
Abstract
Background:
Patients with dementia at the end-of-life frequently visit the emergency department. These visits can be distressing for patients and families and challenging for staff.
Aim:
To explore the perspectives of emergency department health care professionals about end-of-life care for patients with dementia in the emergency department.
Design:
Qualitative study using semi-structured focus groups interviews (n = 23). Interviews took place in-person after recruitment via a contact person and were transcribed verbatim. Reflexive thematic analysis was used.
Setting/Participants:
Physicians, nurses, and health care assistants who regularly work at the emergency department of a tertiary hospital.
Results:
Participants’ views on end-of-life care for patients with dementia in the emergency department produced five main themes: (1) the cultural context and perceived place of patients with dementia in the emergency department and in society; (2) the person with dementia—their dignity and multidimensional needs; (3) end-of-life care in the emergency department—managing uncertainty, setting goals, and meeting specific care needs; (4) conditions for supporting the palliative care needs of patients with dementia at the end of life in the emergency department; and (5) ethics and moral distress of health professionals in caring for patients with dementia at the end of life in the emergency department.
Conclusions:
Health care professionals identify strengthening dementia awareness, implementing structured training programs, and improving the physical environment and care models within emergency departments as key priorities for practice.
Key Message
Emergency department health care professionals identified key priorities for improving end-of-life care for patients with dementia. These include raising awareness of dementia among both the public and health care staff, providing structured training, and improving the emergency department environment and care models.
Introduction
Over 55 million people worldwide live with dementia at present 1 and by 2050, this number is expected to reach 139 million. 1 Attendance of end-of-life patients in the emergency department can be distressing for patients and families and challenging for staff.2,3 Care in this setting, frequently includes rapid decision-making, aggressive disease-modifying therapy, 4 long waiting times, lack of communication, 5 bright lights, and constant noise, all which constrain the care provided, specially to vulnerable populations. Specifically, patients with dementia present an increased risk of delirium, falls, cognitive and functional decline, readmission, and death in emergency department visits.6–8 This suggests that the emergency department may not be the best place to properly care for these patients and attend to their specific needs. However, the literature shows that visits to this setting by patients with dementia are high2,9–19 and tends to increase at the end-of-life.13,15,18,19 Furthermore, patients with dementia at the end-of-life have a high prevalence of palliative care needs during emergency department visits,9,20 with uncontrolled symptoms and recent functional decline being some of the most frequently identified needs. 21 While the presence of comorbidities, neuropsychiatric symptoms, previous hospital transfers, and rural living are factors associated to ED visits of patients with dementia at the end-of-life, 22 infections and neuropsychiatric symptoms are the most frequent reasons of ED admissions. 9 Still, despite the complications mentioned, some authors point out that ED can be considered as an opportunity to identify gaps in care of patients with dementia at the end-of-life.23–26 In this setting, access to palliative care seems to be scarce, and the barriers are identified at different levels, 9 including among professionals themselves.27,28 Nevertheless, intervention studies in ED have shown positive results,23–26,29–33 but it remains to be established which methodologies for integrating CP can work best. Overall, the needs of these patients can generate high expectations in patients and families regarding ED care and its professionals. It is unclear whether the response to these needs is already secured or can be provided in the context of the ED. The present study aimed to explore the perspectives and experiences of emergency department health care professionals about end-of-life care for patients with dementia in the emergency department.
Methodology
Design
We drew on an interpretivist/constructivist paradigm 34 to explore what the perspectives on and experiences of health care professionals with end-of-life care for patients with dementia in the emergency department, while recognizing the importance of researcher experience and background in such interpretations. We conducted semi-structured focus groups interviews and followed the six-step approach proposed by Braun & Clarke.35,36 We present this article in accordance with the RTARG checklist 36 (see Supplementary Appendix SA1).
