
Abstract
Background:
Physician-assisted death (PAD) is a controversial practice, legal in mostly wealthy European countries and U.S. states with a lower-than-average proportion of Black residents. Although studies report lower support for PAD among Black Americans, a comprehensive review of the association between PAD attitudes and race and ethnicity is lacking. This narrative review sought to clarify the association between race and/or ethnicity and attitudes toward PAD, while exploring possible explanatory factors.
Methods:
A comprehensive search of PubMed, Web of Science Core Collection, and PsycINFO databases through December 2024, supplemented by citation follow-up and manual searches.
Results:
The search yielded 64 eligible studies. These studies varied in sampling method, populations, studied, survey questions, and timing. To account for quality, studies were grouped into those employing random (38) versus nonrandom (26) sampling. Across both categories, White respondents consistently demonstrated higher support for PAD than racial and ethnic minority groups, particularly Black Americans, in both unadjusted and adjusted analyses. Although some studies show adding religion variables eliminates this association, the largest and most methodologically rigorous studies still show that race and ethnicity retain an independent association with PAD attitudes. Notably, there was a paucity of studies examining trust in the health care system as a potential factor.
Conclusions:
Overall, the evidence suggests lower support for PAD among racial and ethnic minority groups that may reflect, in part, distinct sociocultural factors extending beyond religion or socioeconomic status. This review highlights the need for more research on trust in health care and nuanced understanding to guide discussions on PAD policy and practice in diverse populations.
Introduction
Since 1997, physician-assisted death (PAD)—also referred to as physician-assisted suicide (PAS) or medical aid in dying—has become legal in 11 jurisdictions in the United States. These laws allow physicians to prescribe lethal medications in response to requests by competent, terminally ill patients (life expectancy of 6 months or less). The practice remains controversial. One notable feature of PAD is its relation to race and ethnicity: it is almost exclusively a policy among wealthy, European countries, 1 and the U.S. states that have legalized PAD generally have a lower percentage of Black residents than the national average (Oregon, Washington, Colorado, etc.). Even in a diverse state like California, the practice disproportionately occurs among the White population. 2
Although most Americans support legalizing PAD, previous studies have shown that Black and other racial and ethnic minority groups are less supportive than White individuals.3–8 Differences also exist in attitudes toward other end-of-life issues such as the use of life-sustaining treatment and advance directives.9,10 The interplay between race, ethnicity, and attitudes toward and participation in PAD is undoubtedly complex, and yet, significant gaps remain in the literature that hinder a comprehensive understanding of this issue. While previous studies suggest racial and ethnic differences in PAD attitudes, they often do not explore the reasons behind these differences.
To our knowledge, this is the first comprehensive review of the literature to date that systematically examines the relationship between race, ethnicity, and attitudes toward PAD. By synthesizing and analyzing existing research, this study addresses critical gaps in understanding the nuanced dynamics that may influence PAD attitudes and participation. With more states considering PAD laws, it seems crucial to understand the values, beliefs, and perspectives of historically disadvantaged groups in this debate.11,12
We therefore conducted a comprehensive literature review and narrative analysis examining two key questions: (1) What is the association between race and/or ethnicity and attitudes toward PAD? (2) What are the potential explanations for such associations?
Methods
Given the extreme heterogeneity in the literature relevant to our study goals, we adopted a narrative review framework with a comprehensive literature search. This approach allowed us to better capture and synthesize diverse study populations, designs, and outcome measures, enabling a broader understanding of the range of evidence available. While a systematic review and meta-analysis were initially considered, substantial variation across studies rendered quantitative synthesis unfeasible.
To be included in the review, articles had to focus on assisted dying [PAD, medical aid in dying, PAS, and euthanasia and/or assisted suicide (EAS)] and report new primary data and/or analysis on the relationship between racial and ethnic groups in the United States and their opinions or attitudes toward PAD. Articles were excluded if they: did not report new primary data or analysis of existing data, did not focus on U.S. populations, were review or opinion articles, or focused on withholding or withdrawing of life-sustaining treatments or on suicide without third-party involvement (i.e., not assisted dying).
To identify potentially relevant studies, PubMed, Web of Science Core Collection, and PsycINFO databases were searched from their inception to December 2024 using strings related to PAD, behavior and culture, and race and ethnicity. The search strategies were drafted by an experienced librarian and further refined through team discussion. Complete details of the search can be found in Supplementary Data S1. The database search was supplemented by a manual search and scanning reference lists of included articles; this was particularly important since even articles whose primary focus was not on race and ethnicity and PAD (and therefore difficult to capture) could still contain “new primary data and/or analysis on the relationship between racial and ethnic groups.” C.S. and M.N. served as independent screeners for the selection of articles; any disagreement was resolved by discussion or, when needed, further discussion with S.Y.H.K.
