
Abstract
Background:
Buprenorphine is an underused opioid therapy for patients with serious illnesses. Using the principles of implementation science, we developed, distributed, and tested a Buprenorphine Pocket Card and Tool Kit (Bupe PC&TK).
Objectives:
We conducted an online survey to assess buprenorphine learning needs, confidence, and knowledge. We then tested the impact of the Bupe PC&TK using a pre-/poststudy design.
Setting/Subjects:
Palliative care clinicians located throughout the United States.
Measurement:
Investigator-initiated online mixed-methods survey at baseline and six weeks following distribution of a Bupe PC&TK.
Results:
Among the 179 baseline participants, most were physicians (n = 114) with more than six years of opioid prescribing experience (n = 99). The majority rated buprenorphine prescribing as an important skill, but only 15 participants reported they were very confident in prescribing or managing buprenorphine, and inaccurate knowledge was common. Participants reported that information on buprenorphine dosing and initiation would be most helpful in a Bupe PC&TK. Fifty-six participants completed the follow-up survey; the majority were physicians (n = 33). Most participants used the Bupe PC&TK (n = 47) and rated it as helpful or very helpful (n = 45). A paired samples t-test revealed that participants were significantly more confident after receiving the Bupe PC&TK (p < 0.001). Knowledge accuracy improved for buccal buprenorphine (p = 0.003) and formulations for opioid use disorder (p < 0.001).
Conclusion:
Palliative care clinicians ascribe a large degree of importance to prescribing buprenorphine but have knowledge and confidence gaps. The Bupe PC&TK can be readily implemented to increase clinician confidence and knowledge in prescribing buprenorphine to patients with serious illness.
Key Message
Buprenorphine is an important tool for patients with serious illness but requires active implementation support. This study describes the development, distribution, and testing of a Buprenorphine Pocket Card and Tool Kit. The resources can be readily implemented to increase palliative care clinicians’ buprenorphine knowledge and prescribing confidence.
Introduction
Buprenorphine is an evidence-based treatment for chronic pain, opioid misuse, and opioid use disorder (OUD).1–3 Given its clinical utility and superior safety profile compared to full opioid agonists, buprenorphine is an important tool for addressing pain, opioid misuse, and/or OUD in patients with serious illness.4–7 Buprenorphine is an underused medication, especially in the context of older adults and those with serious illness. 8
Implementation science aims to bridge the gap between research and practice by using implementation strategies. 9 Implementation strategies are the tools and methods deployed to improve uptake of evidence-based clinical innovations.10–12 Ideally, implementation strategies are not randomly selected but tailored to the context and key parties’ needs. 13 In our prior work, we developed an understanding of barriers to buprenorphine prescribing among palliative care clinicians treating OUD.2,14–16 We identified limited access to information, training, and education specific to palliative care clinicians managing chronic pain, OUD, or opioid misuse. Using the Expert Recommendation for Implementing Change (ERIC) implementation matching tool, we identified possible implementation strategies best suited to overcoming these barriers.11,12,17
For this study, we chose to implement the strategy of developing and distributing educational materials, specifically a Buprenorphine Pocket Card and Tool Kit (Bupe PC&TK). We followed the VA Qualitative Enhancement Research Initiative (QUERI) Implementation Road Map that consists of preimplementation, implementation, and sustainment phases (Fig. 1). Specifically, we used our prior research to characterize the problem (i.e., buprenorphine knowledge gaps).2,14,16 We then used these insights and early stakeholders’ engagement to develop an initial Bupe PC&TK prototype (preimplementation). Next, we conducted an initial survey of end users (i.e., palliative care opioid prescribers) on the Bupe PC&TK as a solution to improve buprenorphine knowledge and confidence (early implementation). In a pre/post study design, we tested the impact of the initial Bupe PC&TK prototype and sought feedback to improve or refine aspects of the Bupe PC&TK (impact/sustainment). We based the Bupe PC&TK evaluation on the four-level Kirkpatrick Model (reaction, learning, behavior, and results), 18 a framework for assessing medical education. We focused on the first two Kirkpatrick levels by measuring satisfaction, confidence, and knowledge. We hypothesized that a Bupe PC&TK tailored to palliative care clinicians’ learning needs would be helpful and improve buprenorphine knowledge and prescribing confidence.
