
Abstract
Background:
Accurately estimating short-term survival in individuals receiving palliative care is crucial for guiding personalized clinical decisions. Existing tools often rely on subjective assessments and have limited applicability. This study aimed to develop a simple, interpretable nomogram integrating objective biomarkers and functional status, applicable to a diverse population of end-stage patients.
Methods:
A total of 167 patients who began working with the palliative care team were retrospectively reviewed, and the cohort was randomly partitioned into a 7:3 training (n = 117) and an internal validation set (n = 50). From an initial pool of 31 variables, independent prognostic factors were identified using least absolute shrinkage and selection operator (LASSO) Cox regression, while optimal thresholds for continuous measures were determined via maximally selected rank statistics. A nomogram was subsequently developed, and its performance was evaluated through time-dependent receiver operating characteristic analysis, calibration curves, and decision curve analysis, as well as sensitivity, specificity, positive predictive value, negative predictive value, and positive and negative likelihood ratios (LR+ and LR−) in the validation set at 30, 60, and 90 days.
Results:
The LASSO model ultimately highlighted three principal predictors: C-reactive protein (CRP), estimated glomerular filtration rate (eGFR), and the Barthel Activities of Daily Living (BADL) score. Elevated CRP (hazard ratio [HR] = 1.005, p = 0.01) and decreased eGFR (HR = 0.99, p = 0.01) were independent risk factors for mortality. The nomogram demonstrated 30-/60-/90-day AUCs of 0.764/0.716/0.705 in the training set and 0.770/0.748/0.788 in the validation set. Calibration plots showed excellent agreement between predicted and observed survival, and Decision curve analysis indicated clinical net benefit across commonly used risk thresholds. In the validation set, the nomogram showed sensitivity/specificity of 69.05%/75.00%, 83.33%/87.50%, and 88.10%/87.50% at 30, 60, and 90 days, respectively; the corresponding LR+ values were 2.762, 6.666, and 7.048, and LR− values were 0.413, 0.191, and 0.136.
Conclusions:
We successfully developed and internally validated a simple, interpretable nomogram integrating CRP, eGFR, and BADL scores, capable of rapidly predicting short-term survival in palliative care patients. In addition to favorable discrimination and calibration, the model demonstrated clinically informative classification performance at 30, 60, and 90 days. The model is applicable to a diverse patient population and may assist in clinical decision-making and resource optimization.
Key Findings
We developed a simple, bedside-applicable nomogram to predict 30-, 60-, and 90-day survival in palliative care patients and internally validated it using a split-sample approach. The model integrates three routinely available, low-cost, objective indicators: C-reactive protein (CRP), estimated glomerular filtration rate (eGFR), and Barthel Activities of Daily Living (BADL) score. Higher CRP, lower eGFR, and lower BADL scores were associated with increased short-term mortality risk.
What is known and what is new?
Previous prognostic tools in palliative care, such as Palliative Prognostic Score, Palliative Performance Scale, and Karnofsky Performance Status, rely heavily on subjective assessments and have limited applicability in noncancer populations. Existing nomograms often focus on terminal cancer patients, ignoring functional status and objective biomarkers. This study adds a practical, interpretable tool that applies to a mixed cohort of cancer and noncancer terminal patients, combining inflammatory, organ function, and functional status markers.
What is the implication, and what should change now?
This nomogram provides a rapid, individualized risk assessment for short-term survival at the bedside or during multidisciplinary team discussions. Its application can support clinical decision-making, guide resource allocation, and facilitate prognostic communication with patients and families. Future implementation via online calculators or mobile apps could enhance real-world utility and promote personalized palliative care.
Introduction
With the aging population, the demand for palliative care is steadily increasing. 1 Accurate prediction of short-term survival is a cornerstone for effective palliative care, facilitating timely symptom management, realistic goal setting, and optimal allocation of medical resources. However, clinicians’ prognostic estimates are often unreliable and tend to overestimate survival, resulting in delayed referrals and suboptimal end-of-life care. 2 Previous studies have shown that prognostic tools such as the Palliative Prognostic Score (PaP), Palliative Performance Scale (PPS), and Karnofsky Performance Status (KPS) exhibit substantial variability in predictive performance across different disease types and healthcare settings, largely due to subjective scoring and the lack of objective laboratory indicators.3–5 Although multiple prognostic tools, including PaP, PPS, and KPS, have been developed, their clinical application is limited by notable shortcomings, such as overreliance on subjective clinical judgment, omission of objective biomarkers, and insufficient validation in diverse patient populations, particularly noncancer patients.6,7 Differences in disease trajectories, symptom reporting, healthcare resource utilization, and end-of-life decision-making preferences further constrain the generalizability of models developed in Western populations to other regions. Worldwide, the growing prevalence of chronic nonmalignant diseases, including heart failure, chronic obstructive pulmonary disease (COPD), and dementia, is gradually altering the demographic profile of patients who would benefit from palliative care.8–10 At present, few tools are available that can accurately estimate short-term survival using routinely collected and objective physiological measures, and that are applicable to both cancer and noncancer populations in routine clinical practice. This underscores the need to establish new predictive models.
In recent years, various machine learning–based survival prediction models have emerged in oncology and critical care; however, models specifically targeting palliative care populations and validated across different cultural contexts remain limited.11,12 Importantly, the least absolute shrinkage and selection operator (LASSO) regression is well suited for situations where the number of potential predictors is large relative to the sample size. It enables simultaneous variable selection and regularization, which helps prevent overfitting and yields a more parsimonious model. 13 In this work, we applied LASSO Cox regression to identify major prognostic indicators from clinical, laboratory, and functional variables, and subsequently developed and internally validated a streamlined and clinically practical nomogram for predicting short-term survival. The model integrates objective biomarkers, including CRP and eGFR, with a standardized functional assessment, the BADL score. BADL is a widely used measure of basic self-care ability that assesses patients’ independence in daily activities such as feeding, bathing, dressing, toileting, transferring, and mobility. CRP reflects systemic inflammatory status, eGFR indicates organ functional decline, and the Barthel index quantifies functional independence; all are closely associated with survival outcomes in end-stage disease and were therefore included as candidate predictors. By focusing on widely available, routinely collected data, we aimed to develop a transparent and user-friendly tool to support clinical decision-making in real-world settings with potential applicability beyond a single regional context.
Materials and Methods
Study design and patient population
This investigation was conducted as a retrospective cohort study at a single institution. This design systematically reviews existing clinical data to compare outcomes (overall survival) across patient groups with different levels of exposure (baseline prognostic variables), thereby exploring associations between variables. We selected this study design based on several considerations. First, the survival of palliative care patients is generally short, making large-scale prospective studies challenging in terms of time and follow-up feasibility. Second, our hospital maintains a relatively complete and structured electronic medical record system, ensuring high-quality and comprehensive data for key variables (e.g., laboratory parameters and functional scores), providing a reliable foundation for retrospective analysis. Finally, the retrospective design is feasible in this context, given the short survival, high data availability, and suitability for exploratory development and preliminary validation of prognostic models. The study population included consecutive hospitalized adult patients who began working with the palliative care team in the Department of Geriatrics at The Second People’s Hospital of Futian District Shenzhen, between January 1, 2023, and September 20, 2025. In this study, initiation of palliative care referred to a transition to primarily symptom management and comfort-oriented treatment, rather than continuation of aggressive life-prolonging interventions.
Inclusion criteria
Patients were considered eligible if they fulfilled all of the following conditions: (1) A confirmed diagnosis of irreversible end-stage disease, including advanced cancer, chronic heart failure, chronic respiratory failure, or chronic renal failure. (2) Expected survival ≤6 months at enrollment, assessed by a combination of PPS ≤60%, KPS score ≤50 points, together with the attending physician’s clinical judgment. (3) Provided written informed consent, either personally or via a legal representative, to receive palliative care aimed at symptom management and quality-of-life enhancement, while foregoing aggressive curative interventions. In our center, palliative care for this study population was primarily focused on symptom control, comfort care, psychosocial support, and quality-of-life improvement, with patients generally not receiving ongoing aggressive disease-directed or life-prolonging treatments after initiation of palliative care.
Exclusion criteria
Patients were excluded if they satisfied any of the following conditions: (1) Unexpected clinical improvement or availability of new effective treatments. (2) Withdrawal of palliative care preference by the patient or family. (3) Missing baseline data: patients with >10% missing values for key variables were excluded; for variables with missing values that could be imputed, multiple imputation was applied.
Ethics statement
The study was approved by the Ethics Committee of the Second People’s Hospital of Futian District, Shenzhen (Approval No.: [20250402094401]). As a retrospective study using anonymized medical records without intervention in patient care, informed consent was waived in accordance with the Declaration of Helsinki and relevant regulations.
Data collection and candidate variables
All baseline information was retrospectively collected from the electronic medical records on the day each patient began palliative care involvement. Candidate variables were selected based on the following principles: first, an extensive literature review of high-quality studies on prognostic factors in end-stage patients14,15; second, expert clinical experience from the hospital’s palliative care team, including indicators with significant impact on physiological status, functional level, and care needs. BADL was selected as a candidate functional variable because it is simple, routinely used in geriatric and palliative care practice, and provides a practical assessment of basic functional dependence. Compared with other functional assessment scales, BADL was considered more feasible for retrospective data collection in our setting and more directly reflective of patients’ daily care needs.
A total of 31 candidate variables were included, encompassing four domains: (1) Demographics: age, sex, height, weight, body mass index (BMI), and education level. (2) Clinical status: presence of pain (yes/no), cognitive function, level of consciousness, and awareness of disease progression. (3) Laboratory parameters included 15 routine biochemical and hematological tests: CRP, eGFR, albumin, platelet count, hemoglobin, red blood cell count, neutrophil count, lymphocyte count, neutrophil-to-lymphocyte ratio, hematocrit, cholinesterase activity, prealbumin, creatinine, uric acid, and D-dimer. (4) Functional assessment and care-related factors: BADL (0–100 points), Glasgow Coma Scale (3–15 points), and use of supportive devices, including nasogastric tube, urinary catheter, drainage tube, and intravenous catheter.
Prior to modeling, multicollinearity among continuous variables was assessed, with variables showing correlation coefficients ≥0.7 retained based on clinical relevance. In the subsequent statistical analyses, continuous variables such as age, CRP, and eGFR were summarized as mean ± standard deviation (SD) or median (interquartile range, IQR), according to their distribution. Categorical variables, including sex and nasogastric tube use, were expressed as counts and percentages. All laboratory tests were performed within 24 hours of signing the palliative care agreement, following routine clinical protocols.
Follow-up and outcome definition
Patients were monitored monthly through telephone contacts or outpatient visits with their primary caregivers until September 20, 2025. The primary endpoint was overall survival, defined as the duration (in days) from the start of palliative care involvement to death from any cause. Dates of death were primarily obtained from electronic medical records and confirmed via family contact; in cases of discrepancy, the medical record was used as the reference. Sixteen patients were lost to follow-up, resulting in a follow-up rate of 91.3%, with their last recorded date considered as the censoring time. A Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) flow diagram is presented in Figure 1 to show the number of patients assessed, excluded, included, and lost to follow-up.