A data charting form was jointly developed by C.S., M.N., and S.Y.H.K. to determine which variables to extract. C.S. and M.N. independently charted the data, discussed the results, and updated the data-charting form in an iterative process. Data on sample frame characteristics, sampling method, sample size, number of participants by race/ethnicity, the specific question asked, the effect of race/ethnicity (both unadjusted and adjusted), and the covariates included in the adjusted analysis were abstracted. Given the highly heterogeneous nature of the studies, we used only a single quality metric to classify them into two main groups—random (i.e., census or probability-based sampling scheme that sought representativeness to a target population) and nonrandom sample studies.
Results
The comprehensive search of databases yielded 587 unique results, providing 33 eligible articles, and an additional 31 articles were found from manual searches and screening citations in the articles, for a total of 64 articles included in the review. A PRISMA flowchart (Fig. 1) documenting the results of the search and screening process is provided. 13
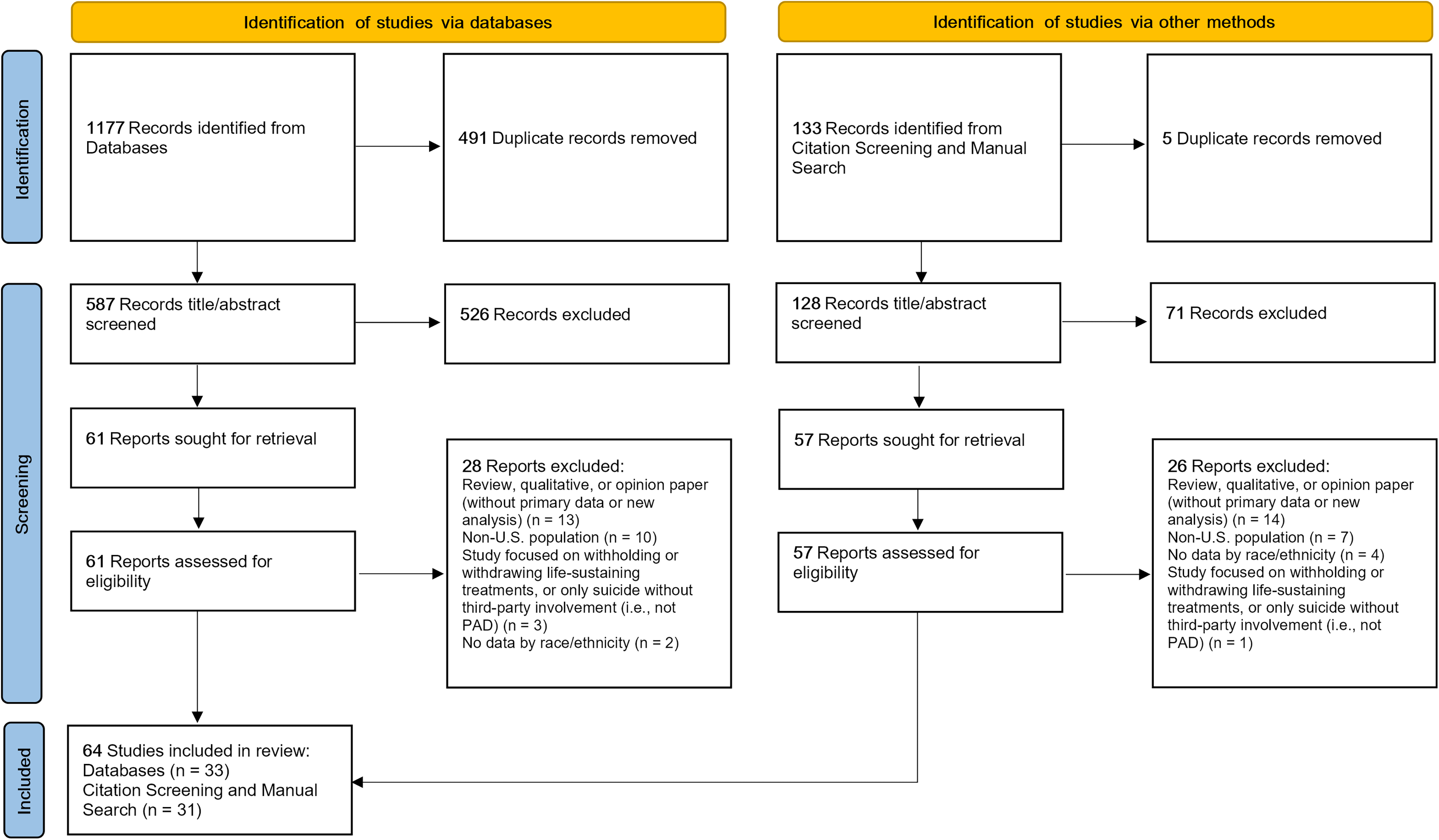
PRISMA flow diagram. Flow of study selection for narrative review on race/ethnicity and attitudes toward physician-assisted death (PAD). A total of 1,177 records were identified through database searches and 133 through citation screening and manual search. After removal of duplicates, 587 and 128 records, respectively, were screened by title/abstract. Following exclusions, 61 reports from databases and 57 from citation screening and manual search were sought for retrieval and assessed for eligibility. After excluding studies that were non-U.S. populations, lacked primary data, did not report data by race/ethnicity, or focused on end-of-life practices outside of PAD, 64 studies were included in the final review (33 from databases and 31 from other methods).
