
Abstract
Background:
Palliative care interventions for children with serious illness require real-world design expertise to bring research to the bedside in ways that are engaging, effective, and feasible.
Objective:
To describe the collaborative process of bringing an evidence-based humanistic care intervention, photo-narratives, through practical user experience (UX) design for future implementation at a children’s hospital.
Methods:
The collaborative design process was completed at an academic university. Researchers at the affiliated children’s hospital approached two teams of UX design graduate students to (1) further refine and (2) develop a technology-integrated implementation strategy for the photo-narrative intervention.
Results:
The researchers and teams met weekly to follow a project-specific seven-step UX design approach, including (1) framing project timeline and deliverables, (2) regulatory and access considerations, (3) understanding the problem and intervention, (4) data collection, (5) design constraints (information technology considerations, workflow), (6) low-fidelity prototyping, and (7) usability testing and high-fidelity prototyping.
Conclusion:
Collaboration between researchers and UX design teams can further the critical intervention design and prototyping that is essential to implementing successful real-world palliative care interventions.
Key Message
This article describes the collaborative process of bringing an evidence-based palliative care intervention, photo-narratives, through practical user experience design for future real-world implementation at a children’s hospital.
Introduction
Health care struggles with fractured, inefficient systems that often leave patients, their families, and their clinicians unsatisfied. 1 This is particularly important for those with serious illnesses, including children with complex chronic conditions, as they frequently utilize health care services, and families say they require more coordinated and whole-person responsive support.2–4
To counter this, strategies are needed that further help to build connection, trust, and humanistic care practices between patients, families, and clinicians.5,6 Driven by research, clinical programs are increasingly using photos and narratives as a way of bringing the full lives of patients as people into health care systems.7–10 These projects have shown promise particularly for building connections, diminishing clinician biases, and furthering whole-person care. 11
Building on this, a team of palliative care researchers interested in strengthening connections between children with complex chronic conditions, their families, and clinicians developed a photo-narrative intervention. 12 In short, the photo-narrative intervention asks children and their families to select up to three photos with captions that show information about (1) who is important in their family, (2) what well-being looks like, and (3) what strengthens them during difficult times. The completed photo-narrative is shared by email and through glossy color prints with the child’s clinicians. The researchers had studied the intervention’s impact through qualitative methods and were in the process of conducting a pilot randomized controlled trial to further understand feasibility, acceptability, and potential efficacy. 7
Yet, ultimately, palliative care researchers developing interventions may lack real-world design expertise to bring research to the bedside in ways that are engaging, seamless, visually appealing, and ultimately effective. 13 Partnering with design teams may be an important method for integrating serious illness intervention research in clinical practice in ways that make them more likely to be successfully implemented.
This article describes the process of bringing an evidence-based photo-narrative intervention through practical user experience (UX) design for implementation readiness at an academic children’s hospital.
Methods
This design process was completed between January and May 2025 as a collaborative capstone project between researchers within the Division of Bioethics and Palliative Care, Department of Pediatrics, and graduate students in the Human Centered Design and Engineering Program at the University of Washington. All use of data collected for research was approved by the Seattle Children’s Hospital Institutional Review Board (IRB).
The researchers aimed to further refine and develop technology-enhanced strategies, using the existing health care technology infrastructure (e.g., Epic and MyChart) to seamlessly bring the photo-narrative into the children’s hospital system. They applied to an existing university program that pairs sponsors with UX Master of Science students for their capstone project. 14 The photo-narrative was selected by two teams of four students who each undertook linked projects: (1) clinician-facing electronic health record, Epic, and integration and (2) family-facing MyChart family experience integration of the photo-narrative. Table 1 lists the researchers’ and design students’ qualifications and prior experiences that informed the project. The details regarding this process and the iterative photo-narrative design prototypes are described in detail below.