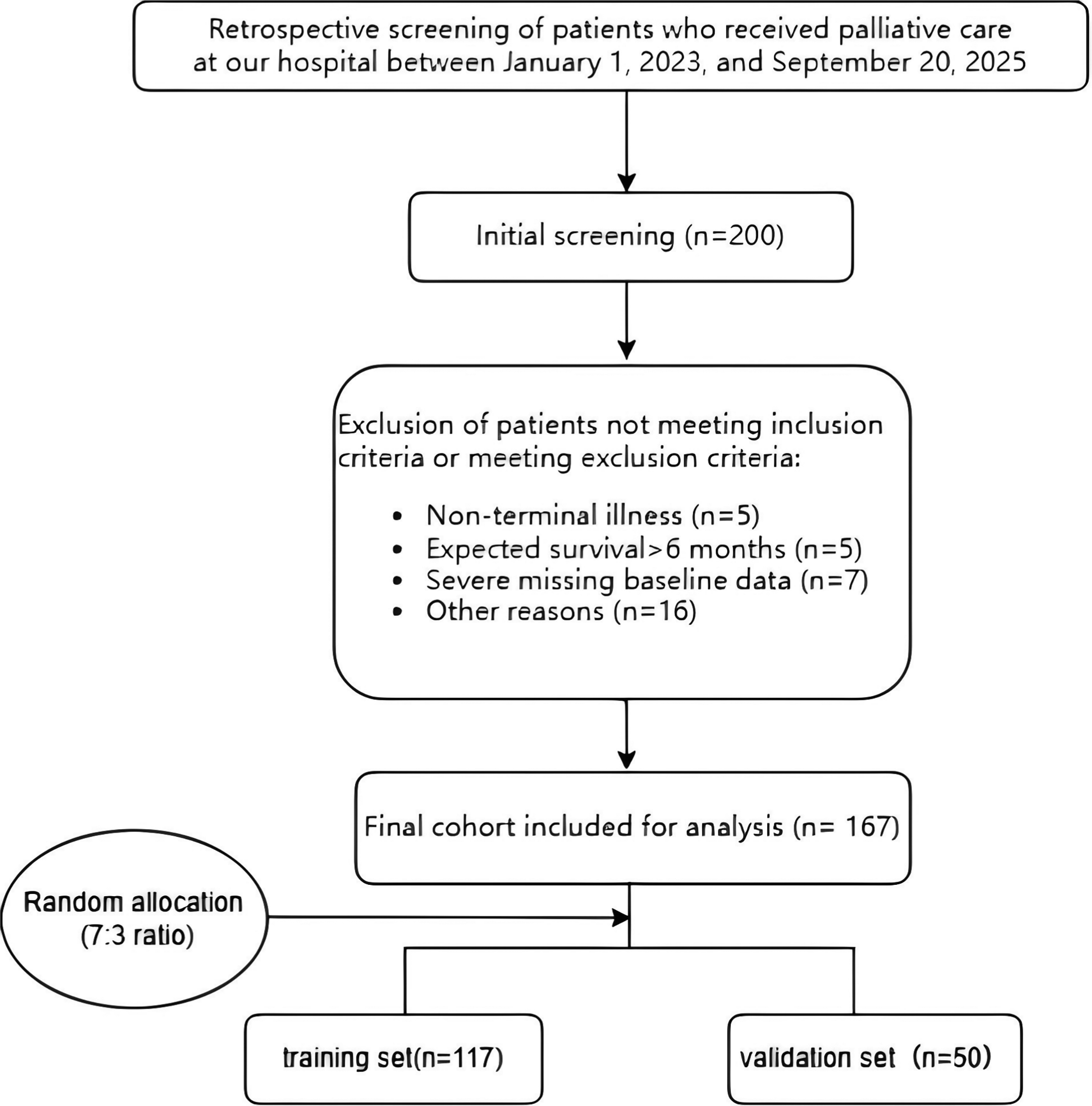
Patient selection flowchart. The diagram illustrates the number of patients screened, reasons for exclusion, and the final cohort included in the study.
Statistical analysis
Data were processed and analyzed using established statistical approaches. Continuous variables were summarized as mean ± SD or median (IQR) based on distribution, which was evaluated using the Shapiro–Wilk test, while categorical variables were reported as counts and percentages [n (%)]. Group comparisons were performed using an independent-samples t-test, Mann–Whitney U test, chi-square test, or Fisher’s exact test as appropriate. Survival analysis was conducted using the Kaplan–Meier method, and differences between groups were assessed using the log-rank test. The dataset was randomly divided into a training set (70%) and an internal validation set (30%) using a split-sample approach; if event rates were imbalanced, weighting or resampling methods were considered.
To develop a parsimonious and robust predictive model, a two-stage modeling process was employed:
Stage 1: Variable Selection. LASSO (Least Absolute Shrinkage and Selection Operator) Cox regression was applied in the training set to select the most relevant prognostic factors from 31 candidate variables. Prior to modeling, multicollinearity among continuous variables was assessed, and for variables with correlation coefficients ≥0.7, the one with higher clinical relevance was retained. LASSO allows simultaneous variable selection and regularization, making it suitable for small sample sizes with high-dimensional data and effectively reducing collinearity. 10fold cross-validation and the one-standard-error rule were used to determine the optimal λ, retaining variables with non-zero coefficients for subsequent modeling. Stage 2: Model Construction and Cutoff Determination. Variables identified by LASSO were incorporated into a multivariable Cox proportional hazards model to calculate hazard ratios (HRs) and their 95% confidence intervals (CIs). To improve clinical interpretability and facilitate risk stratification, optimal cutoff values for continuous variables (CRP, eGFR, and BADL) were identified using maximally selected rank statistics (maxstat). These dichotomized thresholds were used to simplify presentation and stratify patients into clinically meaningful risk groups, but were not intended to be used individually to predict survival; prognostic estimation was based on the integrated nomogram as a whole. Stage 3: Nomogram Development. Using the multivariable Cox model, a nomogram was developed to estimate 30-, 60-, and 90-day survival probabilities. CRP, eGFR, and BADL were included due to their clinical relevance: CRP reflects systemic inflammation, eGFR reflects organ functional decline, and BADL quantifies functional status, all of which are associated with survival in end-stage disease. Stage 4: Model Performance Evaluation. (1) Discrimination: Time-dependent receiver operating characteristic (ROC) curves were generated using the timeROC package in R to calculate the area under the curve (AUC), and Harrell’s C-index was computed to evaluate the overall predictive performance. AUC values with 95% confidence intervals were reported for 30-, 60-, and 90-day survival. (2) Calibration: Calibration plots were employed to assess the agreement between predicted and observed survival probabilities. Internal validation was performed using bootstrap resampling with 1,000 iterations to minimize optimism bias. (3) Decision curve analysis (DCA) was conducted to evaluate the net clinical benefit across various risk thresholds, comparing the nomogram-based approach with the extreme strategies of “treat all” and “treat none,” thereby quantifying the model’s potential value in real-world clinical decision-making. (4) Additional classification performance analysis was conducted in the validation cohort at 30, 60, and 90 days. Based on the corresponding nomogram-predicted classifications, sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), positive likelihood ratio (LR+), and negative likelihood ratio (LR−) were calculated to further assess the clinical interpretability of the model. In addition, overall correct classification rate, misclassification rate, false-positive rate, and false-negative rate were calculated at each time point to quantify potential classification error and support interpretation of the clinical consequences of prognostic misclassification. All statistical tests were two-sided, with a significance level set at p < 0.05. Analyses were primarily conducted using R (version 4.3.2), with supplementary analyses performed in SPSS (version 25.0). The study followed TRIPOD guidelines to ensure methodological rigor.
Results
Baseline characteristics and cohort comparability
A total of 167 patients with palliative care involvement were included and randomly allocated to a training cohort (n = 117) and a validation cohort (n = 50) at a 7:3 ratio (Fig. 1). As presented in Table 1, the two cohorts were generally comparable in terms of demographic, clinical, and laboratory characteristics. No significant differences were observed in age (median 81 versus 78.5 years, p = 0.922), sex distribution (male 54% in both groups, p = 1.000), BMI (19.39 ± 3.10 versus 20.28 ± 2.96 kg/m2, p = 0.081), survival status (mortality 81% versus 84%, p = 0.643), or median observed survival time (11 vs. 12.5 months, p = 0.365). Although cognitive status (p = 0.010) and platelet count (p = 0.015) differed significantly, univariate Cox analysis showed no significant impact on overall survival (log-rank p = 0.48), indicating these differences would not affect model construction. Kaplan–Meier survival curves demonstrated no significant difference in overall survival between the training and validation cohorts (log-rank p = 0.48; Fig. 2), indicating good comparability between the two sets and supporting the use of the validation cohort for split-sample internal validation of the model within the same institution.
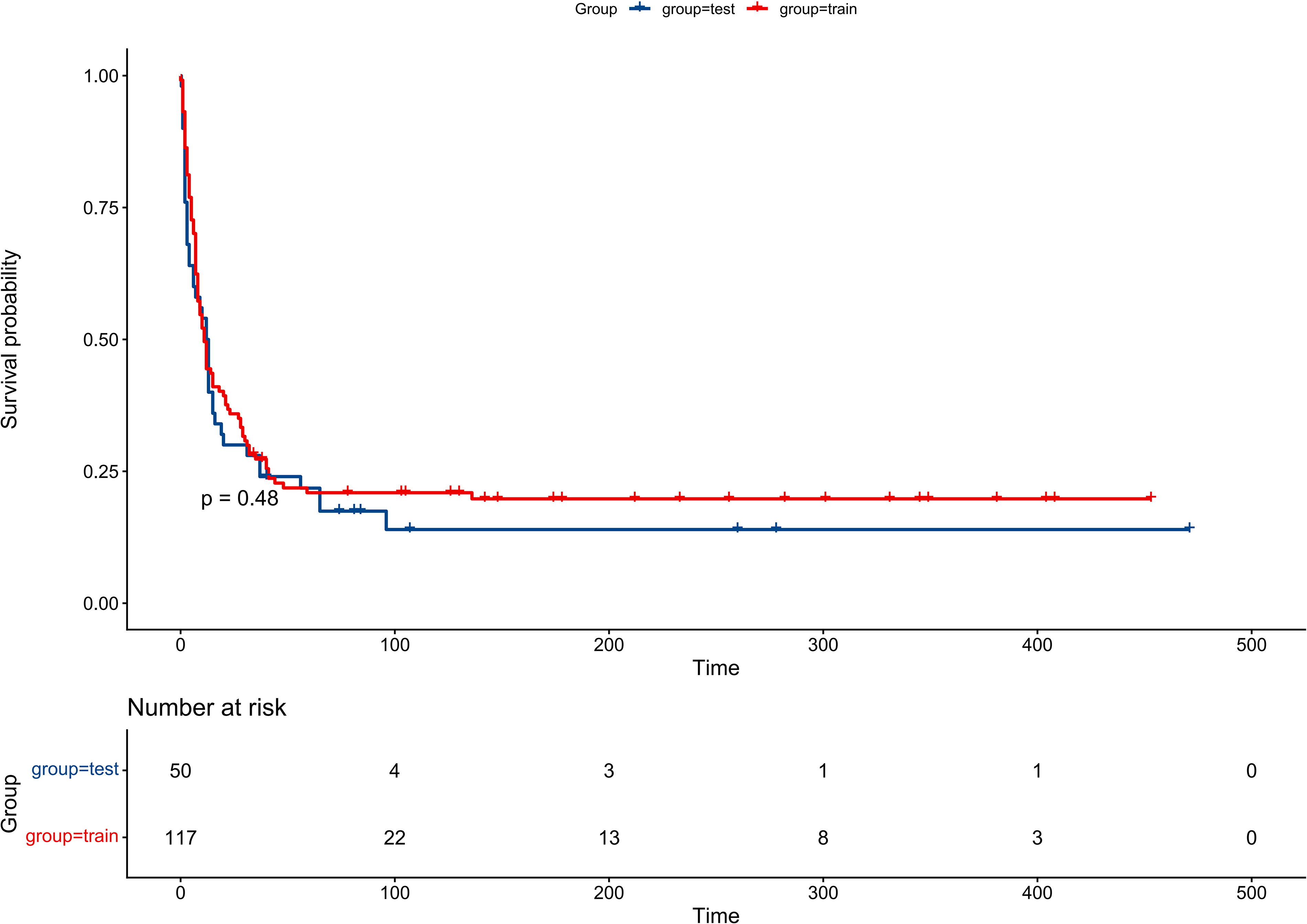
Kaplan–Meier overall survival curves for the training and validation cohorts, comparing survival outcomes between the two groups.