The set of articles was quite heterogeneous regarding PAD questions asked, populations studied (general public, patients, older individuals, physicians, clergy, students, etc.), time of study, racial/ethnic categorizations and terms used, sampling methods, and analytic strategies. Table 1 provides a brief description of how we handled this heterogeneity in synthesizing our findings.
Navigating the Heterogeneity Among Studies
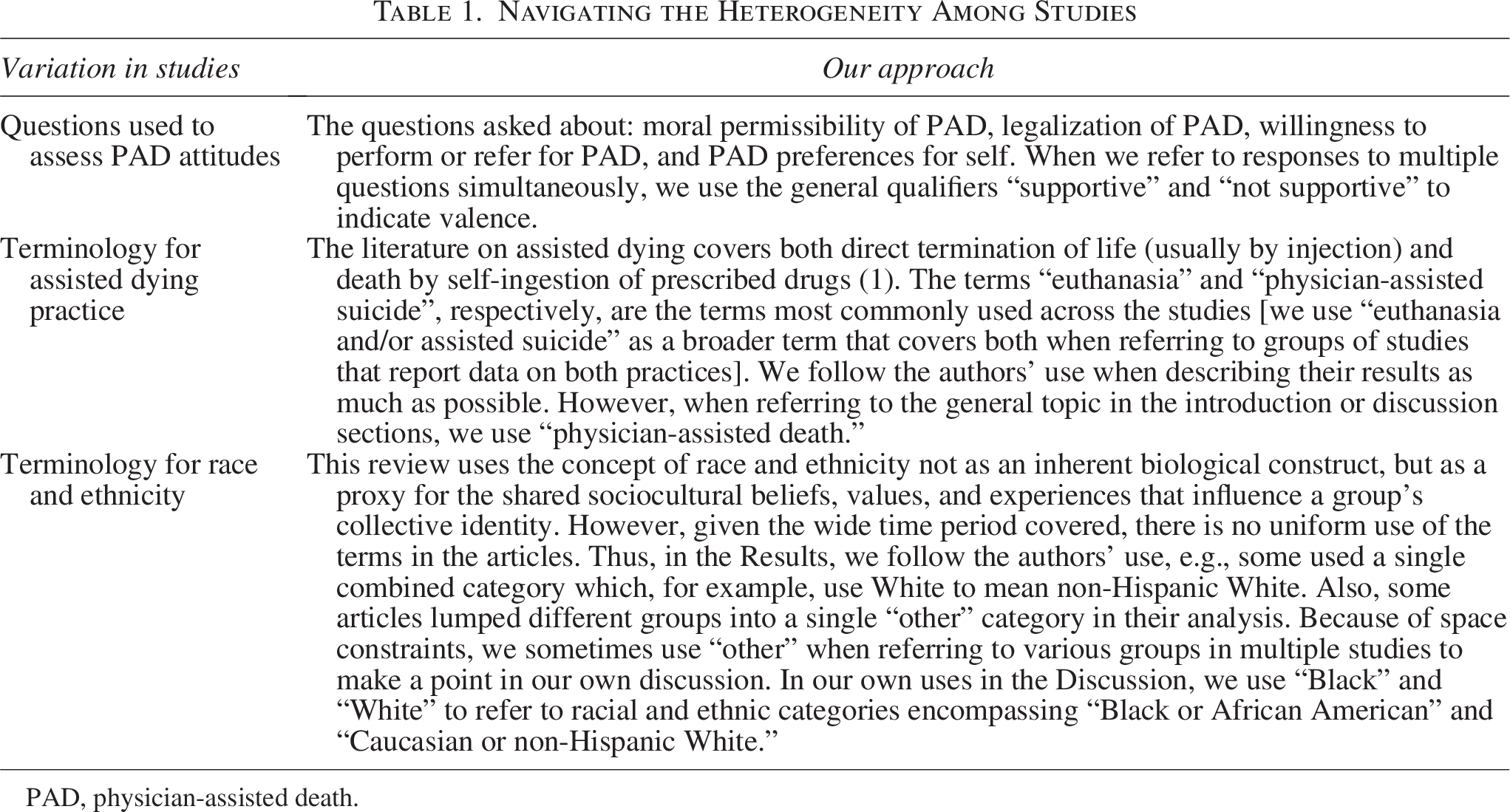
PAD, physician-assisted death.
Table 2 (random sample studies) and Table 3 (nonrandom sample studies) provide concise summaries of significant associations of race/ethnicity and attitudes toward PAD. Detailed p-values or other measures of statistical significance can be found in Supplementary Data S3.