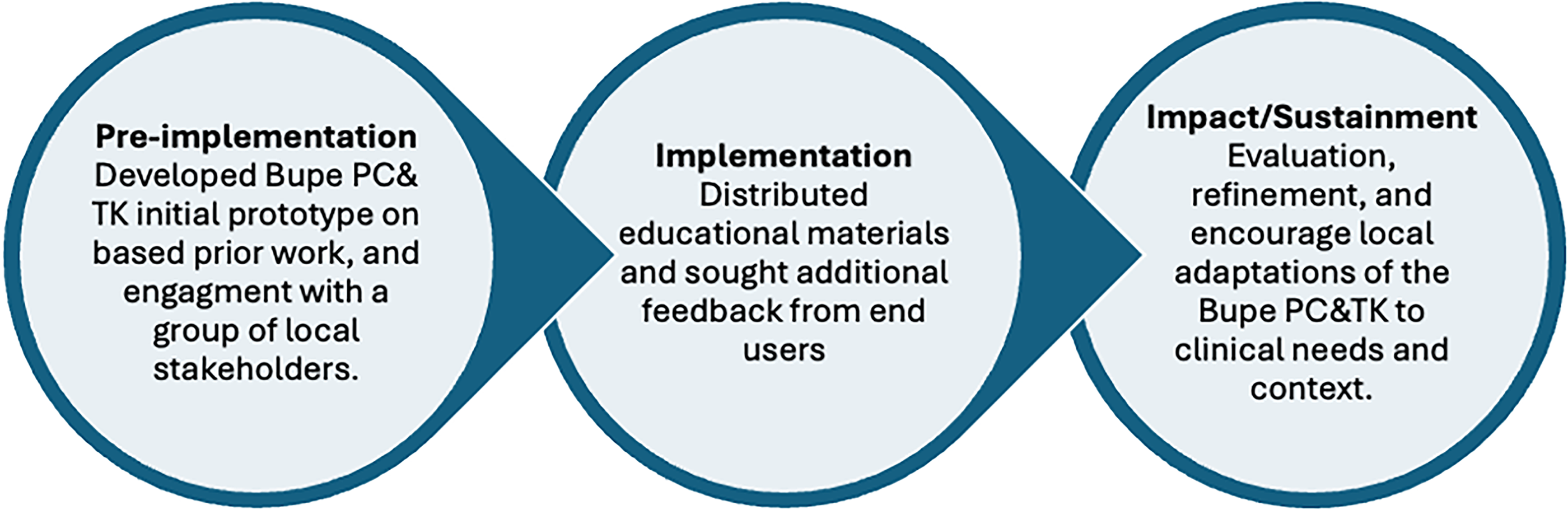
Study methods adapted from the VA Quality Enhancement Research Initiative (QUERI) Roadmap. Adapted from: https://www.queri.research.va.gov/tools/roadmap.cfm. Buprenorphine Pocket Care and Tool Kit is abbreviated as Bupe PC&TK above.
Methods
The study was deemed an educational quality improvement project by the VA Research Determination and IRB. We followed the SQUIRE-EDU extension for reporting education quality initiative projects 19 and the Proctor recommendations for specifying and reporting implementation strategies. 10
Preimplementation: Bupe PC&TK prototype development
The initial Bupe PC&TK prototype was modeled after the Geriatrics 5Ms Pocket Card. 20 The development of the Bupe PC&TK involved collaboration among study authors with expertise in medical education, implementation science, and buprenorphine prescribing. Using think-aloud research methods, 21 we asked stakeholders to identify key resources (e.g., “go to articles”), narrate information they would need to prescribe buprenorphine, how they would access or navigate the Bupe PC& TK, and areas to improve usability. The stakeholders included three education, design, and palliative medicine experts at the Center to Advance Palliative Care (CAPC); two pain pharmacists; two dual-boarded addiction medicine and pain physicians; and six palliative care clinicians with varying buprenorphine prescribing experience. Examples of stakeholder suggestions for the Bupe PC&TK was to include information from key articles (e.g., bioavailability estimates from Hickey et al. 2022), chronic pain guidelines, and provide patient-facing materials. It took approximately six months to create and refine the Bupe PC&TK prototype tested here.
For the initial Bupe PC&TK, we organized the information into six sections: a buprenorphine overview, why prescribe buprenorphine, when to choose buprenorphine, which buprenorphine formulation to select, how to start buprenorphine, what to tell patients, and monitoring considerations (The Bupe PC is included in Supplementary Appendix A1). The online toolkit (pictorial in Supplementary Appendix A2) is located on the free website Padlet (https://tinyurl.com/enj3atw7). It includes a comprehensive reference list and publicly available free resources (e.g., CAPC buprenorphine blog posts, diagnostic criteria for OUD, Clinical Opioid Withdrawal Scale, and patient education materials developed at the VA). The Bupe PC&TK focuses on buprenorphine (sublingual, transdermal, or buccal) formulations, which we believe are most commonly prescribed by palliative care clinicians (e.g., sublingual, transdermal, or buccal buprenorphine).
Implementation: Initial survey of end users
During the initial survey window (March 2024 to June 2024), participants were asked to provide informed consent and complete a brief five- to seven-minute survey (Supplementary Appendix A3). On the survey invitation, we specified that we were seeking participants who prescribe or manage opioid therapy for patients with serious illness or older adults, which was intended to be inclusive of pharmacists and clinicians providing primary or specialty palliative care. The survey questions were developed to encompass the Kirkpatrick levels (i.e., satisfaction, confidence, and knowledge) and modeled after the Geriatrics 5Ms Pocket Card evaluation. 20 The knowledge questions were selected from prior CAPC buprenorphine continuing medical education presentations. The initial survey was piloted by three clinicians (not included in the study) for clarity and functionality. Survey responses were collected using REDCap. 22 Upon completion of the initial survey, participants were provided with the link to access the Bupe PC&TK. We distributed the survey by email through palliative care networks (e.g., program leaders, fellowship directors, and peers) and used snowball sampling by encouraging forwarding the survey to other palliative care colleagues within or outside their institution.