Team Qualifications and Prior Experiences
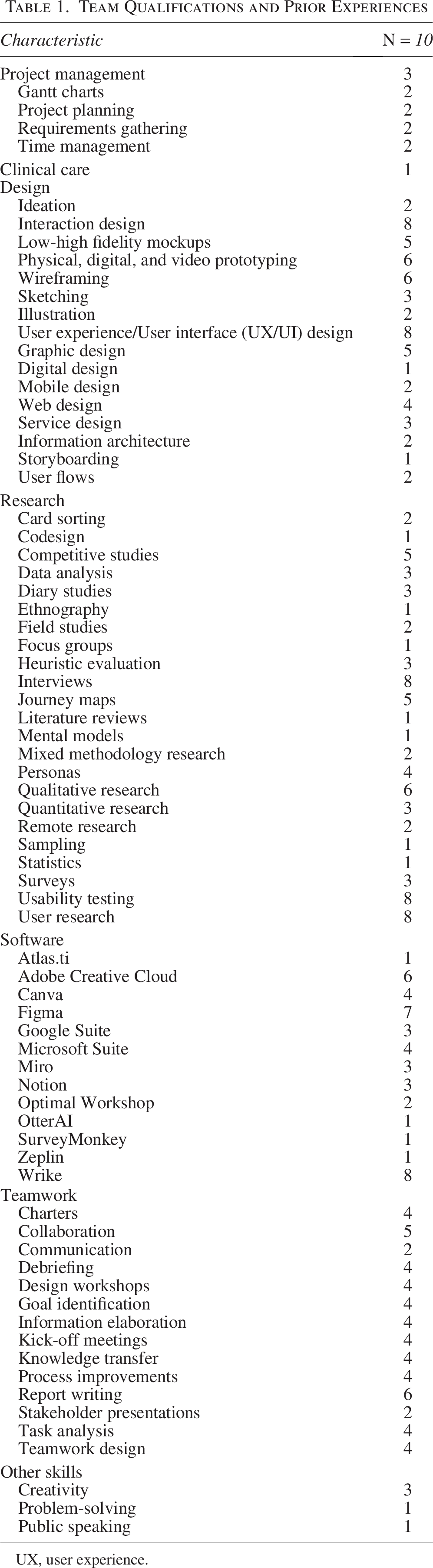
UX, user experience.
Results
The student UX design teams met with the researchers weekly during the project. The teams also worked together to ensure their projects were synergistic. Figure 1 shows the specific human-centered design seven-step process map that each team took. Each step was informed by established user-centered design principles but was developed in sequence to meet the unique context of the photo-narrative UX design process. The specifics of each of these seven-steps are described below.
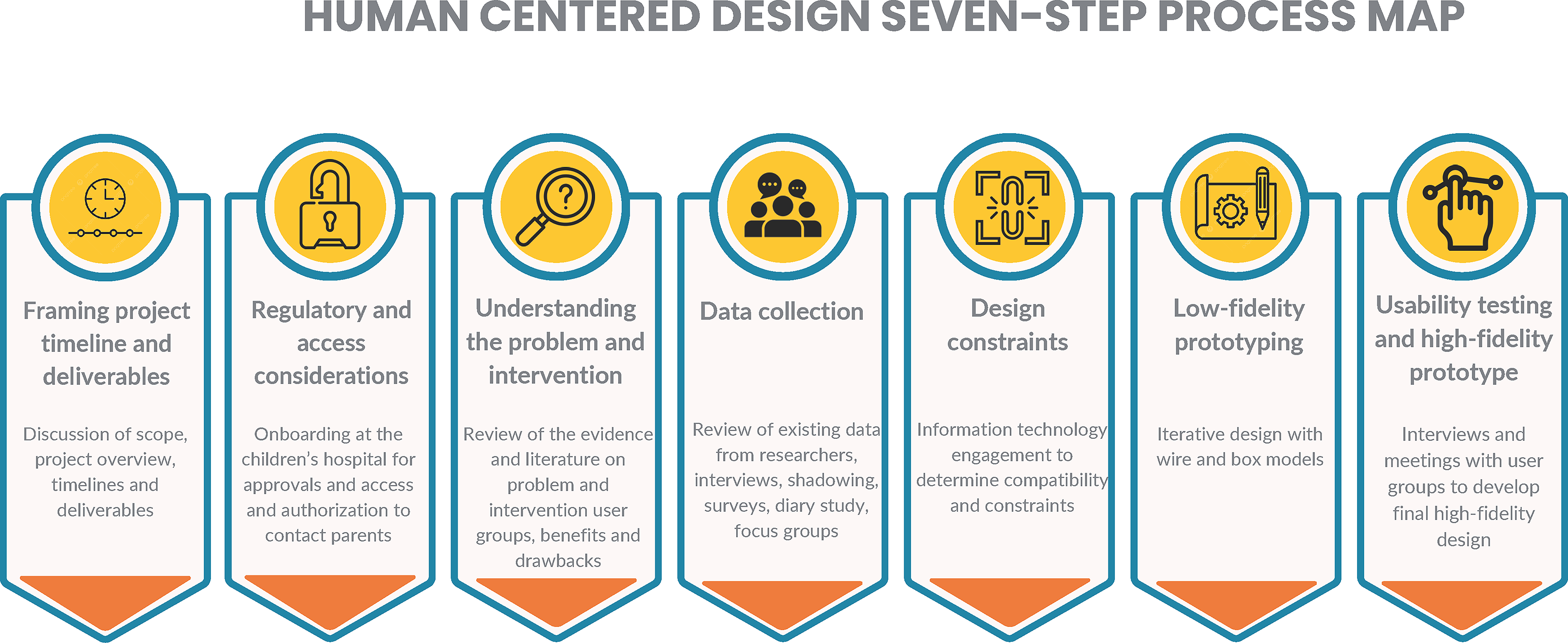
Human-centered design seven-step process map. This figure shows the seven-step UX design process used by the two graduate student teams collaborating with palliative care researchers, including framing project scope, regulatory considerations, understanding the problem, data collection, design constraints, low-fidelity prototyping, and usability testing leading to high-fidelity prototypes. UX, user experience.