Studies with Random Samples or Samples of Entire Populations of Interest
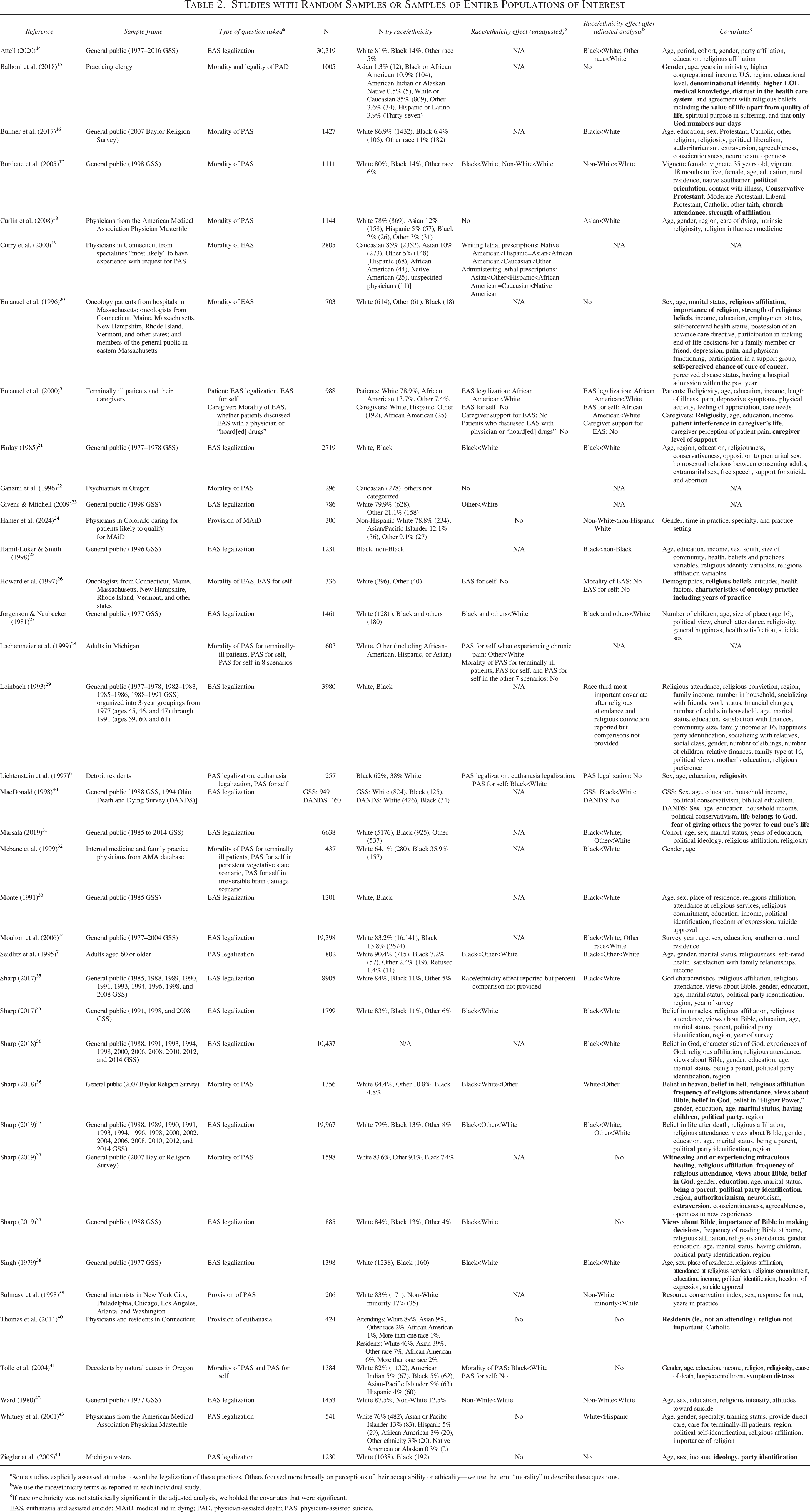
Some studies explicitly assessed attitudes toward the legalization of these practices. Others focused more broadly on perceptions of their acceptability or ethicality—we use the term “morality” to describe these questions.
We use the race/ethnicity terms as reported in each individual study.
If race or ethnicity was not statistically significant in the adjusted analysis, we bolded the covariates that were significant.
EAS, euthanasia and assisted suicide; MAiD, medical aid in dying; PAD, physician-assisted death; PAS, physician-assisted suicide.
