
Abstract
Undocumented patients face structural constraints to accessing life-sustaining treatments in the subacute setting due to gaps in health care coverage. We present the case of a 38-year-old Spanish-speaking woman with short bowel syndrome, dependent on prolonged parenteral nutrition after critical illness, who faced additional challenges as an undocumented and uninsured patient. Despite medical stabilization and a consistent desire to pursue life-prolonging care, discharge planning was complicated by a health care system not designed to support individuals without legal status or insurance. This case illustrates the role of palliative care teams in bridging structural gaps through interdisciplinary collaboration and institutional advocacy.
“When we lean away from rather than into
∼Michael A. Light (2023)
Introduction: Structural Barriers to Subacute Care
Advance care planning does not occur in a vacuum. It is shaped by policies and social conditions that determine which options are realistically available to patients. Such structural constraints affect people’s well-being while they live and when they die. When exploring the goals of care, clinicians must often contend with systemic limitations that shape what is possible, especially for socially marginalized populations. This case illustrates the constrained choices such patients face during serious illness and end of life and highlights how the palliative team can collaborate with other disciplines and institutions to navigate these constraints toward goal-concordant care.
Case description
Adriana (name changed), a 38-year-old Spanish-speaking woman with systemic lupus erythematosus, lupus nephritis, and antiphospholipid syndrome, presented with multiple occlusive deep vein thromboses (DVTs). Her hospitalization was prolonged and marked by intermittent periods of critical illness. She developed toxic megacolon, necessitating an emergent subtotal colectomy, followed by several small-bowel resections. Postoperatively, she was left with a high-output ileostomy and short bowel syndrome.
Psychosocially, Adriana was a mother to two preadolescent daughters. She and her children had emigrated from Central America several years before her hospital presentation. Adriana was undocumented, resided with her daughters and a roommate in the community, and lived below the federal poverty line. A sibling lived locally and was involved in her care. The rest of her family resided in her country of origin.
During her nearly 9
What Happens When the System Can’t Support the Goal?
Although initially consulted during Adriana’s critical illness to address the goals of care and possible end-of-life care planning, the palliative care team quickly recognized that her goals were clear, consistent, and deeply rooted in her role as a mother. She expressed a desire to pursue all life-prolonging interventions to remain alive for her two preadolescent daughters. However, the distress experienced by both the care team and Adriana’s family reflected a deeper dilemma: the disconnect between her expressed goals and the reality of constrained options in a fragmented health system. The palliative care team worked collaboratively to support Adriana’s goals of care, coordinating with medical teams and case management to plan for treatment and to provide family support.
This dilemma is captured by the public health scholar Andrea Grindrod’s framework, which emphasizes that “choice depends on options”—that is, the ability to make meaningful decisions about one’s care is inextricably tied to the availability and accessibility of those options. 2 Social determinants, such as immigration status, social isolation, and housing, shape the conditions under which seriously ill individuals make decisions. In Adriana’s case, her ability to choose long-term artificial nutrition and home-based recovery was constrained due to her immigration status, lack of insurance, and employment status. Furthermore, our public hospital has partnered with neighboring counties to care for residents who are under- or uninsured, but Adriana formally resided outside the hospital’s funded safety net.
In this context, goals-of-care conversations can risk feeling performative: clinicians may skillfully elicit patient values but lack the resources to support them. Exploring goals and values without the ability to support concordant care may challenge the basic ethical principles of patient autonomy and nonmaleficence, leading to moral distress for patients, family caregivers, and clinicians. The dilemma is not about whether Adriana understood her prognosis or made appropriate decisions—it is that the system was not designed to honor the goals she clearly articulated.
Interdisciplinary Strategies and Institutional Support to Bridge Systemic Gaps
Institutional support proved essential in addressing the systemic gaps in Adriana’s care. As the patient’s acute condition stabilized, the hospital ethics service led interdisciplinary planning meetings that brought together case management, the primary surgical team, nutritional services, nursing, and the palliative care team. This committee met almost weekly during the last months of this admission to address the complex discharge. The committee set out to identify and address the patient’s values in the context of her clinical and logistical needs. Each discipline contributed essential expertise. For example, the dieticians recommended nutritional adjustments, while the nursing staff monitored patient distress and intake and output at bedside. The ethics service provided decision-making frameworks, the primary surgical teams monitored clinical complexity, and the case management coordinated potential discharge pathways and provided cost information.