Setting
We proceed to an exploratory study focused on a single center at a university tertiary hospital in Porto, Portugal, which serves a population of 650,000 inhabitants with a polyvalent emergency department, 24 hours a day, 7 days a week. Care is provided by a medical team organized in rotating units—most physicians work in the emergency department once a week, and nurses, and health care assistants’ teams work on a daily basis.
Participants
Inclusion criteria were working in the medical area of the emergency department for at least once/week, providing frequent care for patients with dementia (more than one patient with dementia in each emergency shift) and having more than two years of work experience in the emergency department. The characteristics identified for sampling included profession and experience and, to the extent possible, age and gender, resulting in a predetermined sample size of 6–10 participants per group. To recruit participants from each one of the three professional groups, one staff member (a physician, a nurse, and a health care assistant in leading or management positions) was a “contact person,” informing colleagues about the study and identifying possible candidates. Eligible professionals who showed interest in participating were contacted by the principal researcher (S.V.S.).
Data collection
We conducted semi-structured interviews following a topic guide developed by the principal researcher (S.V.S.), a specialized physician in internal medicine with expertise in palliative care and emergency care. It was then discussed with the other members of the research team and reviewed by another experienced qualitative researcher (JR) at the Unidade Local de Saúde Entre Douro e Vouga. Regarding the research question, the final topic guide version comprised three main topics:
patients with dementia at the end of life and respective palliative care needs, current care for these patients in the emergency department, opportunities and barriers to address the palliative care needs of patients with dementia at the end of life in the emergency department.
Two researchers (S.V.S., JR) piloted the topic guide in two interviews, leading to slight amendments (see Supplementary Appendix SA2). The same two researchers conducted the three focus groups at the point to which no new themes emerged. Interviews were undertaken at the participants’ workplace between June and July 2024 and lasted between 60 and 90 min. Additionally, each interviewee was asked to complete an anonymized and standardized form to collect sociodemographic and professional data.
Focus groups were digitally voice recorded, transcribed verbatim, and anonymized, with field notes taken.
Data analysis
Data analysis followed the Reflexive Thematic Analysis Reporting Guidelines, 36 utilizing NVivo® version 15, to qualitatively explore the perspectives of health care professionals. Considering our clinical and research experience, this allowed us to better explore the complex perspective of health care professionals, from their knowledge to their experiences.
Two members of the research team (S.V.S. and M.B.) independently reviewed the transcripts and derived themes from the data. Consensus coding was developed with both researchers coding the same transcripts and comparing them during regular meetings. Themes were then generated by their shared meaning around a central concept. During the whole analysis process, we gathered feedback from the other members of the research team, and differences in coding and development of themes were further analyzed until consensus was reached.
Ethical issues and approvals
All participants provided written informed consent. The study received approval from the Unidade Local de Saúde de Santo António Ethics Commission and Review Board [reference number 2023.094 (083-DEFI/075-CE)].
