
Abstract
Background:
Chronic obstructive pulmonary disease (COPD) has an unpredictable trajectory and high symptom burden, complicating end-of-life (EOL) decisions around place of death and hospice use. Little is known about how families navigate these decisions.
Methods:
We conducted semi-structured interviews with bereaved caregivers of people with COPD who received pulmonary care at a U.S. academic center and died within 12 months. Two investigators performed template analysis to identify themes.
Results:
We interviewed 18 caregivers (median age 58; 50% Black; 89% female). Fifty-six percent of decedents received hospice; 33% died at home. Caregivers described five themes: missed prognostic cues and poor communication; hospice as both loss and relief; home as ideal but hospital as default; financial influences on decisions; and mismatch between hospice and COPD needs.
Conclusions:
Caregivers identified a readiness gap driven by prognostic uncertainty, communication challenges, and financial constraints. Clearer communication and hospice models better aligned with COPD are needed.
Key Message
Family caregivers of people with chronic obstructive pulmonary disease (COPD) described a readiness gap in end-of-life decision making, marked by delayed communication, crisis-driven hospice referral, and limited support for home death. Addressing this gap will require earlier conversations and hospice models better aligned with COPD’s prolonged and unpredictable course.
Introduction
Chronic obstructive pulmonary disease (COPD) is a leading cause of morbidity and mortality, marked by functional impairment and high symptom burden near the end of life (EOL).1–3 Prognostication in COPD remains challenging because of its unpredictable illness trajectory with periods of stability punctuated by acute exacerbations with partial recovery, making it difficult to prepare for EOL.4–7
Although hospice improves comfort, caregiver support, and reduces intensive care utilization, people with COPD are less likely than those with cancer to receive hospice (39.0% vs. 59.5%). 8 When they enroll in hospice, they do so later and have higher odds of live discharge, including from hospitalization or loss of hospice eligibility.9,10 Designed around cancer trajectories, the Medicare hospice benefit requires forgoing disease-directed care during the terminal phase, which is often difficult to identify in COPD. Hospice was also designed to support dying at home, with limited inpatient coverage. 11 Although most individuals prefer a home death and home deaths in COPD have increased to 35% in recent years, caregivers are often unprepared for the reality of EOL care at home and unaware of hospice limitations.12–14 To better understand these disparities, we conducted a qualitative study of bereaved caregiver perspectives on hospice use and place of death in COPD.
Methods
Sample
We conducted semi-structured interviews with English-speaking unpaid caregivers ≥21 years old of people with COPD who had been seen in Emory Healthcare pulmonary clinics and died within the past 12 months of respiratory-related causes as determined by chart review. Decedents were identified through electronic medical record review using COPD-related International Classification of Diseases-9/10 codes, with spirometry-confirmed airflow obstruction (forced expiratory volume in one second/forced vital capacity <0.70). 15 During the intake call, we confirmed the cause and place of death and identified the family member most involved in caregiving to determine eligibility.
Participant recruitment and interviews
Eligible participants received an opt-out letter and were then called by a research coordinator (C.P.V.). Participants provided informed consent prior to the interviews. The Emory University Institutional Review Board approved this study (STUDY#00004710).
The interview guide (Supplementary Data) was developed through literature review and expert input, pilot-tested for clarity, and informed by the Theory of Dyadic Illness Management, 16 which conceptualizes illness as a shared patient–caregiver experience. Interviews were conducted by phone or videoconference between April 2024 and February 2025 and lasted approximately one hour. All interviews were professionally transcribed via human transcription (Rev.com). All interviews were conducted by a pulmonary and critical care clinician (N.S.) with formal training in qualitative research.
Qualitative analysis
We conducted template analysis, combining predefined codes from existing literature with inductive coding to develop themes. 17 Two investigators (N.S., T.B.) independently reviewed transcripts, refined the coding framework iteratively, and double-coded all transcripts using MAXQDA. 18 To maximize validity and trustworthiness, we used team-based development of the interview guide and codebook, probes, ongoing transcript review, consensus of final coding, and member checking with a lay summary of this article sent to participants for feedback.19,20 Reflexivity was addressed through team discussions of how clinical and caregiving perspectives shaped interpretation. This study adhered to the Consolidated Criteria for Reporting Qualitative Research checklist (Supplementary Table S1). 21 The final sample size was determined by thematic saturation. 22
Results
Of 114 bereaved caregivers mailed recruitment letters, 96 were excluded (primarily due to inability to contact) and 18 enrolled (Supplementary Fig. S1). Participants had a median age of 58 years (interquartile range 53–69); 50% were Black, 89% were female, and 50% were adult children (Table 1). Approximately half of decedents received hospice, and 33% died at home. Illustrative quotes are shown in Table 2.