Studies with Nonrandom Samples
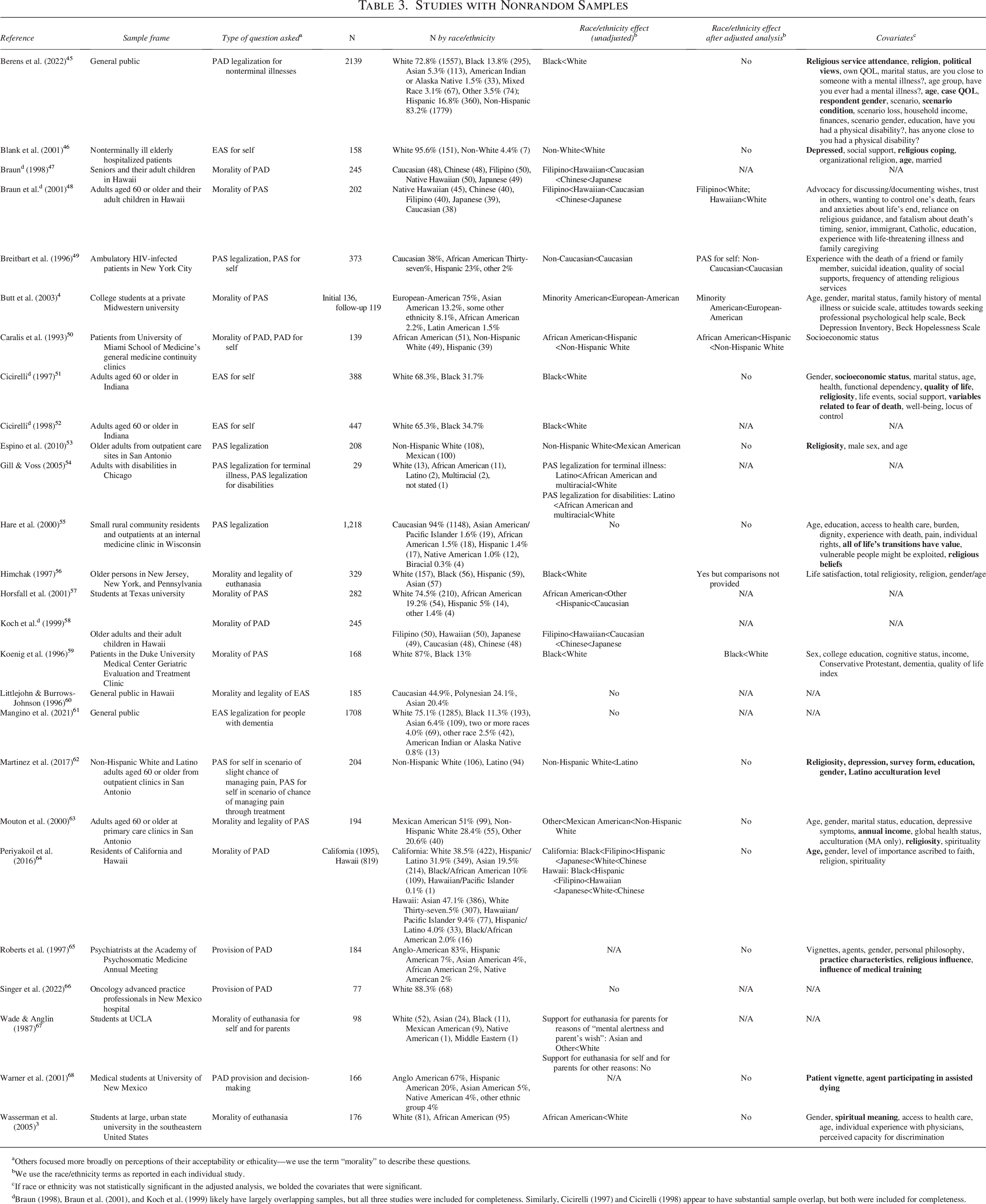
Others focused more broadly on perceptions of their acceptability or ethicality—we use the term “morality” to describe these questions.
We use the race/ethnicity terms as reported in each individual study.
If race or ethnicity was not statistically significant in the adjusted analysis, we bolded the covariates that were significant.
Braun (1998), Braun et al. (2001), and Koch et al. (1999) likely have largely overlapping samples, but all three studies were included for completeness. Similarly, Cicirelli (1997) and Cicirelli (1998) appear to have substantial sample overlap, but both were included for completeness.
Group 1: Studies with Random Samples or Samples of Entire Populations of Interest
38 studies used random sampling or a census of local groups.19,22 Of these, 24 surveyed the general public;6,14,16,17,21,23,25,27–31,33–38,42,44,69–72 4 surveyed terminally ill patients and caregivers, 5 relatives of decedents, 41 oncology patients, oncologists, and the public, 20 or older individuals; 7 9 surveyed physicians;18,19,22,24,26,32,39,40,43 and one surveyed clergy. 15
In total, 34 reported adjusted and/or multivariable analyses (but only 20 also reported unadjusted analyses). The publication dates ranged from 1979 to 2024. The survey questions ranged from attitudes toward the morality and/or legality of euthanasia and/or PAS,5–7,14–23,25–38,41–44,69–72 willingness to perform it (in physician surveys),24,26,39,40 and personally considering it.5,6,26,28,32,41
Eighteen of these studies analyzed data from the General Social Survey (GSS), a nationally representative survey regularly collected since 1972 by the National Opinion Research Center.14,17,21,23,25,27,29–31,33–38,42,70,72 Ten of the GSS studies represent analyses of various overlapping years of surveys, from 1977 to 2016 (see Supplementary Data S2for details).14,21,29,31,33–37,72 Three report analyses from the 1977 GSS,27,38,42 2 report analyses from the 1998 GSS,17,23 2 report analyses from the 1988 GSS,30,70 and 1 reports analysis from the 1996 GSS. 25 Three studies analyzed data from the 2007 wave of the Baylor Religion Survey, a nationally representative survey administered by the Gallup Organization.16,69,71
General public
Twenty of 24 general public studies found Black respondents and other racial and ethnic minority group respondents were less likely than White respondents to be supportive of EAS.6,14,16,17,21,23,25,27,29–31,33–38,40,42,69,72 Five studies provided unadjusted point estimates, with racial and ethnic minority support of EAS legalization ranging from 39% to 56%, and support among White participants ranging from 65% to 76%.6,23,27,38,42
Seventeen of the 22 general public studies that reported multivariable analyses found an independent race and/or ethnicity association, where non-White and/or Black respondents were less likely to be supportive of EAS even after adjusting for several covariates.14,16,17,21,25,27,29–31,33–38,42,72 For example, the largest study in this group (N = 30,319) found Black and ‘other race’ individuals were less likely than White individuals to support legalized euthanasia, after controlling for gender, education, political affiliation, religious affiliation, and after adjusting for age, period, and cohort effects. 14 In 3 studies, adding religion variables such as religiosity, religious beliefs, and/or religious affiliation to the model eliminated the association with race.6,69,70
Patients and caregivers, relatives of decedents, and older individuals