The palliative care team provided a critical role in monitoring clinical milestones and supporting communication and values alignment. The members of the interdisciplinary palliative care team offered tailored interventions rooted in each discipline’s respective expertise. The palliative social worker addressed language barriers to optimize advance care planning discussions; offered culturally sensitive, short-term psychotherapeutic support to the patient, who evidenced depression and grief secondary to her changing role as a critically ill parent; and caregiver support to the patient’s brother, her legal next of kin. The social worker also coordinated Child Life support for Adriana’s daughters, who visited almost daily. The palliative care chaplain followed Adriana’s care closely and offered spiritual and existential support several times. Of note, Adriana and her family were reluctant to receive such support, as they equated spiritual care with the acknowledgment of impending death. The chaplain remained a vital support, however, through his participation in weekly palliative care rounds, wherein the team reviewed Adriana’s status, barriers to goal-concordant care, and the plan moving forward.
Collectively, the multidisciplinary committee comprising ethics and the specialist teams was in communication with the hospital administration, who leveraged community partnerships to identify funding sources and additional support upon discharge. This collaboration allowed the team to identify viable options for discharge and continuity of care (Fig. 1).
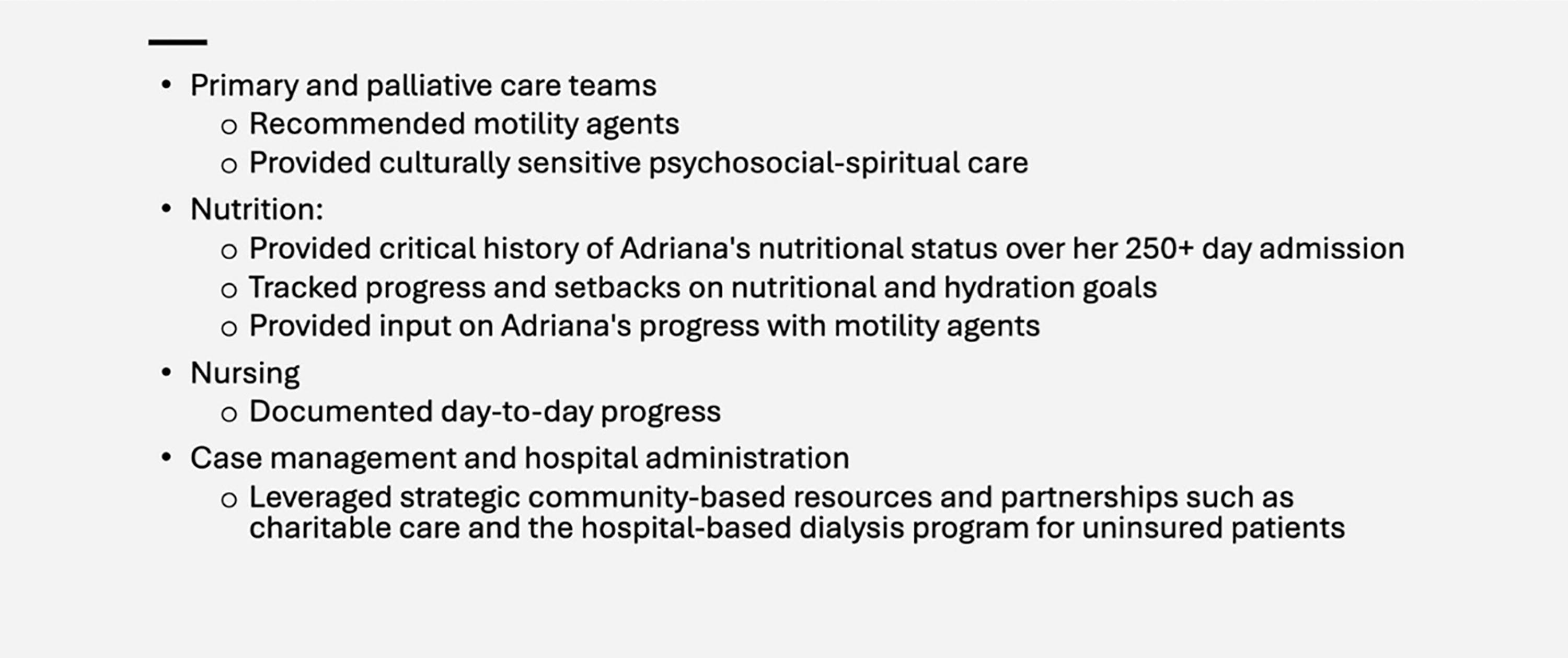
Multidisciplinary collaboration to optimize outcomes.
This collaboration helped reduce moral distress among clinicians and provided a shared framework for navigating complex discharge needs. Each team contributed unique expertise and perspectives, allowing for a coordinated strategy that leveraged both institutional resources and community partnerships. Together, the interdisciplinary group was able to bridge Adriana’s inpatient stabilization to a realistic plan for ongoing care.
