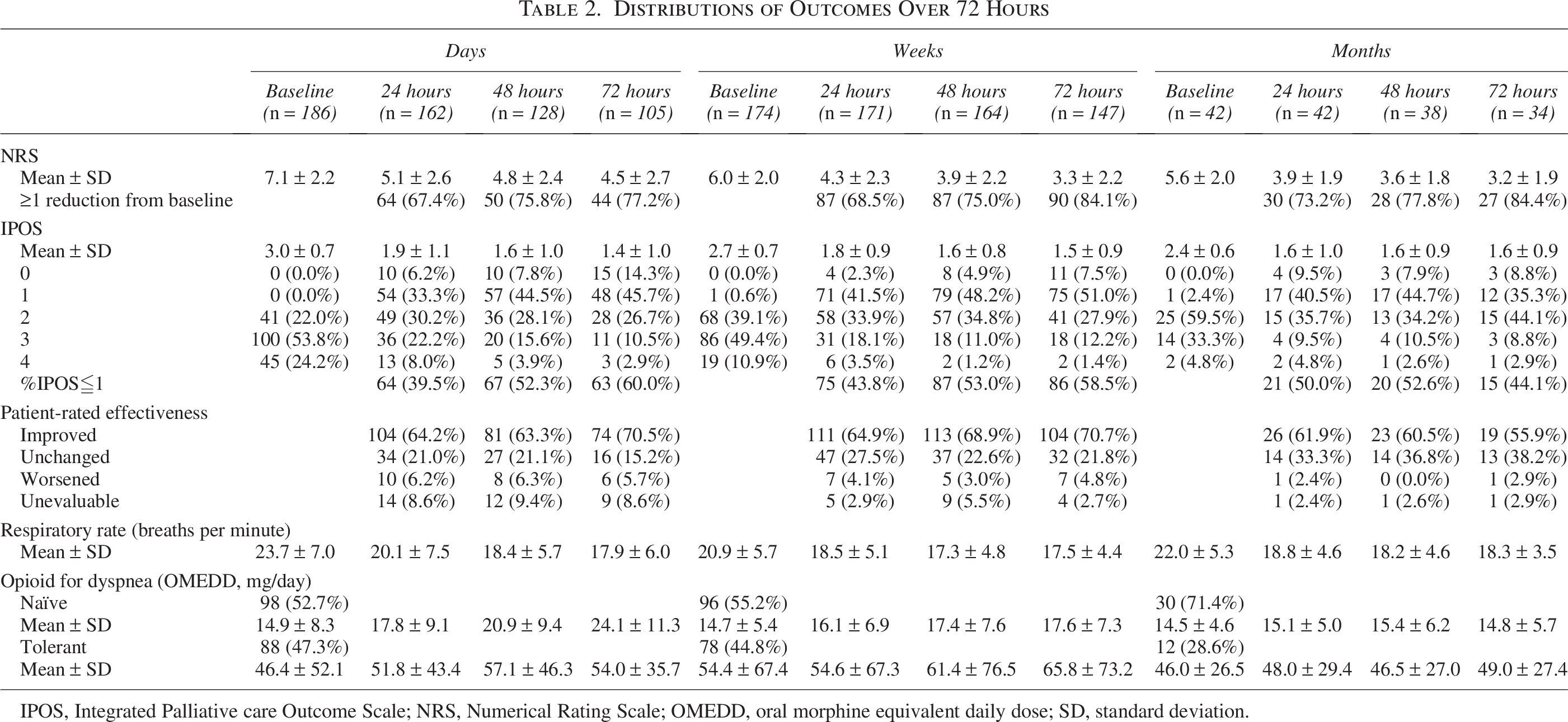
IPOS, Integrated Palliative care Outcome Scale; NRS, Numerical Rating Scale; OMEDD, oral morphine equivalent daily dose; SD, standard deviation.
AEs
Table 3 shows an overview of TEAEs. In the days group, somnolence was the most frequently reported TEAE, with incidence rates of 35.8%, 43.0%, and 48.6% at 24, 48, and 72 hours, respectively, showing a progressive increase over time. Delirium showed a similar trend, with incidence rates of 15.4%, 21.1%, and 25.7% at 24, 48, and 72 hours, respectively. In contrast, no such trend was observed in the weeks or months group. Supplement Table S2 presents AEs recorded. No cases of respiratory depression were reported at any time point (Table 2).
