
Abstract
Background:
An estimated 4.4 million people in Europe require palliative care annually, a number expected to rise with population aging. Telepalliative care (TPC) has been practiced in various settings over the past two decades. The Telepal program was developed to provide individualized palliative care, aiming to improve health-related quality of life (HRQoL) and enhance access to health care professionals.
Objective:
This study examined whether the Telepal program influenced HRQoL, symptom burden, perceived health, and patients’ sense of security among patients receiving specialized palliative care (SPC). We hypothesized that Telepal would improve HRQoL and sense of security compared with standard SPC.
Method:
In this randomized controlled trial conducted in Denmark, 182 patients referred to SPC were followed for up to 26 weeks. The control group (CG) received routine SPC, while the intervention group (TPG) received routine SPC plus TPC. HRQoL and symptom burden were assessed weekly using the European Organization for Research and Treatment of Cancer Quality of life Questionnaire–Core 15–Palliative Care and at weeks 1 and 4 using the EuroQol Five-Dimension Five-Level Questionnaire, including the Visual Analog Scale for perceived health. Sense of security was assessed twice weekly using a Likert scale.
Results:
HRQoL, symptom burden, and sense of security worsened over time in both groups, with no significant group differences. The TPG reported consistently higher pain, while perceived health declined in the CG but remained stable in the TPG.
Conclusion:
Telepal did not prevent declines in HRQoL or sense of security; however, perceived health remained more stable in the TPG. Telepal may serve as a complementary component of palliative care, particularly for patients facing barriers to in-person visits.
Key Message Statement
Telepalliative care did not improve clinical outcomes such as health-related quality of life, symptom burden, or sense of security compared with standard care. However, it may enhance patients’ overall experience by maintaining perceived health and supporting access to care, highlighting its value as a complementary component to palliative care.
Introduction
Palliative care (PC) aims to improve the quality of life for patients and families facing life-threatening illness.1,2 Each year, an estimated 4.4 million people in Europe require PC, 1 a number expected to rise with population aging and increasing prevalence of cancer and chronic lung and heart diseases.3,4 Despite growing need, only a fraction receive PC, 3 partly due to shortages of health care professionals (HCPs), 5 a challenge expected to intensify as health care demand increases.4,6 In Western Europe, many patients prefer end-of-life care at home, where primary care providers (e.g., general practitioners and district nurses) can meet most needs, although complex cases may require specialist hospital-based PC teams.4,7,8
Telepalliative care (TPC), defined as the use of telehealth in PC, has been practiced in various settings for the last two decades. 9 This enables patients, relatives, and HCPs across primary and secondary care to connect virtually. 10 Studies show that TPC is a feasible and acceptable care option,11–15 particularly as demand for telehealth solutions, including PC, increased significantly during COVID-19, when HCPs were unable to see patients in person. 16
Reported benefits of TPC include feelings of security, accessible HCPs, feeling less alone, increased access to care, and improved communication.17,18 A systematic review 17 highlights that video conferencing can improve communication, while patient-reported outcomes (PRO) can provide vital information on symptoms and conditions, supporting more personalized care. Reported telehealth barriers include usability concerns and self-report questionnaires. 17
In 2021, the Danish National Audit Office reported that the Danish regions, responsible for hospital services, had not ensured access to specialized palliative care (SPC), leaving some terminally ill patients without optimal pain relief. 19 Based on this report, and in view of the long driving distances between palliative patients and HCPs and increased demand from patients to receive end-of-life care at home, we developed a telepalliative program named Telepal. Telepal was co-created with patients, relatives, HCPs, and researchers. 20 The program aims to provide individualized PC, increase health-related quality of life (HRQoL), increase access to SPC, and improve communication and collaboration between patients and SPC teams. A detailed description of the program is provided in the Methods section.
In a study from 2017, Hoek et al. found that weekly teleconsultations with PC patients surprisingly led to worse symptom scores in the intervention group. 12 In reviews from 2020 and 2023, Steindal et al. concluded that further studies are needed to better understand TPC’s effect on symptom burden and HRQoL,17,18 and recommended user involvement in design and development. 17
Based on the above, this study aimed to provide more information about how TPC affects HRQoL, symptom burden, perceived health, and sense of security in patients receiving PC. Given limited evidence on these outcomes, we hypothesized that participation in the Telepal program would improve the HRQoL (measured by the EQ5D and the European Organization for Research and Treatment of Cancer Quality of life Questionnaire–Core 15–Palliative Care [EORTC-QLQ-C15-PAL]) and sense of security compared with usual care for patients receiving PC.
Methods
Ethical perspectives
The study was approved by the Ethical Committee in Northern Jutland (N-202000094) and registered at ClinicalTrials.gov (NCT04995848). The study was conducted in accordance with the Declaration of Helsinki, and all participants provided written informed consent.
