
Abstract
Intensive care unit (ICU) mortality rates have substantially declined over the past few decades. Accordingly, there has been an increase in the number of ICU survivors, who are often burdened by long-term sequelae and high morbidity following their discharge. The term postintensive care syndrome (PICS) was first coined in 2012 to describe this constellation of physical, psychological, and cognitive sequelae, which may persist long after acute care hospitalization and may also affect family members. In this context, the timely integration and delivery of palliative care has the potential to alleviate the suffering experienced by both ICU survivors and their families. In this article, an interdisciplinary team presents ten tips to describe PICS and enhance the quality of care for palliative care clinicians caring for people with PICS.
Keywords
Introduction
Despite an increase in both patient age and illness severity at the time of intensive care unit (ICU) admission, ICU mortality rates have steadily declined over the past several decades. 1 Nevertheless, ICU patients often experience pain, immobility, loss of muscle and bone mass, weight loss, and exposure to a distressing environment. Thus, critical illness survivors are at high risk for adverse posthospitalization outcomes, such as reduced survival, impaired health-related quality of life, and significant physical, psychological, and cognitive impairments.2–5
The term postintensive care syndrome (PICS) was first coined in 2012 to describe a condition defined as “new or worsening problems in physical, cognitive, or mental health status arising after a critical illness and persisting beyond acute care hospitalization.” 6 Family caregivers of ICU survivors are similarly vulnerable to a form of PICS known as PICS-family (PICS-F), encompassing psychological and functional complications (e.g., anxiety, acute stress disorder, depression, complicated grief) resulting from their exposure to a loved one’s critical illness and ICU stay. 7 To date, few interventions have been demonstrated to treat or prevent PICS or PICS-F. 8 However, the integration of ICU survivorship clinics, management of physical and psychological suffering, and evaluation of spiritual, social, and caregivers’ needs may be beneficial. Additionally, palliative care interventions to address symptom burden, quality of life, and advance care planning may improve the post-ICU and posthospitalization course among ICU survivors. 8 This contribution, written by an interdisciplinary panel of expert ICU physicians, nurses, chaplains, social workers, and psychologists, provides palliative care teams with an overview of PICS and PICS-F to support ICU survivors and their caregivers after hospitalization (Table 1).
What Palliative Care Clinicians Should Know About Caring for People with Postintensive Care Syndrome
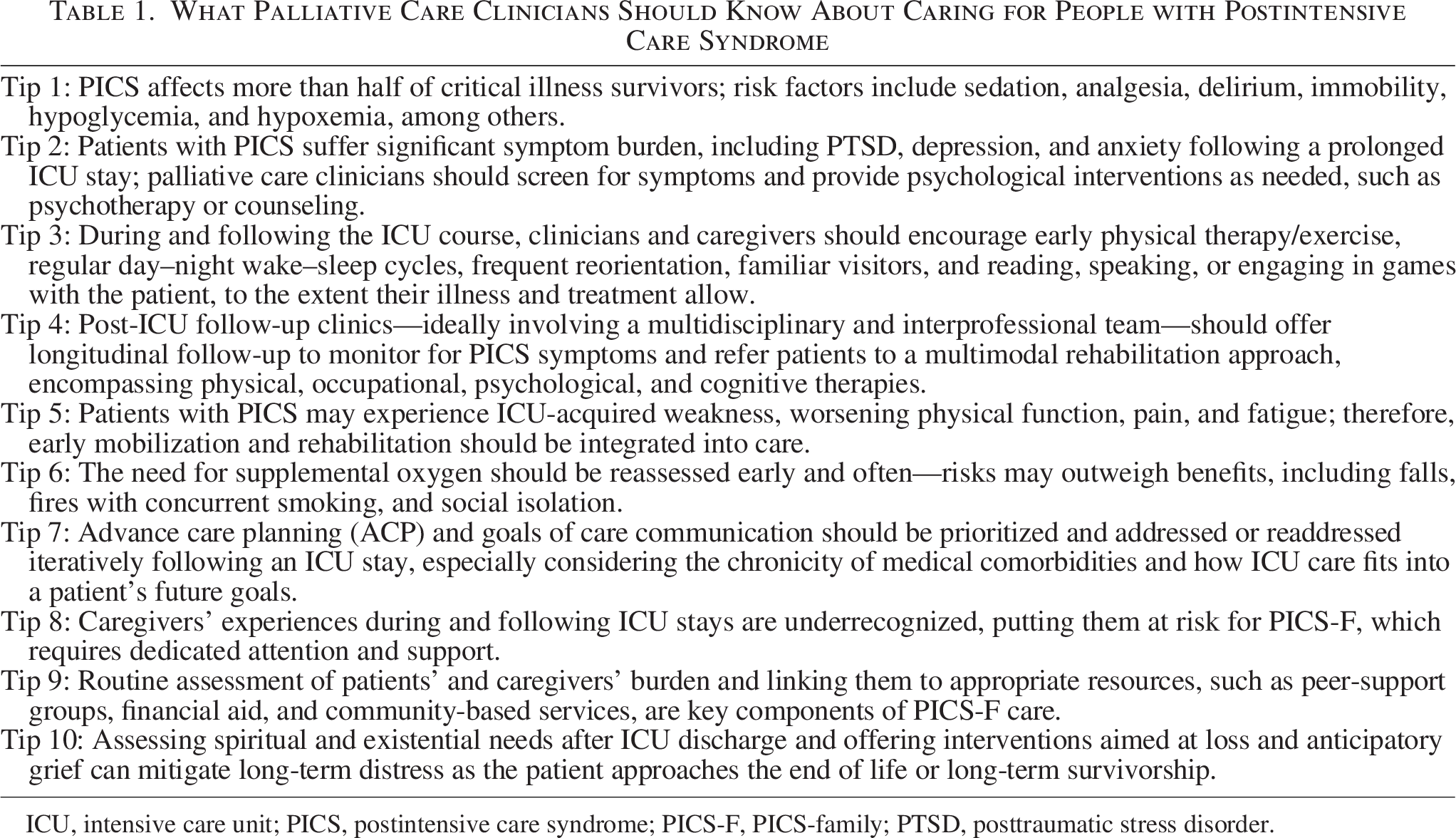
ICU, intensive care unit; PICS, postintensive care syndrome; PICS-F, PICS-family; PTSD, posttraumatic stress disorder.
Tip 1: PICS affects more than half of critical illness survivors; risk factors include sedation, analgesia, delirium, immobility, hypoglycemia, and hypoxemia, among others