Clinical outcome
Adriana was discharged to a long-term acute care facility with a time-limited provision for TPN. She was hospitalized the following month for 3 days with complications related to her bilateral percutaneous nephrostomy tubes. She was hospitalized again the next month for approximately 2 weeks for complications related to her gastrostomy tube and nutritional concerns. In subsequent goals-of-care discussions, Adriana conveyed her understanding of her prognosis and her earlier discussions about hospice eligibility. She maintained her belief that her prognosis was longer than what the medical and surgical teams were considering. Her final hospitalization was after another 2 months at an outside hospital for sepsis associated with pneumonia, decubitus ulcers, and a fungal urinary tract infection. The palliative care team at that hospital further addressed goals of care, which by now had shifted to a focus on her comfort. She was discharged under charity care provisions to an inpatient hospice in March 2025 and died approximately 1 week later.
Conclusion
We present a case that illustrates the impact of the limited options available to undocumented patients for subacute care and underscores the need for systemic and institutional strategies to bridge these gaps.
Federal legislation helps explain why patients, after stabilization during the acute period, are often discharged into systems ill-equipped to support their ongoing medical needs. The Emergency Medical Treatment and Labor Act mandates that hospitals provide emergency stabilization, regardless of immigration status or ability to pay, while the Personal Responsibility and Work Opportunity Reconciliation Act allows for limited emergency Medicaid coverage for undocumented individuals. 3 However, these protections are narrowly defined, focusing solely on acute care. Long-term treatments—such as dialysis, mechanical ventilation, and parenteral nutrition—are generally excluded from emergency Medicaid and are not covered under most state-based safety net programs. 4 These policies create structural disparities, particularly for those with serious illness, that limit patients’ ability to pursue long-term treatments that may support their goals. In addition, given the current federal budgetary considerations, the future of emergency Medicaid funding is uncertain.
Equity in serious illness care requires investment in health care and social systems beyond bedside communication, which is often relegated to a single clinician and can lead to significant clinician distress.5,6 Grindrod urges a public health approach to palliative care, which elucidates how structural inequities and policy shape the feasibility of goal-concordant care. This approach also emphasizes “multisector and civic-driven” strategies that strengthen partnerships, including with other sectors, organizations, and jurisdictions. 2 Within health care systems, forming interdisciplinary committees—including ethics, case management, palliative care, administration, and community partners—may help proactively plan care for seriously ill undocumented patients.
Adriana’s case was psychosocially and ethically complex, and the distress was multilayered for her and for all of those involved in her care. She continued to face severe nutritional challenges and complications even after discharge, and the efforts of her care team, while impactful, were bound by broader systemic constraints. The collaborative efforts that bridged her care from the ICU to the general medical floor to post-acute rehabilitation supported Adriana’s wishes to prolong her life and spend more time with her daughters. However, many were left with distress and questions about the impact of the inequities Adriana faced over the course of her illness. For the palliative care clinician, witnessing and holding suffering is the cornerstone of our work. Providing such care to individuals like Adriana, who face layers of suffering due to the lack of insurance, poverty, systemic racism, and other inequities, can lead to tremendous moral distress. 1 Acknowledging our shared humanity, accompanying seriously ill patients who experience such inequities, and finding ways to connect as individuals, institutions, and a community may help to temper our own suffering. 7 In the case of Adriana’s care, the palliative care team normalized the distress many of us experienced. During the larger treatment planning committee meetings as well as in weekly palliative care rounds, time was allocated to informally debrief as a collaborative team. Clinicians, such as the social worker and medical ethicist, acknowledged and normalized the distress associated with the barriers to care, along with the possibility of not supporting Adriana’s wishes and goals because of systemic constraints. Vital to the effectiveness of this debriefing was the investment of institutional and departmental leadership. 8
Other institutions may be able to replicate similar interdisciplinary strategies, but the greater question lies in how we decide as a society to allocate health care resources. Adriana’s case is an example of complex decisions being made by clinicians and health care systems every day. The growing moral distress among health care clinicians working diligently in such cases to advocate for the best care for each of their patients will hopefully foster a deeper examination of how public policy and structural investment can better align with our shared values as a society.
Footnotes
Acknowledgment
This case study is a follow-up to a presentation at the AAHPM Annual Assembly 2025 in Denver, CO, USA. The authors would like to thank our colleagues who contributed their critical and reflective insights in this case—Gretchen Bell, MD, Anita Sundaramoorthy, MD, Elizabeth Sivertsen, MBE, CCRN, HEC-C, Michael Wiersema, M.Div, BCC-PCHAC.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors have no funding sources to disclose.