
Abstract
Patients with serious medical illnesses may respond to the challenges of their illness in unique ways, shaped by personal, relational, and contextual factors. For many patients, depression and anxiety are common and may feature avoidance or withdrawal, negative expectations for outcomes, repetitive negative thinking (rumination and/or worry), sad mood, and/or irritability. These symptoms often arise from a complex and bidirectional interplay between a patient’s emotions, thoughts, and behaviors. This dynamic system provides clinicians with multiple, clinically actionable entry points to foster patient engagement in treatment and coping with serious illness. This article illustrates how core principles from cognitive behavioral therapy (CBT) can inform serious illness communication, adapted for use by general palliative care clinicians in appropriate clinical contexts. Using a composite clinical case, we demonstrate the use of CBT principles as a way of organizing our clinical understanding of a patient who is feeling “stuck,” from which CBT-informed techniques, such as guided discovery, cognitive restructuring, and behavioral experiments, can be implemented to reduce distress and promote adaptive coping.
Keywords
Introduction
Cognitive behavioral therapy (CBT) is a well-established, empirically supported therapy that has been successfully applied to treating patients with a wide variety of serious medical illnesses.1–7 CBT is grounded in the premise that emotional distress is shaped not only by external circumstances but also by how individuals interpret and respond to those circumstances.8,9 A foundational element of CBT is developing a case formulation, or working hypothesis, about a patient’s core psychological struggle that integrates thoughts, emotions, behaviors, and contextual factors.8–10 This in turn serves as a clinical compass, guiding the selection of cognitive and behavioral interventions to influence emotional experience and coping. 11
In palliative care settings, depressive or anxious symptoms can manifest in patients feeling “stuck,” characterized by diminished agency, behavioral withdrawal, or fixation on negative predictions about the future. In such presentations, CBT-informed serious illness communication (SIC) strategies may serve as effective tools for palliating distress.1,6 This article explores how CBT-informed skills—such as guided discovery, cognitive restructuring, and behavioral experiments—can be intentionally applied by general palliative care clinicians to support more flexible adaptation to the realities of serious illness. A sample composite case will be used to illustrate integration of these skills into palliative care practice to help patients who feel “stuck” re-engage with life in the context of serious illness. This article is the third in a nine-article series on psychotherapeutically informed SIC.
Case Description
Norah is a 27-year-old cis woman undergoing treatment for Hodgkin’s lymphoma who presents for follow-up in an outpatient palliative care clinic for symptom management and psychosocial support.
Ahead of her visit, Norah’s mother sent a message to the clinical team expressing concern that Norah has become increasingly disengaged and withdrawn. When her mother attempts to engage with her, Norah often shuts down or leaves the room. Despite improving white blood cell counts and medical clearance to resume normal activities, Norah remains isolated, sad, and fearful.
When asked about her mood, Norah replies, “It sucks. I have cancer. Anybody would be depressed, but there’s nothing I can do. Just this weekend I missed the show all my friends were at. I watched it on all their online stories.” She trails off, looks down at the floor, and becomes silent.
When asked why she opted not to attend the show despite being medically cleared, Norah remained silent for a moment before blurting out, “No one wants to see me. I’m the ‘Sad Girl with Cancer.’ It just depresses everyone when I’m around. No one knows what to say, and it makes everything weird. It’s better if I just stay home.”
Discussion
Norah’s sense of being “stuck” appears deeply intertwined with and reinforced by her feelings (e.g., depression and sadness), her cognitions (e.g., “No one wants to see me. I’m the ‘Sad Girl with Cancer'”), and her behaviors (e.g., disengagement and withdrawal). Appreciating the ways these contributors perpetuate Norah’s distress, clinicians can identify multiple clinically actionable entry points for palliating her emotional suffering. SIC techniques informed by CBT principles may be particularly well-aligned with Norah’s underlying psychological needs.