PICS occurs in more than half of all critical illness survivors.5,9,10 Physical impairments frequently arise from critical illness myopathy and polyneuropathy, compounded by prolonged bed rest and immobility during ICU hospitalizations. 11 Additionally, patients frequently need sedation and analgesia to tolerate mechanical ventilation and offload the work of breathing, which may require neuromuscular blockade and exacerbate muscular atrophy.11,12 Poor nutrition, endocrine dysfunction, electrolyte abnormalities, and microvascular ischemia may also contribute to critical illness-associated weakness.5,11
Psychological impairments include depression, anxiety, and posttraumatic stress disorder (PTSD), as patients experience pain, discomfort, fear, disorientation, isolation, and dehumanization during their ICU hospitalization. 13 Women, those at a younger age, and those with a history of psychiatric illness, are at higher risk. Additionally, certain aspects of ICU care—for example, sedation, hypoglycemia, and hypoxemia—contribute to increased risk.14,15
Alongside physical and psychological impairments, lasting cognitive deficits may also occur, including impairments in memory, attention, and processing speech. Risk factors include preexisting cognitive dysfunction, frequent or prolonged hypoglycemia or hyperglycemia, hypoxemia, and ICU delirium.5,16
Tip 2: Patients with PICS suffer significant symptom burden, including PTSD, depression, and anxiety, following a prolonged ICU stay; palliative care clinicians should screen for symptoms and provide psychological interventions as needed, such as psychotherapy or counseling
Patients with PICS experience substantial and prolonged psychological symptoms—including PTSD, depression, and anxiety—that can affect daily function and quality of life for both themselves and their caregivers. While nearly half of ICU survivors experience lasting psychological symptoms, people with preexisting mental health conditions are at higher risk.9,17 There may also be an increased risk of self-harm and suicide among ICU survivors. 18 Notably, depression can initially present as a memory or attention deficit, while disordered sleep patterns, either predating an ICU stay or beginning during an ICU stay, can persist and worsen psychological comorbidity following ICU discharge. 19
Consequently, palliative care clinicians should assess ICU survivors for mental health conditions upon initial consultation and with each in-hospital and posthospital clinical encounter. If the palliative care clinician will not be following a patient longitudinally, the palliative care team should discuss the importance of mental health screening and care with the patient’s primary clinical team. Validated scales are available for use by any clinician.20–22
When PTSD, depression, and/or anxiety are identified, palliative care clinicians should discuss their impressions with the patient (and the caregiver, with patient permission) and immediately initiate or coordinate interventions such as pharmacotherapy and psychotherapy (e.g., cognitive-behavioral therapy, mindfulness, and exposure-based therapy) as appropriate and feasible for the patient.
