
Abstract
Background:
Palliative care patients often experience sarcopenia, which can cause overestimation of kidney function by creatinine-based estimated glomerular filtration rate (eGFR) and inappropriate drug dosing. Data on cystatin C (CysC) use are scarce.
Objectives:
To examine intra-individual differences between creatinine- and CysC–based eGFR in palliative patients and assess the frequency of renally eliminated drugs prescribed.
Design:
Retrospective, single-center cohort study.
Setting/Subjects:
All patients admitted in 2023 to the palliative care unit of the University Hospital Zurich, Switzerland. Of 206 patients, 178 had eGFR data, and 144 with consent were included.
Measurements:
Data including creatinine, CysC, and prescribed medications were extracted from electronic records. eGFR was calculated using Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) 2009 (creatinine) and CKD-EPI 2012 (CysC, combined). Intraindividual discrepancies >15 mL/min/1.73m2 were defined as clinically relevant.
Results:
Paired values were available for 85 patients; 53% showed clinically relevant discrepancies (median 17 mL/min/1.73m2). In 22% of patients the discrepancy exceeded 30 mL/min/1.73m2. Diabetes was the only factor associated with differences. Acute kidney injury (AKI) occurred in 32% and was strongly linked to mortality, whereas discrepancies were not. Patients received a median of 19 drugs; of the 20 most frequently prescribed, 7 were renally eliminated. Over one-third with relevant discrepancies received two such drugs.
Conclusions:
Clinically relevant eGFR discrepancies are common in palliative care patients and may cause misclassification and dosing errors. CysC testing should be used selectively when prescribing renally eliminated drugs with toxicity risk, underscoring the need for individualized prescribing and prospective validation.
Keywords
Key Message
In this cohort, more than half of palliative care patients showed clinically relevant discrepancies between creatinine- and cystatin C (CysC)-based eGFR, risking kidney function misclassification and medication dosing errors. Selective CysC testing before prescribing renally eliminated drugs may improve safety and support individualized prescribing in this vulnerable population.
Introduction
Palliative care patients typically suffer from chronic illnesses associated with progressive muscle loss. Cachexia is a multifactorial syndrome of ongoing muscle wasting, with reported prevalence rates ranging from 5 to 15% in chronic heart failure or chronic obstructive pulmonary disease to 60–80% in patients with advanced cancer.1–3
Reduced muscle mass may lead to overestimation of clearance by creatinine-based estimated glomerular filtration rate (eGFR) equations, leading to drug dosage errors. Accurate dosing is crucial in this vulnerable group to avoid adverse effects or shortened survival.
Glomerular filtration rate (GFR) is generally recognized as the best marker of kidney function. Together with albuminuria and urine sediment, it assesses kidney dysfunction and progression of kidney disease. A GFR <60 mL/min/1.73m2 is associated with increased risk of kidney failure and mortality. 4 Impaired kidney function also affects the efficacy and safety of renally metabolized and excreted drugs; therefore, GFR is essential for drug dosage adjustment. Otherwise, altered pharmacodynamics and pharmacokinetics in reduced kidney function may cause toxicity, for example, accumulation of morphine metabolites.5,6 GFR reflects plasma volume cleared of a substance per unit time. Inulin is considered an ideal marker to estimate GFR, but too laborious for routine use. Thus, endogenous markers creatinine and CysC are more commonly used, even though their levels are influenced by endogenous production, tubular secretion and reabsorption, and extrarenal elimination. Hence, GFR estimation formulas (estimated GFR, eGFR) combine them with variables such as sex, age, or body size.
Creatinine production directly depends on muscle mass. Its levels can also depend on protein intake and certain medications that influence creatinine metabolism (e.g., trimethoprim, dronedarone).7,8
CysC is produced by all nucleated cells, freely filtered by the glomeruli, and not significantly reabsorbed. Unlike creatinine, it is less affected by muscle mass, sex, or diet. However, hyperthyroidism, inflammation, smoking, or glucocorticoids may raise CysC-based estimates of GFR, while hypothyroidism may lower them.9–11 Depending on the formula used, intra-individual discrepancies in GFR estimation can occur. In one study, patients whose Cockcroft-Gault-based eGFR indicated a higher carboplatin dose than the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) eGFR were at significantly higher risk of grade 2 adverse events and chemotherapy discontinuation. 12 Kidney Disease: Improving Global Outcomes (KDIGO) 2024 guidelines recommend creatinine-based eGFR (eGFRcr) first. 13 If accuracy is doubtful (e.g., due to low muscle mass) or precise values are needed, combined creatinine–CysC equations (eGFRcr+cys) for GFR estimation are advised. This study aimed to investigate clinically relevant differences in creatinine- versus CysC-based eGFR (eGFRcys) in a palliative cohort. Additionally, the study aimed to identify frequently prescribed active substances during inpatient palliative care and to determine how often these substances are primarily eliminated by the kidneys.
Methods
Setting and participants
We conducted a retrospective, single-center analysis of all patients admitted to the palliative care unit of the University Hospital Zurich (Switzerland) in 2023. Patients admitted were not limited to those in a terminal stage. When appropriate, they may have continued receiving disease- or cancer-directed therapies as part of early palliative care integration. Of 206 patients, 178 had eGFR data. Records of these 178 patients were screened, and 144 with documented general consent were included. Consent was recorded as written general consent in the hospital’s electronic health system and covered within Ethics approval for registry and data use. The study was conducted in accordance with the Declaration of Helsinki and applicable regulatory requirements and was approved by the Local Ethics Board of the Canton of Zurich (BASEC No.2019–02488).
Definition and data collection
Sociodemographic data, comorbidities, medications, and laboratory values were extracted from hospital electronic health records. Additional variables included length of hospital stay, referral and discharge location (or place of death), underlying disease, body mass index (BMI), Karnofsky Performance Index (KPS; 100% = no symptoms, 0% = death), prescribed medications, and selected labs (serum creatinine, serum CysC, eGFRcr, eGFRcys, combined eGFRcr+cys, thyroid hormones [TSH, fT3, and fT4], and C-reactive protein [CRP]) wherever available.
eGFR
Patients were included if CysC had been measured either during the inpatient stay on the palliative care ward or any referring ward during the same hospitalization. In each case, the first CysC value obtained after admission to the palliative care unit was used, or, if unavailable, the most recent value measured on the referring ward prior to transfer to the palliative care unit. On average, blood sampling for CysC was performed on the third day after admission/transfer to the palliative care ward (mean = 2.6 days). If an eGFRcys measurement was available, the corresponding eGFRcr had to originate from the same blood draw. At our institution, the eGFRcr is calculated with the CKD-EPI 2009 equation; cystatin C-based eGFR (eGFRcys) and combined eGFRcr+cys with the CKD-EPI 2012 equations. All three formulas are reported in mL/min/1.73m2. We defined an absolute intra-individual difference between eGFRcr and eGFRcys of >+15 mL/min/1.73m2 as a clinically relevant discrepancy. This cut-off was chosen in part due to clinical considerations, as chronic kidney disease is also staged in 15 mL/min/1.73m2 increments according to KDIGO. 13 This stratification is commonly used for kidney-adapted medication dosing and is based on mean differences reported in previous studies.14,15 Acute kidney injury (AKI) was defined using KDIGO criteria: stage 1 = creatinine 1.5–1.9× baseline, stage 2 = 2.0–2.9×, stage 3 = ≥3.0× or renal replacement therapy. 16 The most recent creatinine from prior hospital stays or outpatient visits was used as baseline. Reference ranges for TSH, fT3, and fT4 were based on institution-specific cut-offs: 0.3–3.18 mU/L for TSH; 4.1–6.7 pmol/L for fT3; and 13.1–21.3 pmol/L for fT4 (or 3.6–6.4 pmol/L and 12.0–20.2 pmol/L, respectively, for female patients).