To describe our sample, we collected information on clinical discipline (physician, nurse practitioner, physician assistant, or pharmacist) and years of prescribing or managing opioid therapy. The initial survey assessed baseline buprenorphine prescribing experience, prior buprenorphine training and knowledge, buprenorphine prescribing self-efficacy, and the degree to which participants felt buprenorphine prescribing was an important skill. To measure self-efficacy, we asked clinicians to rate their confidence to prescribe or manage buprenorphine in patients with serious illness on a 5-point Likert scale (1 = not confident; 5 = very confident). Participants then rated how important buprenorphine prescribing skills were among clinicians caring for patients with serious illness on a 5-point Likert scale (1 = not important; 5 = very important). We assessed baseline buprenorphine knowledge by asking a series of questions on buprenorphine pharmacology and dosing. To avoid guessing the correct response, participants were also given the option to select “I do not know.” Finally, we included an optional free-text box asking participants what they would find helpful in a Bupe PC&TK. We requested that participants provide an email address to distribute a follow-up survey.
Impact of the Bupe PC&TK: Follow-up survey
Using the emails provided in the initial survey, we emailed a six-week (May 2024 to July 2024) follow-up survey with up to three email reminders. The follow-up survey (Supplementary Appendix A3) aimed to evaluate the impact of the Bupe PC&TK on knowledge and confidence. Additionally, we sought feedback on the utility of the Bupe PC&TK and opportunities for improvement.
Data analysis
We analyzed quantitative and qualitative data from all initial survey responders. Among the subset of participants who responded to both surveys, we completed a secondary analysis linking participants’ initial and follow-up responses. We used SPSS and Excel for all analyses.
We calculated descriptive statistics (e.g., frequency, mean, proportion) to describe the clinical discipline of participants, years prescribing opioid therapy, prior buprenorphine training and prescribing, confidence, and importance of buprenorphine as a clinical tool. Initially, we coded the knowledge questions as correct, incorrect, or unsure.
Excel was used to organize and code free-text responses. Participants who reported prior buprenorphine training were organized into five training categories: X-waiver, fellowship, chronic pain-focused, OUD-focused, did not specify, or more than one prior training type. Participants’ recommendations for what would be helpful in a Bupe PC&TK were analyzed using an iterative inductive content analysis approach. 23 Content analysis was selected since free-text responses were relatively brief and not intended to be exhaustive. Two investigators (KF, AS) identified subcodes to develop an initial codebook. The codebook was applied to the data, and discrepancies and clarifications were discussed. The codebook was iteratively refined and applied to responses until no new subcodes emerged. Subcodes were then categorized into larger themes using an inductive process. Finally, we counted the occurrence of different themes 24 to prioritize Bupe PC&TK content and feedback.
For the secondary analyses, we linked initial and follow-up responses for knowledge and self-efficacy questions from only the participants who responded to both surveys. We tested for change on the 5-point Likert scale assessing self-efficacy (i.e., confidence prescribing) using a paired samples t-test. To assess a change in knowledge, we dichotomized responses to the initial and follow-up knowledge questions as correct or incorrect/do not know. We then used McNemar tests to determine whether accuracy significantly improved from before to after receiving the Bupe PC&TK.
Among responses to the follow-up survey, we also calculated descriptive statistics, including how many participants used the Bupe PC&TK (yes, no) and how often. We categorized free-text responses of how often over the past —four to six weeks participants used the Bupe TK&PC as never (0), rare (1–2 times), weekly (3–5 times), or more than weekly (>5 times). We also calculated the mean of Likert responses (1–5) regarding the degree to which the Bupe PC&TK was rated as helpful. To understand the most helpful aspect of the Bupe PC&TK, we categorized qualitative responses into the codes initially created during the analysis of the initial survey (e.g., patient education, buprenorphine initiation) and added other codes as needed. No formal coding method was applied to the free-text additional feedback.