In addition to identifying and addressing specific mental health diagnoses, a palliative care clinician can collaborate with interprofessional colleagues to support patient nutrition, sleep, stress reduction, and social relationships. For example, unemployment for the PICS survivor and financial strain for caregivers are common. 23 As part of stress reduction and to preserve social relationships, palliative care clinicians can engage a hospital or clinic social worker or case manager to help a patient navigate employment and financial instability following an ICU stay. 23
Palliative care clinicians can help patients and families reduce symptoms of posttraumatic stress, anxiety, and depression following an ICU stay by recommending in-ICU interventions, such as a caregiver keeping prospective diaries to help patients understand retrospectively what happened during their ICU stay. 24 During and after an ICU stay, palliative care clinicians can also connect patients with peer-support networks, educate them about their ICU stay and anticipated recovery process, validate personal experiences, and provide anticipatory guidance about PICS and associated mental health sequelae of ICU stays.
Tip 3: During and following the ICU course, clinicians and caregivers should encourage early physical therapy/exercise, regular day–night wake–sleep cycles, frequent reorientation, familiar visitors, and reading, speaking, or engaging in games with the patient to the extent their illness and treatment allow
ICU patients often experience circadian rhythm disruptions due to care timing, medications, organ dysfunction, and systemic stress. 25 This can lead to delirium, diminished immune function, and delayed recovery, as well as long-term sequelae, including PTSD and anxiety.26,27 Multiple evidence-based practices focused on reducing delirium and optimizing awareness and wakefulness in the ICU are available. Recommendations from the Society of Critical Care Medicine’s (SCCM) 2018 Guideline for the Prevention and Management of Pain, Agitation (Sedation), Delirium, Immobility and Sleep Disruption (PADIS Guidelines) highlight the value of a multicomponent nonpharmacologic strategy incorporating improved sleep–wake cycles and early mobilization that can be used to increase physical function and decrease delirium risk in critically ill adults. 28 Meta-analyses of early mobilization in particular suggest that it can also reduce ICU-associated weakness, shorten ICU and hospital lengths of stay, and improve functional status at discharge, therefore potentially alleviating the burden of physical symptoms associated with PICS. 29
Detailed reviews of early mobilization guidelines emphasize the need for staff and environmental assessment, as well as the implementation of structured mobilization processes. These guidelines also encourage engagement from a broad range of clinicians, including specialty consultants, patients, and visitors.30,31 New family-centered care guidelines published by the SCCM in 2025 specifically recommend caregiver engagement in bedside care. 32 This approach has also been demonstrated to improve caregiver satisfaction with ICU care, care quality, and decision-making. 33 In this regard, palliative care clinicians can facilitate early mobilization, sleep–wake optimization, and caregiver engagement through clinical recommendations, but also through their empowerment to actively participate in care.