Baseline Characteristics of Patients Receiving Hospice Care
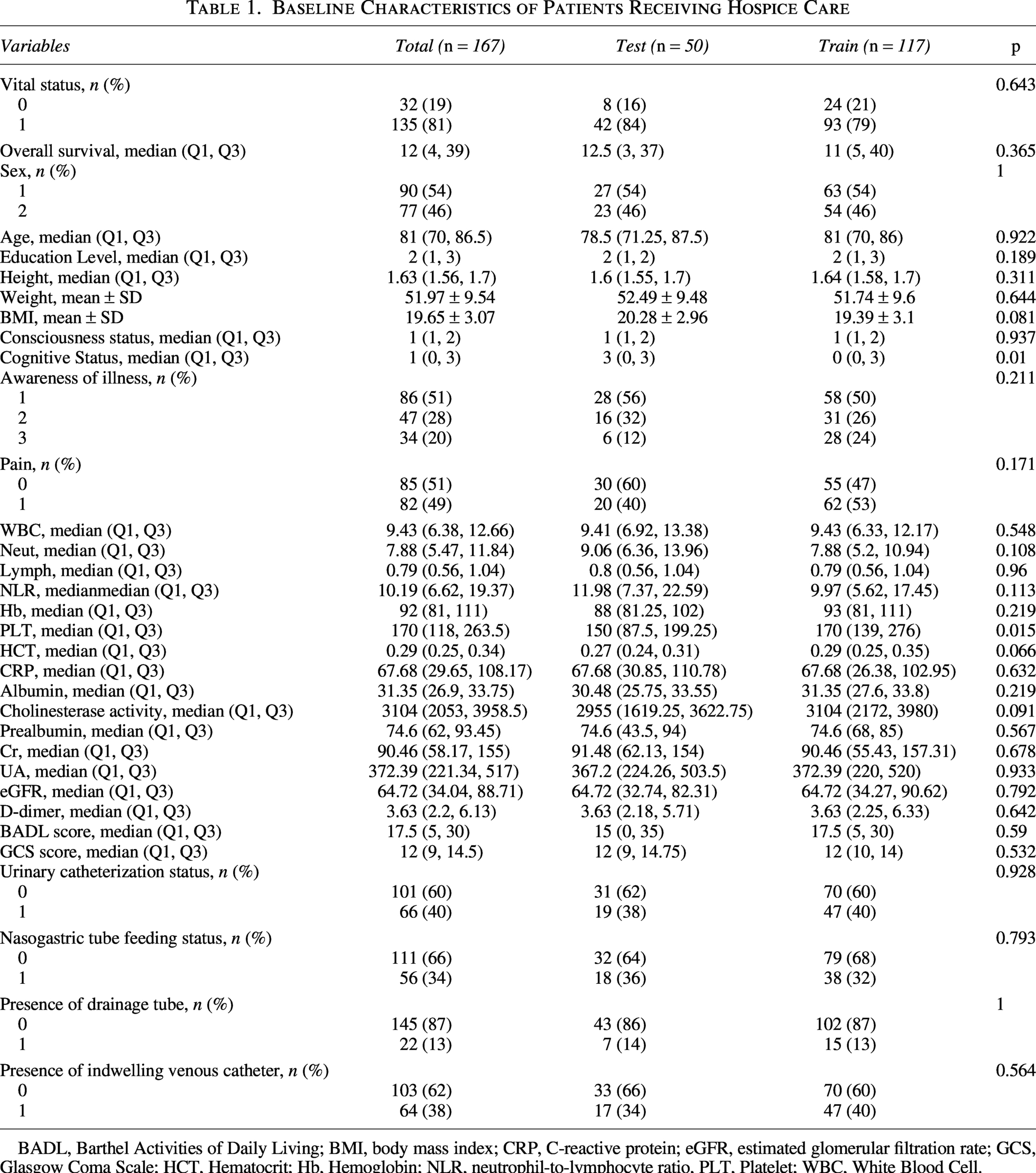
BADL, Barthel Activities of Daily Living; BMI, body mass index; CRP, C-reactive protein; eGFR, estimated glomerular filtration rate; GCS, Glasgow Coma Scale; HCT, Hematocrit; Hb, Hemoglobin; NLR, neutrophil-to-lymphocyte ratio, PLT, Platelet; WBC, White Blood Cell.
Selection of independent prognostic factors for model development
To avoid overfitting and identify the most parsimonious set of predictive factors, 31 candidate variables were analyzed using LASSO Cox regression in the training cohort. Ten-fold cross-validation and the one-standard-error rule were applied to determine the optimal regularization parameter, resulting in three variables with non-zero coefficients: CRP, eGFR, and BADL (Figs. 3–4). In multivariable Cox regression analysis, CRP emerged as an independent predictor of mortality (HR = 1.005; 95% CI, 1.001–1.01; p = 0.01), indicating that each 1 mg/L increase in CRP corresponded to an approximately 0.5% higher risk of death. In contrast, eGFR demonstrated a protective effect (HR = 0.99; 95% CI, 0.99–1.00; p = 0.01), with each 1 mL/min/1.73 m2 increase associated with roughly a 1% reduction in mortality risk. BADL showed borderline statistical significance in the multivariable Cox model (HR = 0.99; 95% CI, 0.98–1.00; p = 0.08), but it was retained in the final model because functional status is clinically central to prognostic assessment in palliative care and represents an important dimension of bedside evaluation. Therefore, variable retention was determined not only by statistical significance but also by clinical relevance and model interpretability.
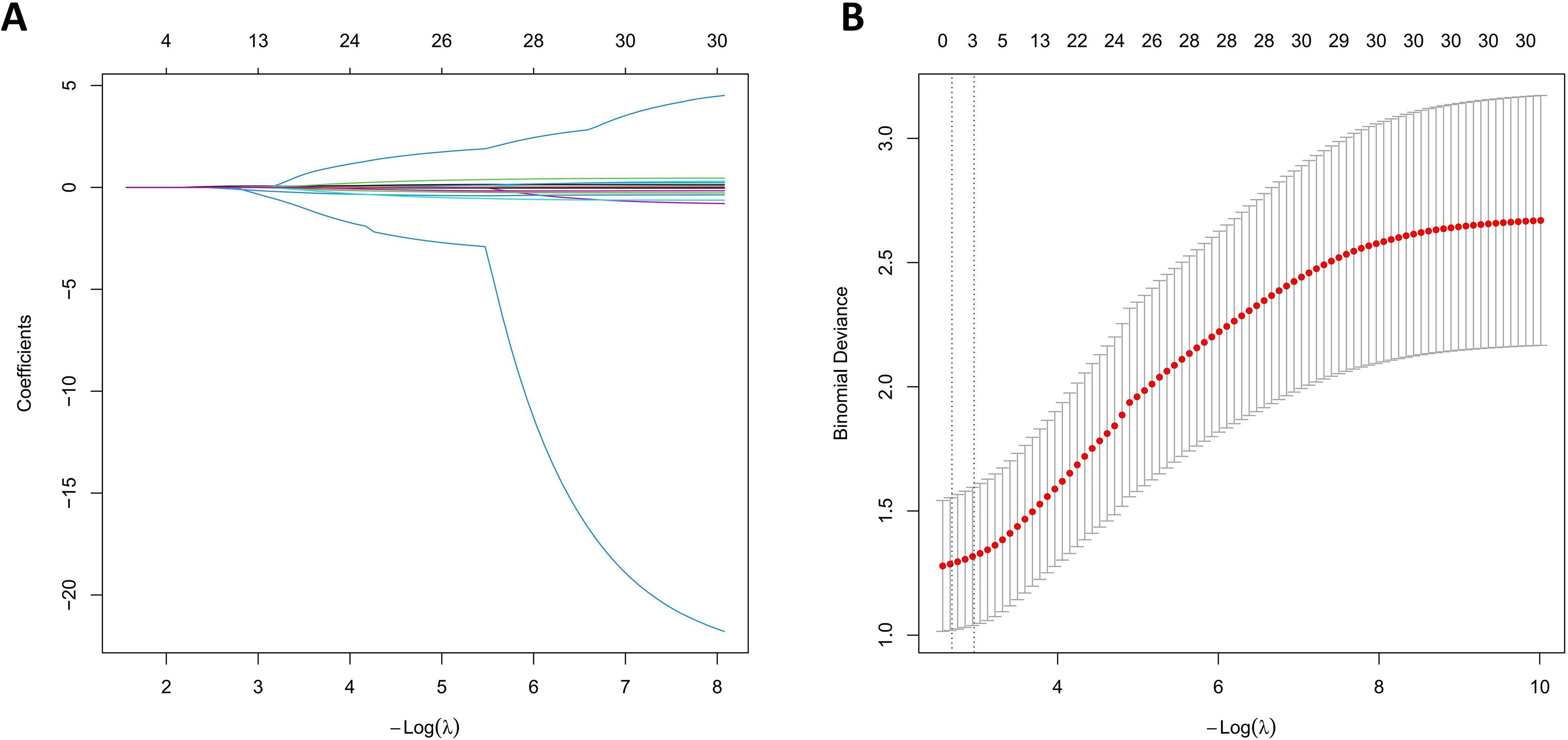
LASSO Cox regression for variable selection.
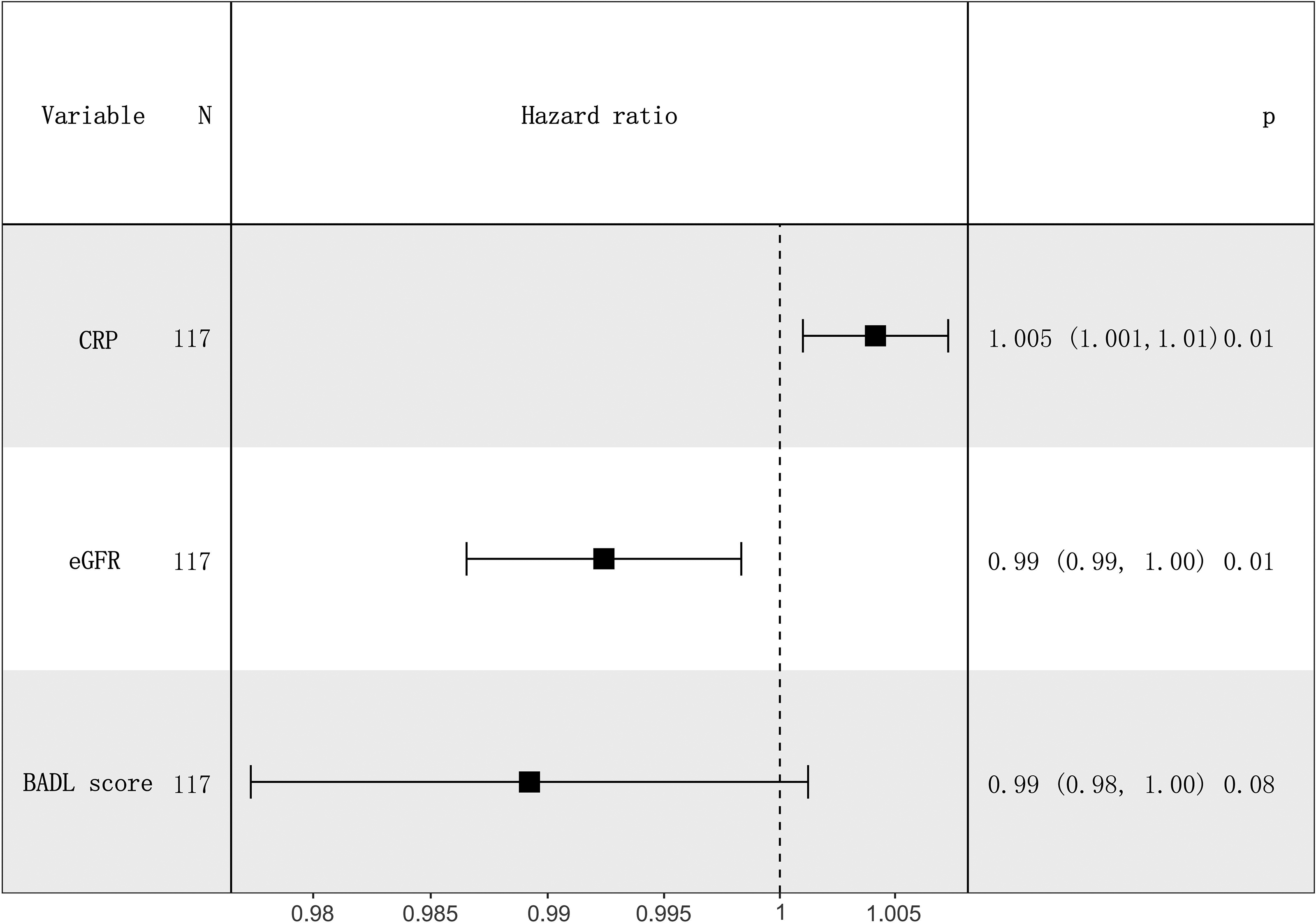
Forest plot of multivariate hazard ratios for selected variables (CRP, eGFR, BADL). HRs and 95% CIs are displayed. 95% CIs, 95% confidence intervals; BADL, Barthel Activities of Daily Living; CRP, C-reactive protein; eGFR, estimated glomerular filtration rate; HRs, hazard ratios.