Because intake of more than 10 mg of prednisolone (PDN) per day (or approximately 0.17 mg/kg/day) may distort cystatin C-based GFR estimates (GFRcys), individuals receiving >10 mg of PDN equivalents per day were categorized as being on systemic steroid therapy.17,18
Medications
All substances prescribed and administered at least once during the hospital stay were recorded. Drugs prescribed as both regular and on-demand were counted once. To determine whether a drug was primarily renally eliminated, various pharmacological reference sources were consulted.19,20 The Q0 value represents the fraction of a drug that is eliminated extrarenally. The lower the Q0 value, the higher the renal excretion. 21 Substances with Q0 <0.7 are considered primarily renally eliminated. 22 Dose adjustment according to renal function becomes particularly important when the extrarenal elimination fraction (Q0) is <0.5.20,21 Q0 values of active metabolites may differ from parent compounds. For example, morphine undergoes only ∼10% renal excretion, but its metabolite morphine-6-glucuronide (M6G) has a Q0 <0.3. 23 The 20 most frequently prescribed medications administered to patients during their hospital stay are summarized in Table 5. Only systemically absorbed medications were included; local drugs and those not given enterally or parenterally were excluded, except for transdermal fentanyl.
Statistical analysis
eGFR
Depending on data distribution, continuous variables were summarized as medians with interquartile ranges or means with standard deviations. For categorical data, counts and percentages were used. Intraindividual differences between eGFRcr and eGFRcys were visualized with a waterfall plot. A Friedman rank sum test compared the three within-subject GFR estimation methods (eGFRCr, eGFRCys, eGFRcr+cys) in patients with and without AKI. For subgroup comparisons (steroid vs. no steroid), the Wilcoxon rank-sum test was applied for continuous variables and Fisher’s exact test for categorical data. When more than two groups were compared, statistical tests were selected based on the distribution of the data: ANOVA was used for normally distributed continuous variables, and the Kruskal–Wallis test for nonnormally distributed continuous variables. Categorical variables were analyzed using Fisher’s exact test. The significance level was set at 0.05.
Linear regression
Associations between eGFR and clinical variables were investigated using simple linear regressions. Model assumptions (linearity, normality of residuals, and homoscedasticity) were checked using residual plots, Q–Q plots, Shapiro-Wilk, and Breusch-Pagan tests. Where appropriate, log transformation was applied to improve model fit. Regression coefficients (β), 95% confidence intervals, and p-values were reported. For continuous variables, β reflects the change in eGFR per unit increase. For categorical variables β reflects the mean difference in eGFR compared to the reference category.
Survival
Survival was assessed from the date of CysC measurement to death on the palliative care ward. To avoid immortal time bias, the measurement date was used as time zero instead of the admission date. Of the 85 patients with available CysC measurements, 6 patients were excluded on this basis. A total of 79 patients were included in the final survival and Cox regression analyses. To evaluate whether mortality differed according to the degree of discordance between GFR estimates based on serum creatinine and CysC, patients were categorized into three groups based on the absolute difference between GFRcr and GFRcys (Group 1: GFRcr-GFRcys ≤ ± 15 mL/min/1.73m2, Group2: GFRcr-GFRcys 16–30 mL/min/1.73m2, Group3: GFRcr-GFRcys >30 mL/min/1.73m2). Subsequently, the association between AKI severity and survival was assessed. Patients were grouped into four AKI stages according to serum creatinine changes: no AKI (<1.5 times baseline creatinine), AKI 1 (1.5–1.9 times baseline creatinine), AKI 2 (2–2.9 times baseline creatinine), AKI 3 (≥3.0 times baseline creatinine). Kaplan–Meier survival curves visualized survival across the analyzed groups, and the log-rank assessed statistical differences between them. A univariable Cox proportional hazards model estimated associations with mortality, reporting hazard ratios (HRs) and 95% confidence intervals (CIs). Analyses were conducted using R Studio Version 2024. 12.0 + 467 (2024 Posit software, PBC).
Results
Patient characteristics
The median stay in the palliative care unit was 13 days (IQR 8–17). Most patients were transferred from another ward within the same hospital (60%, n = 51), followed by admissions from home (33%, n = 28) and the emergency department (4%, n = 3). In total, 45 patients (53%) died during their stay, 22 (26%) were discharged home, 7 (8%) were transferred to a nursing home, and six (7%) to a hospice. Patient demographics and clinical characteristics at baseline are detailed in Table 1.