Tip 4: Post-ICU follow-up clinics—ideally involving a multidisciplinary and interprofessional team—should offer longitudinal follow-up to monitor for PICS symptoms and refer patients to a multimodal rehabilitation approach, encompassing physical, occupational, psychological, and cognitive therapies
Clinical guidelines recommend post-ICU follow-up clinics as a key care delivery model for monitoring and addressing PICS.34,35 Clinics may address the issues of fragmented care, incomplete recovery, and the lack of recovery-specific resources following ICU discharge. 34 However, debate exists regarding whether ICU clinicians should be part of the follow-up team for survivors following discharge, and experts recommend that PICS should be treated by expert rehabilitation practitioners, including physiotherapy, nursing, medical, and psychology, among others. 35 Palliative care clinicians may be a logical choice for inclusion in these clinics, given the significant role they play in the ICU and in managing complex symptom burdens. However, their role in post-ICU clinics is understudied and currently limited to expert opinion.36,37
Despite the controversy of whether ICU clinicians should be involved in outpatient PICS care and a lack of evidence for PICS clinics from trials, 38 clinics continue to be developed and implemented across health systems. Their key features are summarized in Table 2. Historically, these clinics have been delivered in hospital settings; however, telehealth is an increasingly common mode of delivery to improve access. In trials, post-ICU care models that do not require in-person attendance have increased rates of recruitment, intervention delivery success, and participant retention when compared to hospital-based interventions. 42
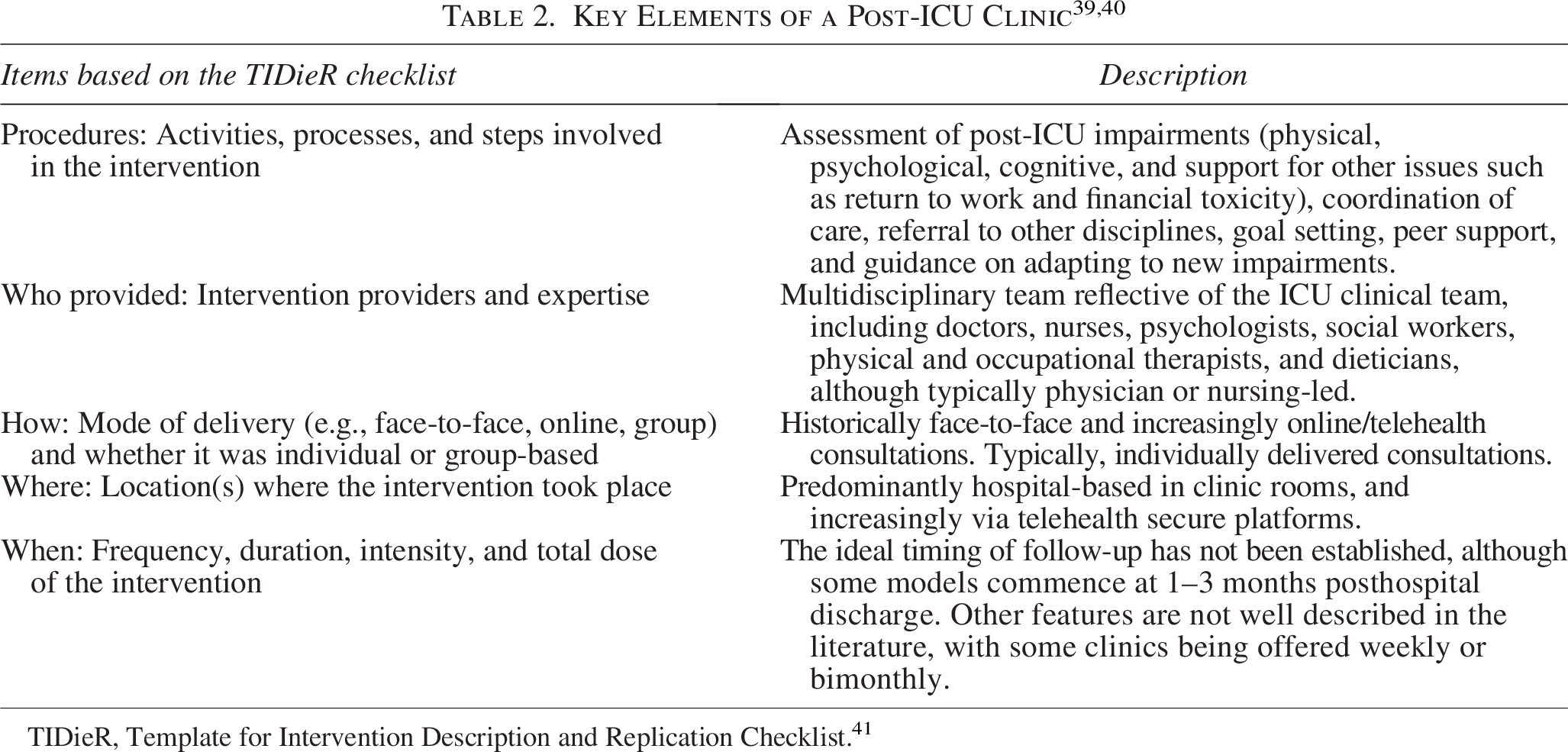
TIDieR, Template for Intervention Description and Replication Checklist. 41
Patients perceive both in-person and telehealth post-ICU follow-up clinics as contributing to their physical and emotional recovery through care continuity, information access, reassurance, normalization of recovery, and the opportunity to be referred to other specialists, when needed. 43 Similarly, clinicians working in follow-up clinics have reported greater awareness of post-ICU complications, thereby influencing their ICU practice. 44 Unfortunately, clinics are not widely available; however, a directory of U.S. clinics is available. 45
Tip 5: Patients with PICS may experience ICU-acquired weakness, worsening physical function, pain, and fatigue; therefore, early mobilization and rehabilitation should be integrated into care
ICU-acquired weakness affects up to 50% of patients who are critically ill 46 and is associated with poor physical function up to 2 years following discharge. 47 Additionally, the prevalence of pain and fatigue is estimated to be 50% 48 and 66%, 49 respectively, during the first year following critical illness. These impairments may co-occur with impaired physical function. Despite inconsistent evidence, early mobilization and rehabilitation may mitigate and/or prevent these PICS-related impairments.