Treatment-Emergent Adverse Events
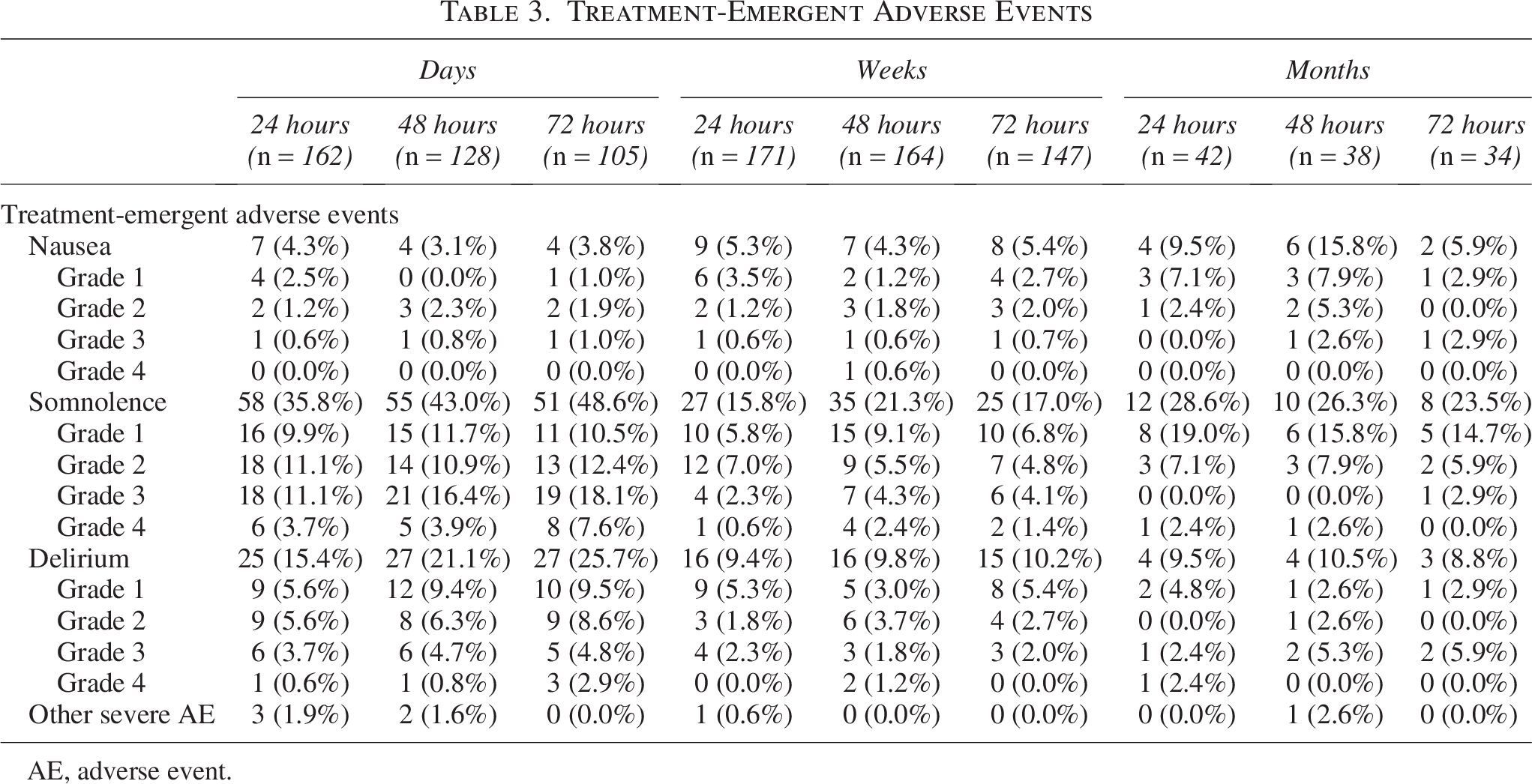
AE, adverse event.
Outcome acquisition rates
Table 4 shows acquisition rates of NRS and IPOS at the baseline and 24-hour intervals following the initiation of regular systemic opioid administration for dyspnea. The NRS acquisition rate in the days group decreased from 136 patients (73.1%) at baseline to 58 patients (55.2%) at 72 hours. In the weeks group, 145 patients (83.3%) were assessed at the baseline, and 112 patients (76.2%) were assessed at 72 hours. In the months group, all 42 patients (100.0%) were assessed at the baseline, and acquisition rates remained high, with 32 patients (94.1%) assessed at 72 hours. Acquisition rates of IPOS remained consistently high at each evaluation time point across all three groups.