Demographics and Clinical Characteristics (Group Comparison Based on eGFR Discordance eGFRcr-eGFRcys)
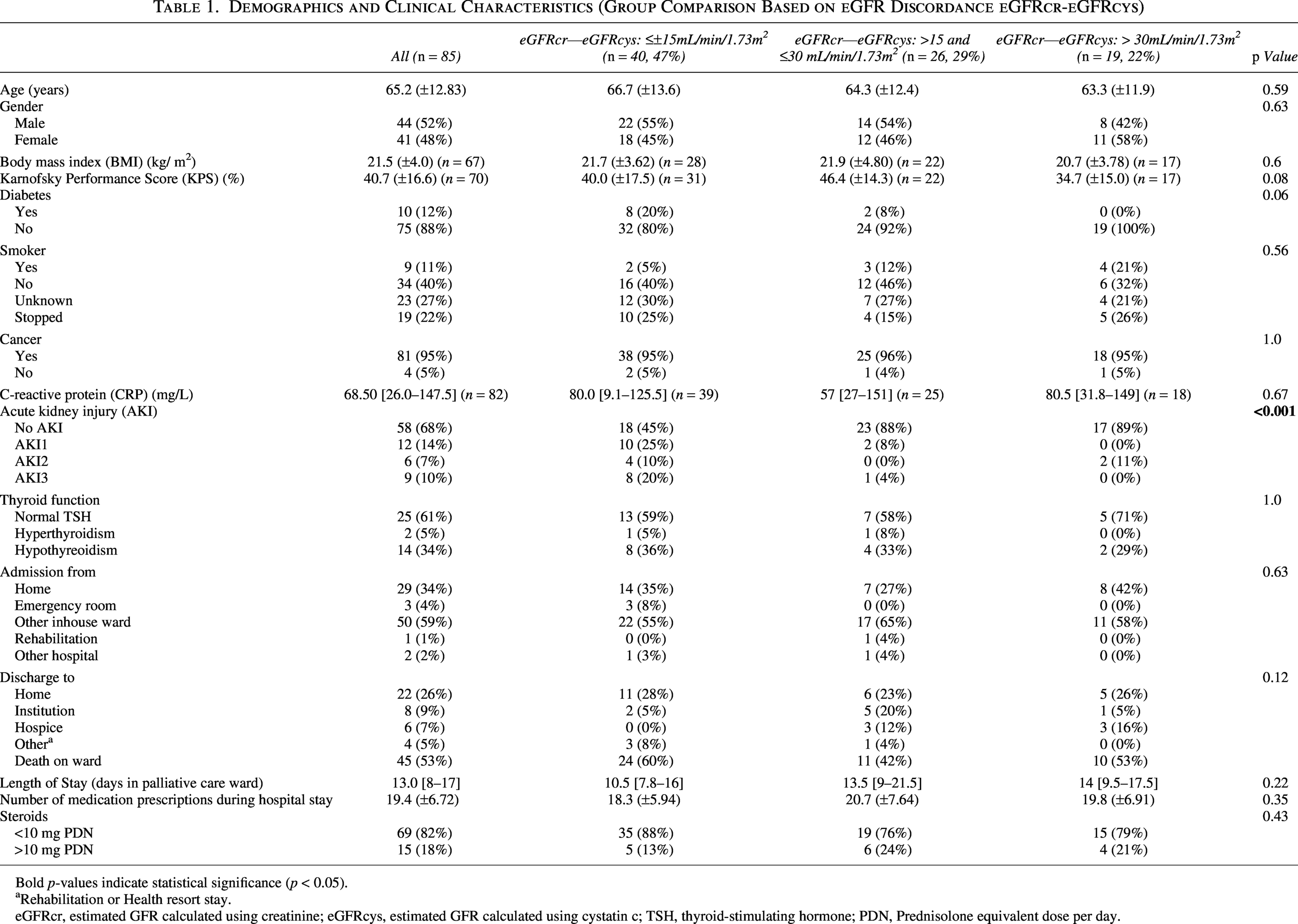
Bold p-values indicate statistical significance (p < 0.05).
Rehabilitation or Health resort stay.
eGFRcr, estimated GFR calculated using creatinine; eGFRcys, estimated GFR calculated using cystatin c; TSH, thyroid-stimulating hormone; PDN, Prednisolone equivalent dose per day.
eGFR
Corresponding eGFRcr and eGFRcys values were available for 85 out of 144 patients. Relevant discrepancies between creatinine- and cystatin C-based eGFR occurred in more than half of patients (n = 45, 53%), with a median intra-individual difference of 17 mL/min/1.73m2 (IQR 7–29). In nearly one-third of patients (29%), eGFRcys was more than 15 mL/min/1.73m2 lower than eGFRcr, and in 22% the difference exceeded 30 mL/min/1.73m2. A waterfall plot illustrates these intra-individual differences (Fig. 1). Medians of eGFRcr, eGFRcys and combined eGFRcr+cys differed significantly from one another (81 mL/min/1.73m2 [46–97], 51 mL/min/1.73m2 [28–73], and 63 mL/min/1.73m2 [36.5–87]; p = < 0.001). Potential confounders reported in the literature to affect eGFRcys (thyroid function, steroid use, and inflammation) did not lead to significant differences in median eGFRcys estimates in our cohort (Table 2).
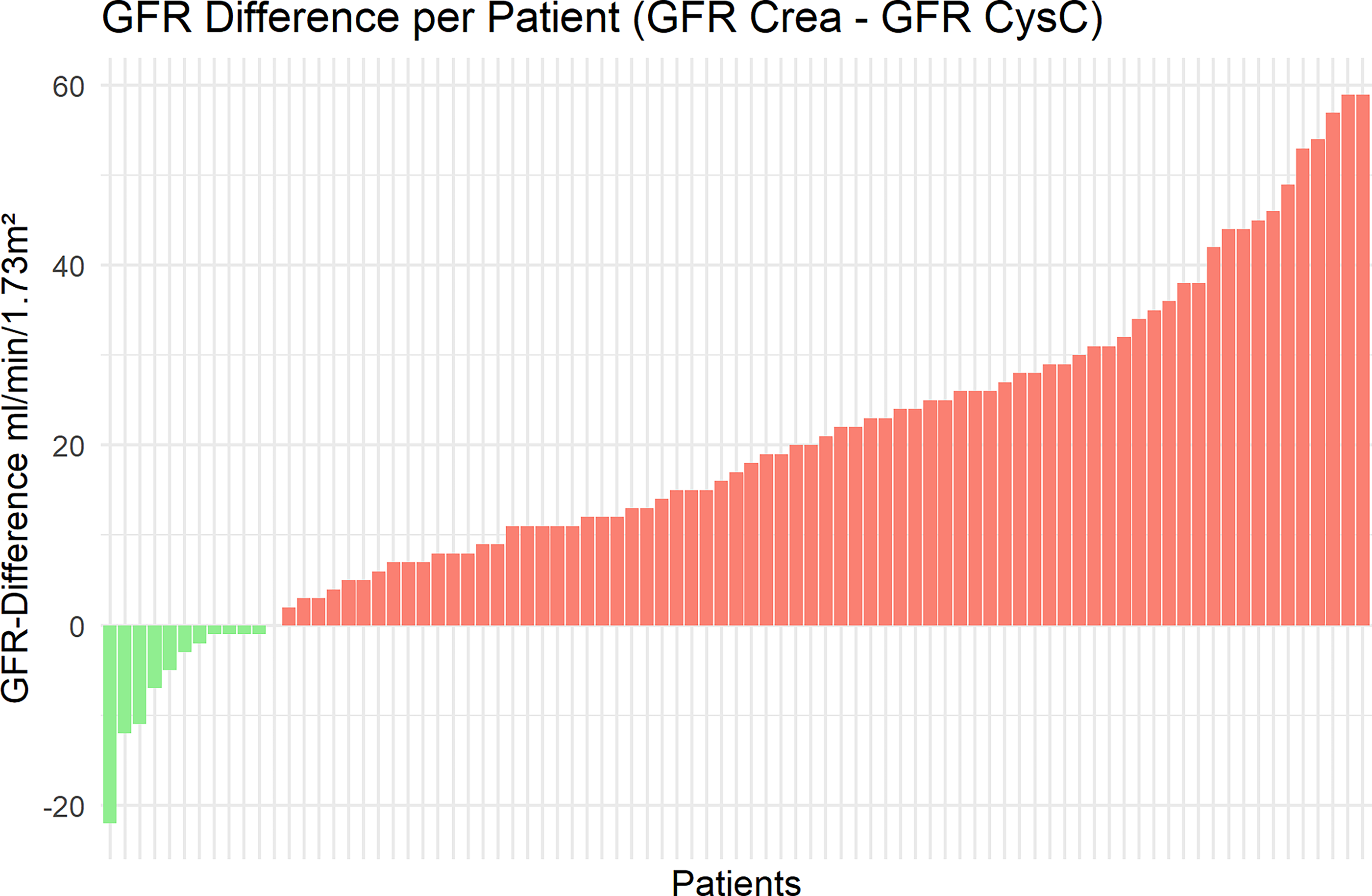
Waterfall plot of intra-individual differences between creatinine- and cystatin C-based estimated glomerular filtration rate (eGFR). Waterfall plot showing absolute differences between eGFR calculated using creatinine (eGFRcr) and cystatin C (eGFRcys) in individual patients. Positive values indicate higher eGFRcr compared with eGFRcys.
