
Abstract
Background:
Residents lack confidence caring for children with severe neurological impairment (SNI). The novel personal history tool, SHINE (Self, Happy, Ill, Names, and Extra), was codeveloped by families and residents to strengthen residents’ confidence in connecting with children with SNI and their families.
Objectives:
To describe SHINE’s use among residents and its impact on residents’ burnout, meaningful work, and confidence in caring for children with SNI.
Methods:
Residents at an academic children’s hospital in the United States received small-group teaching on the use of SHINE. Participants completed baseline, one-, and three-month post-intervention surveys, which included resident demographics; self-reported tool use; and resident burnout, meaningful work, and confidence in caring for children with SNI. Data were analyzed descriptively and using Pearson’s chi-square tests.
Results:
Briefly, 88% (n = 37/42) of eligible residents participated (25 interns [67%], 12 senior residents [32%]). After one month, respondents reported they found the tool helpful/very helpful (n = 11, 92%), were likely/very likely to continue using it (n = 11, 92%), and recommended it to future residents (n = 16, 100%). At baseline, residents reported low confidence caring for children with SNI (mean = 2.08, standard deviation (SD) : 0.84 on a 1 = low to 4 = high Likert scale). After one month, respondents reported improvements in (1) understanding the nonmedical needs of patients (mean increase: 0.71, SD: 0.85, p value = 0.006) and (2) understanding life outside the hospital (mean increase: 0.94, SD: 0.87, p value = 0.003). Respondents reporting higher use of the tool experienced larger gains. No significant differences were seen in burnout or meaningful work.
Conclusion:
SHINE may improve resident self-reported confidence in caring for children with SNI.
Key Message
Children with severe neurological impairment (SNI) often experience prolonged and frequent hospitalizations, and residents report a lack of connection and low confidence related to their care. This study describes the implementation of a family-resident codeveloped personal history tool, Self, Happy, Ill, Names, and Extra, named SHINE, that improved residents’ confidence in caring for children with SNI.
Introduction
Lack of understanding between parents of children with complex medical conditions and clinicians negatively impacts patients, families, and care team members.1–3 Many of these children have severe neurological impairment (SNI), a term that describes permanent central nervous system disorders such as mitochondrial disease or severe epilepsy that result in complex motor and cognitive symptoms.4,5 Families know that clinicians’ holistic understanding of their children with SNI is critical for recognizing patients’ unique pain behaviors, communication abilities, and factors that help them recover during acute illness.6–8 Moreover, in the hospital setting, children with SNI are not at their baseline health or behavior, and families report challenges feeling heard about their child’s health beyond their medical needs.9–12
Residents have a critical role in understanding these patients’ unique needs, yet often lack the training and confidence to elicit this information from children with SNI and their families.13,14 Residents gain these skills not through isolated medical management, but through improved connection with patients.15,16 Contextualizing medical care through the lens of personhood not only drives medical decision-making but also has the potential to improve rates of moral distress and burnout among clinicians caring for children with SNI.10,17
Ultimately, children with SNI, their families, and residents need effective tools to help bridge this communication gap between families and clinicians.18,19 This study introduces a novel tool, Self, Happy, Ill, Names, and Extra (SHINE), which incorporates personal histories from children with SNI into structured history-taking. This study describes the implementation of the SHINE tool with a pilot group of residents on the inpatient pediatrics service and examines the impact of SHINE on residents’ burnout, meaningful work, and confidence in caring for children with SNI.
Methods
This prospective study was conducted between 2022 and 2024 at a single academic children’s hospital in the northwestern United States. The study team included pediatric neurologists and residents as well as researchers with expertise in educational interventions and quality improvement. The study was Institutional Research Board (IRB) approved and received a small grant from the university’s Graduate Medical School Housestaff Quality and Safety Committee to support fees for survey tools as part of the intervention’s assessment.
SHINE tool development
The novel personal history tool, SHINE, was iteratively codeveloped by residents and nine families of children with SNI based on existing literature and best practices in person- and family-centered care.20,21 The final tool incorporated questions designed to enhance relational care for a child with SNI through personal history taking (Fig. 1). It was named SHINE to represent the six questions in the tool and emphasize its role in illuminating the personhood of patients.