Sociodemographic Characteristics of Bereaved Caregivers and Decedents
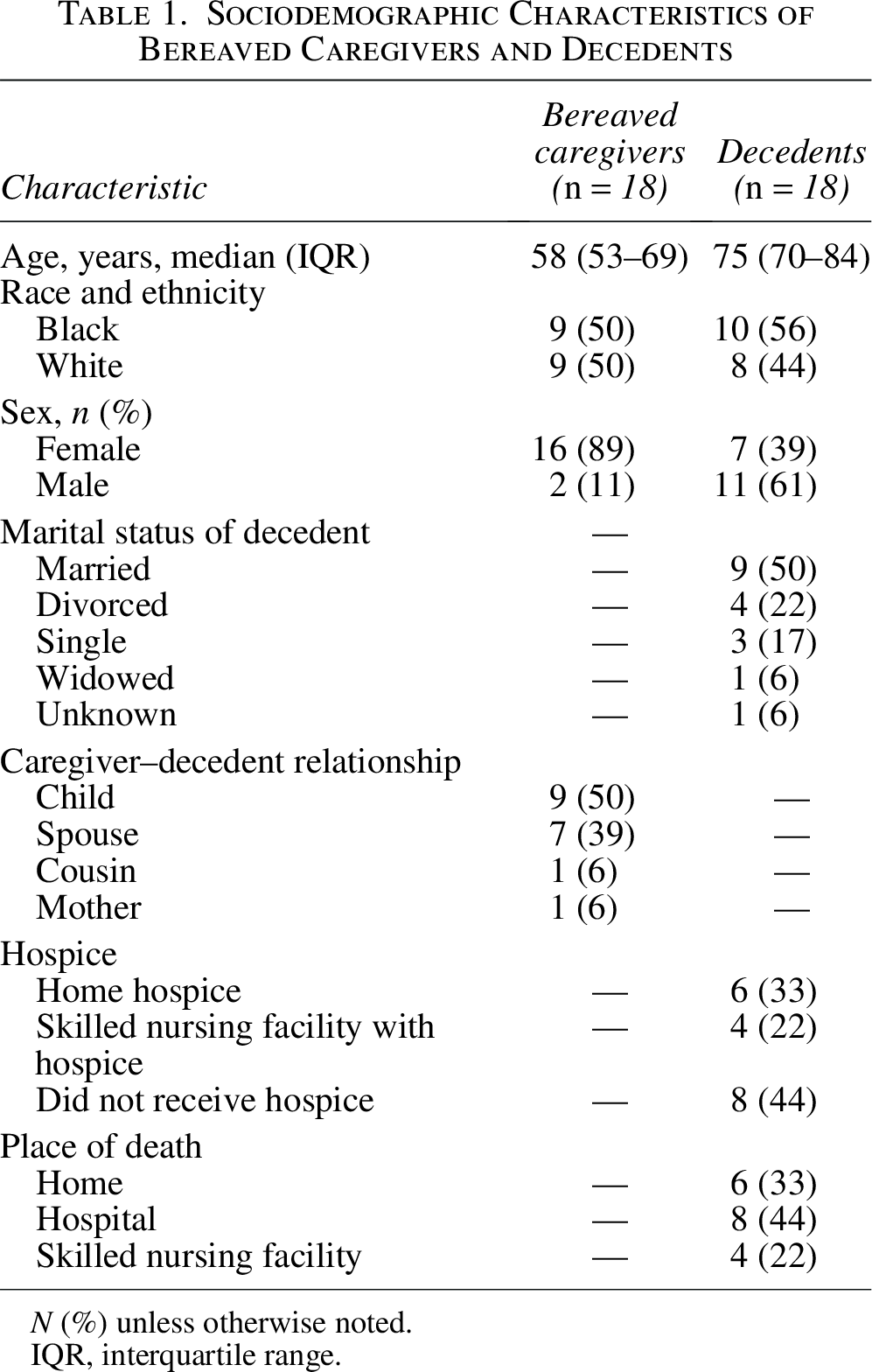
N (%) unless otherwise noted.
IQR, interquartile range.