Subgroups With and Without Steroid Treatment: mL/Min/1.73m² [Interquartile Range], n (%)
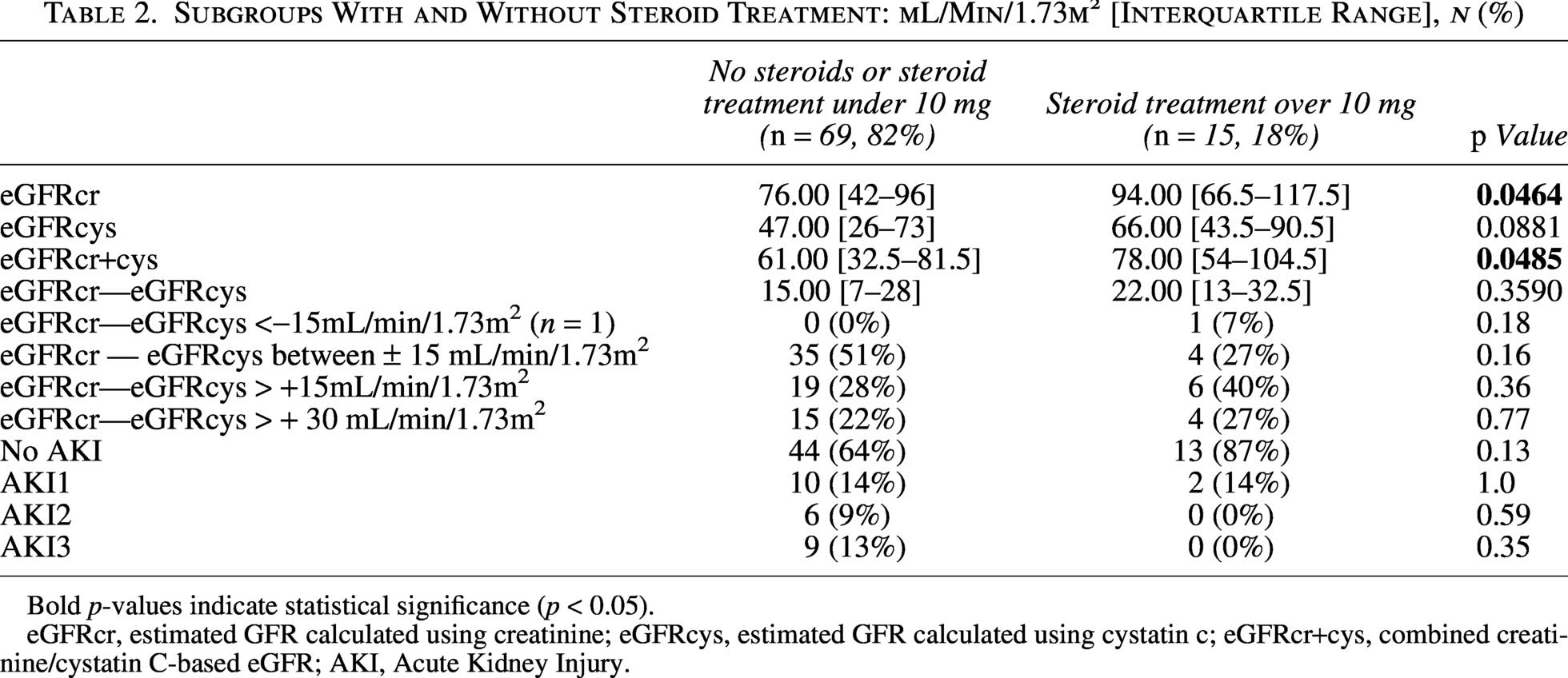
Bold p-values indicate statistical significance (p < 0.05).
eGFRcr, estimated GFR calculated using creatinine; eGFRcys, estimated GFR calculated using cystatin c; eGFRcr+cys, combined creatinine/cystatin C-based eGFR; AKI, Acute Kidney Injury.
Among examined predictors, age and steroid use showed linear associations with eGFR across all formulas. The β1 coefficient represents the average change in eGFR (mL/min/1.73m2) per one-unit increase in the respective variable. Accordingly, age was negatively associated with eGFR, irrespective of the equation used, while steroid use showed a positive association. Elevated BMI and diabetes were related to decreased eGFRcr, whereas smoking was associated with increased values. Among all variables examined, only diabetes impacted GFR discordance (eGFRcr-eGFRcys) significantly. (Table 3).