Step 1: Framing project timeline and deliverables
The researchers and teams initially met together to discuss the scope of the project and to center key design and implementation issues. Together, they developed an overview of the project and a timeline to map methods for data collection, collaboration, and deliverables.
Step 2: Regulatory and access considerations
Next, the researchers worked with both teams to ensure they had completed all regulatory and access needs for the project. Specifically, teams needed extensive onboarding at the children’s hospital to be able to shadow staff and work in the Epic and MyChart play environments during their design process. Team members that planned to use data previously collected by the researchers were also added to the studies’ IRB and completed training in good clinical practice and human subjects research. Researchers also had to collect authorization releases from parents of children with complex chronic conditions from the research team’s parent advisory group who spoke with the students and permission from the children’s hospital family advisory committee to distribute anonymous surveys for design feedback. Finally, the student groups obtained permission from the children’s hospital’s marketing and communication team to use colors and themes in their prototyping designs.
Step 3: Understanding the problem and intervention
During this step, both teams did extensive training to deeply learn about the problems facing children with complex chronic conditions, their families, and their clinicians within the health care system. They also learned about the existing evidence supporting photo-narratives, their drawbacks, their user groups, and implementation challenges. Specifically, the teams were given exemplary publications and links to YouTube videos showing lived experiences of children with complex conditions and their families and also reviewed literature relevant to the project.
Step 4: Data collection
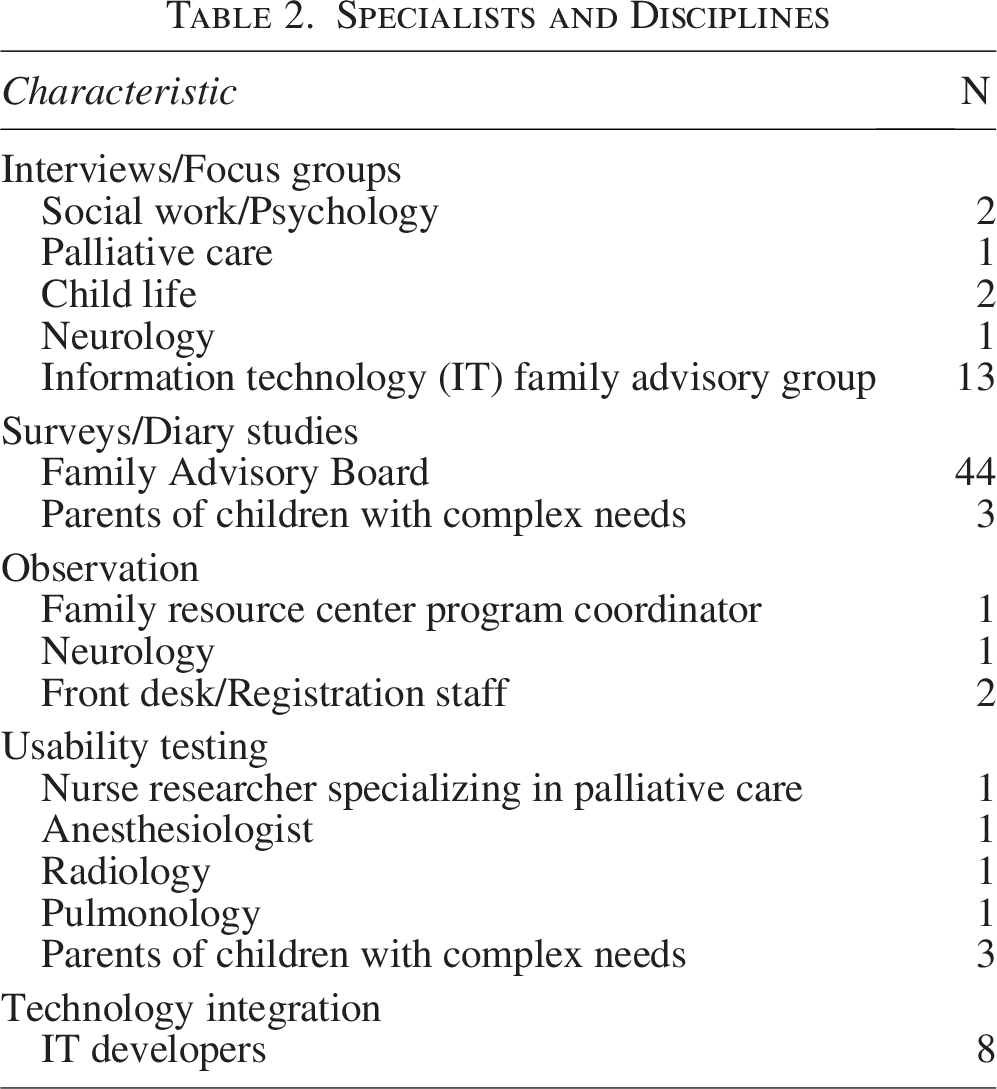