Study design
The Telepal study was conducted as a multimethod randomized controlled trial (RCT) including 182 patients allocated into two groups. The intervention group (TPG) received the Telepal program in addition to standard SPC, while the control group (CG) received standard SPC only. Both groups received SPC from the University Hospital of Southern Denmark and could participate for up to 26 weeks. The study period was May 1, 2021, to August 31, 2024. 20
Presentation of the Telepal program
Description
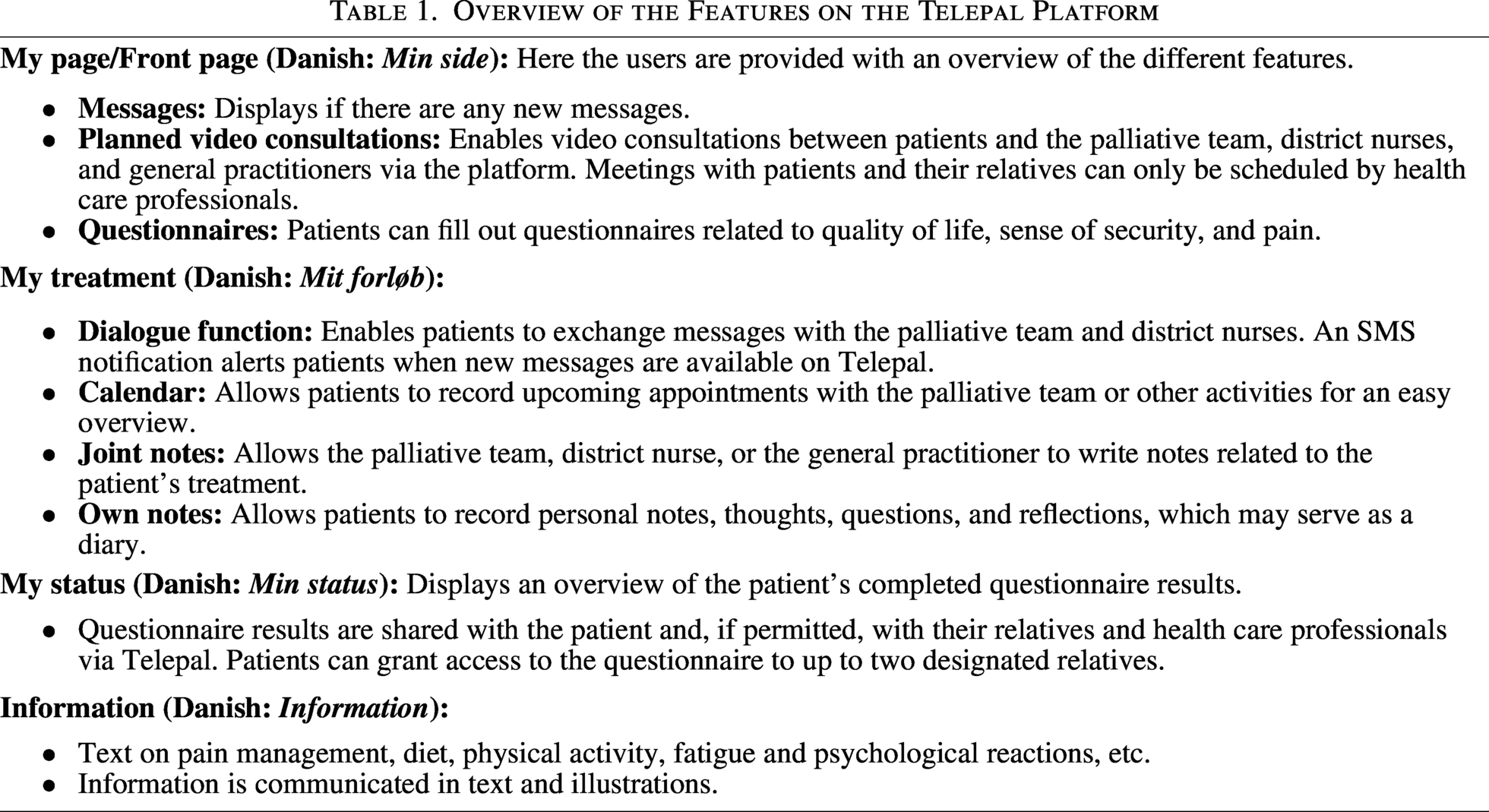
The Telepal program consisted of SPC for palliative patients and their relatives, supported by a web-based digital platform. The platform included several modules: “My page,” offering an overview of features; “My treatment,” containing a dialogue function, calendar, and options for personal or shared notes; “My status,” displaying self-reported HRQoL, pain, and sense of security; and “Information,” providing texts to patients and relatives on themes such as pain management and psychological reactions (see Table 1 for further details).
Data entered into the Telepal platform was accessible to individuals authorized by the patient through written consent, and relatives could participate. The hospital supplied patients with an iPad to access the platform. Figure 1 illustrates the context of the Telepal program.
Overview of the Features on the Telepal Platform
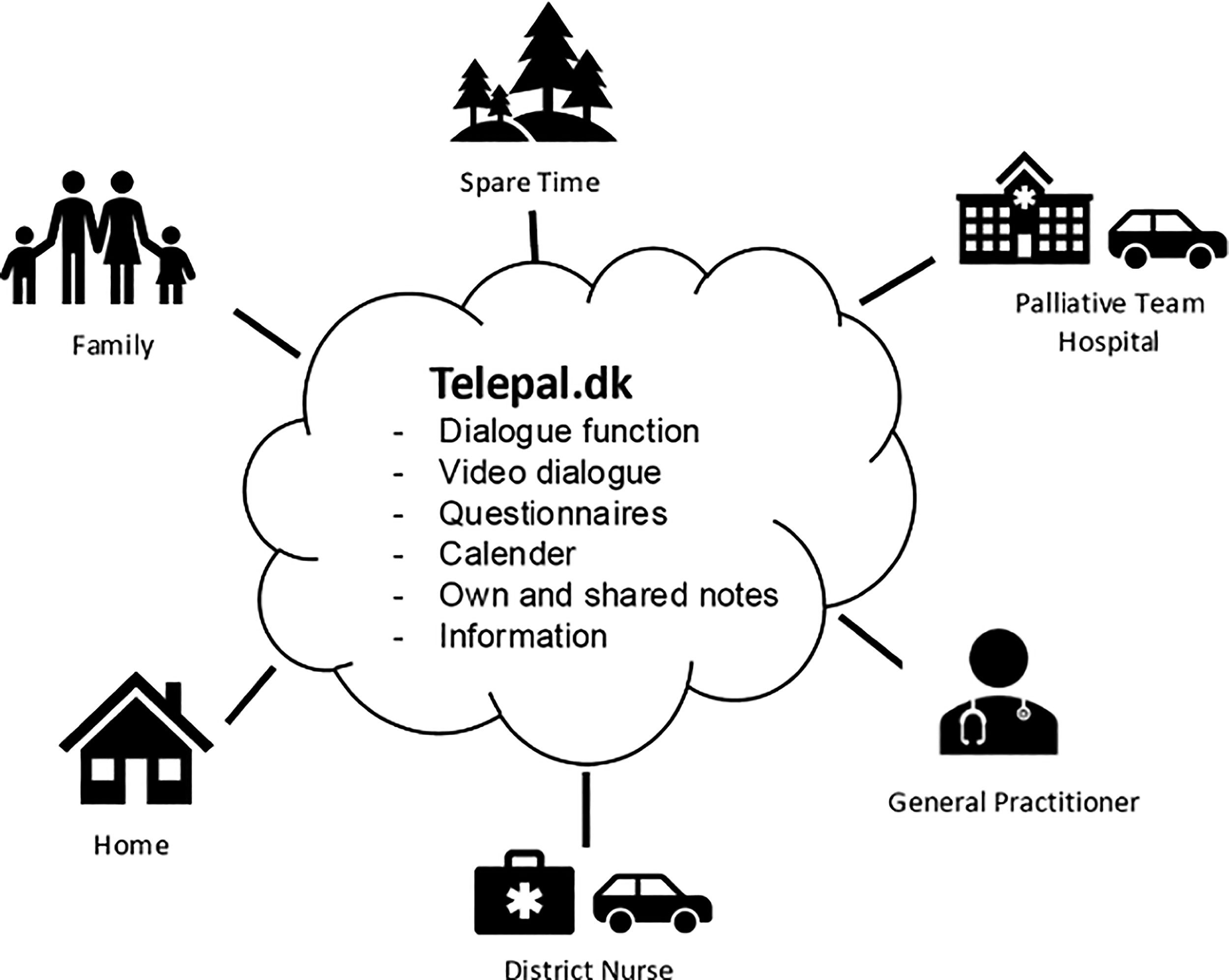
Context for the Telepal program and platform.
Participants