Linear Models Examining the Influence of Explanatory Variables on Different eGFR Estimation Methods
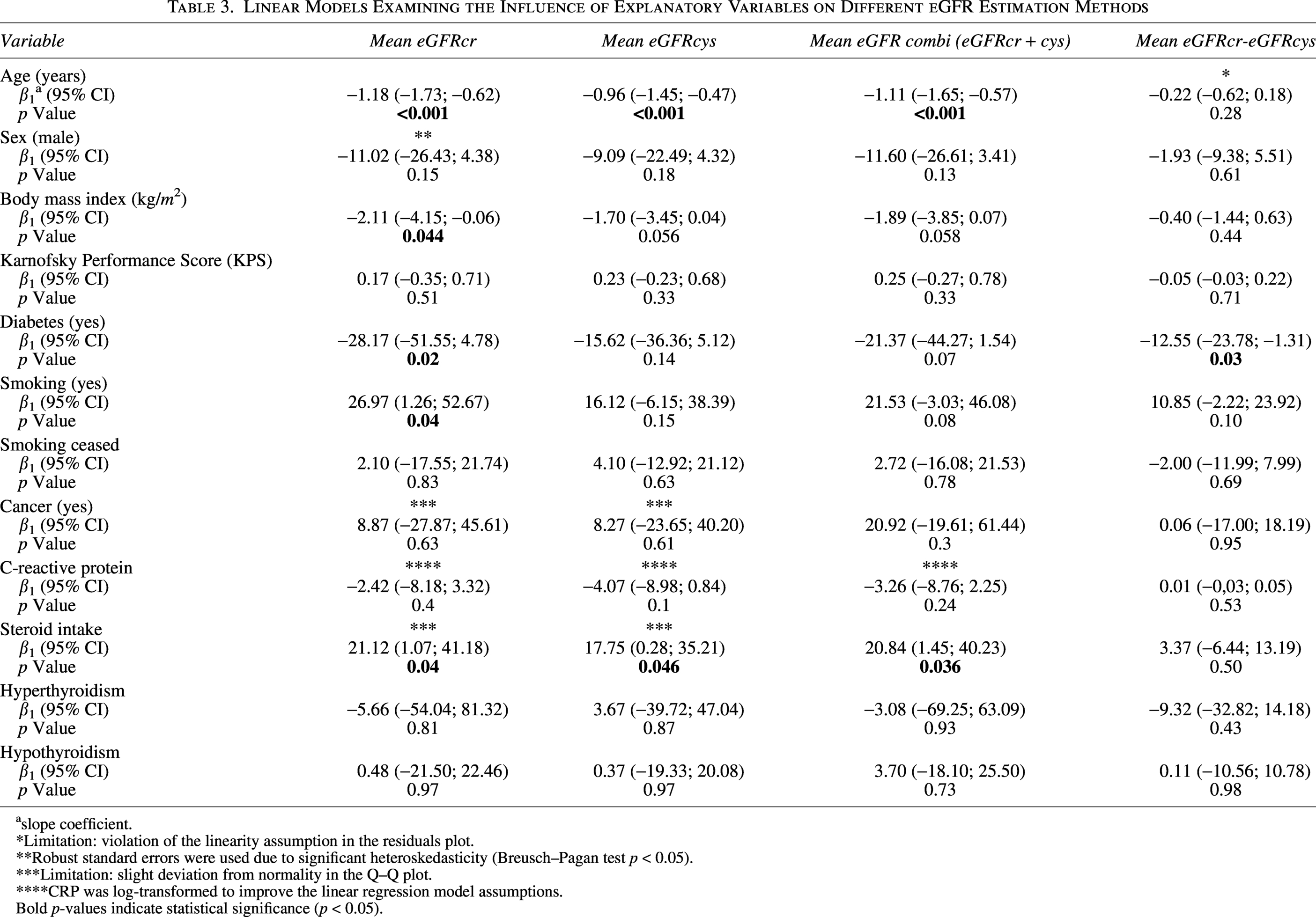
slope coefficient.
*Limitation: violation of the linearity assumption in the residuals plot.
**Robust standard errors were used due to significant heteroskedasticity (Breusch–Pagan test p < 0.05).
***Limitation: slight deviation from normality in the Q–Q plot.
****CRP was log-transformed to improve the linear regression model assumptions.
Bold p-values indicate statistical significance (p < 0.05).
AKI
Almost one-third of the population (n = 27, 32%) experienced AKI, mostly classified as AKI 1 (n =12, 14%) (Table 4). The largest median difference between eGFRcr and eGFRcys in patients with AKI occurred in the stage 1 subgroup (8.5 mL/min/1.73m2, IQR 7.5–12), followed by AKI stage 2 (8 mL/min/1.73m2, IQR 4.2–34.2), and AKI stage 3 (2 mL/min/1.73m2, IQR 1 to 11). Patients without a significant discrepancy between eGFRcr and eGFRcys exhibited more severe forms of AKI compared to those with intra-individual differences of >15 mL/min/1.73m2 or > 30 mL/min/1.73m2. No differences were found between the groups regarding sociodemographic parameters or underlying diseases.
Intra-Individual GFR Differences Depending on the Estimation Method in Patients with Acute Kidney Injury
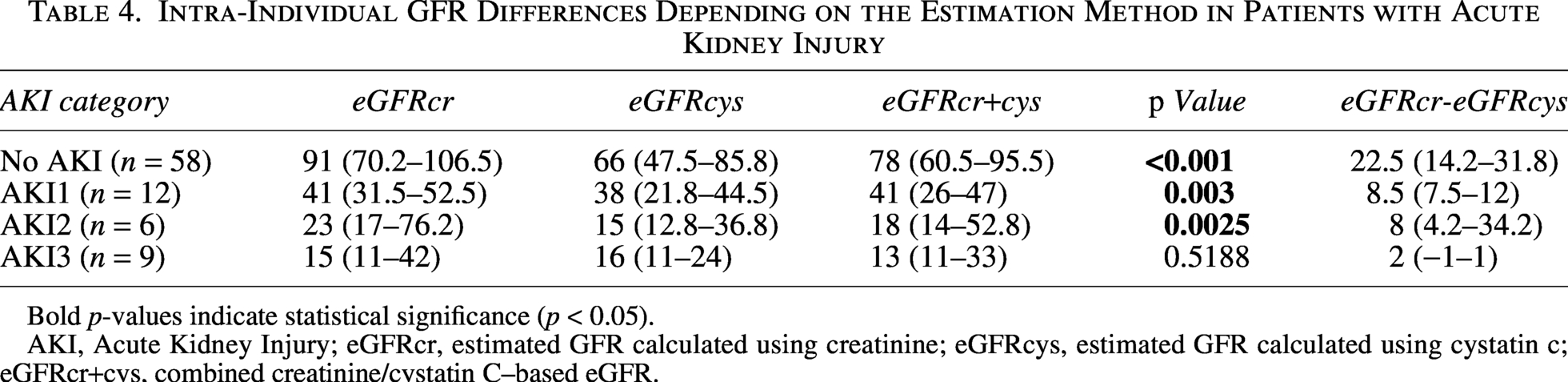
Bold p-values indicate statistical significance (p < 0.05).
AKI, Acute Kidney Injury; eGFRcr, estimated GFR calculated using creatinine; eGFRcys, estimated GFR calculated using cystatin c; eGFRcr+cys, combined creatinine/cystatin C–based eGFR.