Each team used their own distinct process for their respective designs. Figure 2 shows the data collection timelines and methods each team used. Additionally, Table 2 lists the specialists and disciplines of the various groups that the teams met with during the comprehensive UX research and design process. Throughout data collection, the researchers helped ground and guide the students in developing their interview guides, surveys, and methods that would be most effective in collecting information instructive for their designs. For example, the researchers helped edit the language in their interviews and surveys, insisted on flexible processes to gather data from busy families and clinicians, and guided the students in how to best reimburse parents for survey responses.
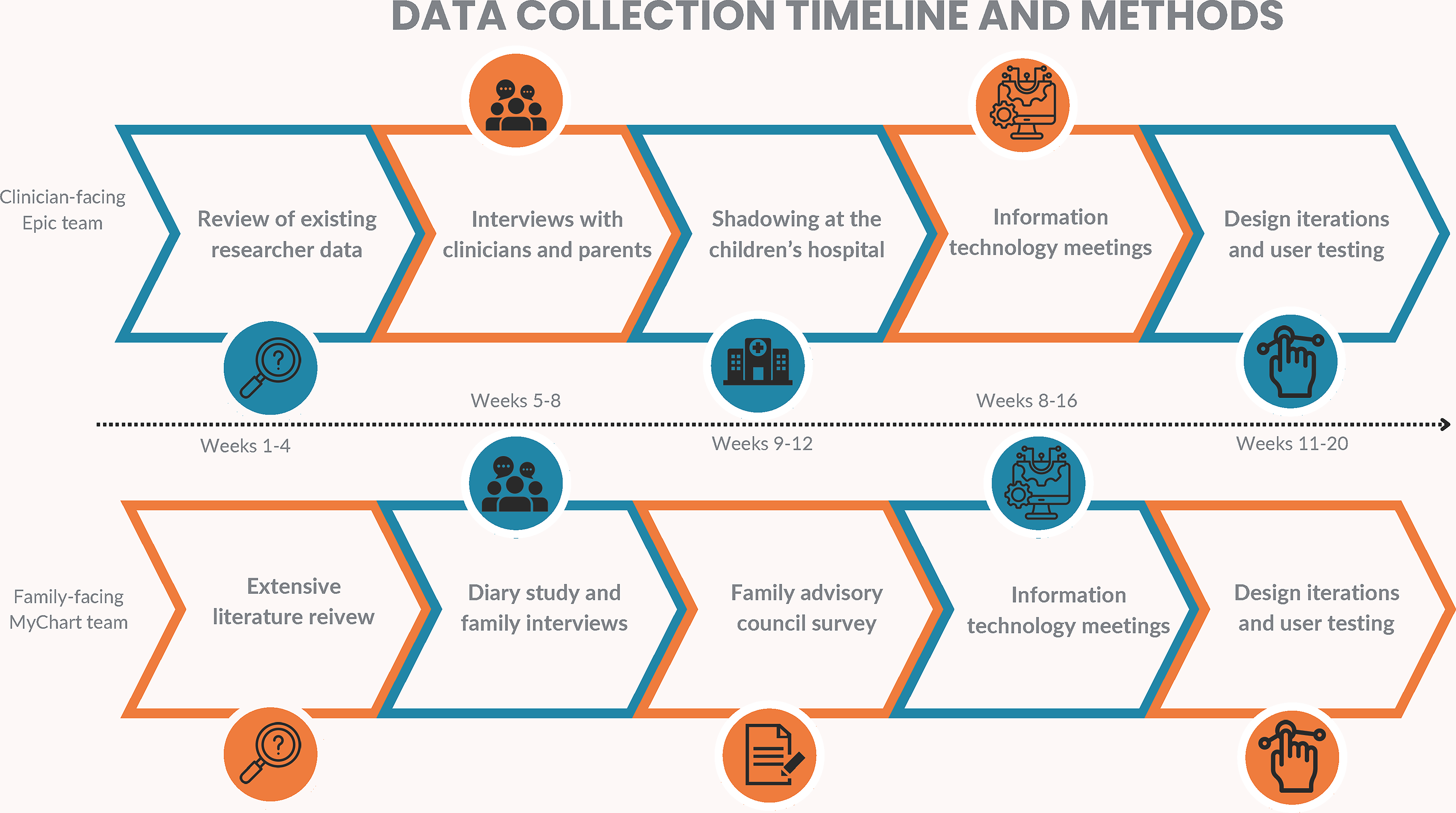
Data collection timeline and methods. This figure outlines the data collection timeline and methods for both UX design teams, including review of existing research data, clinician and parent interviews, shadowing, diary studies, advisory council surveys, IT meetings, and iterative user testing.
Specialists and Disciplines
Specifically, for the clinician-facing Epic integration team, first they reviewed existing coded de-identified data from two of the researchers’ studies that included interviews and brief surveys with families of children with complex chronic conditions and their multidisciplinary clinicians in the intensive and acute care units, respectively. Subsequently, the team also interviewed and shadowed clinicians at the children’s hospital, including (1) front desk clinic and registration staff, (2) physicians in clinic and during inpatient consultations, and (3) child life/family resource center staff (Supplementary Appendix SA1). Conversations with parents of children with complex medical needs from the parent advisory group also informed their design.
For the family-facing MyChart team, they initially completed a diary study with three families of children with complex chronic conditions from the parent advisory group. For the diary study, families were asked to complete a five-minute online survey about their thoughts, feelings, and health care needs each day for four days in a row. They were also asked about what they would want to communicate to clinicians about their child’s health and well-being that day. After the diary study was complete, the team met with each family for an interview to garner a deeper understanding of survey responses. Subsequently, the team created a 15-minute validation survey (Supplementary Appendix