CBT principles: The cognitive triangle
The CBT framework, developed by Dr. Aaron Beck, proposes a bidirectional relationship between thoughts, behaviors, and emotions, as conceptualized through the CBT cognitive triangle (see Fig. 1).8,9
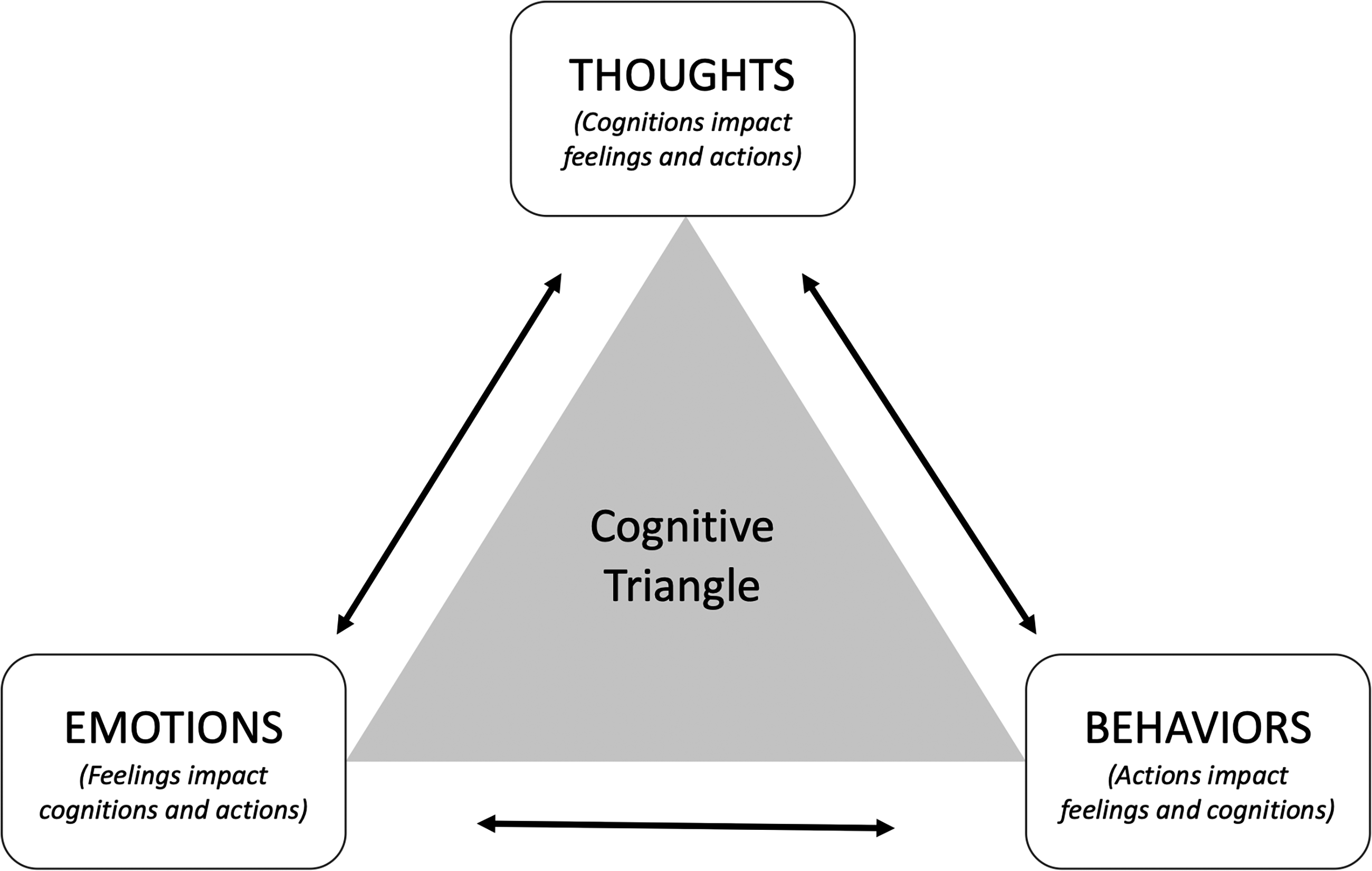
Life experiences are interpreted through an individual’s thoughts and beliefs, which in turn shape their emotional and behavioral responses. Importantly, different individuals may respond quite differently to the same activating event, a phenomenon commonly observed in serious illness care. Moreover, the consequences vary depending on the person’s underlying beliefs, cognitions, or habits. Due to the bidirectional relationship between thoughts, emotions, and behaviors in the cognitive triangle, some patients may feel stuck or trapped in their distress. Mapping the relevant details onto this framework helps clinicians conceptualize a given patient’s pattern of distress and understand how it is being maintained.