Most Used Drugs
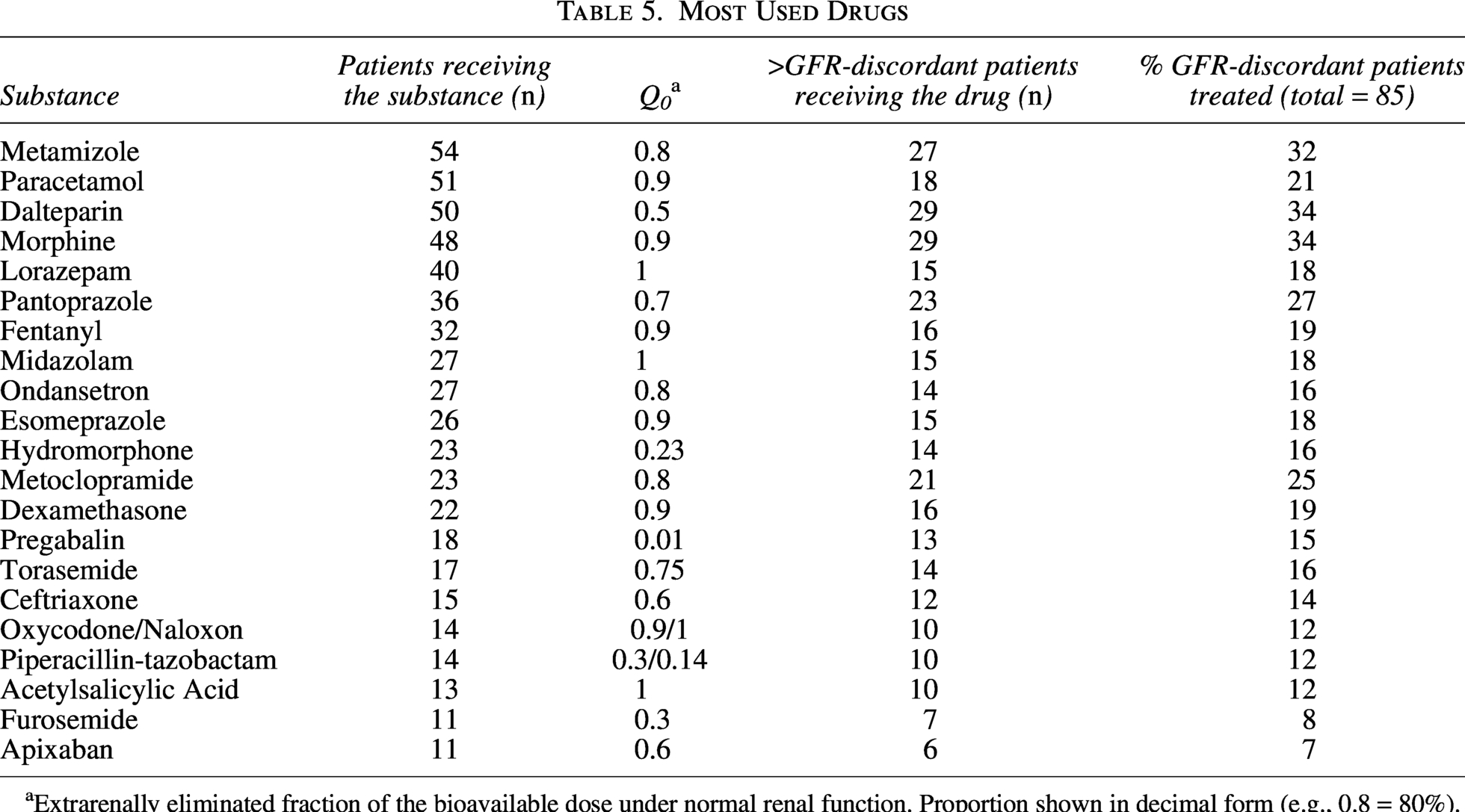
Extrarenally eliminated fraction of the bioavailable dose under normal renal function. Proportion shown in decimal form (e.g., 0.8 = 80%).
Survival
An intra-individual eGFR discrepancy had no significant effect on survival (p = 0.4) (Fig. 2). In contrast, AKI significantly affected survival (p = 0.001) (Fig. 3). Compared to the reference group without AKI, patients with AKI stages 2 and 3 had a significantly increased risk of death (HR 3.60 [95% CI: 1.23–10.5], p = 0.019; and HR 3.89 [95% CI: 1.73–8.76], p = 0.001, respectively).
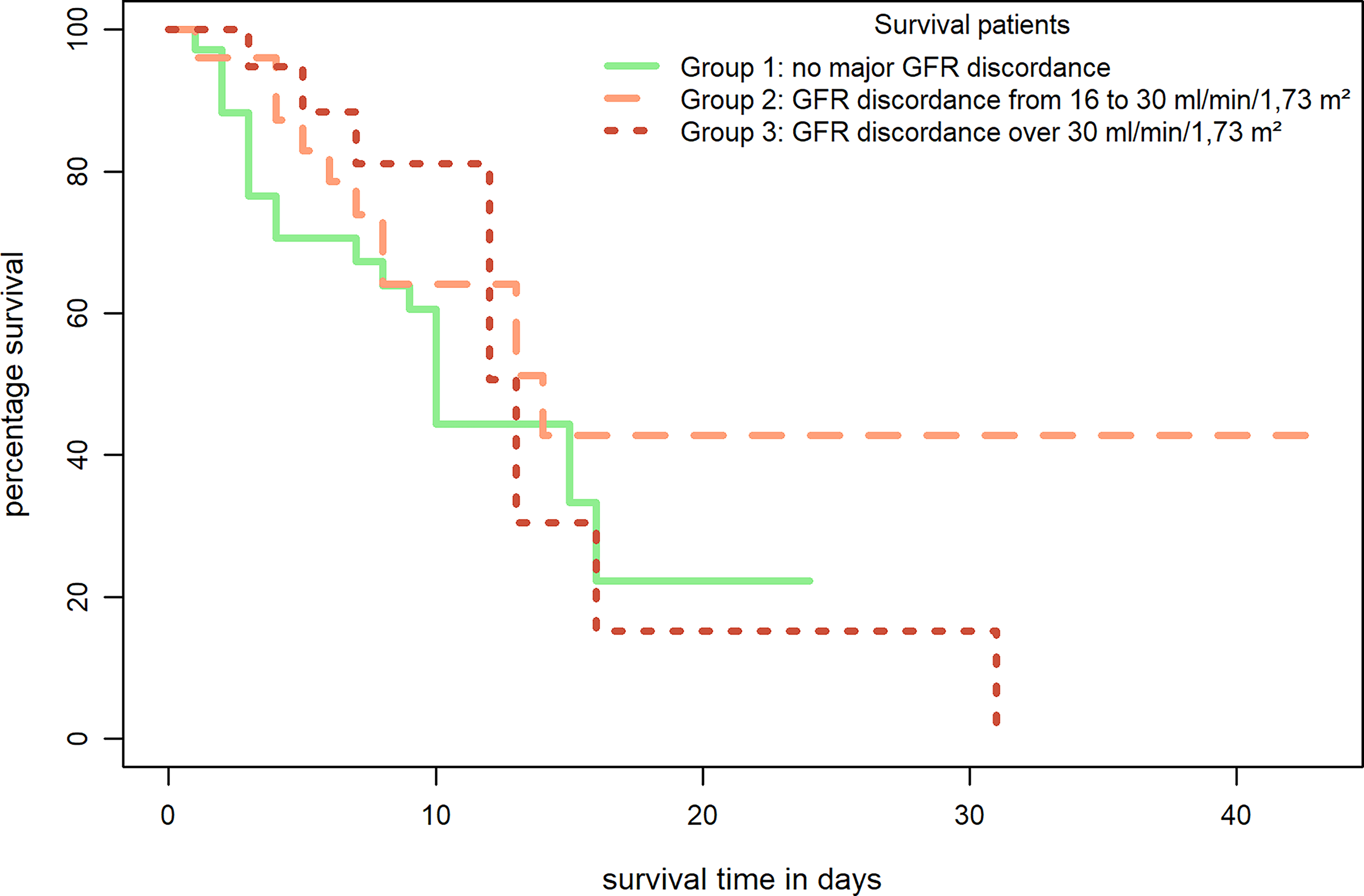
Survival according to eGFR discordance between creatinine- and cystatin C-based estimates. Kaplan-Meier survival curves stratified by the absolute difference between eGFRcr and eGFRcys (<±15, 16–30, and >30 mL/min/1.73 m²). No significant differences in survival were observed between groups (log-rank test).