SA2) that was sent to the children’s hospital’s family advisory committee to provide feedback on specific design considerations raised by the families in the diary study. Finally, the team synthesized all the data collected to guide the creation of their prototype through the use of user scenarios, journey maps, storyboards, and prototype sketches.
Step 5: Design constraints
The teams used access to the children’s hospital’s Epic and MyChart play environments to understand what the systems looked like from clinician and patient/family perspectives. The teams also met with the children’s hospital family information technology advisory board and the hospital’s information technology development team over a series of meetings to learn about important design considerations and technology constraints going into their initial prototyping. This involved joining existing one-hour meetings with these groups to present the photo-narrative design and to gather suggestions about its use and implementation. These sessions used human-centered design tools, such as interactive collaborative online whiteboards such as Figma and Miro, and methods such as participatory design and brainwriting to gather information and feedback during sessions. During this step, the teams learned about important technology considerations, including data security, data storage, and the many different software programs used throughout the children’s hospital system.
Step 6: Low-fidelity prototyping
After synthesizing these data, the teams each developed their initial prototypes using black and white wireframe renderings that were either hand-drawn, digitally drawn, or created using Figma design software. Key considerations were (1) entry points to enter information and/or view the photo-narrative, (2) ways to simplify the structure and streamline with technological processes children/families and clinicians already use, (3) efforts to provide affordances and signifiers to be self-evident and easy to understand, and (4) design elements to further clinical utility and engagement. Design considerations that were difficult to solve for included efforts to (1) engage overburdened clinicians, (2) show ineffable aspects of the child’s life, and (3) mitigate reliance on technology. These barriers are shown in Figure 3.