In the early 2000s, studies evaluating early mobilization and rehabilitation began to emerge, with the first randomized clinical trial (RCT) published in 2009, comparing early rehabilitation to a “usual care” control group that did not receive rehabilitation while mechanically ventilated. 50 Given the positive results of this RCT, many institutions implemented early mobilization and rehabilitation programs. However, “usual care” has evolved since that time, now frequently including some form of rehabilitation. This has likely contributed to inconsistent findings reported in more recent studies surrounding the benefits of early mobilization and rehabilitation programs. 51
In 2018, the SCCM published the PADIS Guidelines, providing a “conditional recommendation” (as per Grading of Recommendations Assessment, Development, and Evaluation methodology) to perform rehabilitation or mobilization in critically ill adult patients. 28 More recently, the guidelines were updated to include enhanced mobilization and rehabilitation (i.e., anything more than a unit’s usual mobilization, including cycling or stepping, earlier interventions, more frequent interventions) over usual care. 52 In accordance with these guidelines, palliative care clinicians can play a role in promoting the early integration of mobilization and rehabilitation in patients’ care plans during the very early stages of their critical illness, coordinating the involvement of multiple specialists.
Tip 6: The need for supplemental oxygen should be reassessed early and often—risks may outweigh benefits, including falls, fires with concurrent smoking, and social isolation
ICU admissions for respiratory conditions are often associated with a requirement for supplemental oxygen at discharge. 53 While the prevalence of home oxygen therapy in the PICS population has not been clearly elucidated, the sequelae of critical illness, such as residual pulmonary fibrosis in acute respiratory distress syndrome (ARDS), new-onset cardiac failure with pulmonary congestion, and ICU-acquired muscle weakness, may precipitate the need for oxygen therapy in this population. 3 Patient-centric management of oxygen starts with clarifying the intention for its use. When management of underlying pulmonary and cardiac disorders is the goal, long-term oxygen therapy is the established approach for chronic hypoxemia (PaO2 ≤ 55 mmHg or SaO2 ≤ 88%) with the goal of improving survival. 54 Palliative oxygen therapy is targeted at treating dyspnea in patients, although its effectiveness is uncertain.55,56 When used for comfort, the primary goal should be symptom management, rather than targeting pulse oximetry readings.
In addition to disease and quality of life benefits in selected patients, home oxygen delivery is associated with certain risks. These include physical risks, such as burns, fires, or falls due to entanglement in tubing. Further, patients can experience negative social effects, including stigma associated with oxygen use and difficulty navigating crowds with portable tanks.57,58 The potential financial costs are also significant. As such, the American Board of Internal Medicine Foundation and Consumer Reports “Choosing Wisely Campaign” recommends that “for patients recently discharged on supplemental home oxygen following hospitalization, do not renew the prescription without assessing the patient for ongoing hypoxemia.” 59 This recommendation acknowledges that patients may improve after discharge and no longer require supplemental oxygen. Patients should be evaluated at rest and then with exertion via six-minute walk tests. If SaO2≤ 88% is not met, then discontinuation of supplemental oxygen among these patients is appropriate. 60
Tip 7: Advance care planning (ACP) and goals of care communication should be prioritized and addressed or readdressed iteratively following an ICU stay, especially considering the chronicity of medical comorbidities and how ICU care fits into a patient’s future goals
The presence of post-ICU symptoms and impairments in the PICS population obviates the need for ongoing conversations about medical decisions, goals of care, and the need for long-term therapies. Palliative care involvement can be crucial in addressing physical symptoms, providing interdisciplinary support for patients and families, and aligning care that is value-concordant as they transition through different care settings. 61
Patient priorities have been demonstrated to evolve over time: from basic survival while hospitalized to active physical recovery immediately after discharge, to more holistic and aspirational priorities following discharge. 62 In addition, patients and caregivers who have experienced suffering may have a new understanding or shifted perspective of what is most important to them based on their experiences. Therefore, iterative ACP conversations should be implemented throughout a patient’s clinical trajectory. 62
Given that PICS can persist well beyond someone’s ICU stay or hospitalization, it is crucial for patients and their caregivers to be connected with palliative care at discharge for continued support and ACP.