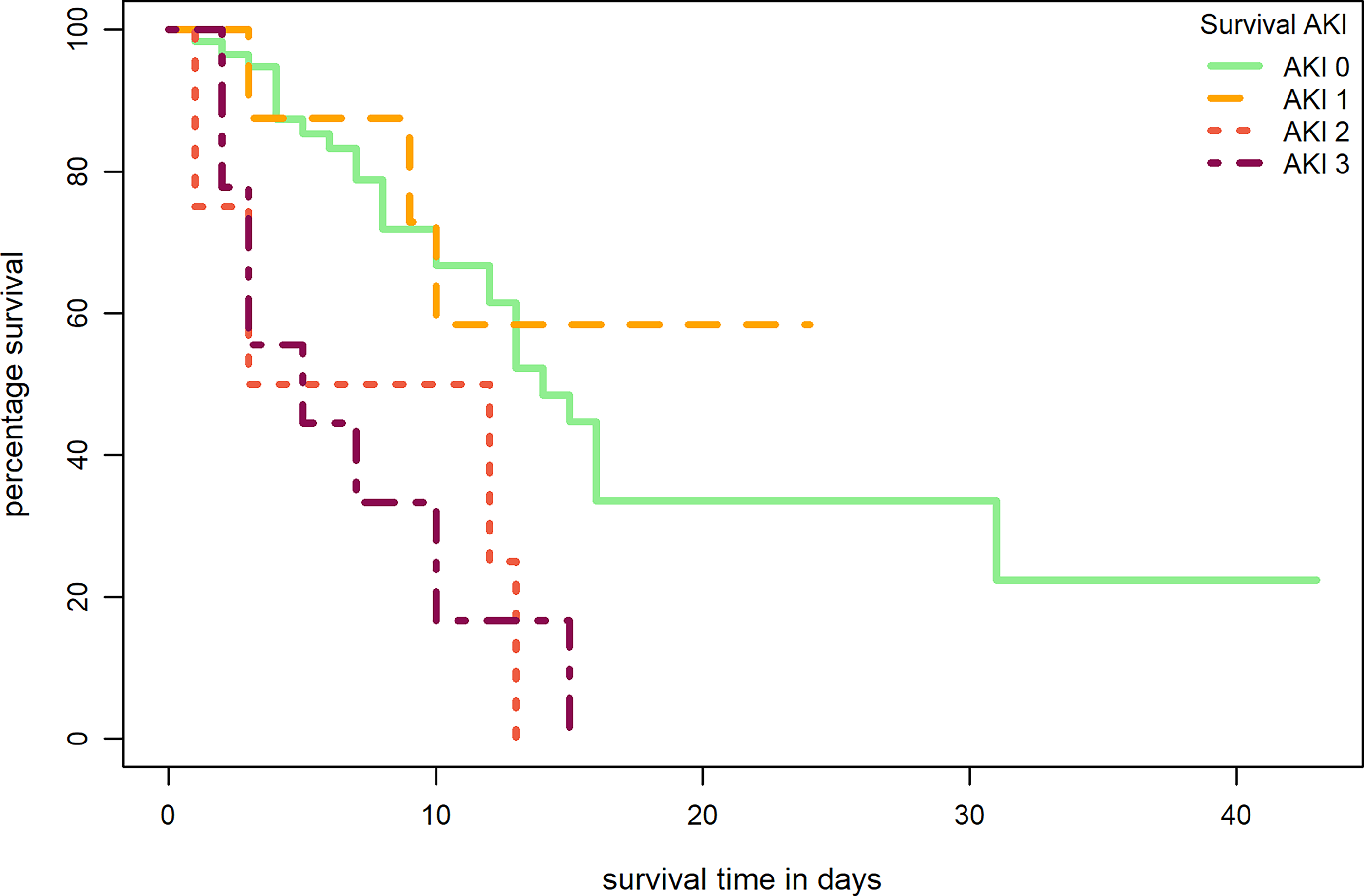
Survival according to acute kidney injury (AKI) stage. Kaplan-Meier survival curves comparing patients without AKI and those with AKI stages 1–3. Compared to the reference group without AKI, patients with AKI stages 2 and 3 had a significantly increased risk of death.
Drug interaction
On average, each patient received 19 different medications during hospitalization (Table 1). In total, 2704 prescriptions were recorded. The 20 most frequently prescribed drugs are listed in Table 5; 7 are significantly renally eliminated (Q0 < 0.7): Dalteparin, hydromorphone, pregabalin, ceftriaxone, piperacillin-tazobactam, furosemide, and apixaban. Analgesics were commonly prescribed, comprising seven substances, including four opioids. The top three—metamizole, paracetamol, and dalteparin—were given to over half of patients. Among patients with a relevant eGFR discrepancy, more than one-third received dalteparin and morphine, both primarily renally eliminated.