With Norah, for example, perceived sadness in her friends appears to have been an activating event for her distress. The thoughts she shares suggest an underlying belief that she is the cause of their perceived sadness (e.g., “No one wants to see me,” “I depress everyone,” and “It’s better if I stay home”). Behaviorally, she is isolating, withdrawing, and disengaging from meaningful relationships to protect others from being around her. Emotionally, she is left feeling “stuck,” depressed, and somewhat hopeless. These thoughts, emotions, and behaviors are all self-reinforcing, resulting in elevated, sustained levels of distress that she is having trouble breaking free from.
The foundational premise is that helping a patient like Norah recognize and understand this process through collaborative exploration can empower her to influence her emotional experience. Clinicians partner with patients to develop awareness of the hidden logic linking thoughts, emotions, and behaviors that shape each person’s experience of distress. From here, rather than simply telling somebody to “feel differently,” therapeutic attention can be directed toward thoughts that are centrally implicated in suffering, particularly when these beliefs contain distortions or interfere with effective adaptation to current life circumstances, as well as toward behaviors that reinforce suffering. Through joint exploration, we can support a patient in considering alternative perspectives and developing greater flexibility in responding to the realities of their situation. While operationalized CBT therapy would be outside the scope of general palliative care practice, the section that follows explores ways that foundational principles of CBT can inform SIC strategies.
SIC techniques aligned with CBT principles
Clinician: Gosh, Norah, this sounds really challenging. Even though you received medical clearance to resume parts of your life, it seems you are still feeling disconnected. (Validation) Norah: What life?! My life basically ended when I started treatment. No one even knows how to talk to me anymore, and I don’t think they really want to anyway. Nobody gets it or knows what to do. Clinician: Well, I don’t know if I get it yet, but I’d like to try. Do you think I could hear a little more about what’s been going on so I can try to understand a little better? Norah: What is there to know? I told you I’m the “Sad Girl with Cancer.” Everyone just gets depressed when I’m around. Clinician: That phrase, “Sad Girl with Cancer,” really stands out to me. Where did that come from? Did someone say that to you? Norah: No. My friends never said that to me. But I can just tell. Whenever I see my friends, they look so sad. I just depress everyone when I am around. It is like the sadness is contagious. This statement from Norah represents a potential key (or “hot”) cognition, meaning a belief that is strongly linked to emotional distress. Norah may be accurately perceiving sadness in her friends, or she may be making assumptions about ambiguous or neutral cues. Our aim is not necessarily to change Norah’s mind or persuade her to adopt a different belief, but rather to increase her awareness of thoughts that contribute to feeling “stuck,” which lays the groundwork to consider alternative possibilities. Clinician: I can see how that would really sting and make you want to retreat. Have you ever tried talking to your friends about any of this? Norah: It would be hard to talk about. When people do visit, half the time we just sit there. They don’t seem to want to talk to me anymore. Clinician: It sounds like talking might feel uncomfortable for everyone. Can you think of any other reason your friends might go quiet when you are together? Norah: Like what? Clinician: Well, I can make some guesses, but you know them best. I wonder if you think it’s possible that they might be afraid of saying something that could upset you or whether they might think silence is safer than risking saying the wrong thing. Norah: Maybe they don’t know what to say, like you said. I don’t know, I hadn’t really thought about that before. In this example of cognitive restructuring, we focus on Norah’s interpretation of her friends’ apparent quietness. However, several additional hypotheses could be explored based on what has already emerged, including the source of her friends’ sadness, whether they truly are feeling sad, and whether social withdrawal is the only response to the discomfort she perceives. As we work collaboratively with Norah to identify her beliefs and cognitions, we assess them together for possible distortions, such as whether she may be making assumptions about the meaning of her friends’ silence. Table 1 reviews different cognitive distortions frequently encountered in serious illness care. Importantly, the goal is not to argue with Norah or persuade her that her interpretation is incorrect. Rather, by gently exploring beliefs on both sides of this equation, clinicians can support patients in arriving at a less distorted understanding of their situation and, in many cases, recognizing greater resilience and coping capacity than they initially perceived.