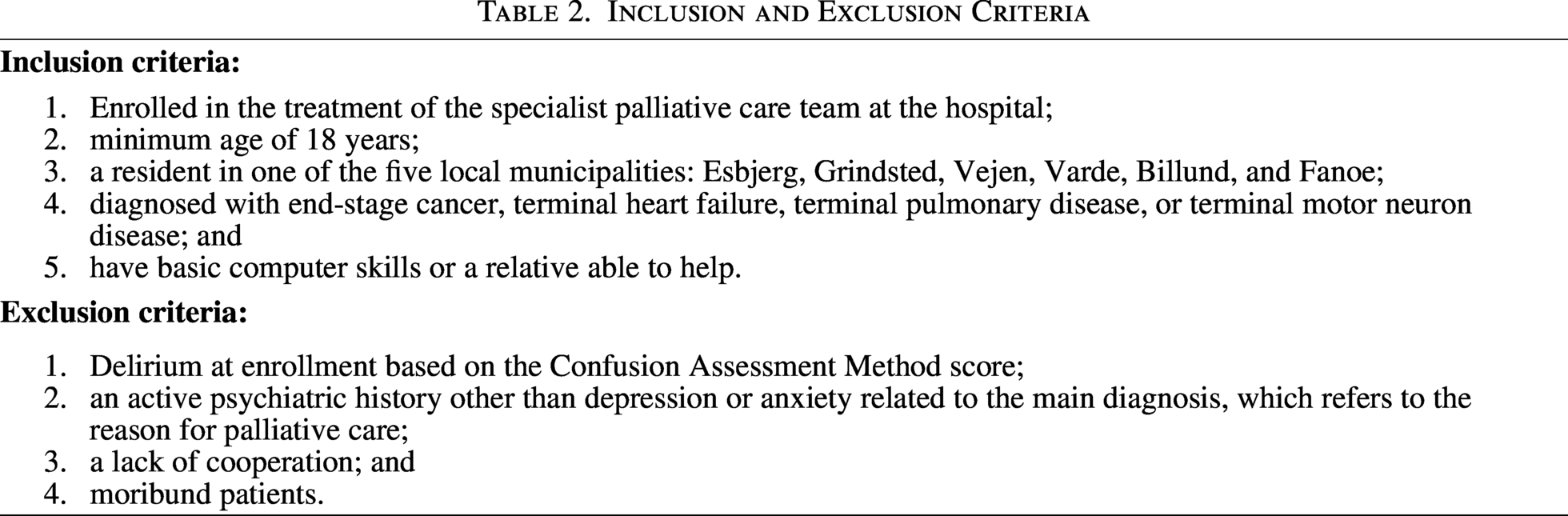
Participants were recruited from the SPC clinic at the University Hospital of Southern Denmark in Esbjerg. Screening for eligibility was integrated into the initial home visit, during which a physician and nurse assessed inclusion and exclusion criteria. Eligible patients were subsequently recruited by two project nurses from the SPC team through personal contact and an information letter. Upon consent, randomization was conducted the same day in the patient’s home, and written consent was obtained. Inclusion and exclusion criteria are presented in Table 2.
Participants were block-randomized in equal numbers to TPG or CG using a digital tool. Due to the nature of the intervention, randomization was not blinded. The TPG received Telepal in addition to SPC, while the CG received SPC alone, both following Danish Health Authority and WHO recommendations.1,21
Inclusion and Exclusion Criteria
Data collection
Baseline characteristics
Sociodemographic (gender, age, civil status, level of education, IT use) and clinical data (diagnosis) were collected from the electronic patient records for all participants.
Questionnaires
EQ-5D-5L includes five items (one per dimension, e.g., mobility) scored on a 5-point scale plus a Visual Analog Scale (VAS) assessing perceived health ranging from 0 (worst) to 100 (best) health.
24
Rather than utility scores, dimension scores and the VAS were used for comparison with the EORTC QLQ-C15-PAL. The EQ-5D is validated in PC with strong psychometric properties.