Illustrative Quotes for Each Theme
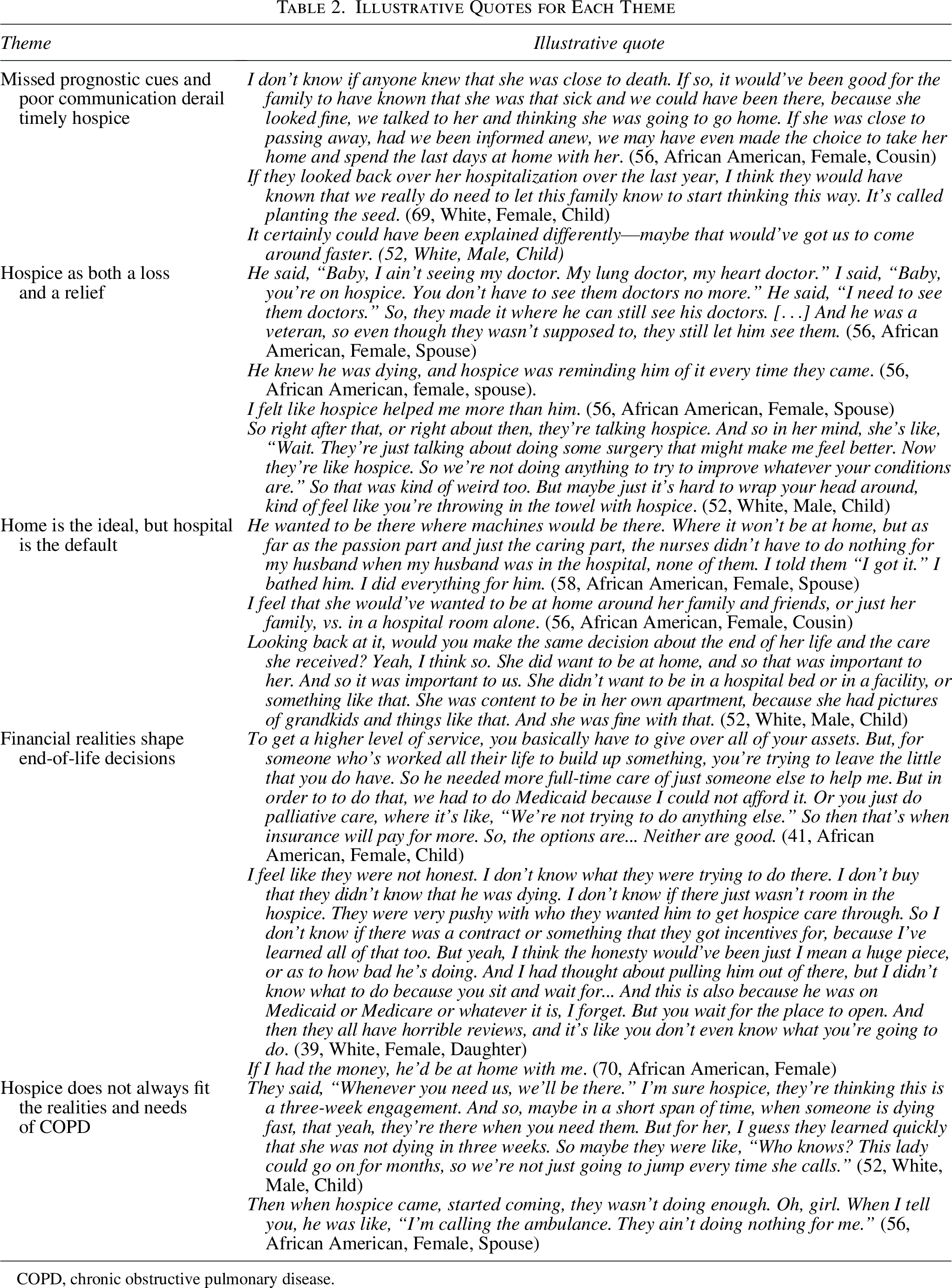
COPD, chronic obstructive pulmonary disease.
Missed prognostic cues and poor communication derail timely hospice
Caregivers described how limited prognostic awareness, emotional avoidance, and inconsistent clinician communication left them unprepared for timely EOL decisions. Many said no one clearly communicated that death was approaching, even as functional status declined and hospitalizations increased, leaving families expecting recovery rather than preparing for rapid decline. Conversations about avoiding life-sustaining treatments often occurred during hospitalizations rather than through ongoing outpatient planning.