Cognitive Distortions Commonly Encountered in Serious Illness Care
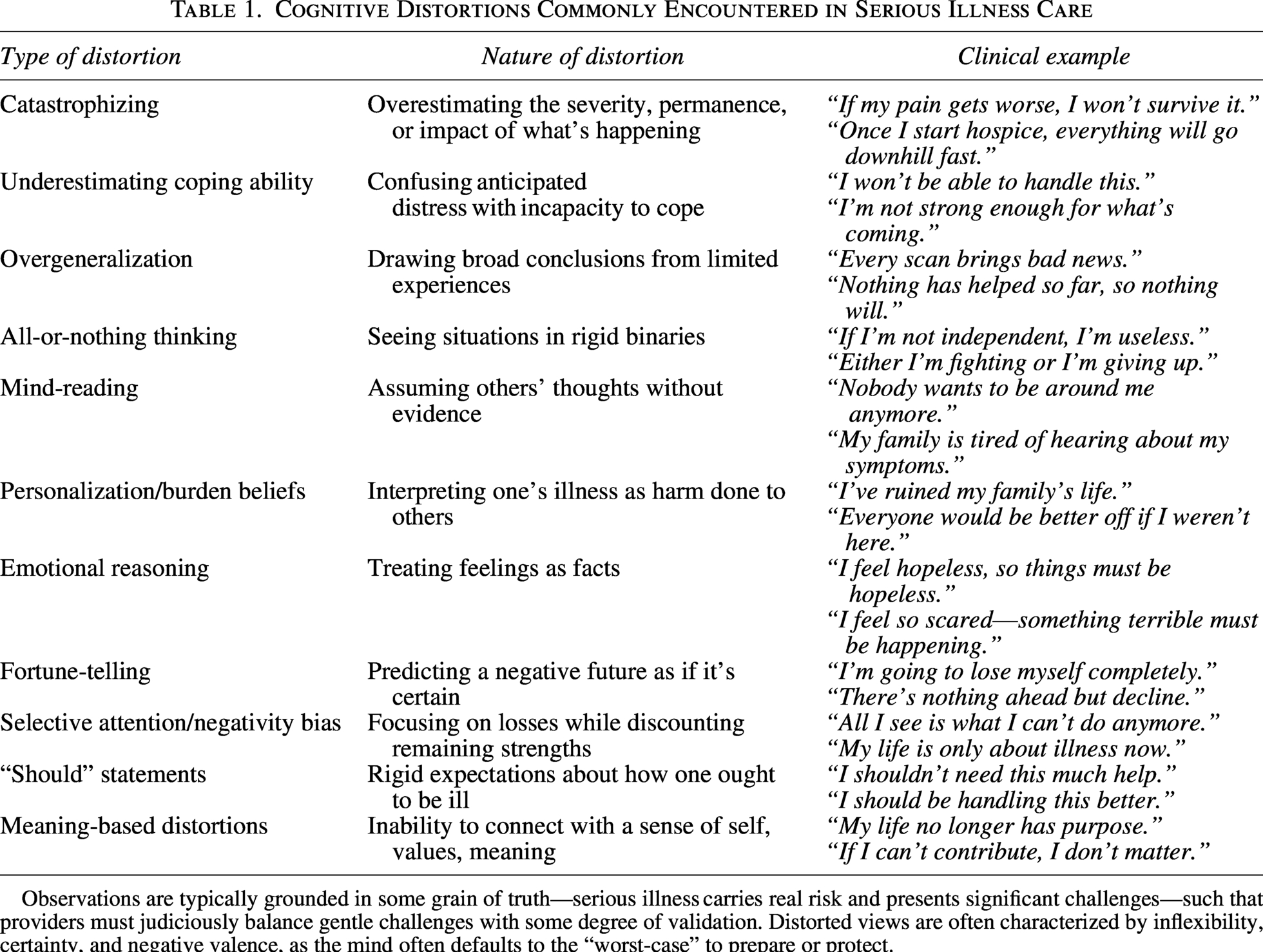
Observations are typically grounded in some grain of truth—serious illness carries real risk and presents significant challenges—such that providers must judiciously balance gentle challenges with some degree of validation. Distorted views are often characterized by inflexibility, certainty, and negative valence, as the mind often defaults to the “worst-case” to prepare or protect.
Clinician: I wonder how we might learn more about the sadness you notice in your friends and where the silence seems to come from. As we are talking about this, do any ideas come to mind for you? Norah: I mean, yes. I guess I could just ask them. Right? Clinician: Does that feel like a conversation you could have with one of your friends? Is there someone you would feel especially safe talking with about this? Norah: I could talk to Amanda. Before I got sick, we could talk about anything. But now, it feels like she doesn’t have anything to say to me. Clinician: It sounds like having that kind of space back would matter to you, where you could talk about anything. How do you imagine you might start that conversation? Just as clinicians routinely inquire about medication trials at follow-up appointments, behavioral experiments can be revisited in subsequent visits. Behavioral experiments are intentionally designed as “no-lose” opportunities for learning. Regardless of the outcome, useful information is gained. If Norah’s friend engages openly and communicates her feelings, Norah may develop a clearer understanding of their dynamic and recognize ways in which her prior beliefs were distorted. If her friend responds with avoidance and withdraws, the experience may be painful, but it yields valuable information about the