Discussion
Despite frequent malnutrition and cachexia in palliative patients—and CysC being recommended as a muscle mass-independent marker—its use for GFR estimation in palliative care remains limited. Relevant differences between creatinine- and CysC–based estimates are known in geriatrics but have not been studied in palliative populations. Our study identified an intra-individual difference of 17 mL/min/1.73m2 between eGFRcr and eGFRcys in hospitalized palliative patients, with 53% showing a clinically relevant discrepancy exceeding 15 mL/min/1.73m2. Thus, renal function may be overestimated in up to every second palliative patient, increasing the risk of medication misdosing. In 53% of our cohort, this discrepancy would shift the chronic kidney disease classification by at least one stage, which is associated with a higher risk of kidney failure and mortality. 4 The intra-individual GFR difference in our study is comparable to other studies,15,24,25 but higher than in Carrero et al. 26 This may reflect differences in study populations: the former examined hospitalized or geriatric patients, while Carrero et al. analyzed outpatients. Hospitalized and older patients are more comparable to our cohort due to the associated frailty. Overall, we observed differences of >15 mL/min/1.73m2 in 31% (n = 26) and >30 mL/min/1.73m2 in 22% (n = 19) of patients. Unexpectedly, no linear association between BMI and eGFRcys was observed, despite nephrology guidelines recommending the use of CysC–based GFR equations over creatinine-based ones in patients with low muscle mass. 13 Among examined variables, only age and steroid use were significantly associated with mean eGFRcys. The missing linear relationship between BMI and eGFRcys may be explained by several confounders acting simultaneously, each exerting a modest effect that cumulatively influenced eGFRcys but did not reach individual statistical significance. The high average CRP level (65 mg/L) is indicative of an inflammatory burden, uncommon in standard populations. Negative associations between age and eGFR across all formulas are expected, as kidney function physiologically declines by approximately –1 mL/min/1.73m2 per year with aging, even without hypertension. 27 Diabetes, a leading cause of end-stage renal disease requiring dialysis, is well known to accelerate kidney function loss, explaining the negative association with eGFRcr. In contrast, smokers may exhibit a transiently higher eGFR due to hyperfiltration, which likely explains the positive correlation between active nicotine use and eGFR. 28
Approximately one-third of patients (32%) had AKI: 14% stage 1, 7% stage 2, and 11% stage 3, which is consistent with previous studies. 29 The largest intra-individual eGFR difference occurred in patients without AKI (22.5 mL/min/1.73m2, IQR 14.2–31.8). In stage 1 and 2 groups, the difference was similar, at approximately 8 mL/min/1.73m2, and smallest in stage 3 (2 mL/min/1.73m2). Hernandez et al. 15 also reported no relevant discrepancies across AKI groups. One possible explanation is that during an episode of AKI, both creatinine and CysC rise rapidly as GFR declines, such that non-GFR determinants (e.g., muscle mass for creatinine) become less influential than in stable conditions, where they typically drive eGFR discordance. However, the current evidence on this issue is inconsistent, and further research is needed to better elucidate this phenomenon.
This underscores the challenges and variability of GFR assessment in the acute setting, as well as the uncertainty about which hospitalized patients benefit most from CysC measurement. Mortality risk was nearly fourfold higher with AKI stage 2 or 3 (HR 3.60 [95% CI: 1.23–10.5], p = 0.019; and HR 3.89 [95% CI: 1.73–8.76], p = 0.001), consistent with Wang et al., who found similar results. 30
Of the 20 most prescribed medications, seven are primarily renally eliminated. Over 30% of patients with a relevant eGFRcr–eGFRcys discrepancy received morphine or dalteparin. For morphine, predominantly its active metabolites—not the parent compound—cause adverse effects when accumulated.5,6 Assessing pharmacokinetics is the physician’s responsibility. Often, alternatives not primarily renally excreted are available, or drug activity can be monitored, e.g., anti-factor Xa levels for low molecular weight heparin. 31 CysC-based eGFR currently costs about eight times more than creatinine analysis (University Hospital Zurich, July 30, 2025). Routine use is therefore not cost-effective and should be reserved for cases with high clinical suspicion of a relevant GFR discrepancy or when prescribing primarily renally eliminated drugs with significant toxicity risk. Because metamizole was the most frequently prescribed medication in our cohort but not approved in several countries, including the United States, the generalizability of our findings to these settings is limited.
A key limitation is the absence of comparison with a gold standard such as inulin clearance, which, although accurate, is very resource-intensive. Therefore, we cannot determine which of the two estimations better reflects true GFR. Analyses of laboratory parameters in heterogeneous clinical populations carry confounding risks and limit causal inference. We also could not assess whether discrepancies led to outcomes such as increased toxicity or mortality, owing to the retrospective design and lack of serial laboratory data. In palliative care, particularly the terminal phase, diagnostics without therapeutic consequence are usually omitted. For example, anti-factor Xa levels were not measured, precluding evaluation of drug accumulation (e.g., low molecular weight heparins). In addition, CysC-based eGFR measurement was not standardized but performed at the discretion of treating teams, introducing potential selection bias. Finally, given the high mortality rate and AKI in a third of the patients, the population in our study is highly morbid, and their creatinine levels are unlikely to be in a steady state. Therefore, the initial laboratory value in our analysis represents more of a snapshot than a stable creatinine baseline.
A key strength of this study is that, to our knowledge, it is the first to investigate intra-individual differences between eGFRcr and eGFRcys in a palliative care population, characterized by multimorbidity, advanced disease, and sarcopenia—factors that complicate renal assessment and increase the risk of misdosing. The data stem from routine practice and reflect a representative Swiss palliative care unit. With over 50% of patients showing a relevant eGFR discrepancy, the clinical importance of accounting for creatinine- versus CysC-based eGFR in palliative medication prescribing should be considered.
Conclusion
Clinically relevant intra-individual differences between creatinine- and CysC-based eGFR are common in palliative care patients, highlighting the risk of renal function misclassification with implications for drug selection and dosing. Given the higher cost of CysC testing, routine measurement is unlikely to be cost-effective. Instead, a targeted strategy is advisable: consider CysC when prescribing primarily renally eliminated drugs with a narrow therapeutic index or significant toxicity. A more precise eGFR determination might be even more relevant in outpatient palliative care, where long-term therapies are often administered, requiring ongoing consideration of kidney function to optimize the balance between therapeutic effects and side effects. Our findings emphasize the importance of clinical vigilance and individualized prescribing in palliative care. Prospective, multicenter studies, including those focused on outpatient palliative care populations, with correlation of pharmacokinetic/toxicity outcomes are warranted to define when CysC adds actionable value and to develop pragmatic algorithms balancing accuracy, cost, and patient-centered care.
Authors’ Contributions
S.P. developed the study conception and design. Data collection was performed by I.K. and S.P. Data analysis was performed by I.K. Analysis results were interpreted by S.P. and I.K. M.S., C.H., and D.B. provided supervision and oversight of the study. The first draft of the article was written by S.P., supported by I.K., and all authors commented and contributed on previous versions of the article. All authors read and approved the final article.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for the submitted work.
Statement of Ethics
The study was conducted in accordance with the Declaration of Helsinki and applicable regulatory requirements. Consent was based on documented written general consent in the internal electronic health record of the University Hospital Zurich. Consent is covered within the Ethics approval for registry and use of data. This study was approved by the local ethics board of the canton of Zurich (BASEC No.2019-02488).
Data Availability
All data that support the findings in this study are not openly available due to reasons of sensitivity and are available from SP upon reasonable request in anonymized form after approval by the local ethics board.