Results
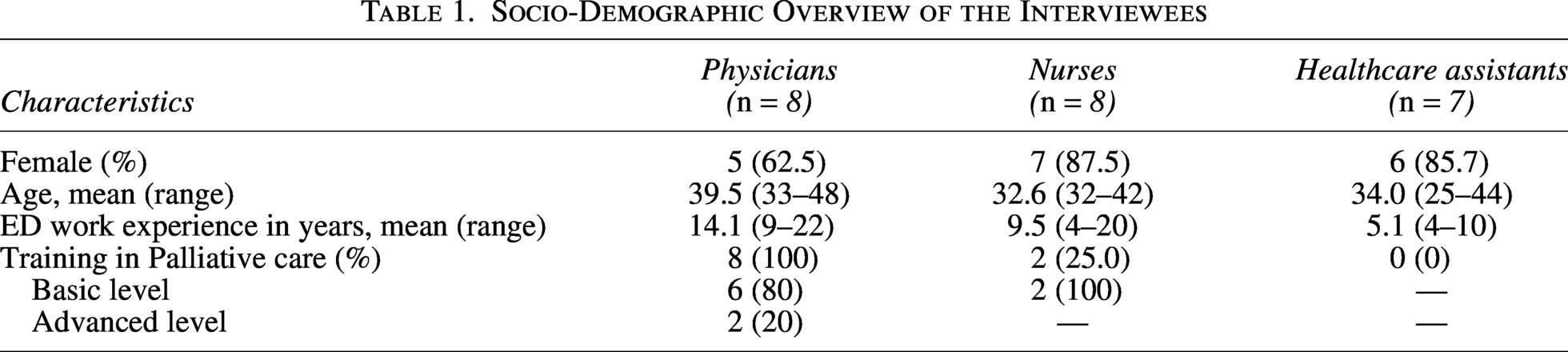
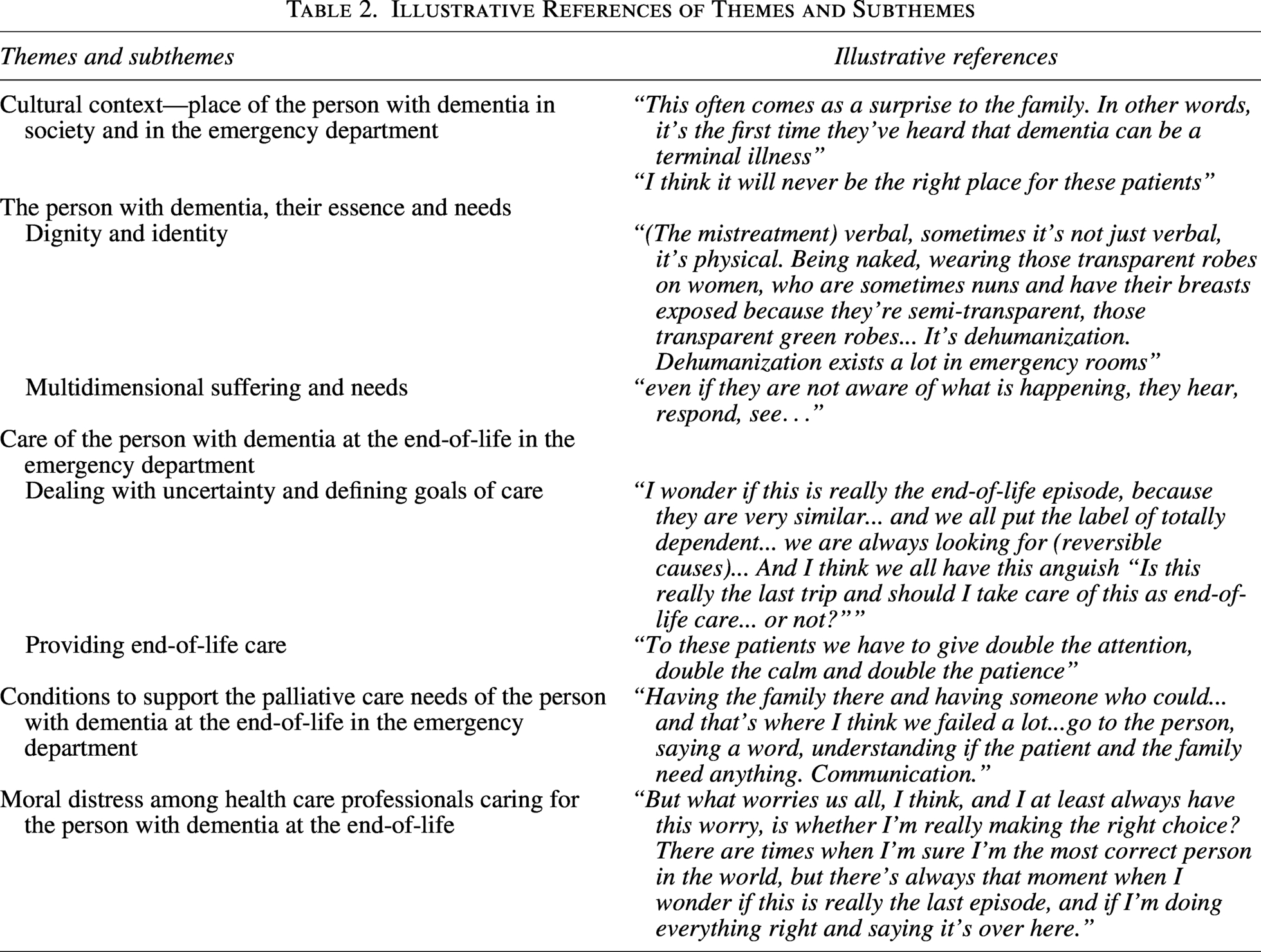
We conducted three focus groups: one with physicians (n = 8), one with nurses (n = 8), and one with health care assistants (n = 7), for a total of 23 emergency department professionals. The majority were female (n = 18, 78.3%) with a mean age of 37.0 years. They presented a mean of 9.8 years of emergency department work experience, and the majority had no training in palliative care (n = 13, 56.5%) (Table 1). Although all professionals had significant emergency department work experience and acknowledged frequently working with patients with advanced dementia in the emergency department, none of the assistants had any palliative care training, unlike all the physicians, who had, mostly, basic training, as did 25% of nurses. Five main themes emerged: (1) Cultural context—place of the person with dementia in society and in the emergency department; (2) The person with dementia; (3) Care of the person with dementia at the end of life in the emergency department; (4). Conditions to support the palliative care needs of the person with dementia at the end of life in the emergency department; and (5). Moral distress in the care of the person with dementia at the end-of-life in the emergency department. The themes, subthemes, and categories derived are presented in the Supplementary Appendix SA3. Illustrative references to themes and subthemes are presented in Table 2.
Socio-Demographic Overview of the Interviewees
Illustrative References of Themes and Subthemes
Theme 1: Cultural Context—Place of the Person with Dementia in Society and in the Emergency Department
The prevailing perspective of health care professionals is that society in general, and the emergency department in particular, are largely unaware of the reality of patients with dementia. The natural history of dementia, the needs of these patients, and care demands are generally unknown.