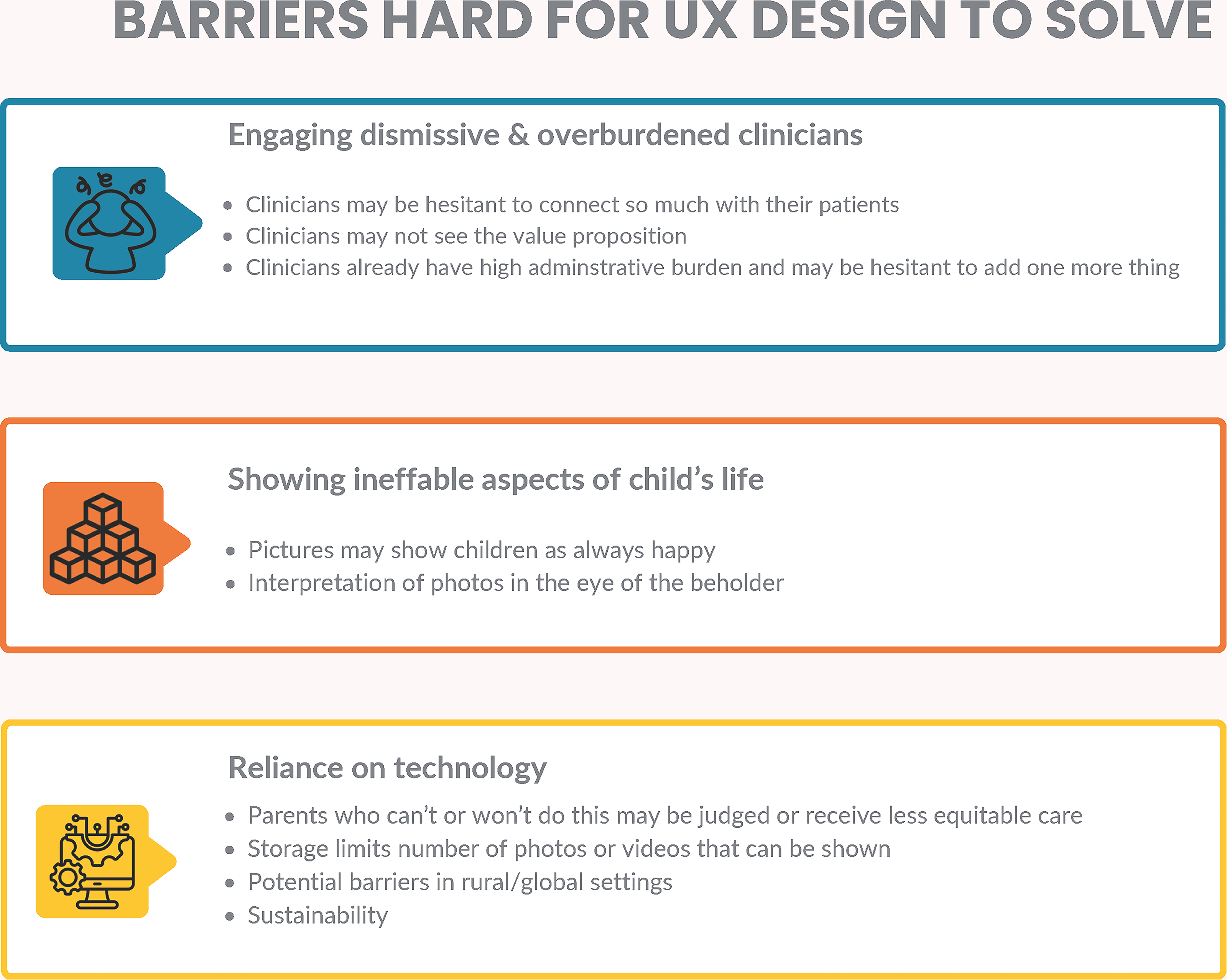
Barriers are hard for the UX design to solve. This figure summarizes key design-resistant barriers identified during the UX process, including difficulty engaging overburdened clinicians, representing ineffable aspects of children’s lived experiences, and challenges related to technological reliance and accessibility. UX, user experience.
Step 7: Usability testing and high-fidelity prototype
Iterative refinement of the prototypes occurred through interviews and discussions with clinical workgroups at the children’s hospital for concept testing and usability testing. Specifically, the teams showed their prototypes across numerous specialties, including palliative care, ethics, neurology, pulmonology, oncology, neonatology, interventional radiology, and anesthesiology. They also included multidisciplinary clinicians such as physical therapists, psychologists, social workers, family resource specialists, child life specialists, physicians, and nurses, as well as parents of children with complex medical needs. Along the way, notes were taken during this process, and adjustments were made weekly to the photo-narrative after discussion with the researchers.