25
It was administered twice: at the date of inclusion and after four weeks. An ad hoc questionnaire assessing the patients’ sense of security in PC (“Overall, how secure have you felt during the past 24 hours”) on a 5-point scale (1 = very insecure, 5 = very secure) was developed for use in this study. This questionnaire was completed twice weekly during the study.
Statistical analysis
Prior to analysis, data were screened for missing values, and subscale scores were calculated. Cases with at least one scale score on the EORTC QLQ-C15-PAL, EQ-5D, or sense of security measures at any time point were included. Baseline and clinical characteristics were compared between groups using t tests or chi-square tests as appropriate (see Table 3).
Baseline Characteristics
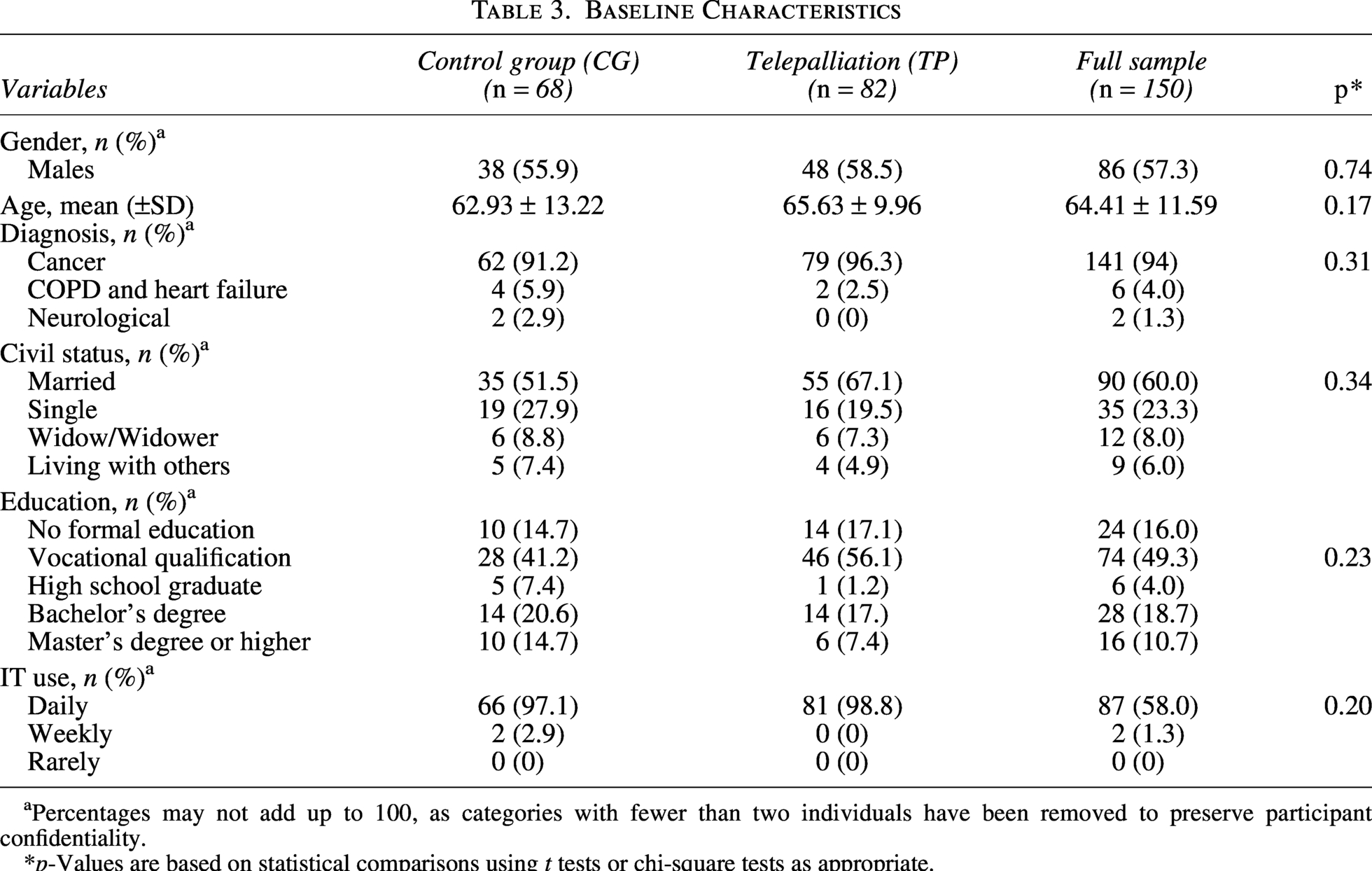
Percentages may not add up to 100, as categories with fewer than two individuals have been removed to preserve participant confidentiality.
*p-Values are based on statistical comparisons using t tests or chi-square tests as appropriate.
Mixed linear models (MLMs) were used to compare groups and assess changes over time on EORTC QLQ-C15-PAL and EQ-5D subscales. MLMs accommodate missing observation-level data, allowing retention of cases despite missing scores at some time points, which is important given the expected dropout due to the deaths of participants. All measures were treated as continuous variables, with MLMs estimated via restricted maximum likelihood. Data were hierarchically structured with time (level 1) nested within individuals (level 2). The basic model included random intercepts and fixed effects for time, group, and time × group interaction. Covariates included cohabitation status, education level, and age group. A diagonal covariance structure was selected based on Akaike Information criterion and Bayesian information criterion, with final model selection based on –2LL change tests. 26 Despite negative skewness in some EORTC QLQ-C15-PAL subscales, residuals were normally distributed, supporting model validity. Alpha was set at 0.05. Analyses were performed using SPSS 29.0.
Results
Baseline characteristics are displayed in Table 3. Statistical analyses revealed no significant differences between groups on any of the baseline or clinical characteristics (see Table 3).