“This often comes as a surprise to the family. In other words, it’s the first time they’ve heard that dementia can be a terminal illness” (P1)
Caregiving experiences, whether by family or professionals, shape caregivers’ knowledge and capacity. Health care assistants note that the (mis)treatment of patients with dementia at the end-of-life in the emergency department reflects broader societal attitudes, including assumptions of impaired relational capacity and loss of identity.
“Well, because dementia is considered: “Oh, he has dementia…put him aside.” It’s true: “He doesn’t know what he’s saying, he’s put to the side a bit.” “We waste time with someone who doesn’t know where they are, don’t know what they want?” It’s true, it’s a reality we live in today in the emergency department.” (H1)
Most respondents noted that the fast pace of life limits caregiving and drives patients with dementia to the emergency department, with hospital, remaining the dominant perceived place of death.
“It’s a cultural issue, nobody has time…lately we have never seen so many patients with dementia as end-of-life social cases that stay in the ED” (N1)
Respondents viewed the emergency department as unsuitable for end-of-life care of patients with dementia due to its curative focus, linking this to risks of overtreatment and displacement from the community, while nurses stressed that care is overly hospital-centered and patients with dementia are routinely deprioritized.
“I think these patients don’t get the priority they deserve because “they’re at the end of their lives and destined to die, so let’s treat others that are for investment”.” (N1)
Physicians noted that dementia is often not recognized as terminal, affecting end-of-life care. Respondents from all groups reported that cognitive changes and memory limitations may protect the patient from the suffering they experience. On the contrary, severe psychomotor agitation often leads to the almost normalized use of physical restraints.