African American terminally-ill patients and caregivers were less likely than White, Hispanic, or other race respondents to support or have personally considered euthanasia or PAS, even after controlling for religion/religiosity (support among patients: 38% versus 64%; support among caregivers: 12% versus 31%; personally considered: 6% versus 11%). 5 Older White respondents were more likely than Black or other race respondents to support PAS legalization, even after controlling for religiosity (51% vs. 15%). 7 Family members of White Oregon decedents were more likely than those of Black decedents to report that decedents were in favor of PAS as a policy and had personally considered PAS (policy: 35% versus 15%; for self: 18% versus 0%). However, in the logistic regression for personally considering PAS, religiosity, age, and symptom distress were the only significant associations. 41 In a study of oncology patients, oncologists, and the general public, race/ethnicity was not a predictor of EAS attitudes. 20
Physicians and other professionals
In the 9 physician surveys, 5 found White physicians were more likely than physicians from racial and ethnic minority groups to support PAS;18,19,24,32,39 the effect remained in 4 of the 5 studies even after adjusting for various covariates.18,24,32,39 Racial and ethnic minority physician support for PAD ranged from 21% (Asian) to 70% (Other), while support among White physicians ranged from 33% to 76% in the 4 studies reporting unadjusted results.18,19,24,32 One study reported that Hispanic physicians were less likely than White physicians to oppose legalized PAS (AMA master file sample plus delegates N = 1000, but containing only 22 African American and 33 Hispanic respondents). 43 Finally, 3 physician studies22,26,40 (with very few respondents from racial and ethnic minority groups) and 1 study surveying U.S. clergy 15 reported no association with race.
Group 2: Studies with Nonrandom Samples
26 studies nonrandomly selected respondents from various groups (8 general public;45,47,48,55,58,60,61,64 3 older individuals;51,52,56 1 inpatient; 46 6 outpatients;49,50,53,59,62,63 5 undergraduate or medical students;3,4,57,67,68 1 each of persons with disabilities, 54 psychiatrists, 65 and oncology advanced practice professionals); 66 of these, 17 reported adjusted analyses. The publication dates ranged from 1987 to 2022. The questions ranged from attitudes toward the morality and/or legality of EAS,3,4,45,47–50,53–61,63–65,68 personally considering it,46,49–52,62,63,67 and a provider’s willingness to perform or refer a patient for it.65,66 Only 4 studies had more than 1000 respondents.45,55,61,64
General public
Of the 8 studies that surveyed the general public on a variety of questions regarding attitudes toward EAS,45,47,48,55,58,60,61,64 3 reported Black respondents were less supportive (60% Black/African American versus 76% White 64 ; Black or African American OR= 0.75, compared to White respondents 45 ; Black or African American OR = 0.51, White OR = 0.75, with ‘other race’ as reference) 61 while 3 Hawaiian studies47,48,58 reported that Filipino respondents were less supportive (26–33% Filipino versus 58–74% Caucasian versus 71–90% Japanese). In 3 of these studies, the race and ethnicity effect were nonsignificant when controlling for variables such as age and religiosity.45,61,64 Two studies did not report any difference in attitudes toward EAS between racial and ethnic groups.55,60
Older individuals
All 3 studies of older individuals (≥60 years old) reported that White respondents had more positive attitudes toward EAS than Black respondents,51,52,56 of which 1 study provided point estimates (21% White versus 15% Black individuals “endorsed” voluntary euthanasia for themselves; 16% White versus 6% Black individuals “endorsed” assisted suicide for themselves). 51 In all 3 studies, the association with race remained even after adjusting for a variety of variables, including religion.