Results
Initial assessment of buprenorphine prescribing practices, knowledge, and self-efficacy
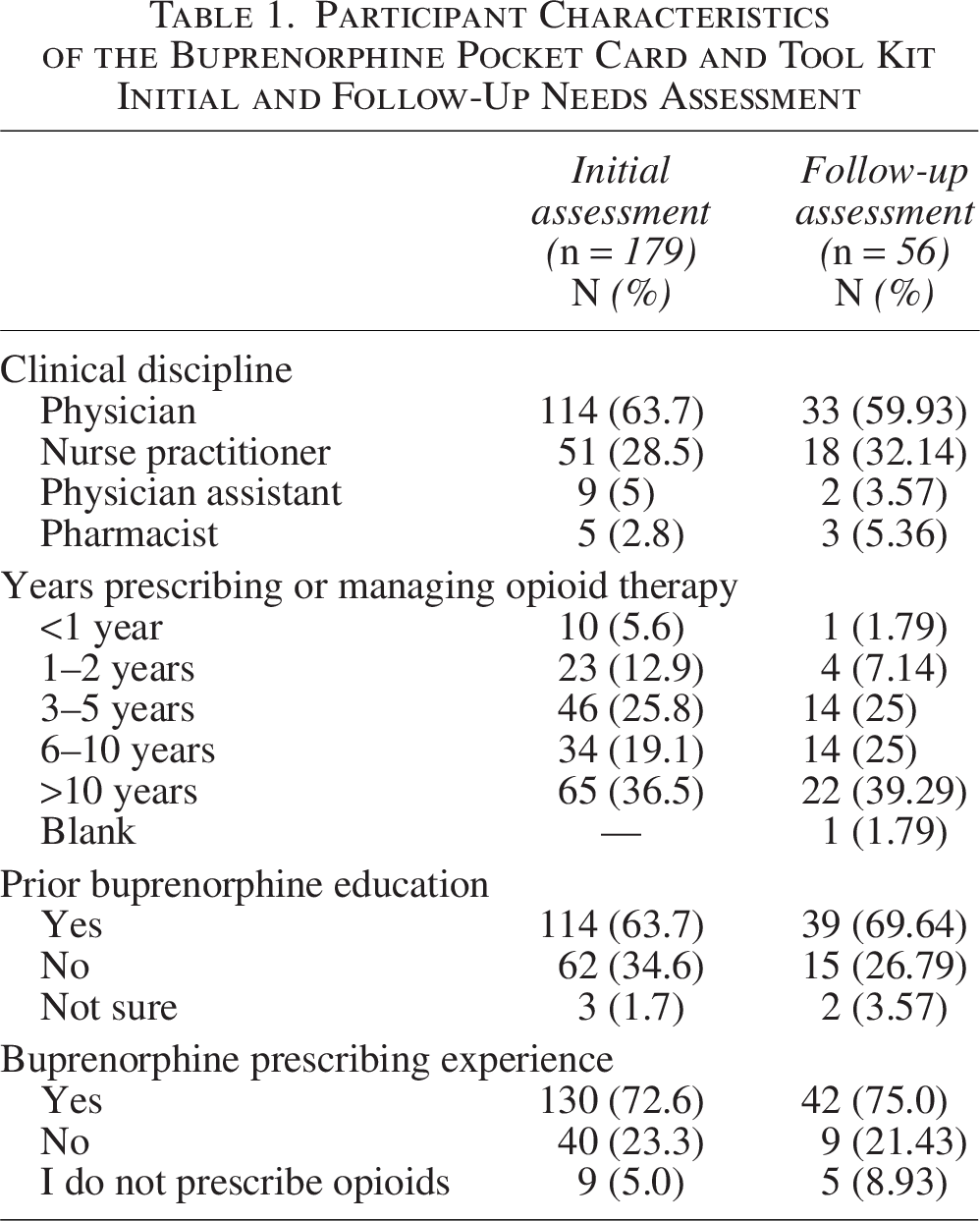
Among the 179 participants who answered the initial survey, 63.7% (n = 114) were physicians, 28.5% (n = 51) were nurse practitioners, 5.0% physician assistants (n = 9), and 2.8% pharmacists (n = 5). More than half (n = 99, 55.6%) had more than six years of experience prescribing opioids and 72.6% (n = 130) had previously prescribed buprenorphine. The majority of respondents had completed at least one prior buprenorphine training (n = 114, 63.7%) including X-waiver training (n = 24, 24.02%), chronic pain training (n = 15, 8.38%), and OUD training (n = 9, 4.47%), and some participants (n = 33,18.44%) completed more than one buprenorphine training. Most participants rated their confidence in prescribing buprenorphine to patients with serious illness as somewhat confident (n = 51, 28.7%), neutral (n = 49, 27.5%), or not at all confident (n = 21, 11.8%). Only 15 participants (8.4%) rated their confidence in prescribing or managing buprenorphine as very confident. Table 1 describes the initial survey sample.
Participant Characteristics of the Buprenorphine Pocket Card and Tool Kit Initial and Follow-Up Needs Assessment
Most participants who completed the initial survey reported buprenorphine prescribing was an important or extremely important skill for caring for people with serious illness with any indication (n = 165, 92.18%) and important or extremely important for pain (n = 171, 95.5%) and OUD (n = 166, 92.7%). Zero participants reported that buprenorphine prescribing was not at all an important skill for clinicians caring for people with serious illness, pain, or OUD. Among the 179 participants, buprenorphine knowledge accuracy per question ranged from 36.3% to 72.6%. For example, 130 (72.6%) correctly identified that sublingual buprenorphine could precipitate opioid withdrawal, and 35 participants (19.6%) did not know. Over one-third of participants incorrectly identified that low-dose buprenorphine (i.e., buccal or patch) could precipitate opioid withdrawal (n = 57, 31.8% for buprenorphine 10 µg patch and n = 76, 42.5% 300-µg buccal buprenorphine). One-hundred fifty-four (86.0%) correctly identified buccal, sublingual, and transdermal buprenorphine formulations that can be used for chronic pain, and 13.9% either did not know (n = 14, 7.8%) or incorrectly answered (n = 11, 6.1%). Fewer participants (n = 65, 36.3%) correctly responded that it is false that all buprenorphine formulations (e.g., buccal, transdermal, and sublingual buprenorphine) can be used to treat OUD.
Initial needs assessment
One-hundred thirty-one participants provided free-text responses of what they would find helpful in a Bupe PC&TK. These responses were coded into eight themes. The themes included information on dosing, buprenorphine initiation, obtaining patient buy-in, managing full opioid agonists, indications and contraindications, a comprehensive resource, and monitoring parameters. Table 2 provides information on the buprenorphine needs assessment, including themes, subthemes, and frequency.