Once the teams had their near-final prototype, they consulted with the children’s hospital marketing and communications department to facilitate branding. This included using colors, icons, fonts, and text styles that would match the hospital’s existing materials. The final prototype from each team was presented at their capstone showcase that was attended by all members of the Human Centered Design and Engineering program, faculty and staff, family and friends, and the general public. Figure 4 shows the low-fidelity and final prototypes.
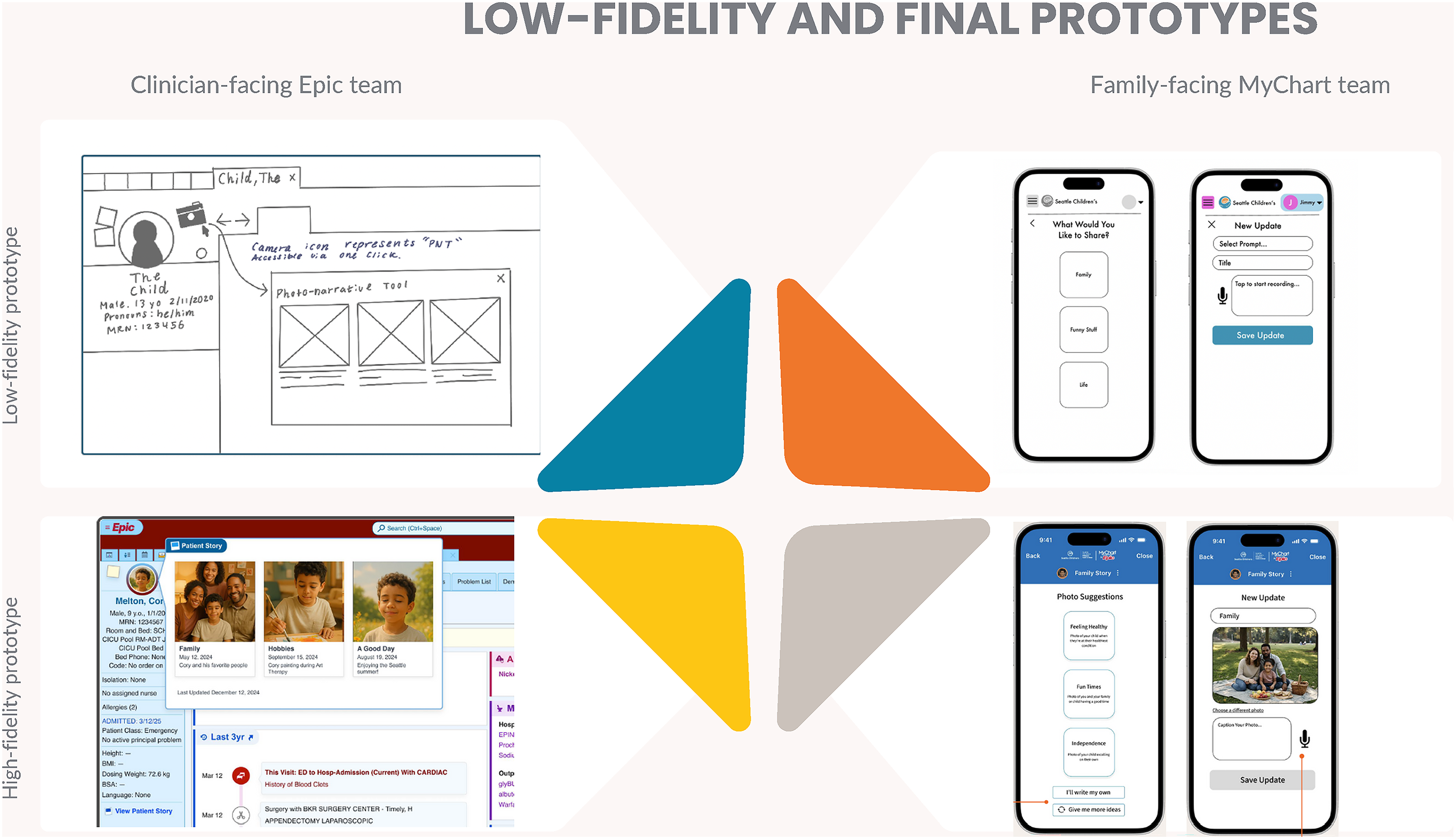
Low-fidelity and final prototypes. This figure compares early low-fidelity wireframes with polished high-fidelity prototypes for both the Epic clinician-facing and MyChart family-facing designs, illustrating the evolution of UI structure, branding, and usability refinements.