Patients
One study surveyed older inpatients, 46 while six studies surveyed outpatients (older,53,59,62,63 HIV-positive, 49 and general outpatients). 50 Five of these seven studies reported that White patients were more likely to support EAS.46,49,50,59,63 In the two studies that reported unadjusted percentages,49,50 Non-Hispanic White support for EAS legalization ranged from 61% to 76%, while non-White (non-Caucasian, African American) support ranged from 36% to 57%. Non-Hispanic White support for EAS for oneself ranged from 46% to 50%, while non-White support ranged from 20% to 28%. In 3 of these 5 studies, White race was associated with positive attitudes toward EAS even in multivariable models.49,50,59 In 1 study that compared Mexican-American individuals and non-Hispanic White individuals, the association was present only for the assisted suicide for oneself question, but not the policy question, when controlling for gender, income, and religiosity. 63 There was no race association when controlling for depression, age, and religiosity in the last study. 46
In two studies that asked about PAS when experiencing extreme chronic pain, Latino and/or Mexican American older outpatients reported greater support than non-Hispanic White patients (N ≤ 208), although there was no effect when controlling for covariates such as age, gender, and religiosity.53,62
Other surveys
Five studies surveyed undergraduate3,4,57,67 or medical 68 students; 4 reported that White students were more likely to have positive attitudes toward EAS than various non-White groups.3,4,57,67 However, a path analysis model in one study indicated that spiritual meaning was the primary mediating variable in explaining race and ethnicity differences in attitudes toward euthanasia. 3
In 1 small study (N = 29) of individuals with disabilities, White participants were more likely to support assisted suicide. 54 Two small surveys of health professionals [psychiatrists (N = 184; 83% Anglo-American) 65 and oncology advanced practice professionals (N = 77; 88% White)] 66 reported no difference in attitudes between racial and ethnic groups.
Discussion
This narrative review of the literature brings together heterogeneous data examined over nearly 45 years, confirming the robust relationship between race and ethnicity and attitudes toward PAD. The studies with large, randomly selected samples consistently report this association,14,34,35,37 showing significantly lower rates of support for PAD among racial and ethnic minority groups, particularly among Black respondents. Negative studies tended to have very few Black and/or racial and ethnic minority respondents.20,22,26,40,60,65,66,68 It is important to note here that race and ethnicity serve as proxies for the broader sociocultural factors that reflect the shared history, experiences, and values within communities. Even so, race and cultural influences are many and complex, and cultural values and experiences are one of many factors that may influence attitudes toward PAD, with the understanding that these may vary significantly across individuals and subgroups within a broader community.
Although one cannot draw causal inferences, the results provide evidence regarding potential explanations for the finding. For instance, socioeconomic status did not appear to explain racial differences in attitudes toward PAD. 30 In surveys of physicians (i.e., persons with similar socioeconomic status), studies, including the one study we found with a substantial representation of Black physicians, 32 showed differences, even after adjusting for various covariates.18,19,24,39 Several other studies show that the association between race and PAD attitudes is largely independent of socioeconomic factors.25,29,30,33,38,50,59
The most frequently examined explanatory factor in the association between race/ethnicity and PAD attitudes is religion. Among the 24 studies that did not find a significant association with race and ethnicity in adjusted analyses, 21 contained at least one statistically significant religion-related variable (see Supplementary Data S3 for a summary). These religion-related variables ranged from: religiosity or self-reported strength of religious beliefs; religious affiliation/denominational identity; frequency of religious service attendance; and specific religious beliefs (e.g., life belongs to God, belief in miraculous healing, etc.).
Previous research has shown that Black Americans are more religious and participate more often in both organized and individual religious practices than White Americans. 73 Some speculate this may arise from religion providing meaning and refuge in overcoming a long history of oppression. Some Black Americans may regard illness and death as another struggle to overcome, and treatment decisions may be guided by a spiritual framework that emphasizes survival in the face of adversity. 73 This may also explain the greater preference of Black Americans for life-sustaining treatment at the end of life.74,75
However, differences in religious commitment between Black and White Americans may not entirely explain the difference in attitudes toward PAD. Although some studies do show that adding religion variables eliminates the association between race/ethnicity and PAD attitudes, the largest, highest-quality studies still show an independent race association, particularly significant for Black and “other” race respondents.14,21,29,31,35–37 Notably, in 21 of the 43 studies that included religion-related variables, race and ethnicity remained significant, suggesting that cultural, historical, or structural factors beyond religion may also influence these attitudes.