Survival analysis and risk stratification based on optimal cutoff values
To improve clinical interpretability and enable risk stratification, optimal dichotomous cutoff points for the continuous variables (CRP, eGFR, and BADL) identified via LASSO Cox regression were determined using maximally selected rank statistics (maxstat), selecting thresholds that maximized separation of survival curves within the study cohort (Fig. 5). The optimal cutoffs were 13.78 mg/L for CRP, 68.46 mL/min/1.73 m2 for eGFR, and 30 points for BADL, stratifying patients into high- and low-risk groups (Figs. 6). Kaplan–Meier analyses revealed significant differences in overall survival between high- and low-risk groups for all three variables. Specifically, patients with CRP levels above 13.78 mg/L exhibited markedly poorer survival compared to those with lower CRP values (log-rank p = 0.0026; Fig. 6A). Conversely, patients with eGFR >68.46 mL/min/1.73 m2 showed better survival outcomes (log-rank p = 0.0015; Fig. 6B). Although BADL did not achieve statistical significance in the multivariable analysis (p = 0.08), patients with higher functional independence (BADL ≥30) exhibited a favorable survival trend (log-rank p = 0.042; Fig. 6C). These findings underscore the prognostic value of CRP, eGFR, and BADL in this population.
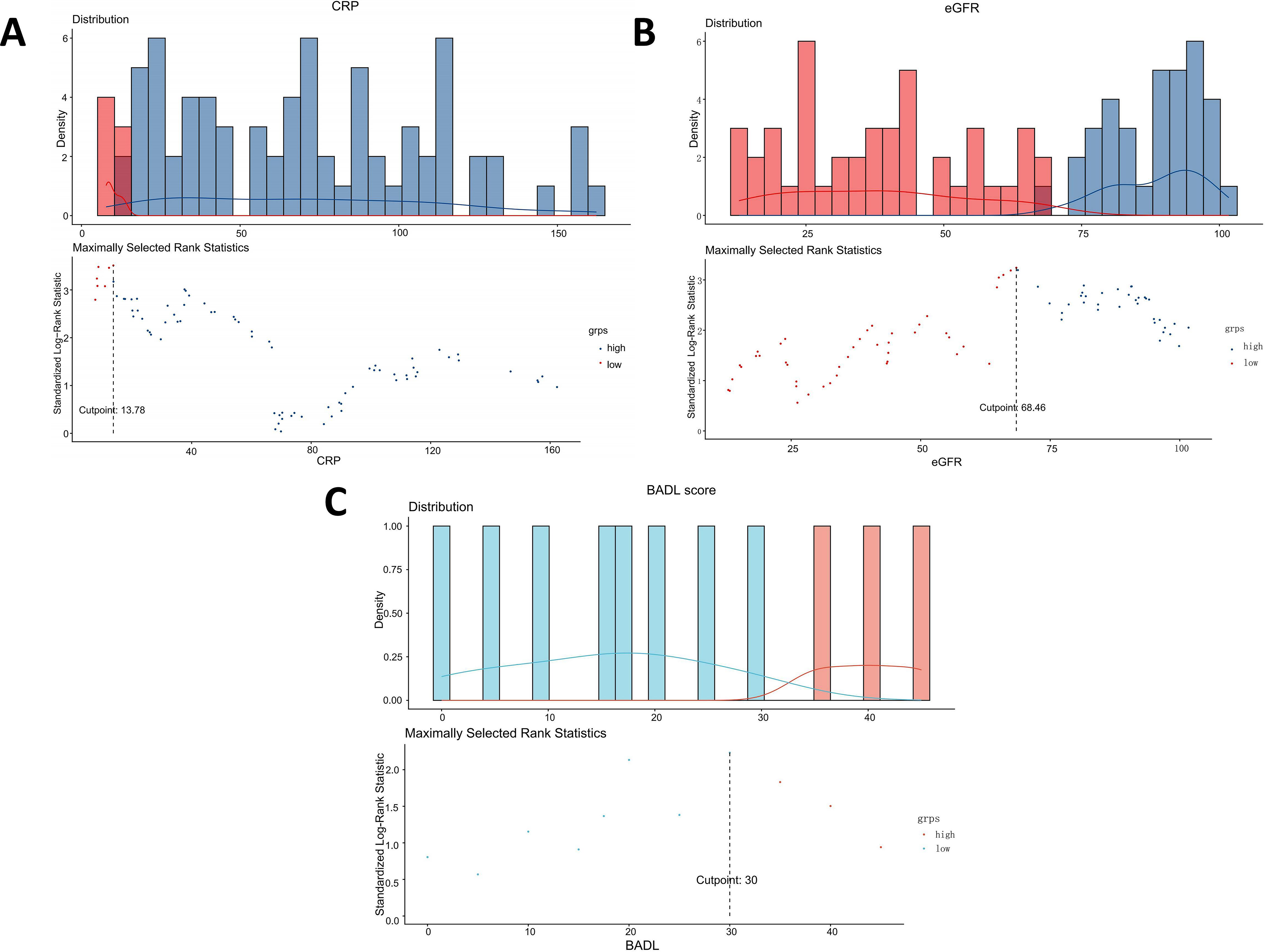
Determination of optimal cut-off values for prognostic variables using maximally selected rank statistics.
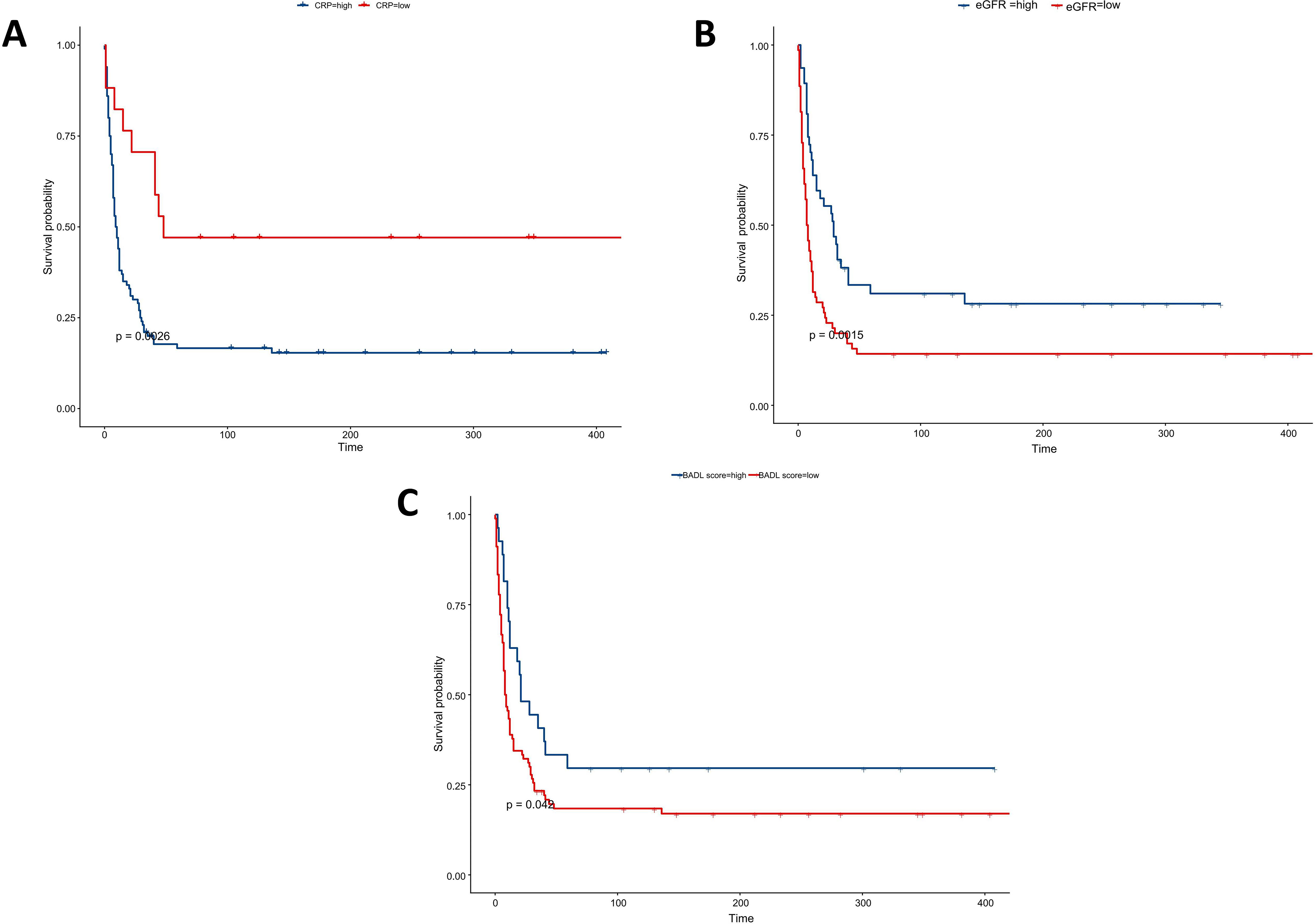
Kaplan–Meier survival curves stratified by high- and low-risk groups:
To further validate the prognostic value of the LASSO-selected variables and enhance clinical interpretability, univariate Cox regression was conducted for each high- and low-risk group (Fig. 7). Patients with lower CRP (≤13.78 mg/L) had a significantly reduced risk of death (HR = 0.33; 95% CI, 0.17–0.67; p = 0.002), whereas those with lower eGFR (≤68.46 mL/min/1.73 m2) had a significantly increased risk (HR = 1.86; 95% CI, 1.20–2.88; p = 0.006). Patients with lower BADL (<30) tended to have higher mortality risk (HR = 1.58; 95% CI, 0.94–2.65; p = 0.085), although not statistically significant at the conventional p < 0.05 level. The three-variable Cox model included 95 deaths in the training set, satisfying the 10-events-per-variable principle, supporting model reliability. These results were consistent with the Kaplan–Meier curves (Fig. 6) and further confirmed that CRP, eGFR, and BADL are independent prognostic factors in this cohort. These dichotomized cutoffs were introduced to enhance clinical interpretability and risk stratification, whereas final survival prediction was based on the combined nomogram rather than any single variable threshold. Accordingly, the contribution of BADL should be interpreted as part of the integrated prognostic model rather than in isolation.