nature of that relationship and provides material for further discussion in future visits. The possibility that behavioral experiments may evoke distress underscores the importance of a strong therapeutic alliance and a commitment to nonabandonment. As in all aspects of palliative care, meeting patients where they are and accompanying them through difficult emotional terrain is essential. This stance of presence and support helps establish the psychological safety needed for patients who feel “stuck” to take risks, test new behaviors, and re-engage with life in meaningful ways.
Conclusion
Maintaining a holistic, whole-person approach to palliative care requires clinicians to recognize and respond to the full range of suffering patients may experience, including patients who feel “stuck” in despair. In this context, feeling stuck can reflect distorted or unhelpful beliefs and behavioral patterns that limit agency, narrow perceived options, and perpetuate emotional distress, withdrawal, or interpersonal conflict. Familiarity with CBT principles, such as the cognitive triangle, and integration of CBT-informed communication tools, including guided discovery using Socratic questioning, cognitive restructuring, and behavioral experiments, can support palliative care clinicians in addressing this form of suffering. 1 These approaches deepen therapeutic alliances, enhance patient coping and self-efficacy, and reduce distress by developing greater flexibility and capacity to navigate the challenges of living with serious illness.3–5
Footnotes
Consent to Publish
Al cases presented in this series are hypothetical composites developed for ilustrative and educational purposes. They do not represent real patients, and therefore, consent to publish was not required.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.