One possible factor explored by scholars is distrust in the medical system that may be rooted in both individual experiences with racial discrimination and the shared historical experiences of Black Americans, including systemic barriers to health care access and instances of medical exploitation (e.g., the Tuskegee syphilis study, Henrietta Lacks).30,76 Black Americans may be less likely to believe that physicians or the medical establishment will follow their best interests when it comes to end-of-life care. 6 There is perennial concern in PAD discussions that PAD may be offered as an alternative to quality end-of-life care, especially for those who receive poorer quality end-of-life care, pain management, hospice use, and provider communication.11,77–79 However, only 1 small study (of undergraduates) looked at the role of trust in medicine and PAD attitudes and found that while Black American students do exhibit higher levels of distrust of medicine, it was not associated with PAD attitudes. 3
These findings suggest there may be some other unmeasured factor related to the shared sociohistorical experiences and religio-cultural values of Black Americans. Some scholars have proposed given the history of oppression Black Americans have experienced, “suffering may be an expected part of life rather than a reason to terminate life.”32,80 Others have further noted that familiarity with struggle and extreme hardship and other factors may also explain racial differences in attitudes toward PAD.6,42 Another factor may be differences in attitudes toward community and relationships, as PAD seems to fit better with a White, Western, individualist view of life that prioritizes individual control.11,81–83
The findings of our review highlight the potential reasons why PAD is used predominantly by White patients even in racially diverse states like California where Whites make up less than 40% of the population but account for nearly 90% of PAD cases, 11 with much lower relative use of PAD among Black and Latino individuals. This trend appears to be present in all jurisdictions that report race and ethnicity data for individuals who request or receive PAD—including Oregon, Washington, Colorado, Hawaii, New Jersey, Maine, and Washington DC.84,85 Although some have suggested access to health care as a factor affecting access to PAD, 41 these trends are also likely due to the social and cultural influences of race and ethnicity, enumerated above, that affect preferences for PAD.
Policymakers should be sensitive to the diversity of views on PAD associated with race and ethnicity. Washington DC, for example, reportedly passed its Death with Dignity Act in 2016 following advocacy efforts primarily led by White individuals, despite reservations within the Black community. 86 Members of historically privileged groups, who may have greater access to care, may feel empowered to seek a right to PAD (and trust a health care system to safely provide it), but they may not fully appreciate the implications for others who, because of structural or other reasons, lack such privilege. While distinct from racial and ethnic minority perspectives, the concerns voiced by Canadian disability advocates similarly highlight issues of structural vulnerability and potential coercion in the implementation of PAD. Despite opposition from these groups and expressions of concern from the UN Human Rights Council, 87 the Canadian government enacted legislation that critics argue effectively makes PAD more accessible than the standard interventions and resources that many people with disabilities would rather have.88–92 Thus, when debating not just whether but also how to implement PAD policy, policymakers should carefully consider the views of marginalized groups.
Further, our findings suggest that in jurisdictions where PAD is legal, it is important for health care providers to understand the cultural values of the populations they serve and how these values might influence health behaviors, including requests for PAD. While it is essential to avoid stereotyping, knowing that differences in views exist supports the practice of taking a cultural and spiritual ‘history.’ Asking open-ended questions about beliefs and attitudes—which may indeed be influenced by an individual’s race or ethnic membership—can help providers gain a more comprehensive understanding of patients’ preferences and ensure that care decisions align with their values. 75
Our study has limitations. Many studies included small samples and/or very small numbers of non-White participants (limiting usefulness of models in them), recruited participants from a single center, and used nonprobabilistic sampling. There were multiple GSS studies included in our review that reported analyses from various overlapping years of surveys; we included them all as they used different analyses to test their hypotheses. Findings were also difficult to compare across studies because of the large heterogeneity in populations surveyed, in classifications of race and ethnicity, sampling methods, questions asked, analyses used, and the wide time frame of the studies. Definitions of euthanasia and PAS also varied across studies and over time. In several studies, euthanasia and PAS were not treated separately and racial and ethnic minority groups were often lumped together as “other” or non-White. Because our inclusion criteria were broad, if race and ethnicity appeared in a study’s analysis model, we included the article even if race/ethnicity relationship to PAD was not its primary focus. This likely explains why our database search yielded 33 eligible articles, supplemented by 31 additional articles from manual searches and reference lists, reflecting the secondary nature of race/ethnicity data in many studies.
Despite these limitations, our main findings confirm that there are significant differences between racial and ethnic groups regarding their attitudes toward PAD. These differences are likely due to a complex array of variables, the most prominent of those examined being factors related to religion. While the impact of distrust in the health system has not been sufficiently studied, socioeconomic factors appear to play only a minor role. There seems to remain an independent association with race and ethnicity, particularly among Black Americans, which deserves further study. Such studies might include not only empirical questions, such as the role of trust in the health care system which has been relatively unexplored in relation to PAD, but also ethical questions about how such findings ought to inform policy debates on PAD.
Authors’ Contributions
All authors have read and approved the final version of the article. M.N.: Methodology, formal analysis, investigation, data curation, writing—original draft, writing—review and editing. C.S.: Methodology, formal analysis, investigation, data curation, writing—review and editing. K.S.J.: Writing—review and editing. S.Y.H.K.: Conceptualization, methodology, formal analysis, investigation, writing—review and editing, supervision.
Footnotes
Acknowledgments
The authors thank Talia Bernhard and EJ Jardas for early-stage assistance with preliminary title and abstract screening, and Alicia Livinski for support with database searches.
Author Disclosure Statement
The authors of the study have no potential conflicts of interest to declare with the research, authorship and publication of this article. The opinions expressed are the authors’ own and do not represent the views of the NIH, DHHS, or the U.S. government.
Funding Information
This work was funded by NIH Clinical Center Department of Bioethics. The funding body played no role in the design of the study and collection, analysis, interpretation of data, and in writing the article.
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.