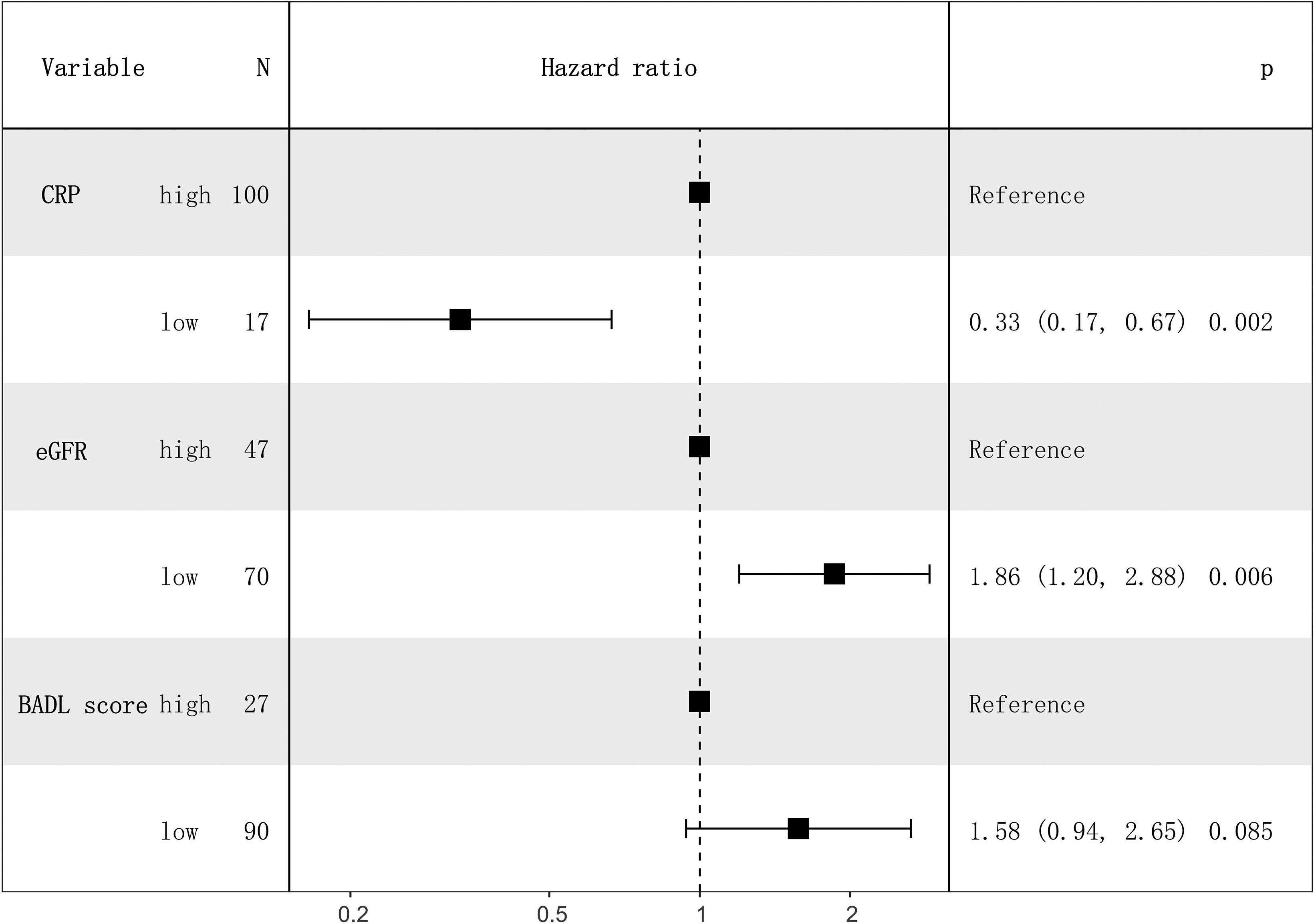
Univariate Cox regression analysis of dichotomized high- and low-risk groups based on CRP, eGFR, and BADL.
Nomogram construction
Based on the three independent prognostic factors (CRP, eGFR, and BADL) identified by LASSO Cox regression and validated through univariate Cox analysis, a nomogram was constructed to predict short-term survival probability in palliative care patients (Fig. 8). For example, a patient with a total score of 45 corresponds to an approximate 30-day survival probability of 70%, whereas a patient with a total score of 60 corresponds to a survival probability of roughly 40%, indicating that higher total scores reflect higher risk.
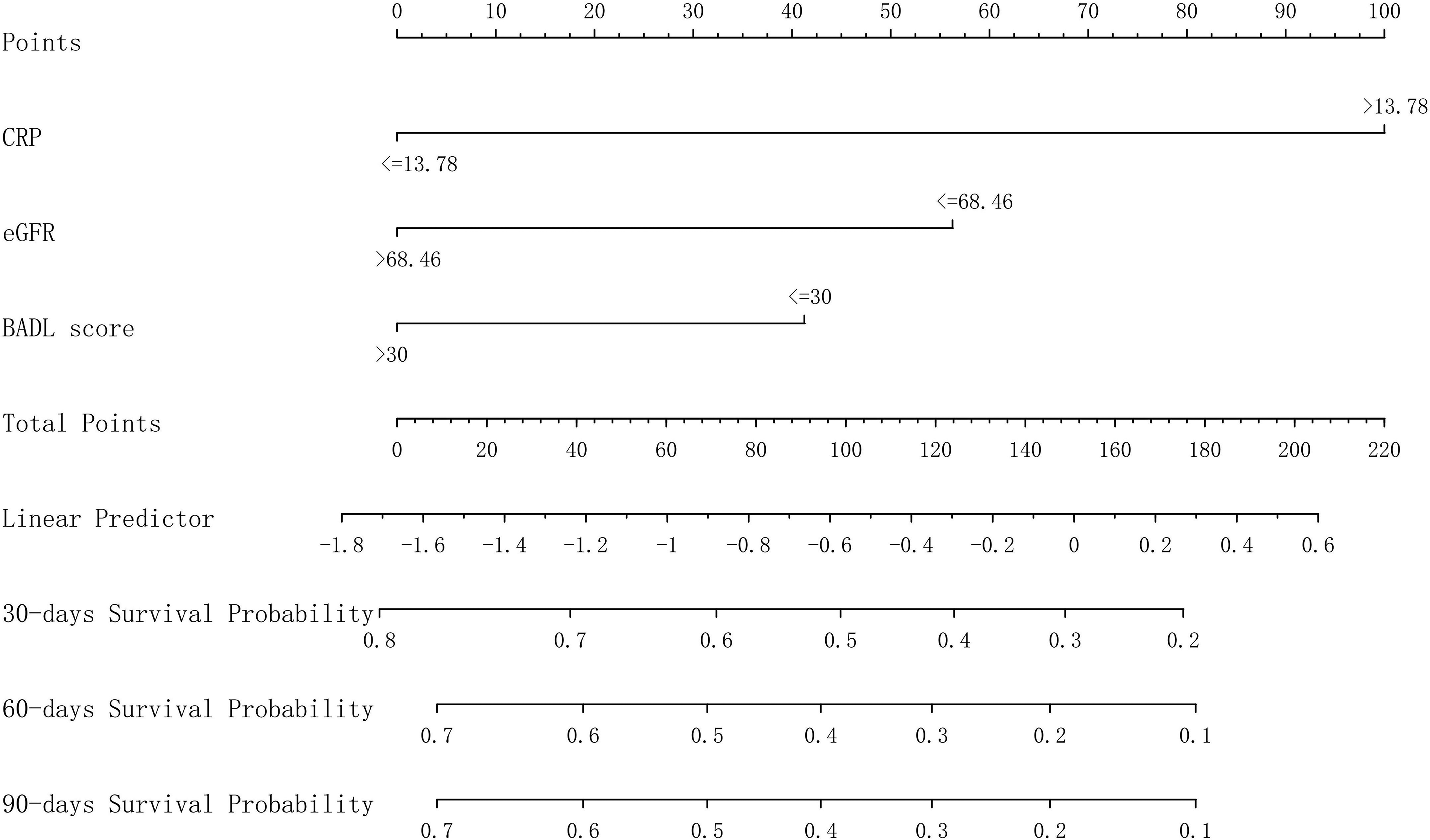
Nomogram predicting 30-, 60-, and 90-day survival probabilities in palliative care patients. Higher total points correspond to higher mortality risk.
Points were assigned according to the following risk stratification: CRP >13.78 mg/L, eGFR ≤68.46 mL/min/1.73 m2, and BADL ≤30 were each assigned higher points, with cumulative total points inversely correlated with predicted survival probability. By mapping total points to the linear predictor, the nomogram enables estimation of 30-, 60-, and 90-day survival probabilities. This visual tool integrates the three dimensions of inflammation (CRP), renal function (eGFR), and functional status (BADL), providing a simple and clinically interpretable method for short-term risk stratification and supportive prognostic assessment.
Model performance evaluation
The nomogram integrating CRP, eGFR, and BADL demonstrated good performance in discrimination, calibration, and clinical utility. Time-dependent ROC analysis revealed that the model’s AUCs for predicting 30-, 60-, and 90-day survival in the training set were 0.764, 0.716, and 0.705, respectively. Notably, the model performed similarly or even better in the split-sample internal validation set, with AUCs of 0.770, 0.748, and 0.788, indicating robustness and absence of significant overfitting (Figs. 9 and 10). Calibration curves demonstrated strong concordance between predicted and observed survival probabilities at all time points in both the training and validation cohorts, with points closely following the ideal 45° line (Figs. 11 and 12). DCA showed that the nomogram offered a positive net benefit across a wide range of risk thresholds compared with the “intervene-all” or “intervene-none” strategies, particularly for 90-day survival predictions within the 20%–40% risk range (Fig. 13). These findings indicate that the model performed favorably in terms of discrimination, calibration, and population-level clinical utility.