Discussion
This collaboration between researchers and graduate students in human-centered design and engineering resulted in high-fidelity prototypes of a photo-narrative intervention to further humanistic care for children with complex chronic conditions, their families, and clinicians. A seven-step process was used to iteratively refine the prototype and tailor the design to support its future implementation in real-world clinical settings.
Through this UX design process, we learned how important it was to children and families that clinicians engaged in the topics included in their photo-narratives. This presented an important design consideration as we determined how to ensure sharing of photo-narratives seamlessly in clinical care. Considerable time was taken on certain design considerations, including entry points to enter information and/or view the photo-narrative, ways to simplify the structure and streamline with processes children/families and clinicians already use, and efforts to make photo-narrative use self-evident and easy to understand with existing technology at the children’s hospital. For example, the initial researchers’ version of the photo-narrative had prompts to stimulate clinician engagement, whereas the final high-fidelity prototype lacked this element. Concerns remained as to how to motivate busy clinicians to discuss the concepts from the photo-narrative with children and families, which UX design did not solve for. Further work is needed to understand how clinician time constraints factor into real-world use of the photo-narrative, how long the intervention takes, and how it works as a possible preventative strategy to avoid communication conflict and ultimately save time.
Additionally, lessons from the UX process included the substantial collaborative learning throughout the design process in developing the data collection tools, reviewing responses, and integrating that information into the next phase of design. Ultimately, the UX design process could not have been achieved by the researchers or the students independently. Specifically, researchers learned about human-centered design methods and resources, while students gained insight into working within health systems and with clinicians and families of children with medically complex needs. Researchers also learned about internal processes, groups, and resources at their own institution that they were not previously aware of, which were pivotal in the data collection and design process. For example, the research team was not aware of the lack of integration of Epic and the GetWellNetwork, 15 which provides interactive software for patients in hospital rooms on iPads and television screens. This also included the importance of branding and design elements such as color and icons that are crucial to effective implementation. As we incorporated more of this into the photo-narrative prototype, users and the children’s hospital’s information technology groups could envision the intervention within their existing systems. We also were intentional to build upon common design elements from other technologies that parents and clinicians were accustomed to using. Specifically, we intentionally incorporated buttons, limited wording to key concepts, and provided ways to customize through entry points and views of the photo-narrative to facilitate its use. Making the photo-narrative visually appealing and engaging was important to both the design and the process of bringing it to the bedside.
In addition, the researchers learned about challenges related to designing for integration with existing information technology infrastructure at the children’s hospital. Since the hospital used numerous technology systems that did not communicate with one another, this required the design teams to select where to focus and provide workarounds to limit the number of applications that the photo-narrative would need to be built within. We decided to design for both Epic and MyChart, and while this may be suboptimal, it met the functional needs of the intervention and maintained the intentional design elements and branding. Families also could share their photo-narrative by uploading photos through MyChart, which would require rigorous privacy and confidentiality protections. These were important issues when we considered implementation of the photo-narrative in other global/cultural contexts that might not have access to these same technologies and platforms. Ultimately, this project illuminated some of the ways in which health care systems are further fractured through health information technology systems, making chronic complex care more difficult. Moreover, it highlighted the imperative that technology should be used to further humanistic practices in health care and not impede them.
Limitations
This project has several limitations. The initial steps of framing the project timeline and deliverables, and completing regulatory and access needs for the graduate students, were time-consuming and administratively demanding. The research team included dedicated project management support, without which this collaboration may not have been possible. The graduate students also had to be persistent in their efforts to obtain proper permissions and committed to the project amid other demands from coursework and their other jobs/obligations. Notably, the students identified several groups and individuals to include in the design process because of their resourcefulness. Initially, we also wondered if having two teams working on linked aspects of the photo-narrative implementation might be difficult. Ultimately. the scope of design was much larger than the researchers had anticipated, and the project benefited from having both teams. Moreover, the amount of research and work each team was able to accomplish was essential and only added value to the UX design. The next steps for this project are for the researchers to work towards the implementation of the photo-narrative at the children’s hospital.
Conclusion
Collaboration between researchers and UX design teams can further the critical intervention design and prototyping essential to implementing successful real-world interventions for children with serious illness, including those with complex chronic conditions, and their families.
Footnotes
Acknowledgments
The authors would like to thank the Center for User Centered Design and Engineering at the University of Washington, with special thanks to the Capstone Program leadership, Melissa Ewing and Dr. Daniela Rosner. The authors also thank the Information Technology Family Advisory Board at Seattle Children’s Hospital.
Author Disclosure Statement
The authors declare that they have no conflicts of interest.
Funding Information
No funding was received for this article.
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.