A readiness gap emerged, with families lacking the information needed to recognize approaching EOL (Fig. 1). Inconsistent communication caused confusion: clinicians reassured families about improvement, only to recommend hospice weeks later. Many described crisis-driven transitions, including recurrent breathing episodes and 911 calls, that prompted hospice discussions. Misunderstandings that hospice was limited to facilities or the final days further widened this gap. Caregivers recommended earlier, clearer explanations, including framing hospice as a flexible service that could be initiated and discontinued if goals changed.
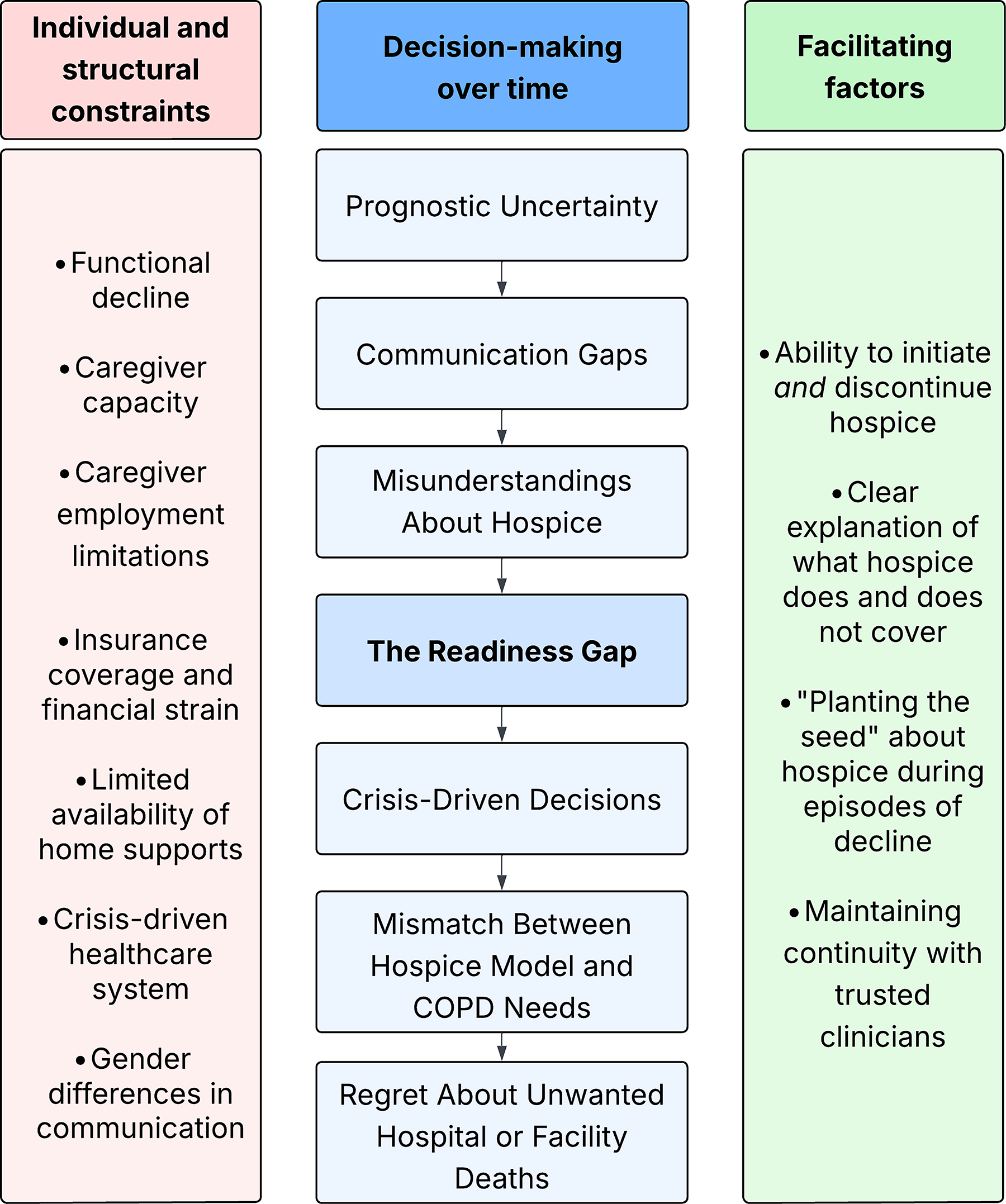
Caregiver pathways contributing to the readiness gap in end-of-life decision making in chronic obstructive pulmonary disease.
Hospice as both a loss and a relief
Accepting hospice often felt like “throwing in the towel” after years of fighting to preserve health and independence. Caregivers described difficulty shifting from active treatment to comfort-focused care, particularly when patients were still taking familiar medications or seeing their usual doctors. Some described hospice visits as a painful reminder of dying.