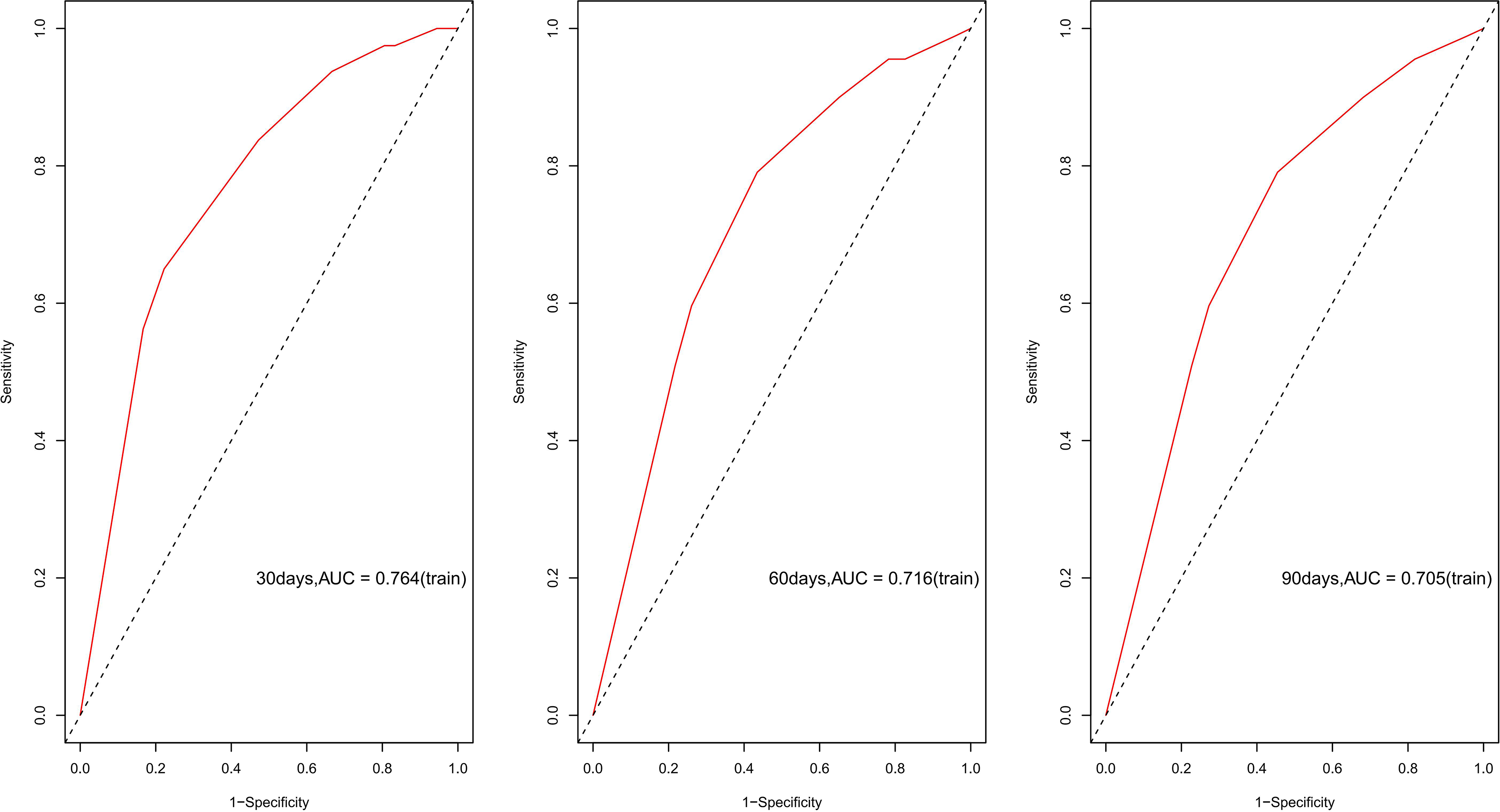
Time-dependent ROC curves for predicting 30-, 60-, and 90-day survival in the training cohort, with respective AUC values. AUC, area under the curve; ROC, receiver operating characteristic.
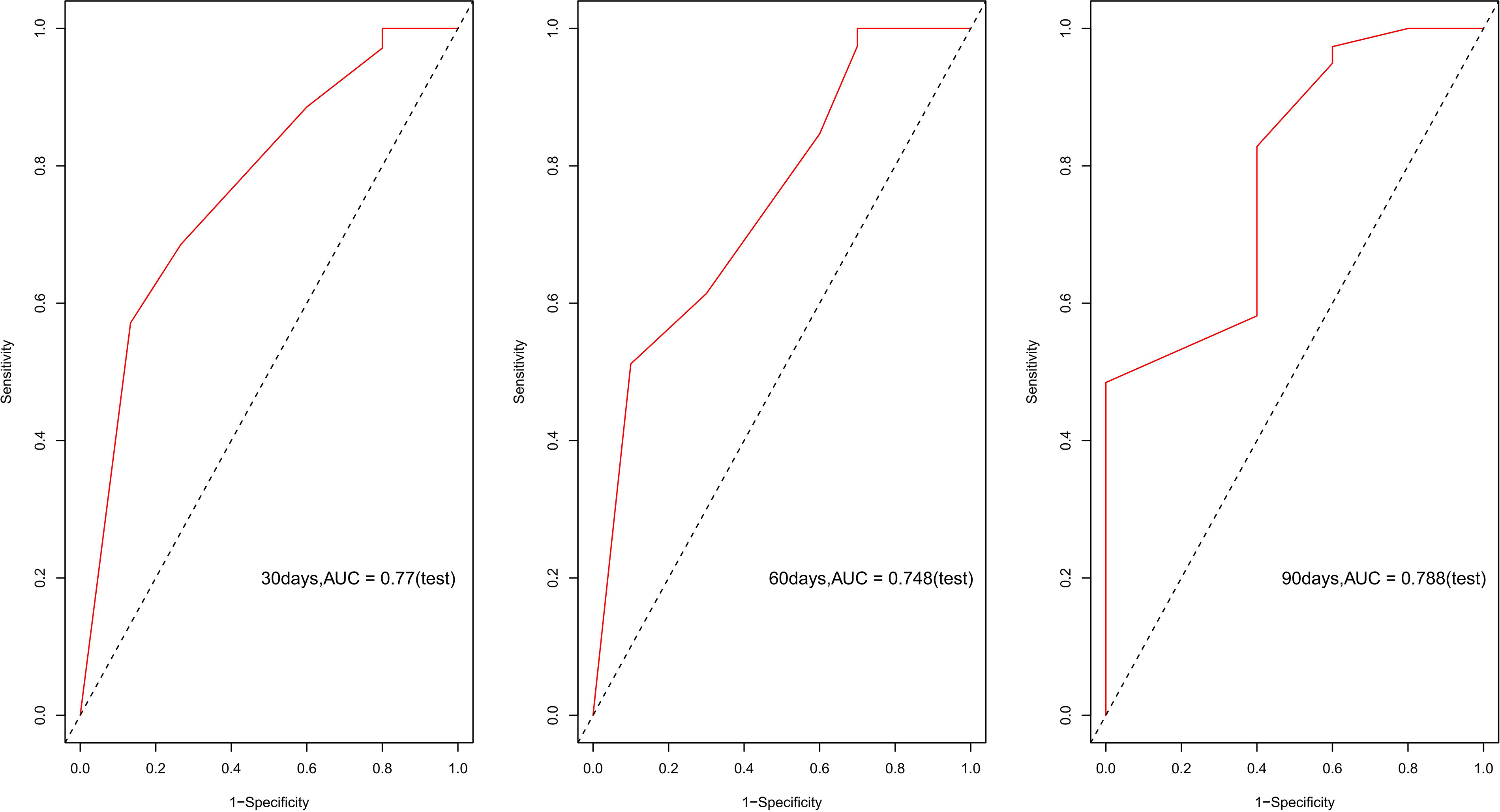
Time-dependent ROC curves for 30-, 60-, and 90-day survival predictions in the validation cohort, with corresponding AUCs.
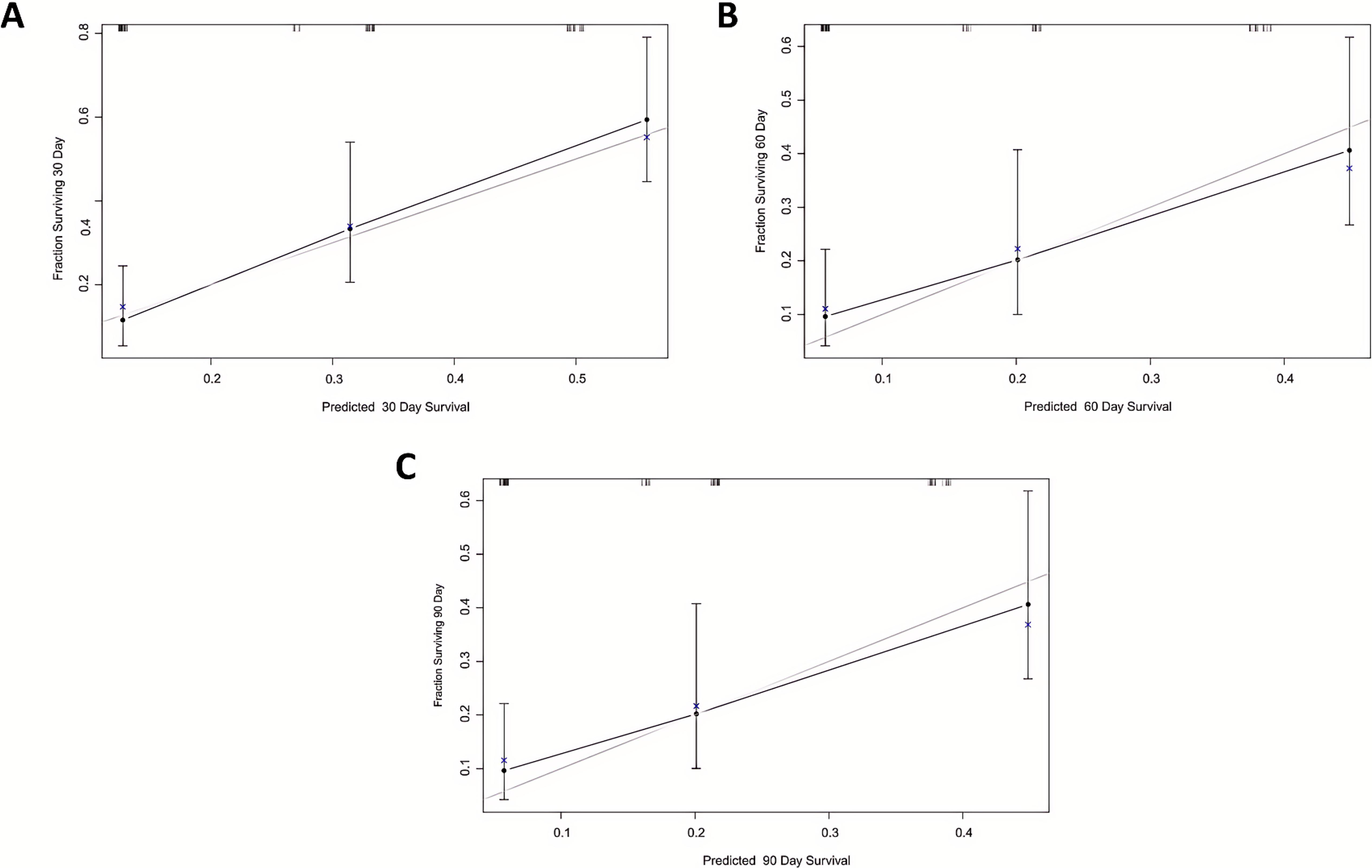
Calibration plots for the training cohort model:
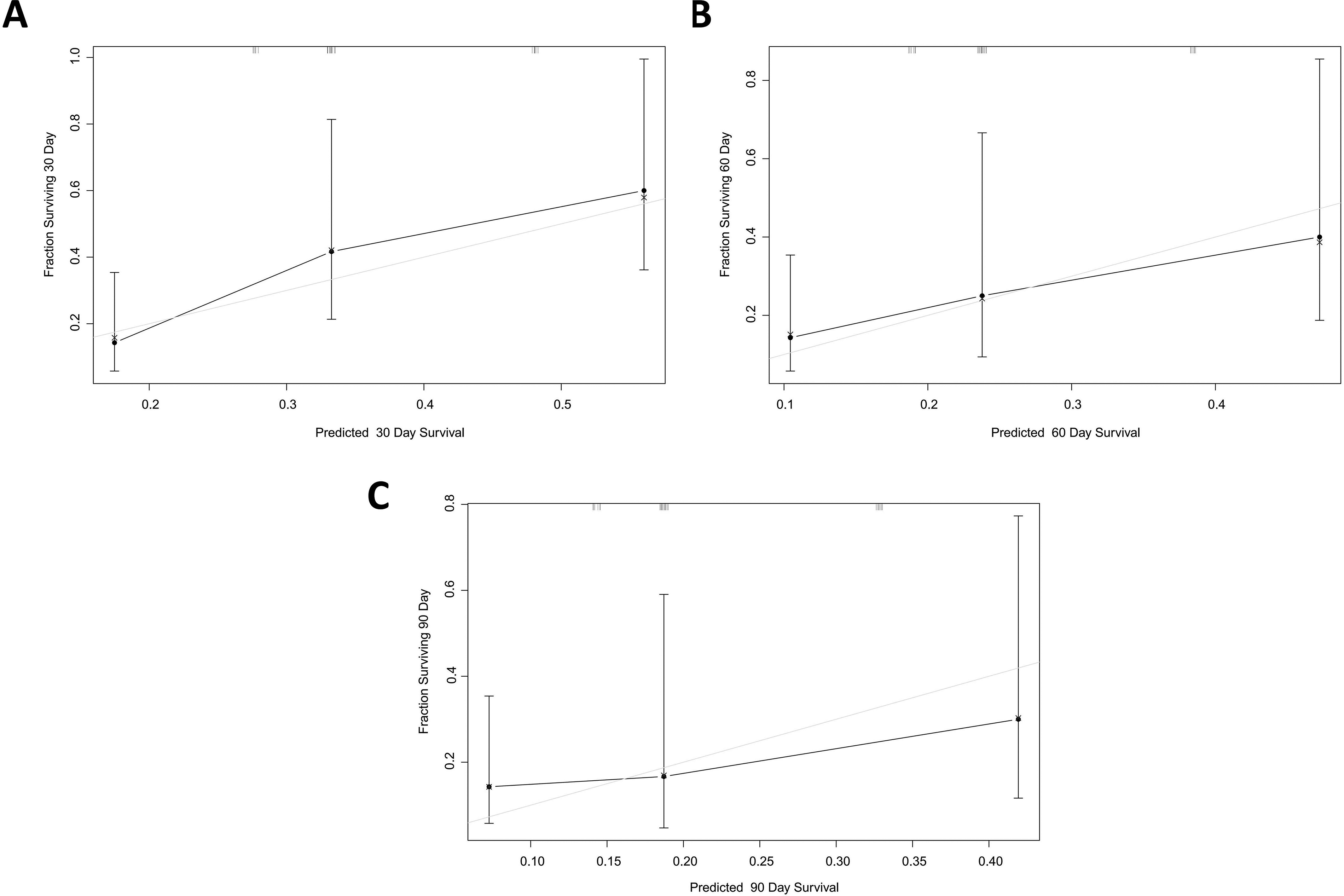
Calibration plots for the validation cohort model:
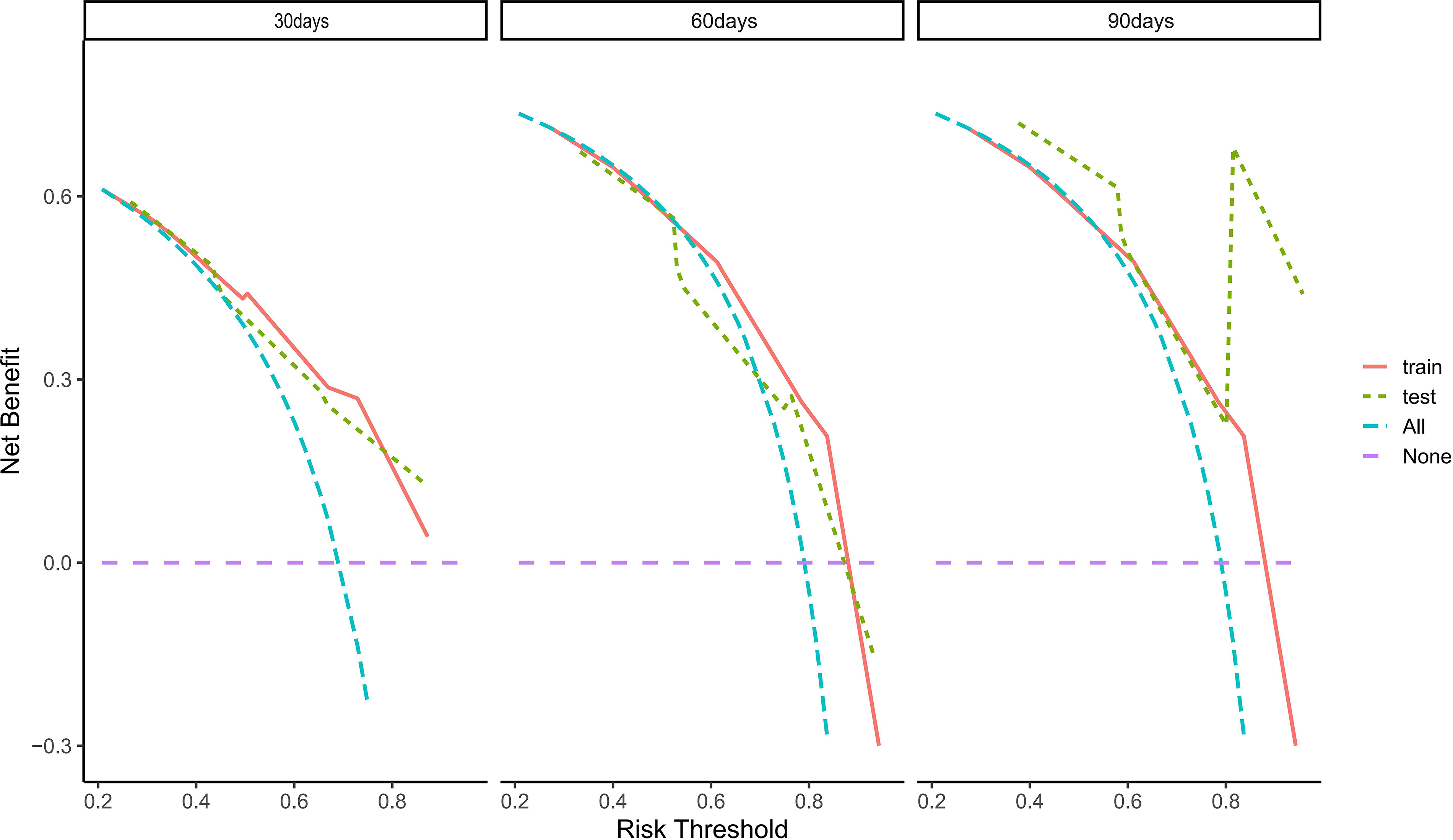
Decision curve analysis for 30-, 60-, and 90-day survival predictions. The net clinical benefit across risk thresholds is compared with “intervene-all” and “intervene-none” strategies.
Additional classification and diagnostic performance analysis were performed in the validation cohort to further assess the nomogram at 30, 60, and 90 days, including accuracy, misclassification rate, false-positive rate, and false-negative rate in addition to sensitivity, specificity, predictive values, and LRs (Table 2). At 30 days, the model showed a sensitivity of 69.05%, specificity of 75.00%, PPV of 93.55%, NPV of 31.58%, LR+ of 2.762, and LR− of 0.413. The corresponding correct classification rate was 70.00%, with a misclassification rate of 30.00%, a false-positive rate of 25.00%, and a false-negative rate of 30.95%. At 60 days, sensitivity and specificity increased to 83.33% and 87.50%, respectively, with PPV of 97.22%, NPV of 50.00%, LR+ of 6.666, and LR− of 0.191. The correct classification rate increased to 84.00%, corresponding to a misclassification rate of 16.00%, with false-positive and false-negative rates of 12.50% and 16.67%, respectively. At 90 days, the nomogram achieved its best classification performance, with sensitivity of 88.10%, specificity of 87.50%, PPV of 97.37%, NPV of 58.33%, LR+ of 7.048, and LR− of 0.136. The correct classification rate further improved to 88.00%, with a misclassification rate of 12.00%, a false-positive rate of 12.50%, and a false-negative rate of 11.90%. These results indicate that the nomogram had progressively improved classification performance over time, particularly at 60 and 90 days.
Classification and Diagnostic Performance of the Nomogram in the Validation Cohort at 30, 60, and 90 Days
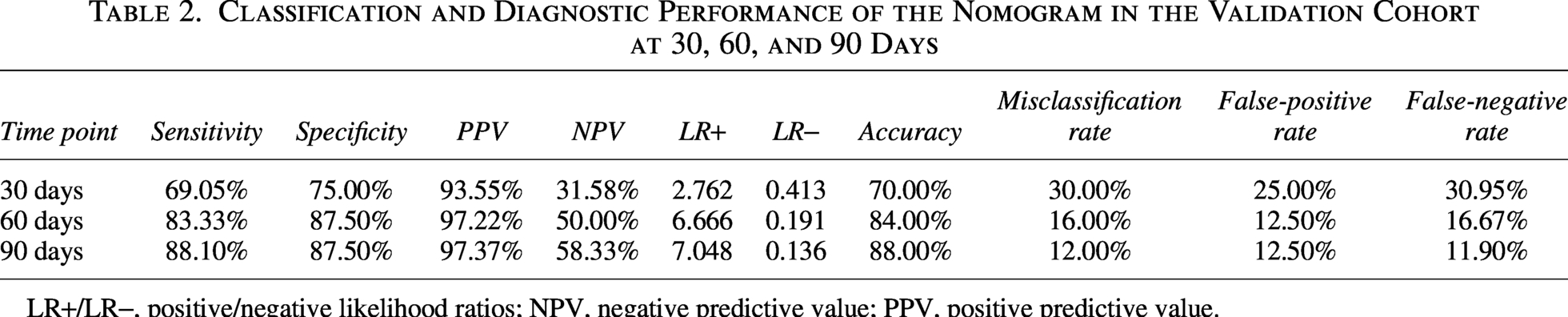
LR+/LR−, positive/negative likelihood ratios; NPV, negative predictive value; PPV, positive predictive value.
Discussion
In this study, we constructed and internally validated a reliable and interpretable nomogram for predicting short-term survival in palliative care patients. The model integrates three routinely available, low-cost, and objective clinical indicators: CRP, eGFR, and BADL score. Its primary intended use is short-term risk stratification and supportive prognostic assessment in palliative care settings, particularly to inform bedside communication and multidisciplinary discussions rather than to serve as a standalone determinant of individual clinical decisions.