“Unfortunately, society still can’t fully grasp the need to restrain someone.” (H2)
These perspectives reflect a broader unawareness, and at times invisibility, of patients with dementia in the emergency department, reinforcing the sense of non-belonging and the belief that the emergency department is ill-suited to their care, potentially causing more harm than good. Community-based care is considered the most appropriate form of assistance for these patients.
“I think it will never be the right place for these patients”. (N2)
Surprisingly, all professional groups acknowledged that the emergency department offers opportunities to identify advanced disease and palliative needs, facilitate communication with families and caregivers, and establish goals of care for patients with dementia.
“But (in the emergency department) you have the opportunity to identify a patient and their symptoms.” (P2)
Finally, not only is the emergency department often the patient’s gateway into the health care system, but all professional categories recognize that the emergency department is a place for direct care, especially for comfort during the management of physical symptoms and to address some of the caregivers’ needs.
“(emergency department) It’s the entry point (to the healthcare system).” (H3)
“Yes. (In the emergency department we provide) Comfort, hydration and hygiene. Body care.” (H4)
“Yes, symptom control, despite everything…it may not be in the most effective time, but we eventually get there. We control the agitation; we control the pain…we manage to involve the family” (N2)
Theme 2: The Person with Dementia, Their Essence and Needs
Dignity and identity
In both nurses and health care assistants’ groups, the perspective on dignity is based on each person’s ability to relate to others. For patients with dementia at the end-of-life, who frequently experience communication and relationship limitations, their dignity is embodied in the human presence and care, by the health care professionals and family—by not being alone.
“Because [as family members complain] “my father died alone, my mother died alone, I couldn’t be with her”. That’s inhumane.” (H2)
These two professional groups demonstrate ambivalence regarding their understanding of dignity in patients with dementia, specifically, whether living can be considered the same as existing. They attribute dignity as external to the person and not as intrinsic to the patients with dementia at the end of life.
“They (patients with dementia) can’t communicate, they no longer recognize themselves, they often don’t even speak to their family members, and from then on, they can also become more dependent on self-care in daily life. And we end up wondering what are the benefits” (N2)
Physicians seem to incorporate the idea of dignity as stemming from how patients with dementia are treated—the language used, how their body is cared for. They suggest that dehumanization is the antithesis of dignity and that the dignity of life of patients with dementia at the end of life depends on their ability to relate to others, to communicate and of self-care.
“(The mistreatment) verbal, sometimes it’s not just verbal, it’s physical. Being naked, wearing those transparent robes on women, who are sometimes nuns and have their breasts exposed because they’re semi-transparent, those transparent green robes… It’s dehumanization. Dehumanization exists a lot in emergency rooms” (P3)
Multidimensional suffering and needs
All three groups identify suffering of patients with dementia at the end of life as multidimensional. At a physical level, eating-related problems stand out due to their frequency and complexity of approach.
“Eating is always everyone’s biggest problem.” (P1)
Aspiration, weight loss, and pressure ulcers are highlighted, and all groups recognize the total dependency of these patients. Health care assistants focus on behavioral issues, nurses and physicians on fragile interpersonal relationships, while all value family involvement—assistants for managing agitation and feeding; nurses for supporting the patient-family relationship; and physicians for addressing complex family communication and representing the voice of the patients with dementia.
“I often ask family members if they’ve ever talked about what they want? And the answer is always a surprise, ‘No, but why would anyone ever ask?’” (P4)
Recognition of spiritual needs appears to be almost exclusively centered on the importance of religion and its disregard in the emergency department, particularly among physicians.
“The other issue has to do with religion, because I think we are also there to facilitate religious support, but we often end up ignoring it.” (P5)
The health care assistants emphasize the importance of continuing to see the patient as a person and acknowledging gratitude. Nurses stress the importance of adapting the measures instituted to the condition of advanced disease—quality of life as the priority.