At the same time, hospice brought relief from physical, logistical, and emotional burdens. Families valued reduced treatment burden, symptom management for breathlessness and anxiety, and support with oxygen, medications, and bathing.
Home is the ideal, but hospital is the default
Most caregivers shared that their loved one would have preferred to die at home, describing home as a place of comfort, familiarity, and control. However, hospital or facility deaths often occurred by default, driven by medical crises, limited caregiving resources, and structural barriers such as inaccessible housing. Some caregivers recalled that only facility-based hospice was offered. In some cases, families faced discordant preferences: patients wanted to remain home, whereas caregivers felt unable to manage home care. Many expressed regret about unwanted hospital deaths, whereas those who achieved home deaths expressed none.
A minority of caregivers noted that some decedents preferred the hospital setting, finding reassurance in access to medical care and equipment. When families could remain actively involved in caregiving, even hospital settings could preserve the connection and comfort decedents sought at the EOL.
Financial realities shape EOL decisions
Cost shaped decisions about where and how patients died. Some caregivers said that with adequate resources, their loved one would have died at home. Many caregivers described trade-offs between unpaid caregiving, hiring private aides, and facility placement. Private in-home help was often unaffordable, whereas hospice was typically covered.
As a result, hospice was often chosen out of financial necessity rather than preference, leading to disappointment when support fell short of expectations. Caregivers who hoped to keep loved ones at home described needing extensive, unaffordable assistance while facing lost wages or job insecurity. In contrast, comprehensive insurance coverage eased financial anxiety by fully covering hospitalizations and medications.
Several caregivers noted that clinicians rarely discussed the financial implications of EOL options, leaving families to navigate insurance rules and hidden costs on their own. Financial strain also eroded trust, with some questioning whether clinicians or facilities had incentives to promote certain hospice agencies.
Hospice does not always fit the realities and needs of COPD
Families wanted a more responsive nursing presence, respiratory symptom management, and physical therapy to maintain function. Some said the limited number of home visits felt inadequate given how much hands-on help patients required, and that they still performed most caregiving tasks: monitoring oxygen, assisting with transfers, and managing breathing crises. Caregivers also emphasized a disconnect between assurances of 24/7 availability and the reality of delayed responses, especially when patients lived longer than expected.
Discussion
We identified a readiness gap, in which bereaved caregivers often lacked information, emotional preparedness, and system-level support to recognize when hospice was appropriate in COPD. Financial constraints and limited home support further shaped where and how patients died. Once enrolled, hospice eased physical and logistical burdens but required relinquishing access to trusted clinicians and hospital-based care during exacerbations.
Our findings suggest that delayed hospice use in COPD stems from unclear prognostic communication, misconceptions about hospice, and a mismatch between hospice structures and the prolonged, crisis-prone illness course. These findings extend prior research showing that individuals with COPD are less likely to receive hospice and tend to enroll later than those with cancer.9,23 Our study illuminates why the fluctuating COPD course complicates prognostication, and the prolonged need to manage dyspnea crises and oxygen dependence at home exposes limitations in traditional hospice structures.
Strengths include purposive sampling of a sociodemographically diverse cohort, with half identifying as Black, and rigorous qualitative methods that enhanced trustworthiness. A single site may limit generalizability, although caregivers were recruited from three different clinics. The modest response rate may introduce selection bias. Retrospective accounts may cause recall bias, although enrollment was limited to deaths within the prior year.
Caregivers recommended that clinicians frame hospice as a flexible, supportive service that can begin early and be discontinued if goals change, clearly explain the level of support it does or does not provide, and correct misconceptions that hospice requires facility-based care. At the system level, policies should adapt hospice for noncancer disease, including longer enrollment periods, home-based supportive services, and concurrent care, which may serve as a psychological bridge for families reluctant to forgo disease-directed treatment. 24 These adaptations would align hospice care with the lived experience of families facing advanced respiratory illness.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
N.S. is funded by the Georgia Clinical and Translational Science Alliance (UL1TR002378 and KL2TR002381) and the National Heart, Lung, and Blood Institute (NHLBI) Loan Repayment Program (L30HL170378). S.H.C. is funded by the NHLBI (1K01HL175212-01A1). D.K. is funded by the NHLBI (1R01HL171735). This material is the result of work supported with resources and the use of facilities at the Atlanta VA Health Care System. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the Department of Veterans Affairs.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.