Potentially Helpful Information to Include in a Buprenorphine Pocket Card and Tool Kit: Themes and Subthemes from the Initial Survey
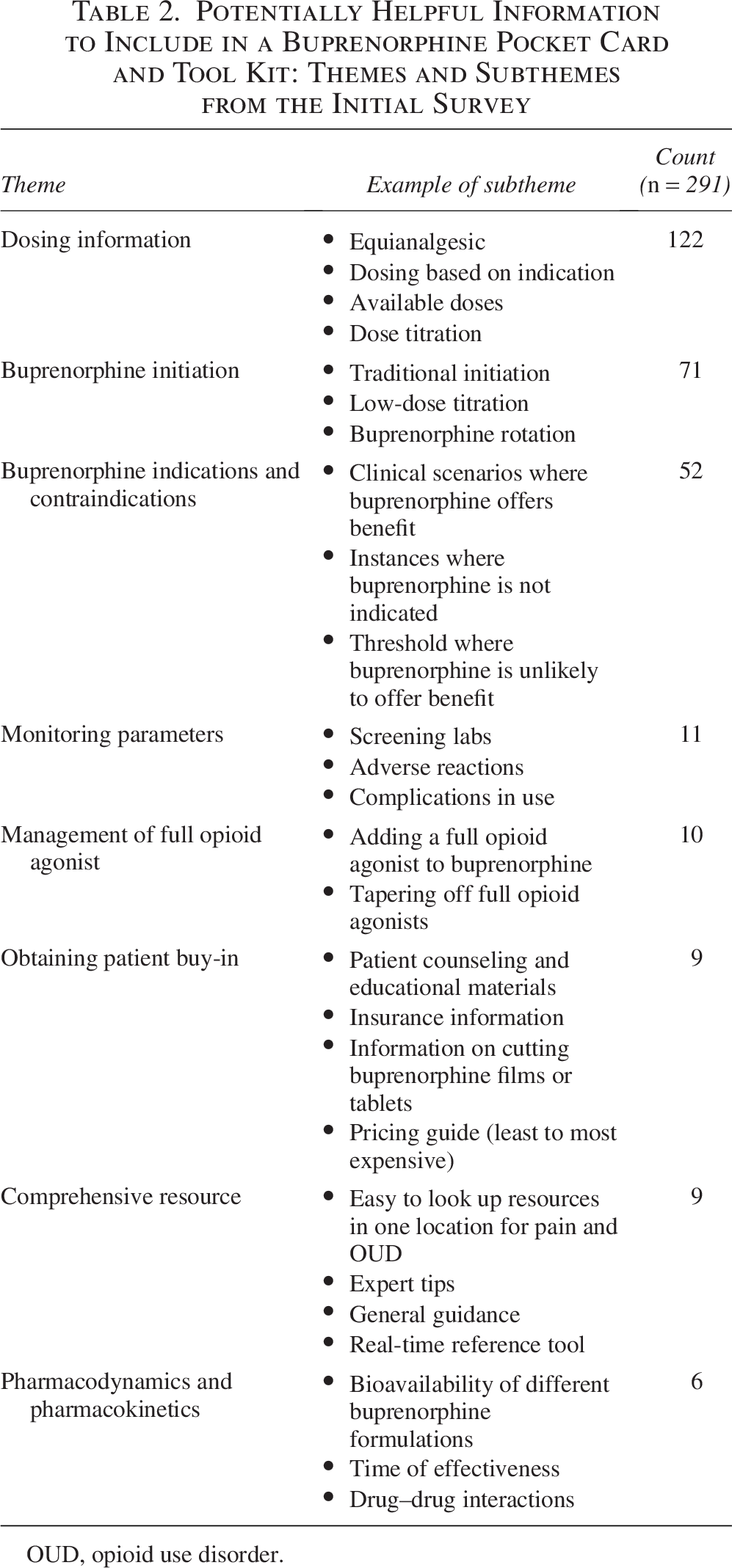
OUD, opioid use disorder.
Follow-up survey
Of the 179 participants who responded to the initial survey, 56 (31.3%) completed the follow-up survey. Among those who responded to the follow-up survey, the majority were physicians (n = 33, 59.9%) or (n = 20, 35.71%). Respondents to the follow-up survey were similar to respondents to the baseline survey regarding prior training and opioid prescribing (Table 1).
Among the 56 participants, most used the Bupe PC&TK (n = 47, 83.83%) within six weeks of receiving it, and 43 reported using it at least once/week. The majority rated the Bupe PC&TK as helpful or very helpful (n = 45, 80.36%); two (3.57%) participants reported it was neutral or somewhat helpful, and 9 (16.07%) left the question blank. No participants responded that the Bupe PC&TK was not helpful.