The consort diagram (Fig. 2) illustrates patient attrition during the 26-week study period. In total, 32 participants dropped out, leaving 150 for final analysis (intervention: n = 82; control: n = 68). Participant numbers declined by more than half within the first 12 weeks, and only 38 remained at week 26. Given the palliative population, many participants were unable to contribute data across the full study period.
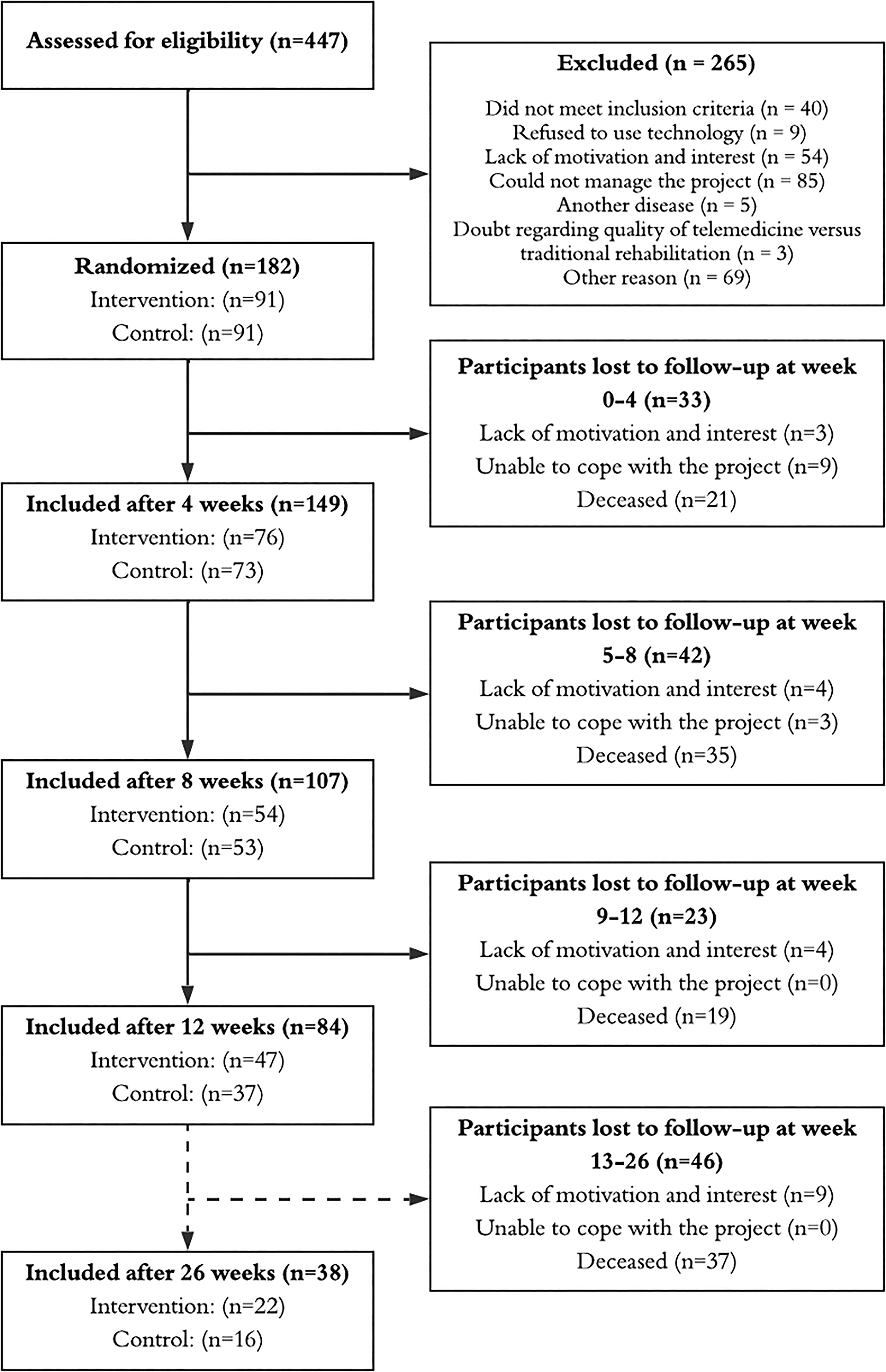
Consort diagram over the 26-week study period.