The model showed good overall discriminative ability in both the training and validation cohorts, with Harrell’s C-index of 0.73 and 0.76, respectively. AUC values for 30-, 60-, and 90-day survival consistently exceeded 0.70 (training set: 0.764/0.716/0.705; validation set: 0.770/0.748/0.788). The three-variable Cox model included 95 death events in the training cohort, satisfying the ≥10 events-per-variable rule and thereby supporting the model’s reliability. Calibration plots demonstrated strong agreement between predicted and observed survival probabilities, and decision curve analysis (DCA) indicated that the nomogram provided net clinical benefit within the commonly used 20%–40% mortality risk range. However, because DCA reflects population-level net benefit rather than how an individual prediction changes posttest probability, it does not replace individual-level classification performance metrics. In addition, the dichotomized cutoffs for CRP, eGFR, and BADL were introduced mainly to improve clinical interpretability and usability. They were not intended to be used individually to predict survival; instead, prognostic estimation was based on the integrated nomogram as a whole. Therefore, we further evaluated sensitivity, specificity, predictive values, likelihood ratios, and classification error-related measures, including misclassification, false-positive, and false-negative rates, at 30, 60, and 90 days in the validation cohort to improve the clinical interpretability of the model. At the same time, retention of BADL in the final model reflected the principle that predictor selection in palliative prognostic models should consider both statistical performance and bedside clinical relevance. Because the nomogram was specifically developed to estimate 30-, 60-, and 90-day survival, interpretation of predictor effects in this study should be understood within this short-term prognostic horizon rather than as evidence for longer-term survival prediction.
The nomogram demonstrated progressively improved classification performance over time, with the best performance observed at 90 days. This finding may be explained by the reduced discriminative ability of prognostic variables in the final stage of life. As patients approach the last month of life, clinical and biological characteristics such as elevated CRP levels and functional decline (low BADL scores) tend to become increasingly prevalent and relatively homogeneous across the population. When these adverse features are almost universally expressed, their ability to distinguish between individuals with different short-term outcomes is diminished, leading to a reduction in model discrimination at 30 days.