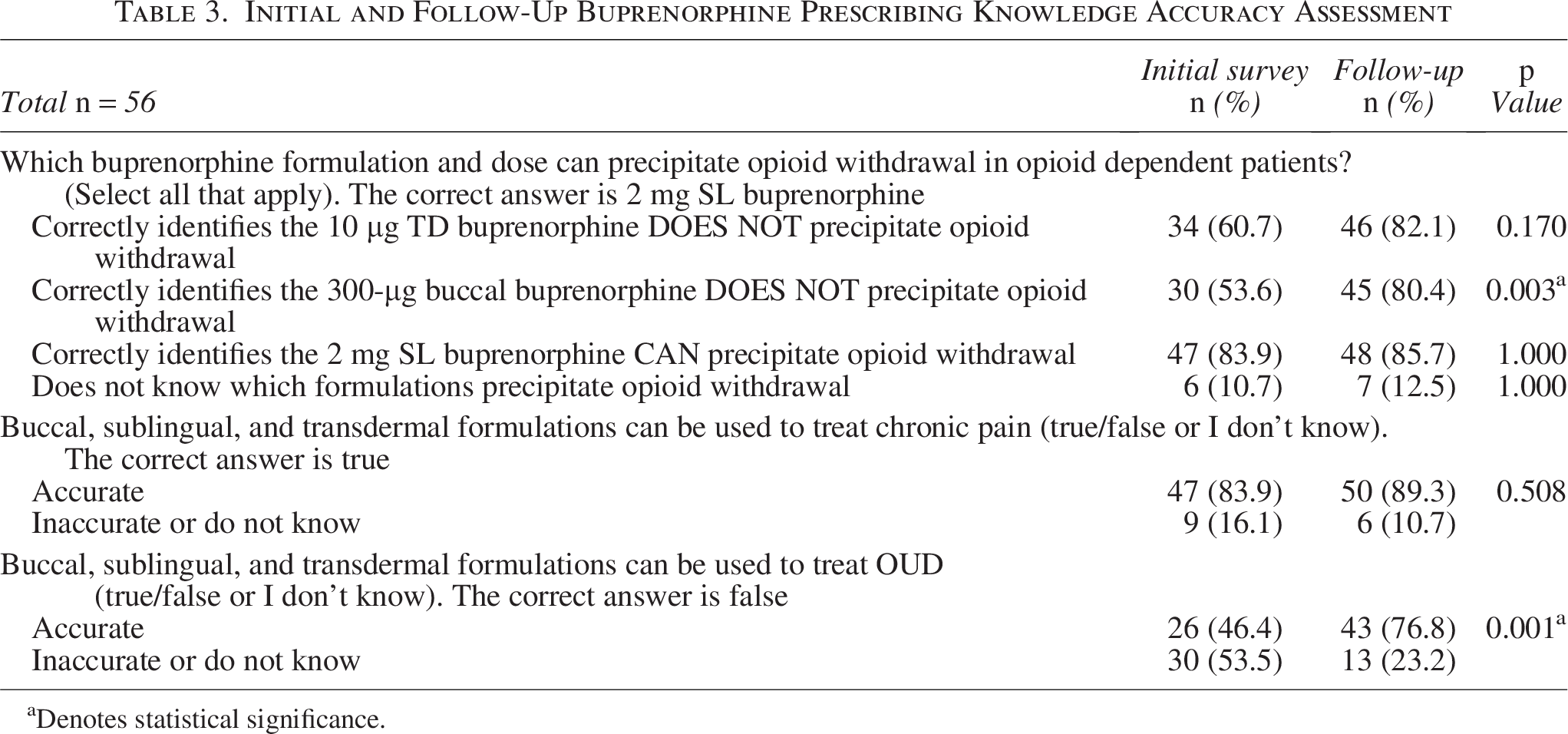
A paired samples t-test revealed that, among participants who responded to both surveys, participants were significantly more confident after receiving the Bupe PC&TK (M = 3.67, SD = 0.94) than before (M = 3.02, SD = 1.03), p < 0.001, Cohen’s d = 0.93. Figure 2 depicts the change in confidence levels from the initial and follow-up surveys. Knowledge accuracy improved across the series of questions, ranging from 46.3% to 83.9%. Participants had a significant improvement in knowledge of buccal buprenorphine (p = 0.003) and identification of correct buprenorphine formulations for OUD (p < 0.001). Accurate knowledge of the buprenorphine patch and sublingual buprenorphine was high at baseline and did not significantly change after receiving the Bupe PC&TK. The results of initial and follow-up knowledge questions are shown in Table 3.