EORTC
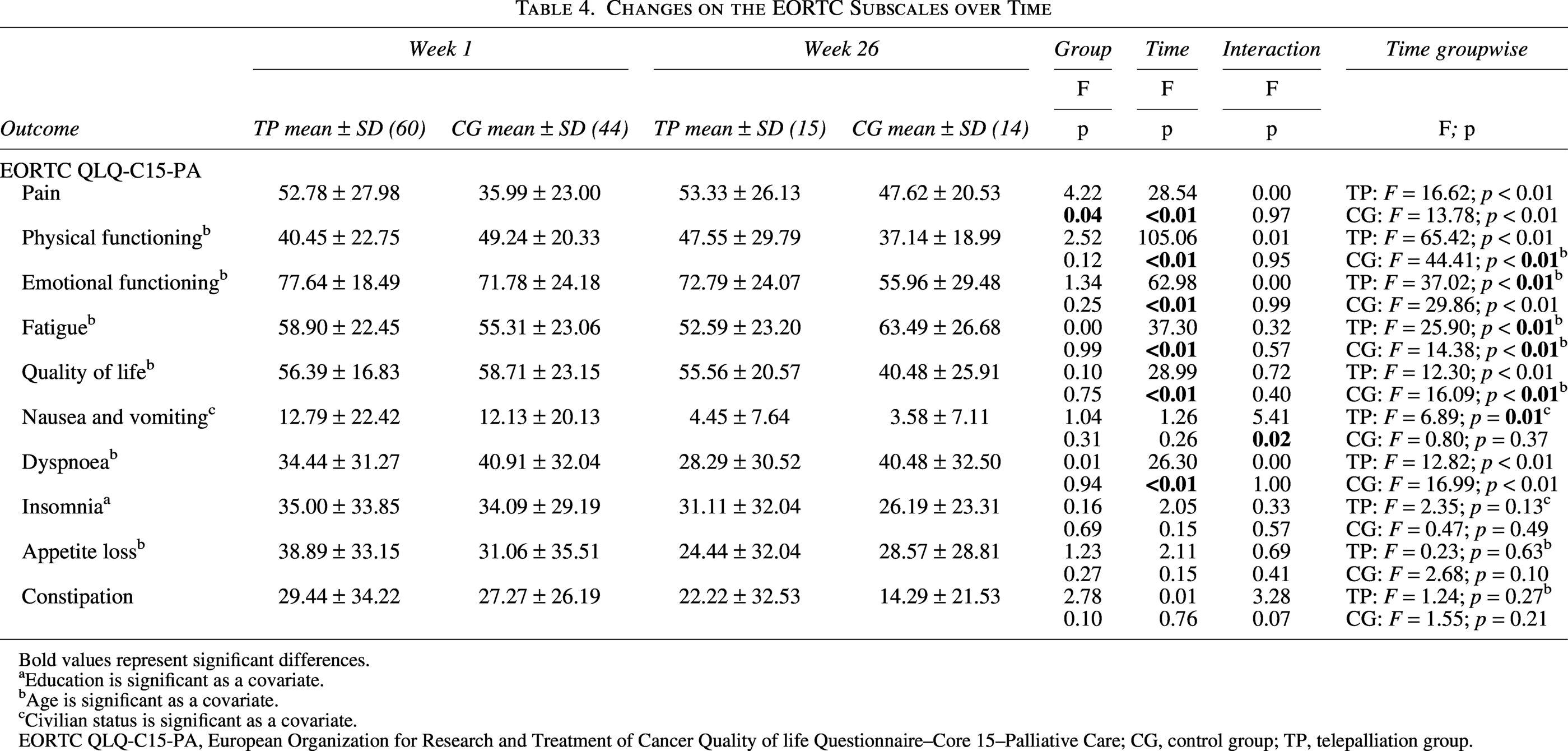
HRQoL significantly decreased over time (F = 28.99, p < 0.01) in both groups, and analyses did not indicate significant differences between groups over time.
Significant main effects of time (F = 28.54, p < 0.01) and group (F = 4.22, p = 0.04) were observed for pain, with consistently higher pain reported in the TPG; however, no significant interaction between time and group was found (F = 0.00, p = 0.97). Pain increased significantly over time in both groups (p’s < 0.01), with the initial group difference remaining stable over time (Table 4).
Changes on the EORTC Subscales over Time
Bold values represent significant differences.
Education is significant as a covariate.
Age is significant as a covariate.
Civilian status is significant as a covariate.
EORTC QLQ-C15-PA, European Organization for Research and Treatment of Cancer Quality of life Questionnaire–Core 15–Palliative Care; CG, control group; TP, telepalliation group.
Significant decreases in other HRQoL-related measures over time were found for Physical Functioning (F = 105.06, p < 0.01), Emotional Functioning (F = 62.98, p < 0.01), Fatigue (F = 37.30, p < 0.01), and Dyspnea (F = 26.30, p < 0.01) across both groups. Age had a major effect on Fatigue in both groups, but only on Physical Functioning and HRQoL in the CG and Emotional Functioning in the TPG. A significant interaction between time and group was observed for Nausea and Vomiting (F = 5.41, p = 0.02), and additional analyses suggest that this was due to a significant decrease over time in the TPG only (p < 0.01). Cohabiting was associated with Nausea and Vomiting in the TPG, whereas age was associated with Constipation and Appetite Loss across groups. Results for covariates are not specified in Table 4, and no other significant effects were observed (Table 4).
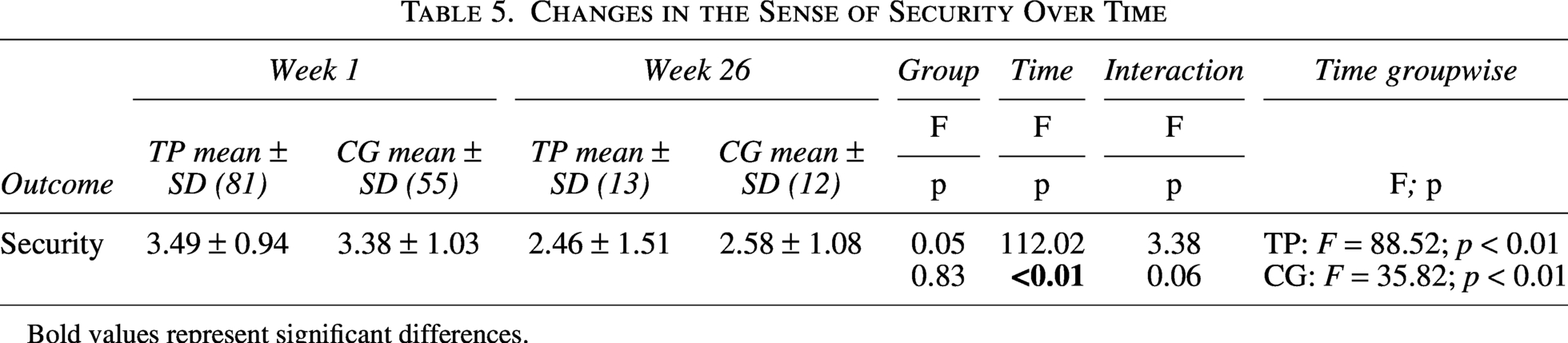
Participant numbers decreased considerably over time (see Table 5). Therefore, MLM results should be interpreted with caution, as the sample remaining for analysis at week 26 had diminished considerably from baseline, which could affect results.