Tip 8: Caregivers’ experiences during and following ICU stays are underrecognized, putting them at risk for PICS-F, which requires dedicated attention and support
In addition to patients, PICS-F can present in caregivers following ICU stays. 7 Witnessing patient suffering, physical and cognitive changes, and often feeling powerless can contribute to caregiver distress that manifests as anxiety, depression, and PTSD. 63 Preexisting anxiety, depression, or PTSD, witnessing the patient’s death, or experiencing the death as traumatic or unexpected are risk factors for developing PICS-F. 7 Additional factors, including lack of communication, conflict of interactions between caregivers and ICU staff, and poor caregiver involvement in healthcare decision-making, are also associated with PICS-F. 7 As in other settings, an emerging body of literature highlights the detrimental impact of PICS on caregiver burden and overall well-being. 25 PICS-F may also be exacerbated by the additional stressors placed on caregivers when patients transition out of the ICU setting and prepare for eventual hospital discharge; indeed, caregivers are increasingly tasked with shouldering patient care responsibilities postdischarge that were once assumed by healthcare professionals, adding to their already significant logistic and financial burden, and further complicating PICS-F. To prevent and address PICS-F, palliative care clinicians should identify all caregivers, screen them for distress and unmet psychosocial needs, and connect them with appropriate support and care, ideally beginning while patients are still admitted to the ICU.
Tip 9: Routine assessment of patients’ and caregivers’ burden and linking them to appropriate resources, such as peer-support groups, financial aid, and community-based services, are key components of PICS-F care
The challenges PICS-F pose to ICU survivors and their caregivers underline the need for interdisciplinary management of both patients and caregivers. 64 Caregiver assessments should include emotional burdens and social determinants of health (SDOH). According to the World Health Organization, SDOH account for 30–55% of health outcomes. 65 An example of such screening is the Protocol for Responding to and Assessing Patient Assets, Risks, and Experiences, which includes assessment of food and housing insecurity, transportation and utility needs, and interpersonal safety. 66 SDOH screening can also support alignment among patients and care teams, thereby encouraging shared decision-making. 67
Inpatient and post-ICU support groups can connect caregivers with appropriate services while fostering dialogue about challenges that extend beyond hospital settings. As caregiver burden can affect sleep patterns and quality of life, group settings offer opportunities to decrease isolation and garner helpful information. Other modalities of post-ICU caregiver support include structured education programs, post-ICU clinic services and coordination, financial and employment referrals, and exploration of tools promoting self-care. 68 Caregivers also emphasize the importance of practical care, including staff attentiveness to immediate needs (e.g., water, food), physical space, and encouragement of rest.
There are various assessments available to staff supporting patients and their families as they navigate ICU care. The Zarit Burden Interview (12 items) offers a complete biopsychosocial assessment. 64 Utilization of a Family Information Leaflet has also been found to increase communication among families and care teams. 64 Self-assessment tools such as the Caregiver Self-Assessment Questionnaire may also be shared with families to assess their need for connection with primary care providers and/or community-based resources.