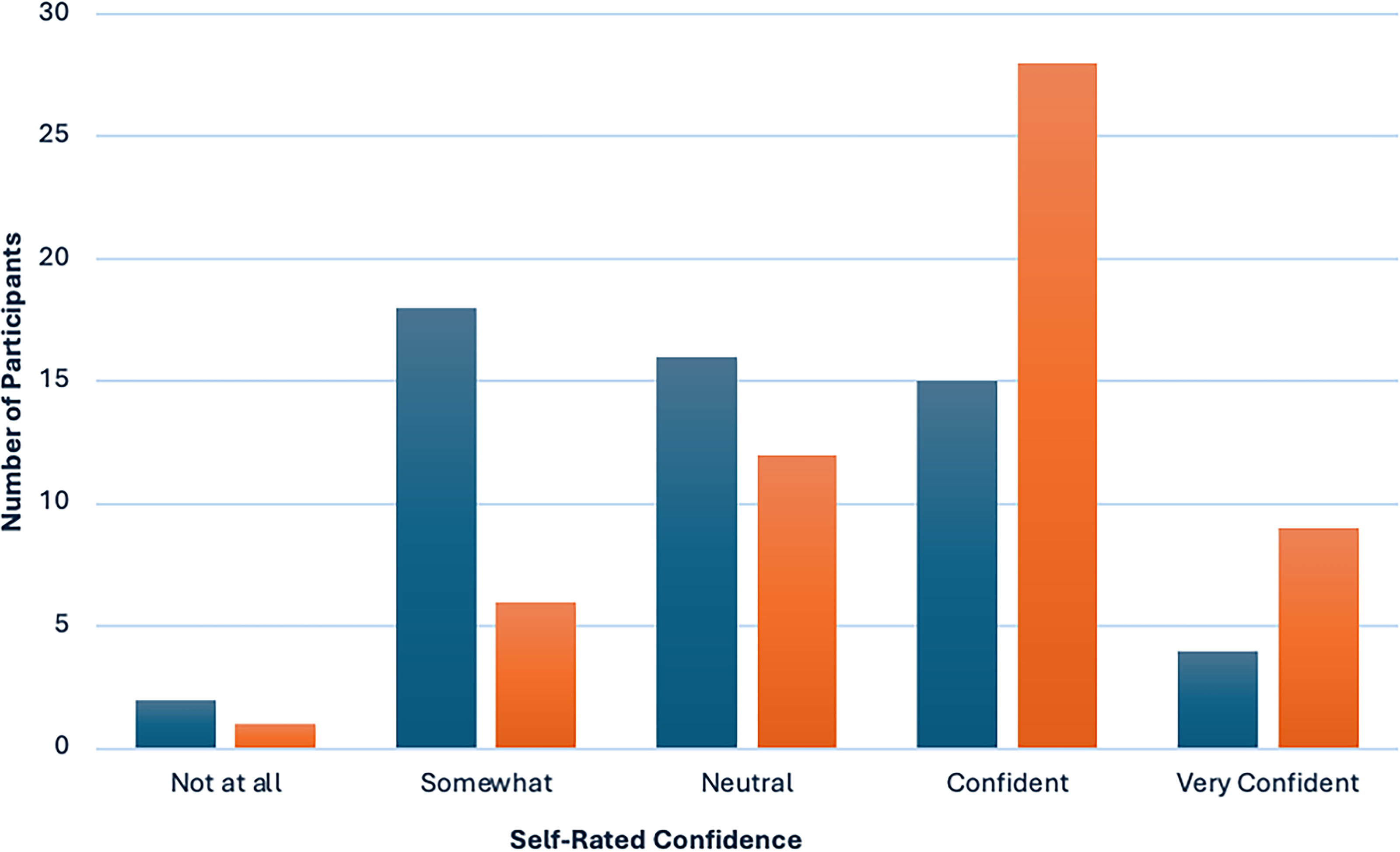
Initial and follow-up assessment of confidence in prescribing and managing buprenorphine after receiving the Buprenorphine Pocket Card and Tool Kit.
Initial and Follow-Up Buprenorphine Prescribing Knowledge Accuracy Assessment
Denotes statistical significance.
Forty-three participants responded to an optional question on aspects of the Bupe PC&TK that were most helpful. Many participants (n = 23) identified information on buprenorphine dosing as the most helpful. For example, one participant said, “The flowcharts and dosing algorithms are very clinically useful,” and another said, “the conversion chart is so helpful! I think buprenorphine conversion is the most challenging part of buprenorphine dosing.” Participants found it beneficial to have a comprehensive buprenorphine resource tailored to patients with serious illness (n = 8). One participant said, “There is so much information about buprenorphine for OUD that it is sometimes hard to search quickly for an answer for other indications.” Several participants (n = 11) appreciated the format of a pocket card. For example, one participant noted, “The pocket card gives very specific and user-friendly information.” Another said, “It completely takes the guesswork out of prescribing buprenorphine for those who are just beginning to incorporate this into their practice.” Many participants noted that they carried the pocket card with them, distributed it to colleagues and learners, or displayed it in their workrooms.
Of the 27 additional comments, the majority were positive. One participant wrote, “This is an outstanding resource and has already begun to change the way our group manages pain.” Another participant said, “I have a way to go before I’m really comfortable with buprenorphine, but this resource really helps.” Although many participants appreciated the comprehensive nature of the Bupe PC&TK, one participant said, “at first, it was overwhelming.” Participants also commented that the Bupe PC&TK did not address systemic and institutional barriers to buprenorphine prescribing, such as insurance coverage for buprenorphine and availability at their institution. A few participants recommended adding information on converting buprenorphine to or from methadone and buprenorphine pricing.
Discussion
There is a groundswell of support to incorporate buprenorphine into the opioid armamentarium of palliative care clinicians. Yet, many palliative care clinicians endorse barriers. There are limited implementation strategies tailored to palliative care clinicians to increase buprenorphine adoption for chronic pain, opioid misuse, and/or OUD. Among 179 participants, we identified buprenorphine prescribing perceived importance, confidence, knowledge, and educational needs. Six weeks after Bupe PC&TK distribution, a subset of 56 palliative care clinicians rated the implementation strategy as helpful, and the results demonstrated a significant improvement in confidence and knowledge.