Changes in the Sense of Security Over Time
Bold values represent significant differences.
EQ-5D
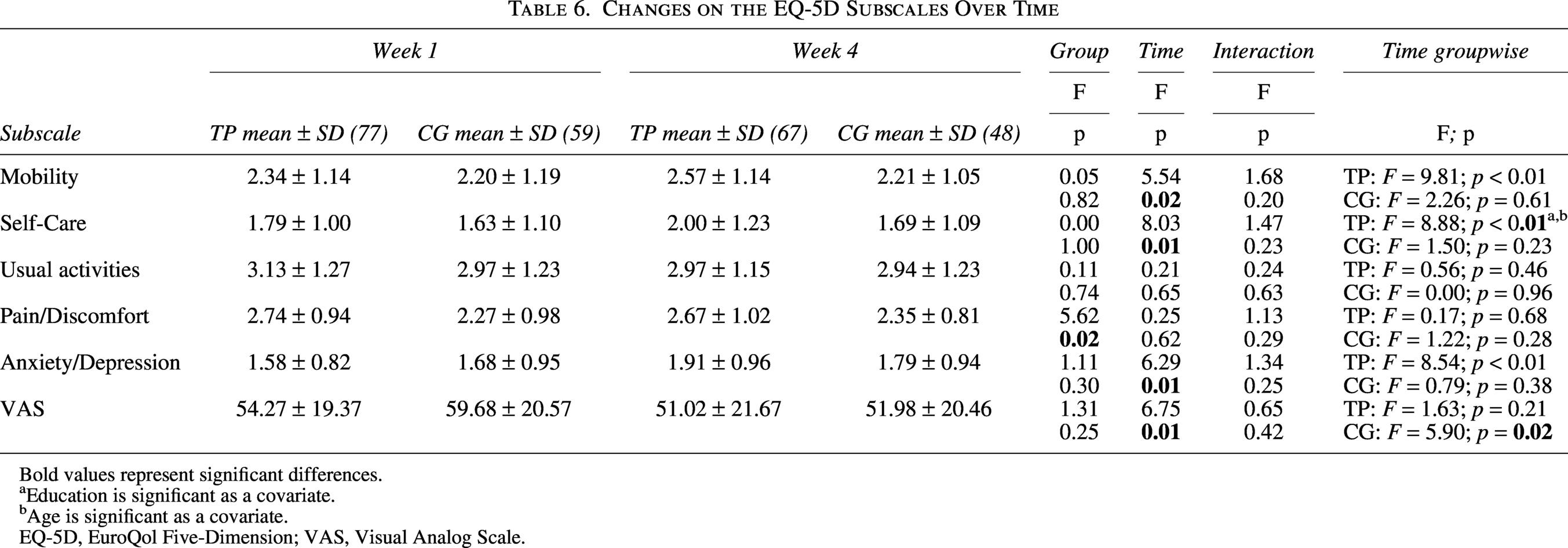
The TPG reported significantly more pain/discomfort than the CG over time (F = 5.62, p = 0.02). Negative changes over time, regardless of group, were observed in Mobility (F = 5.54, p = 0.02), Self-Care (F = 8.03, p = 0.01), Anxiety/Depression (F = 6.29, p = 0.01), and VAS (F = 6.75, p = 0.01). perceived health (VAS) scores decreased significantly over time in the CG but remained stable in the TPG. For Mobility, Self-Care, and Anxiety/Depression, the TPG showed the greatest level of change. Education and age had major effects on self-care scores (results not shown). No other significant effects were found (Table 6).
Changes on the EQ-5D Subscales Over Time
Bold values represent significant differences.
Education is significant as a covariate.
Age is significant as a covariate.
EQ-5D, EuroQol Five-Dimension; VAS, Visual Analog Scale.
Sense of security
Sense of security declined over time in both groups (F = 112.02, p < 0.01), with no significant group effect (p = 0.83) and a trend for an interaction between time and group (p = 0.06).
Discussion
This study aimed to explore how TPC affects HRQoL, symptom burden, perceived health, and sense of security compared to usual care. We further hypothesized that participation in Telepal would improve HRQoL, measured by the EQ5D and EORTC QLQ-C15-PAL, and enhance the sense of security compared to usual care in palliative patients.
Overall, these hypotheses were not supported. HRQoL declined significantly over time in both groups, with no significant differences between them. Similarly, sense of security decreased over time with no clear difference between groups.
On the EORTC QLQ-C15-PAL, pain increased over time in both groups, with consistently higher pain reported in the TPG. However, there was no significant interaction between time and group suggesting that telepalliation did not alter pain trajectories and that the observed group differences likely reflect baseline differences in symptom severity rather than intervention effects as the difference between groups remained relatively stable over time. Both groups also showed significant increases in fatigue and dyspnea alongside declines in physical and emotional functioning, reflecting the expected deterioration in a palliative population.
EQ-5D-5L findings were largely consistent with the EORTC results. The TPG reported higher pain and discomfort over time, while both groups showed negative changes in mobility, self-care, and anxiety/depression. However, perceived health, as measured by the EQ-5D VAS, decreased over time in the CG but remained relatively stable in the TPG, suggesting a possible buffering effect on perceived health. Age and education were associated with self-care. However, while the EORTC QLQ-C15-PAL assesses health over a one-week recall period and was collected weekly throughout the 26-week study period, the EQ-5D reflects perceived health “today” and was only measured at baseline and week four, and thus, these findings should be interpreted with caution.
When interpreting these results, the characteristics of the study population must be considered. Participants were receiving SPC, indicating advanced, life-threatening illness and complex care needs, which may partly explain the observed declines in HRQoL and sense of security and increased symptom burden, as opportunities for measurable improvements may be limited in late-stage disease. In Denmark, median survival from first SPC contact is 48 days, suggesting late referral. 27 Supporting this, Hansen et al. reported higher odds of fatigue, impaired physical functioning, and poor HRQoL among SPC patients compared with those receiving basic PC. 28 With this in mind, intervention effects should be interpreted in the context of a population with advanced disease trajectories.