Tip 10: Assessing spiritual and existential needs after ICU discharge and offering interventions aimed at loss and anticipatory grief can mitigate long-term distress as the patient approaches the end of life or long-term survivorship
Survivors of critical illness frequently face profound existential and spiritual challenges, including disrupted identity, grief over lost abilities, and a search for meaning. A cross-sectional study of 196 ICU survivors found that over half reported spiritual distress, including feelings of abandonment by God or lack of support from their faith community. 69 These unmet spiritual needs were significantly associated with PICS-related symptoms such as anxiety, depression, and cognitive dysfunction. 69 Targeted spiritual-care interventions during hospitalization improved hope, life satisfaction, and reduced loneliness, underscoring the therapeutic value of chaplain engagement. 70 Likewise, post-ICU COVID-19 survivors described “trying to reconnect with a changed reality,” highlighting the long arc of existential disruption beyond discharge. 71
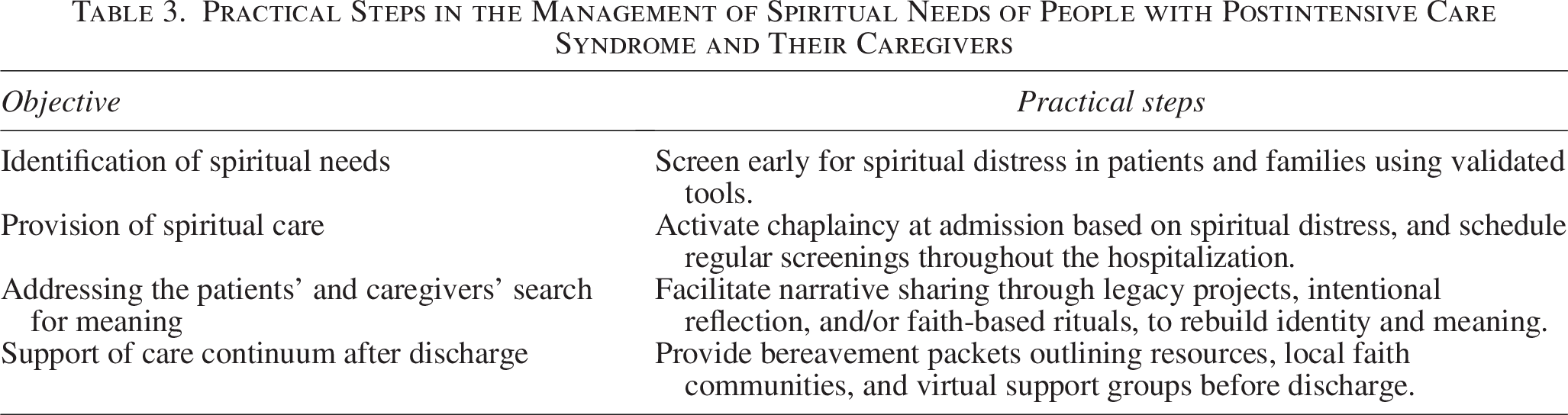
Caregivers share this burden. Anticipatory bereavement support, including structured meetings, consistent emotional check-ins, and clear information, mitigates later anxiety, depression, and prolonged grief.72–74 Embedding chaplains in the ICU team amplifies these gains; an RCT showed proactive chaplain visits lowered surrogate anxiety and raised spiritual well-being. 75 Studies demonstrate that sustained chaplain follow-up fosters healthier adjustment for caregivers after death or difficult recoveries. 75 Table 3 presents practical steps that can be implemented by palliative care clinicians to ease spiritual suffering, support healthier grieving, and promote resilience during vulnerable care transitions.
Practical Steps in the Management of Spiritual Needs of People with Postintensive Care Syndrome and Their Caregivers
Conclusion
Patients with PICS are burdened by a wide range of physical, psychological, and cognitive impairments and may experience significant concomitant social and spiritual suffering long after their ICU stay. Current evidence highlights a complex interplay between PICS, preexisting vulnerabilities, and SDOH. Caregivers may similarly be affected and experience PICS-F, with significant social, spiritual, and psychological sequelae. Recognizing and treating PICS and PICS-F with a comprehensive, interdisciplinary approach is essential and should begin early in the ICU, continuing throughout the patient’s care continuum. Integration of palliative care can support this process through the coordination and implementation of early mobilization, structured follow-up sessions, provision of psychological support, symptom management, spiritual care, and clear communication about the goals of care. These measures can alleviate suffering and promote recovery. As our awareness of PICS and PICS-F deepens, so must our commitment to informed and longitudinal palliative care for both ICU survivors and their caregivers.
Footnotes
Author Disclosure Statement
A.J.A. reports relationships with PsyOnc Partners, LLC, and Genmab. All other authors declare they have no competing interests.
Funding Information
B.T. receives research funding from the C.G. Swebilius Foundation.