The majority (92%) of the 176 participants rated buprenorphine prescribing as an important or extremely important skill when caring for patients with serious illness, and no participants rated buprenorphine as an unimportant skill. These findings may reflect the degree of interest of our convenience sample. However, it also likely reflects shifting attitudes among palliative care clinicians to prioritize training and buprenorphine prescribing skills, 25 with over half of the sample engaging in prior buprenorphine training. The high degree of interest and importance ascribed to buprenorphine prescribing is notably higher than in other specialties (e.g., primary care), where lack of clinician buy-in is often a barrier to implementation. 26 These findings suggest a window of cultural readiness for buprenorphine adoption within the specialty of palliative care. Cultural alignment is a key predictor and precondition for implementation success. 27
Our Bupe PC&TK was developed to enhance buprenorphine implementation for patients with serious illness. We targeted palliative care clinicians using a single implementation strategy, specifically deploying educational materials without other active implementation support (e.g., audit and feedback, facilitation, academic detailing). Although a single implementation strategy and simple distribution of educational materials are rarely sufficient to change practice, 28 early results suggest the Bupe PC&TK had a large effect on clinician prescribing confidence, increasing it by nearly a full standard deviation. This finding is noteworthy because even though the majority completed buprenorphine education training and had prescribing experience, few participants were highly confident or had accurate knowledge before Bupe PC&TK distribution. The follow-up survey responses suggest improvements in knowledge and confidence may be attributed to having key information that matched prescribing needs readily available. For example, participants indicated dosing and bioavailability information would be important information to include in a Bupe TK&PC. This information was included on the initial Bupe PC&TK prototype under the header “Which buprenorphine formulation to select.” However, participants and journal reviewers described potential improvements to the Bupe PC&TK prototype, including buprenorphine pricing, extended-release buprenorphine, and conversion to methadone. Furthermore, there were suggestions to broaden the resources Bupe PC& TK to include more upstream resources to improve clinical decision making, such as screening tools for unhealthy substance use. We agree that widespread adoption of buprenorphine will require multifaceted implementation strategies. 29 In the future, we intend to pair the Bupe PC&TK with other implementation strategies. Buprenorphine implementation facilitation and interactive clinical decision-making tools demonstrate success in other buprenorphine prescribing contexts.30,31 Participants named issues with buprenorphine insurance coverage and pharmacy availability; these barriers are pervasive and have been described elsewhere.32,33 Alternative implementation strategies are needed to address larger barriers unrelated to clinician knowledge.
The study has several limitations. We used a convenience sample of palliative care clinicians recruited through palliative care networks, including many with high levels of baseline buprenorphine prescribing knowledge and skills. The findings may be less generalizable to other specialties and among clinicians without prior buprenorphine training or prescribing experience. Participation was not anonymous (email addresses were required), and our response rate was lower than ideal, albeit typical of online surveys. 34 Both of these limitations may have introduced desirability bias. We believe completion of the postsurvey was less than that of the initial survey for several reasons. We did not offer monetary or other completion incentives. We used only one survey distribution modality (i.e., email) with a relatively short turnaround time. Our target population was clinicians who often have many competing demands on their time. We did not measure the downstream impact on clinical outcomes, such as patient outcomes and clinician behavior. Most of the participants had previously been prescribed buprenorphine, making it a difficult outcome in which to assess change. Further, determining the optimal outcome of buprenorphine implementation efforts requires careful consideration since prescribing metrics alone may fail to capture opioid management complexity. 35 Despite these limitations, our study is among the first to focus on the development of a buprenorphine implementation strategy that is not solely focused on the context of OUD.
Conclusion
We used the principles of implementation science to develop and test a Bupe PC&TK tailored to the needs of palliative care clinicians. The study findings suggest the Bupe PC&TK increases clinician confidence and knowledge in prescribing buprenorphine to patients with serious illness. The Bupe PC&TK is available on the CAPC website and can be downloaded (https://tinyurl.com/enj3atw7), customized, adapted, and reproduced to meet the specific needs of palliative care practices or other specialists seeking to improve buprenorphine adoption. Indeed, we encourage clinicians to consider implementation adaptations to better “fit” their context or needs. Participants in our study also used Bupe PC&TK to educate colleagues, learners, and patients. Future research will build on our findings, including iteratively refining the Bupe PC&TK resources and deploying them with multifaceted implementation strategies.
Authors’ Contributions
The authors confirm contributions to the article as follows: Study conception and design: K.F.J., A.W.S., A.M.L., J.S.M., W.C.B., and D.E.M. Intervention development: K.F.J., A.W.S., W.C.B., A.M.L., D.E.M., J.S.M., M.J.S., L.M.K., D.P., and J.J.W. Analysis and interpretation of the results: K.F.J., J.B.W., and A.W.S. Funding acquisition: J.S.M. Writing the original draft, reviewing, and editing: K.F.J. and A.W.S. Writing review, editing, and supervision: J.B.W., W.C.B., D.G., A.M.L., D.E.M., J.S.M., M.J.S., L.M.K., D.P., J.J.W., and A.W.S. All authors have read and approved the final version of the article and agree to be accountable for the work.
Footnotes
Author Disclosure Statement
Some of these materials are the result of work supported with resources and the use of facilities at the Veterans Affairs Boston Healthcare Center and the New England Geriatric Research Education and Clinical Center. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government.
Funding Information
This mentored research was supported in part by the National Institute of Health (1K24DA056837) to J.S.M.
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.