Outcome Acquisition Rates
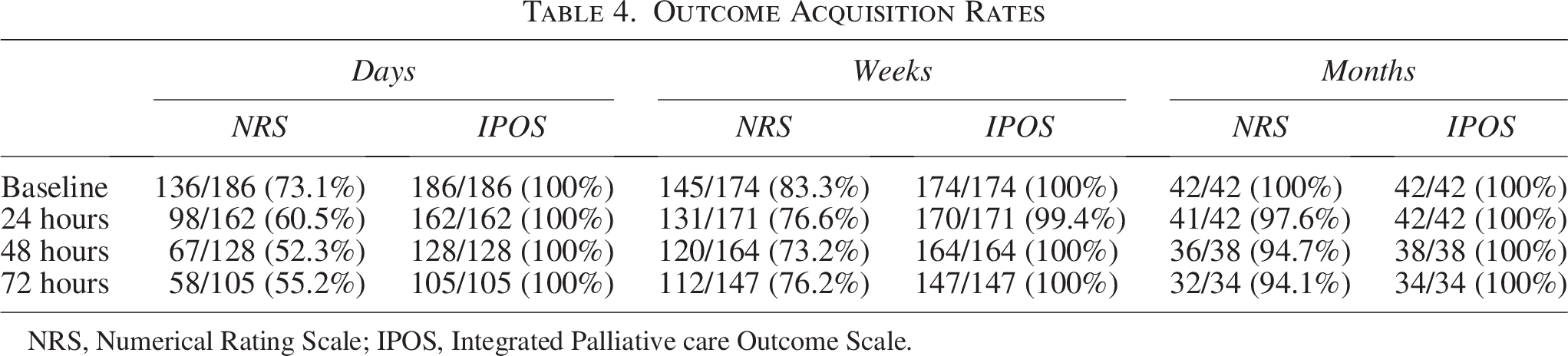
NRS, Numerical Rating Scale; IPOS, Integrated Palliative care Outcome Scale.
Discussion
This study is the first to investigate the clinical characteristics of terminal dyspnea in patients with cancer starting regular systemic opioid therapy for dyspnea management, including clinical features, opioid effects and AEs, and rate of outcome acquisition, stratified by clinician-predicted prognosis (days, weeks, months). Patients in the days group showed a higher severity of dyspnea and an increased incidence of adverse AEs such as somnolence and delirium, and the rate of patient-reported outcomes was lower.
The first important finding concerns the intensity of dyspnea. The degree of dyspnea was more severe in the days group compared with weeks and months groups, which were in more stable conditions. However, both NRS and IPOS scores for dyspnea decreased over 72 hours after the initiation of regular systemic opioids in all three groups. This indicates that opioid therapy should be proactively administered for dyspnea regardless of the prognosis. Opioids were effective even for patients in the dying phase, highlighting the applicability of evidence for the days group, which is a vulnerable population often excluded from clinical studies. In all three groups, opioids were effective, as indicated by the percentage of patients showing a reduction of at least 1 point on dyspnea NRS 24 and the percentage of patients reporting improved dyspnea. Similarly, improvement in dyspnea was observed based on dyspnea IPOS scores. However, it is clinically important to note that only 40–60% of patients had a dyspnea IPOS score of 1 or lower, with the remaining patients continuing to experience moderate to severe dyspnea. This finding is consistent with a prospective observational study investigating the effectiveness of continuous morphine infusion for dyspnea in patients with cancer. 10 While opioid therapy is internationally recognized as the first-line pharmacological treatment at any stage, there remains an urgent need for effective treatment options in cases where opioids do not provide adequate relief. Particularly in the days group, further titration of opioids may be clinically controversial because uncomfortable opioid-related side effects can occur. Therefore, the development of second-line treatment beyond opioid titration becomes an urgent priority at this stage.
The second important finding concerns opioid-related AEs. The days group showed higher frequencies of somnolence and delirium at the baseline, with subsequent increases in these symptoms after the initiation of opioid therapy. These observations are consistent with the previous literature, 4 which indicates that patients who are imminently dying frequently experience delirium and impaired communication. However, given the observational nature of this study, it remains uncertain to what extent these symptoms were attributable to pharmacological effects. As death approaches, achieving optimal control of dyspnea while preserving cognitive function becomes increasingly difficult. 25 The potential trade-off between symptom palliation and cognitive preservation remains a clinically important consideration in the management of terminal dyspnea. Future studies should consider somnolence and delirium as key outcome measures in terminal dyspnea and ensure that meaningful outcomes can be assessed even in patients with impaired consciousness.
The third important finding concerns the method of assessing dyspnea. Conventionally, assessment of dyspnea using NRS has been challenging in patients with terminal cancer due to impaired communication. In this study, the limitations of NRS were evident, as approximately half of the patients in the days group were unable to provide NRS after 72 hours. In contrast, IPOS was feasible in almost all patients, suggesting that it is a promising surrogate measure for patients with terminal cancer. Since patient-reported outcomes are the gold standard for subjective assessments in both clinical practice and research,2,3 but are not always available, proxy assessments of dyspnea should be considered. Future studies should investigate how accurately IPOS reflects the degree of dyspnea in patients with impaired consciousness, whether alternative assessment methods may be more suitable for this patient population, and the establishment of its minimally clinically important difference as a crucial next step.