“even if they are not aware of what is happening, they hear, respond, see…” (H4)
“Most of the time, they’re affectionate because we turn them around and they put their hands on our waist, grab our arms. I think it’s a way of showing gratitude.” (H7)
Theme 3: Care of the Person with Dementia at the End-of-Life in the Emergency Department
Dealing with uncertainty and defining goals of care
Physicians explicitly acknowledge uncertainty, linking it to prognosis and decision-making. Emergency department constraints—time pressure, limited patient communication, scarce information, and lack of advance care planning—exacerbate this, while family expectations to “do everything” increase pressure, often leading to defensive decisions to “do more.”
“I wonder if this is really the end-of-life episode, because they are very similar… and we all put the label of totally dependent… we are always looking for (reversible causes)… And I think we all have this anguish “Is this really the last trip and should I take care of this as end-of-life care… or not?”” (P2)
Nurses believe that uncertainty is amplified by the lack of clear decisions from physicians. They emphasize the need to define goals of care to adapt and avoid disproportionate care.
“Sometimes completely unnecessary procedures are performed. Blood cultures, for example. It’s a struggle…(Physicians need to) Decide once and for all whether to invest or not… because if not, I’ll stick a catheter in, and, and…” (N3)
They suggest the implementation of identification protocols, some even decision-making protocols. However, they do not propose a method of person-centered care and shared decision-making. For health care assistants, uncertainty is directly related to the interpretation of the behavior of patients with dementia.
Providing end-of-life care
All groups agree that patients with end-of-life dementia have profound communication limitations, total dependence, positioning needs, and frequent feeding difficulties. At the same time, they consider that recognition of these needs is low and that responses from the ED are inadequate; they emphasize the importance of sufficient professional time and availability to meet these needs.
“To these patients we have to give double the attention, double the calm and double the patience” (H4)
Physicians emphasize that to effectively manage these patients, they must be proficient in identifying the often-challenging end-of-life situation. This group, along with nurses, highlights the importance of having a more dedicated area of the emergency department for caring for patients with dementia—calm environment, privacy, and trained professionals are key features.
“Area dedicated to optimizing the care provided to patients with terminal dementia. And the dedicated team assigned to this area should have minimum training for this.” (P4)
Nurses stress that it is beneficial to review unnecessary therapeutic proposals, especially invasive procedures, and that adequate treatment of agitation must be ensured, minimizing situations of physical constrain.
“There must be a review of treatments and there must be no unnecessary and invasive nursing procedures.” (N4)
All professional groups recognize that patients with dementia at the end of life in the emergency department benefit from family support. Health care assistants add that human contact from professionals is as important as comfort and body care.
Theme 4: Conditions to Support the Palliative Needs of the Person with Dementia at the End-of-Life in the Emergency Department
Professionals simultaneously present the perspective that patients with dementia at the end of life in the emergency department cannot see their dignity respected, and the conditions that the emergency department should have to safeguard their dignity.
“Dying in the emergency department is not dignified…but there are situations that are not avoidable and that we cannot offer more…” (P3)
Whether for decision-making or communicating and caring, extra time is considered essential. Greater awareness among families and better conditions to allow family presence, and especially greater knowledge among emergency department professionals about these patients and their needs, is highlighted.
“Having the family there and having someone who could…and that’s where I think we failed a lot…go to the person, saying a word, understanding if the patient and the family need anything. Communication.” (N1)
More competent professionals are needed, with appropriate attitudes and communication skills.
“In-hospital palliative care teams will likely have to consider the need for increased emergency room response.” (P1)
Finally, a greater response from community care, before or after the use of the emergency department, is highlighted by physicians and nurses.
“And maybe if this home support in the community worked… because I know that in some places it exists… maybe those patients wouldn’t need to go to the emergency room as much. Maybe they wouldn’t end up here.” (N4)
Theme 5: Moral Distress Among Emergency Department Health Care Professionals Caring for the Person with Dementia at the End-of-Life
The need for ethical consideration and the moral distress of professionals that arises “when one knows the right thing to do, but institutional constraints make it nearly impossible to pursue the right course of action,” 37 emerged across practically all topics covered in all focus groups. Because the human experience cannot—and should not—be separated from the professional role, society’s understanding of end-of-life and death, and the suffering it evokes in those who accompany it, appears to be a key, cross-cutting factor contributing to professionals’ moral distress.