Inconsistent findings on telepalliative care’s impact on health and HRQoL17,18,29 may reflect differences in disease stage and may help explain why Telepal did not result in measurable improvements in perceived health or HRQoL in this study. Steindal et al. reported mixed patient experiences with telehealth in PC, with some describing increased symptom burden, fear, or anxiety, while others reported no such challenges. 17 Similarly, other reviews have reported inconsistent effects of telehealth on symptom management and HRQoL, with studies either reporting positive or negative outcomes or no change.18,29 Additionally, end-of-life quality in palliative patients typically declines over time due to disease progression, 30 which may influence PRO. This highlights the need for further research into factors affecting telepalliative care’s impact on HRQoL and symptom burden.
Assessment tools for HRQoL varied across studies in the reviews, with many relying on qualitative methods or proxy indicators such as symptom burden or psychological outcomes.17,18 Only two studies used measures comparable to the current study, namely the EORTC QLQ-C30 31 or the QLQ-C15-PAL. 32 Besse et al. reported a significant decrease in QoL measured by the EORTC QLQ-C30 from baseline to four weeks, 31 whereas Nemeck et al., using the EORTC QLQ-C15-PAL, found no difference between intervention and control groups over 10 weeks. 32 Both included patients with advanced cancer. As over 90% of participants in the current study had cancer and were receiving SPC, the populations are likely comparable, suggesting that when direct HRQoL measures are used in advanced palliative populations, telepalliative interventions may not result in measurable changes in HRQoL over time.
Overall, symptom burden increased over time in both groups, with no evidence that telepalliation altered symptom trajectories. Hoek et al. reported worsening symptom burden over time in patients receiving PC who participated in weekly teleconsultation. 12 The authors suggested that increased symptom focus through continuous dialogue may have contributed to heightened symptom awareness. In the current study, however, symptom perceptions were largely similar between groups, possibly because both groups completed repeated symptom questionnaires, which may have increased awareness regardless of group allocation. As noted, these findings likely reflect the expected deterioration in a palliative population.
Sense of security decreased significantly over time, with no difference between the groups. This contrasts with prior literature suggesting that home-based telepalliative care may enhance security. Steindal et al. reported increased feelings of security, primarily based on qualitative interviews, which may capture aspects not assessed by the quantitative measure used in the current study. 18 Similarly, Kirby et al. described telehealth as promoting security, comfort, independence, and control, while noting that benefits depend on patient engagement and comfort with technology. 33 Bakitas et al. emphasized assessing individual needs and highlighted digital illiteracy as a potential barrier unless adequate support is provided. 34 Bauer et al. likewise found that telepalliative care can increase convenience and allow patients to remain at home, but outcomes depend on alignment with patient needs. 35 Together, these findings suggest that telepalliative care’s impact on sense of security may depend on individual characteristics, including digital competence and the extent to which the intervention aligns with patient needs.
A qualitative substudy of Telepal found that participation enhanced patients’ sense of security and coherence by improving communication with HCPs, 36 although this was not reflected in the quantitative measure used in the current study. Similarly, Lind et al. reported that a digital pain diary improved contact with HCPs and increased sense of security, 37 and Gurp et al. found that patients felt a sense of safety and relief knowing an SPC team was available through teleconsultation. 14 Considered alongside the present findings, this suggests that while a digital platform may not affect symptom levels, it may support patients by improving communication and perceived security. Telepal may therefore serve as a complementary component of PC beyond symptom management. Communication appears central to its value, and future studies should consider quantitative measures that more directly assess communication-related aspects of care and their influence on outcomes.
Limitations
As a single-center study, context-specific social, cultural, or environmental factors may limit generalizability. The high attrition rate complicates evaluation of psychological outcomes, raising questions about whether an RCT is optimal to evaluate SPC programs such as Telepal. As intervention content was identical and only differed in delivery mode, many outcomes, except health care cost evaluation, could have been explored through case studies, avoiding ethical concerns related to control group assignment. Nonetheless, an RCT was necessary for robust assessment of health care costs, planned for further analyses.
Conclusion
HRQoL and sense of security declined, while symptom burden increased over time in both groups, with no significant between-group differences, suggesting that the observed deterioration reflects disease progression rather than effects of Telepal. Telepal did not alter symptom trajectories; however, perceived health (EQ-5D VAS) remained more stable in the TPG, indicating a potential buffering effect. Considered alongside qualitative findings of improved communication and security, perhaps, Telepal may serve as a complementary component of SPC by supporting patients’ overall experience, even when clinical outcomes remain unchanged. Telepalliation may therefore be best positioned not as a replacement for in-person SPC, but to create access for patients who face barriers to clinic visits, including those in rural areas or with travel or mobility limitations.
Authors’ Contributions
B.D. and J.V.A.S. conceived and designed the study. J.V.A.S., H.S., E.D.R.J., E.S.B.R., and B.D. performed the data analysis and drafted the article. J.V.A.S., H.S., E.D.R.J., E.S.B.R., M.K.R., and B.D. contributed to data collection and interpretation of results. All authors gave feedback to the article. All authors approved the submitted version.
Footnotes
Acknowledgments
The authors thank the Danish Cancer Society for funding, the Hospital of Southwest Jutland for technological support, all partners for in-kind contributions, the patients and relatives for participating, and project nurses, Hanne Christensen and Sanne Skov.
Consent for Publication
As stated, written informed consent was obtained from all participants in both the telepalliation and control groups. Any potentially identifying patient characteristics have been omitted, including baseline characteristics where two or fewer participants were represented.
Data Availability
Data are not available for public access, as we have not received consent on this issue from patients enrolled in the study.
Author Disclosure Statement
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding Information
The Telepal study was funded by the Danish Cancer Society.