The strengths of this study include its multicenter design, consecutive sampling, longitudinal measurement of validated outcomes every 24 hours over a 3-day period, and a large sample size. However, there are several limitations. First, as a secondary analysis of an observational study, our findings should be considered exploratory. Second, patients were classified into prognostic groups based on CPS. CPS has often been criticized for its limited accuracy and tendency to be overly optimistic.26,27 Nevertheless, a subsequent large validation study reported that CPS is at least as accurate as other validated prognostic models (e.g., Palliative Prognostic Index [PPI]) and even superior to PPI for short-term prediction. 28 Moreover, the European Society for Medical Oncology Clinical Practice Guideline acknowledges that CPS tends to overestimate survival but still recommends its use for prognostication. 29 Thus, although CPS has limitations, its application in our study reflects real-world clinical practice. Third, although participating palliative care physicians managed dyspnea in accordance with national guidelines, 30 their approaches were not fully standardized. Variations in clinical practice may have influenced treatment outcomes, and the use of concomitant therapies was not restricted, potentially affecting dyspnea intensity. Fourth, the absence of a placebo group prevents definitive confirmation of the specific effects of systemic opioid therapy. Thus, future placebo-controlled trials will be necessary to accurately assess the effects of opioids. Fifth, the group with a poorer clinical prognosis had a lower proportion of NRS assessments, suggesting that the analysis may have been biased by the inclusion of patients with relatively better conditions, which could have potentially influenced the results regarding the effectiveness of opioids. No subjective measure of dyspnea for this population has been established. Future research needs to investigate how to assess the subjective experiences of patients in the dying phase with deteriorating communication skills. In this context, the IPOS was used as a proxy assessment of dyspnea. 19 Although it represents ordinal data, we summarized scores using mean values. Previous studies have summarized IPOS scores using means and presented interpretable results.12,14 We, therefore, adopted this previously used approach to facilitate the description of changes over time and comparisons between groups. While this represents methodological and statistical limitations, we considered it appropriate in palliative care settings where patients in the dying phase are unable to provide NRS assessments. Sixth, in the poorer prognosis group, the number of available data decreased over time due to clinical deterioration and death. As a result, patients with relatively better conditions were more likely to be included in the analyses, and those with the poorest prognosis may have been underrepresented. This limitation may have influenced the interpretation of opioid effectiveness. Finally, as palliative care physicians conducted this study, its generalizability to primary care or other clinical settings remains uncertain, warranting further research.
In conclusion, this study highlights the clinical characteristics of terminal dyspnea in patients with cancer initiating regular systemic opioid therapy. Opioids were effective across all prognostic groups, although moderate to severe dyspnea persisted despite treatment in some patients. Somnolence and delirium were common, particularly in the days group, emphasizing the need to balance symptom relief and cognitive function. While NRS assessments were limited in patients with poor prognoses, IPOS proved to be a useful proxy tool. These findings support future efforts to improve the assessment and management of patients with terminal dyspnea.
Footnotes
Acknowledgments
The authors are grateful to the Japanese Organization for Research and Treatment of Cancer (JORTC) for their support in protocol development and data management for this study.
Author Disclosure Statement
M.M. received lecture fees from Daiichi-Sankyo, Takeda Pharmaceutical Co., Ltd., and Shionogi & Co., Ltd.; Y.M. received lecture fees from Daiichi-Sankyo, Takeda Pharmaceutical Co., Ltd., and Shionogi & Co., Ltd., Hisamitsu Pharmaceutical Co., Inc., TEIKOKU SEIYAKU CO., LTD., Kyowa Kirin Co., Ltd., TERUMO CORPORATION; Y.M. received lecture fees from Hisamitsu Pharmaceutical Co., Inc., Takeda Pharmaceutical Co., Ltd., Daiichi Sankyo Co., Ltd., and Fujimoto Pharmaceutical Corporation; S.A. received lecture fees from Daiichi-Sankyo, and Shionogi & Co., Ltd.; T.Y. received lecture fees from Shionogi & Co., Ltd., Daiichi Sankyo Co., Ltd., and Hisamitsu Pharmaceutical Co., Inc., and Fujimoto Pharmaceutical Corporation. T.Y. received fees as a part-time employee. The other authors declare no conflicts of interest.
Funding Information
This study was supported by the Japanese Society for the Promotion of Science KAKENHI (JP21H02829).
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.