“I think it’s a lot, not just because of the work, but because of fear of getting involved or because of… all of us who face death…” (N4)
The awareness that it is impossible to respond to every situation with the same quality, combined with the understanding that empathy fluctuates, reinforces concerns that patients with dementia may not always be treated with full dignity. The arising process of dehumanization is seen as inevitable, even defensive, by some, while others say it must necessarily be countered.
“Dehumanization exists—there’s the ignoring, the looking ahead, we go down the hallway and don’t want to see what’s going on because there’s a patient there screaming…Absolutely, but what I mean is that sometimes we have to realize that there’s a man there pulling on the IV line… it’s up to us to intervene” (P2)
More specifically, decision-making is the most challenging aspect listed by the group of physicians. Managing uncertainty, fear of harm, limited alternatives, and the need to monitor progress, compounded by the emergency department’s limited response time, are the main causes of distress identified.
“But what worries us all, I think, and I at least always have this worry, is whether I’m really making the right choice? There are times when I’m sure I’m the most correct person in the world, but there’s always that moment when I wonder if this is really the last episode, and if I’m doing everything right and saying it’s over here.” (P3)
Health care assistants report distress when using physical restraints despite protective intentions, frustration at feeling undervalued by other professionals, and the ongoing psychological burden of working under such conditions.
“It breaks my heart to have to restrain them.” (H5)
“Because there’s a certain lack of credibility among nurses and assistants, because I speak for myself; I’m not there just to help patients urinate…we’re the ones who have to call the nurses because that person isn’t well or…” (H5)
“So, where’s the psychological support for us?” (H6)
Discussion
This exploratory analysis of the emergency professionals’ perspectives on dementia end-of-life care revealed five key themes. The way society views dementia suggests that people living with it are often misunderstood and do not clearly fit into places like emergency departments or even wider society; this emerged in one theme named “Cultural context—place of the person with dementia in society and in the emergency department.” Dignity is understood through interpersonal relationships and treatment, while suffering is recognized as multidimensional. End-of-life care in the emergency department poses challenges in managing uncertainty, defining goals, and addressing specific care needs. Professionals navigate a dual perspective, recognizing both the emergency department’s limitations in safeguarding dignity and the conditions required to enable it. Across all groups, ethical considerations and moral distress emerge when institutional constraints hinder provision of appropriate care. 37
While the emergency department is often seen as unsuitable for patients with dementia at end-of-life, professionals acknowledge that these patients frequently present with significant needs. This perspective is aligned with the reality that the hospital is the main place of death in many developed countries 38 and emergency department visits by patients with dementia at the end of life have increased.13,15,18,19 Raising awareness and fostering environments that promote positive behaviors toward patients with dementia have been identified as important strategies. 39 Furthermore, the transfer of end-of-life care for patients with dementia to community settings, as suggested by respondents, is already recommended for this population. 40 Regardless, the emergency department can play a fundamental role in determining the goals of care of patients with dementia, in discussing prognosis and initiating palliative care,41,42 all of which are central aspects of end-of-life care.
The understanding of dignified treatment for patients with dementia in the emergency department appears diverse, encompassing both intrinsic and extrinsic aspects. Lindwall et al 43 reviewed perspectives on dignity in clinical practice and emphasized its recognition through respect, acknowledgment, and supportive community contexts. In the emergency department, health care professionals perceive the needs of patients with dementia as multidimensional, with feeding and eating difficulties posing challenges, consistent with findings by Sharma et al 44 linking dementia severity to caregiver distress during mealtimes. The family emerges as a key partner in end-of-life care for patients with dementia in the emergency department, requiring special attention in communication. This is consistent with previous evidence 31 that insufficient support for families may compromise the quality of end-of-life care.