In addition, analysis of likelihood ratios suggests that this phenomenon is not due to a shift in prognostic directionality. When negative likelihood ratios are expressed using the Weissler transformation (1/LR−), the balance between mortality-dominant (LR+) and survival-dominant information remains relatively stable across 30-, 60-, and 90-day horizons (with LR+×LR− values close to 1). This indicates that the model does not become increasingly biased toward predicting either mortality or survival over time. Rather, the observed improvement in discrimination at longer time horizons reflects an increase in the absolute strength of prognostic information, rather than a change in directional balance. In particular, the consistently high PPV values suggested that patients classified as high risk were very likely to experience short-term mortality, which may support timely goals-of-care discussions, referral planning, and appropriate resource allocation. However, the relatively modest NPV values, especially at 30 days, indicate that patients classified as lower risk may still experience early mortality and should therefore be interpreted with caution. Clinically, false-positive classification may lead to earlier goals-of-care discussions or closer monitoring in patients who ultimately survive longer than predicted, whereas false-negative classification may result in under-recognition of near-term mortality risk. The observed decline in misclassification rates from 30 to 90 days suggests that the nomogram performed more reliably at 60 and 90 days than at 30 days, although lower-risk classifications should still be interpreted cautiously. Therefore, the nomogram should be interpreted as a supportive prognostic tool in conjunction with comprehensive clinical judgment rather than as a definitive decision rule. Taken together, these findings suggest that the nomogram has favorable statistical performance and potential clinical applicability as a supportive tool for short-term risk stratification and prognostic assessment in palliative care patients.
CRP is a key prognostic marker reflecting systemic inflammation and declining physiological reserve in terminal patients and has broad predictive value across end-stage diseases.16–18 In this study, a 1 mg/L increase in CRP corresponded to a 0.5% higher risk of mortality (HR = 1.005, p = 0.01). Patients with high CRP (>13.78 mg/L) showed significantly poorer short-term survival, consistent with the direction of effect observed in the Kaplan–Meier analysis and the nomogram predictions for 30-, 60-, and 90-day survival. This supports the role of CRP as a clinically relevant marker for short-term prognostic assessment in palliative care. Notably, the cut-off value of 13.78 mg/L determined by maximally selected rank statistics is close to the clinically recognized threshold for mild inflammation (normal < 10 mg/L), demonstrating good clinical relevance. These results align with previous research indicating that systemic inflammation contributes to muscle wasting (cachexia), impairs immune function, and triggers endothelial damage and multi-organ dysfunction. In noncancer terminal patients, such as those with acute exacerbations of COPD or decompensated heart failure, CRP levels are often elevated, reflecting heightened disease activity and sharply reduced physiological reserve. 19 Therefore, CRP, as an objective, low-cost, and widely accessible marker of inflammation, effectively quantifies patients’ “biological age” and disease burden, complementing subjective clinical assessments. 20
eGFR is an important marker of organ function and systemic frailty. 21 In this study, a 1 mL/min/1.73 m2 decline in eGFR was linked to a 1% higher mortality risk (HR = 0.99, p = 0.01), and patients with eGFR ≤68.46 mL/min/1.73 m2 also showed poorer short-term survival, supporting the value of renal functional decline as a predictor within the 30-, 60-, and 90-day prognostic horizon. This finding is underpinned by pathophysiology: terminal patients often experience renal function decline due to dehydration, hypoperfusion, drug toxicity, or progression of chronic kidney disease, which in turn further compromises overall physiological reserve. Even in patients without primary renal disease, mild reductions in eGFR are closely linked to adverse outcomes, highlighting its value as a marker of systemic vulnerability. 22 Compared with serum creatinine alone, eGFR incorporates age, sex, and body weight, providing a more accurate reflection of renal function and greater stability for prognostic prediction, making it suitable as a core input for assessing systemic frailty and organ function.23,24
The BADL score is a key functional measure that rapidly reflects patients’ functional independence and systemic vulnerability at the bedside.25,26 Although BADL showed only borderline statistical significance in the multivariable Cox model (p = 0.08), it was retained because functional decline is a core component of prognosis in palliative care and provides clinically meaningful information that may not be fully captured by laboratory indicators alone. In our study, patients with BADL < 30 tended to have a higher mortality risk, and Kaplan–Meier analysis further demonstrated significant survival differences between BADL-based groups (p = 0.042), supporting the clinical relevance of functional status in short-term end-of-life prognostic assessment. Therefore, the inclusion of BADL was intended to enhance the clinical interpretability and bedside applicability of the nomogram, rather than to emphasize statistical significance alone. BADL assessment requires no specialized equipment and can be performed by nursing staff or family members, offering convenience and direct clinical relevance. This aligns well with Chinese elderly palliative care culture and high levels of family involvement, allowing short-term survival evaluation to naturally integrate with quality-of-life considerations, thereby enhancing the model’s clinical applicability and communication effectiveness. 27
Compared with previous studies, our model demonstrates clear advantages in population inclusivity and methodological simplicity and robustness. Gui et al. developed a nomogram based on five clinical and laboratory variables—including treatment preference, dyspnea, serum albumin, blood urea nitrogen, and neutrophil count—in patients with terminal cancer. 14 However, their cohort was limited to advanced malignancies, restricting generalizability to a broader, more diverse population of noncancer terminal illnesses (e.g., heart failure, COPD, and neurodegenerative diseases), which constitute the majority of real-world palliative care patients. In contrast, our model was developed and internally validated using a split-sample approach in a mixed cohort of cancer and noncancer terminal patients, reflecting the clinical diversity of modern palliative care practice and potentially improving its applicability across a broader palliative care population, although formal external validation is still required.
Additionally, prior models such as those by Ruggiero et al. (hip fracture survival prediction) and Wang et al. (cardiovascular event prediction in acute coronary syndrome) primarily relied on physiological or laboratory indicators using traditional Cox proportional hazards regression.15,28 In contrast, our study uniquely incorporates patient-centered nonphysiological factors, such as treatment preferences, symptom burden, and functional status, together with objective biomarkers, in line with the World Health Organization’s definition of palliative care as “an approach that improves the quality of life of patients and their families facing life-threatening illness”. 29 This integration addresses a notable gap in existing models that often overlook psychosocial dimensions.
Methodologically, we employed LASSO-Cox regression to optimize variable selection, reducing overfitting risk and ensuring model simplicity and robustness. The model underwent rigorous evaluation using a split-sample internal validation cohort, time-dependent ROC curves, calibration plots, and DCA, demonstrating substantial net clinical benefit across a broad spectrum of risk thresholds and outperforming “treat-all” or “treat-none” approaches. Collectively, this study presents a practical multivariable survival prediction tool combining population inclusivity, methodological simplicity, and clinical interpretability. By integrating three routine, low-cost clinical indicators, CRP, eGFR, and BADL score, the nomogram is simple, intuitive, and may be readily used for outpatient screening, inpatient risk stratification, bedside communication, or multidisciplinary discussions, thereby enhancing its feasibility and translational potential in clinical practice.
Nevertheless, several limitations merit consideration. First, this study was a single-center retrospective cohort with a relatively small sample size, and the nomogram was developed for 30-, 60-, and 90-day short-term survival prediction, which may restrict its utility for longer-term prognostic assessment. Given the retrospective design and single-center setting, the study may be susceptible to both selection bias and information bias. For example, certain patient populations may have been more likely to be included, and some clinical information may have been incompletely documented, which could affect the generalizability of the model. In addition, because all patients were recruited from a single institution in Shenzhen, the generalizability of the model to other clinical settings and populations remains uncertain. Moreover, although a separate validation cohort was used, this cohort was derived from the same institution through a split-sample approach and therefore represents internal validation rather than true external validation. Differences in healthcare systems, referral patterns, disease spectrum, and palliative care practices across different regions of China and other countries may affect the model’s performance. Therefore, further multicenter studies with larger sample sizes, including patients from different regions in China as well as international populations, are needed to externally validate and refine this nomogram before broader clinical application. Second, although AUC values >0.70 indicate clinically acceptable performance, further improvements are possible. Future models could incorporate nutritional assessment (e.g., NRS2002), comorbidity burden (e.g., Charlson comorbidity index), or composite inflammatory indices (e.g., systemic immune-inflammation index, platelet-to-lymphocyte ratio, systemic inflammation response index), or apply more advanced algorithms such as random survival forests or deep learning to enhance predictive accuracy and external generalizability.
Nonetheless, the present model is innovative in several aspects: it encompasses a mixed cohort of malignant and nonmalignant terminal patients, integrates functional status with objective inflammation and organ function markers, and employs LASSO-Cox regression combined with maximally selected rank statistics for simplified modeling and clinically interpretable risk stratification, thereby extending the applicability and generalizability of short-term survival prediction tools in palliative care. Although established prognostic tools such as PPS and PaP are widely used in clinical practice, a direct quantitative comparison with the present nomogram was not performed in this study. This is partly because these tools typically provide relatively broad prognostic categories or survival ranges rather than precise time-specific probability estimates, making direct comparison with a time-dependent prediction model challenging. In addition, their reliance on subjective clinical judgment may further limit comparability with models based primarily on objective variables. Future studies incorporating standardized head-to-head comparisons are warranted to better evaluate the relative performance and clinical utility of different prognostic approaches. Future directions include developing an online calculator or mobile application to enable rapid bedside assessment in clinical, caregiving, and home settings, supporting shared decision-making and optimizing palliative care resource allocation, ultimately improving quality of life for terminal patients.
Conclusion
We successfully developed a simple, transparent, and clinically actionable nomogram for predicting 30-, 60-, and 90-day short-term survival by integrating objective biomarkers (CRP and eGFR) with functional status assessment (BADL score). This model provides individualized, quantifiable survival risk predictions for palliative care patients. The nomogram exhibits strong discrimination and calibration and can be readily applied at the bedside or in multidisciplinary team discussions, providing an evidence-based tool for clinical risk stratification, prognostic communication, and care planning. Future efforts will focus on developing an online calculator or mobile application to facilitate rapid implementation across clinical, caregiving, and home contexts, supporting shared decision-making, optimizing resource allocation, and ultimately enhancing the quality of life for terminally ill patients. This tool not only provides a practical approach for short-term prognostic assessment in palliative care but also offers a new avenue for personalized care and evidence-based decision-making.
Footnotes
Acknowledgments
We sincerely thank all patients and their families for participating in this study. We are grateful to the staff of The Second People’s Hospital of Futian District Shenzhen for their assistance with patient recruitment and data collection. We also appreciate Chao Qin (Senior Engineer, Qualcomm Communication Technologies, Shenzhen) for statistical guidance and Lei Su (Associate Chief Physician, The First Affiliated Hospital of Sun Yat-sen University) for valuable comments on article revision.
Authors’ Contributions
L.T. conceived the study and wrote the main article text. L.Y., Y.H., and Z.C. contributed to study design and article revision. Y.L., W.G., J.L., S.Z., and Z.G. were responsible for patient data collection, follow-up, and documentation. G.W. and W.Z. established and maintained the database. C.Q. performed statistical analysis using R and prepared the figures. All the authors reviewed and approved the final article.
Data Availability Statement
The datasets generated or analyzed in this study are not publicly available due to patient privacy and ethical considerations but can be obtained from the corresponding author upon reasonable request. Requests for access should be directed to L.T. and will be evaluated on a case-by-case basis with approval from the Institutional Ethics Committee.
Ethical Statement
This study was approved by the Ethics Committee of The Second People’s Hospital of Futian District Shenzhen (Approval Number: 20250402094401). As a single-center retrospective cohort study involving anonymized patient data, the requirement for written informed consent was waived in accordance with the Declaration of Helsinki and relevant national regulations. All patient data were handled confidentially, and no interventions were performed that affected patients’ clinical care.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
This study was funded by the Chronic Disease Management Research Project of the National Health Commission Capacity Building and Continuing Education Center (grant No. GWJJMB202510010088) awarded to L.T.