Interestingly, uncertainty was acknowledged by all groups of health care professionals and as a multidimensional reality in end-of-life care for patients with dementia in the emergency department. Uncertainty was assumed in the establishment of prognosis by physicians, in how to care according to goals of care by nurses, and the understanding of what patients feel and think by health care assistants. This perspective seems quite in line with the concept of total uncertainty previously described by Etkind et al, namely, the multidimensional experience of unpredictability in serious illness, encompassing disease, health care, relational, and existential domains. 45 Uncertainty has been associated with increased resource utilization and higher rates of burnout. 46 Proper identification of the often-challenging end-of-life situation and a model of person-centered care and shared decision-making are recommended. 47 Addressing better end-of-life conditions in the emergency department was also emphasized. Proposals include education and communication training as previously recommended, 48 improving physical conditions, with an emphasis on privacy, silence, and a calm environment, and improving organizational aspects as access to information, developing specific protocol for identifying and/or treatment of patients with dementia at the end of life, psychological support, and prior and early referral to palliative care. Complementary and integrative palliative care approaches in the emergency department have yielded positive results, 49 although with uncertainties about the best models. Finally, the recurring reference throughout the interviews to the moral distress of professionals deserves our attention and is known50–53 to benefit from an approach to support professionals in the different levels at which this suffering arises. Strategies to improve person-centered care and shared decision-making are expected to help support health care professionals. 47
Strengths and limitations
The group of professionals interviewed share extensive experience working in the emergency department and has diverse training in palliative care, which mirrors many emergency departments. The researchers, with experience in both these contexts, facilitated reflection and subjectivity analysis of their perspectives. There are also limitations, namely the fact that this is an analysis of a single center, possiblely influenced by the local cultural context either in terms of the patient population and the attitudes and practices of the health care professionals. In addition, the recruitment methodology in which the contact person may have suggested certain interlocutors based on prior knowledge of some of their perspectives, and also there is a known risk of professional and social bias on the part of professionals who may tend to present a false positive image. Finally, respondents used their own definitions about patients with dementia and end-of-life.
Conclusion
The perspectives of emergency department professionals reflect a broader context of limited awareness of dementia and a perception that patients with dementia do not fully belong in the emergency department. Nevertheless, emergency department resources are essential and can provide important opportunities to address some end-of-life needs of these patients. Despite structural and organizational constraints, it is essential to ensure an appropriate place for patients with dementia in the emergency department at the end of life. Priorities for practice include raising awareness of dementia in society through greater general knowledge about patients with this disease but also greater recognition by health care professionals of their needs at different stages, including at the end of life. At the same time, consideration should be given to implementing structured training programs for health care professionals and improving the physical environment and care models in emergency services. Applying the Platinum Rule 40 “doing unto patients as they would want done unto themselves” can guide more person-centered responses. Closer coordination with families, community services, and palliative care teams is also critical to ensure continuity and quality of care. Finally, systematic support mechanisms are needed to address and mitigate the moral distress experienced by emergency department professionals in providing end-of-life care for patients with dementia. We believe that these perspectives, although limited to the opinions of different professional groups within a single ED, point to possible interventions to improve the quality of care provided to patients with dementia at the end-of-life. These results highlight a potential opportunity for intervention in this particular ED while also supporting the rationale for future multicenter investigations.
Authors’ Contributions
Study concept and design: S.V.S., C.T., and B.A. Acquisition of data: S.V.S. and J.R. Analysis of data: S.V.S. and M.B. Interpretation of data: all authors. Drafting of the article: S.V.S. and M.B. Critical revision of the article for important intellectual content: all authors.
Footnotes
Acknowledgments
The authors thank all the health care assistants, nurses, and physicians who shared their experiences and views in the interviews and focus groups. In addition, they thank the contact persons at the participating centers for supporting the recruitment of participants. Finally, they thank Joana Rente (JR) for her contribution as an experienced qualitative researcher during the interviews.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.