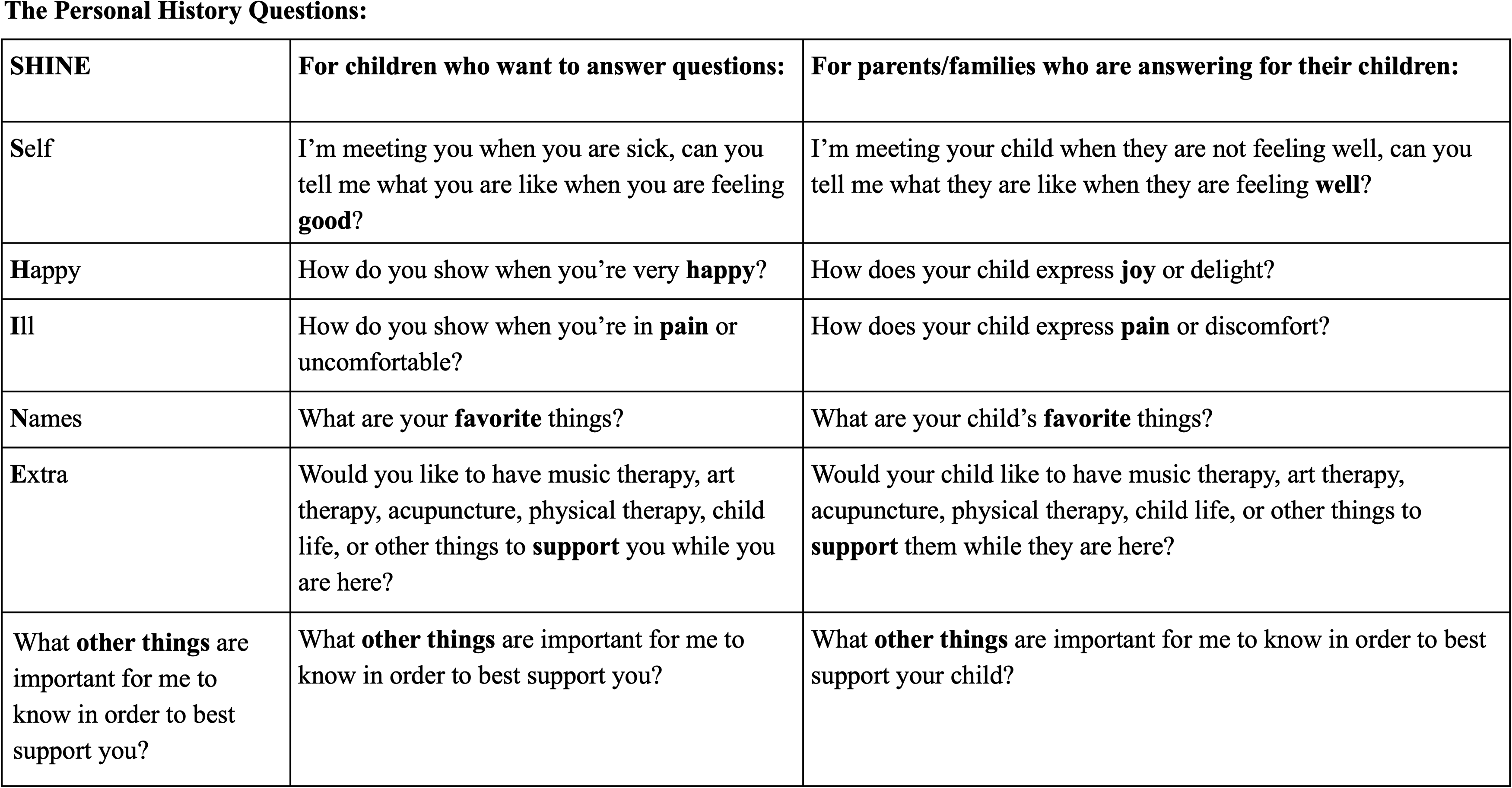
SHINE: The Personal History Tool. SHINE, Self, Happy, Ill, Names, and Extra.
SHINE implementation
Initially, the study team met with divisional leaders in hospital medicine and relevant subspecialties to get their approval to implement the tool with residents during their four-week inpatient clinical service rotations. After approval, the study team, together with a parent involved in the development of the SHINE tool, presented during the resident noon conference to provide information about the tool, its rationale, and the purpose of the study. Subsequently, every month for three consecutive months, across two cycles separated by six months (for six total months of recruitment), one to two members of the study team (P.A.W., A.X., D.O., I.D., and K.W.) met with residents from the inpatient services for 30 minutes for small-group sessions to introduce the study, obtain verbal consent, and teach about use of the SHINE tool. After consent, participants were given a clinician summary sheet (Supplementary Data S1) and instructed to use the SHINE tool anytime they were admitting a child with SNI or joining the child’s medical team. Residents were also asked to (1) document responses in the electronic health record (EHR) using an Epic dot phrase provided by the study team and (2) to include elements of the SHINE tool in their handoffs. Participants also received printed copies of the tool to optionally use with families who preferred to answer the questions in writing (Supplementary Data S2).
SHINE evaluation
Participants completed baseline, one-, and three-month post-intervention surveys on Research Electronic Data Capture (REDCap), 22 including demographic information, tool use, burnout, meaningful work, and confidence in caring for children with SNI. Demographic information included residency specialty, and post-graduate year (PGY), which was separated into interns and seniors. Tool use was self-reported as the number of times the tool was used in the last month prior to survey completion. On one- and three-month follow-up surveys, residents were asked on 5-point Likert scales how helpful they found the tool when caring for children with SNI (1 = very unhelpful to 5 = very helpful), how likely they were to continue using the tool (1 = very unlikely to 5 = very likely), and whether they would recommend teaching future residents about the tool (yes and no) with a free text response area to explain their answer.
Assessment of self-reported confidence was based on similar educational intervention studies measuring confidence in relational aspects of care.16,23,24 Residents were asked to indicate their degree of confidence on a 4-point Likert scale (1 = need further basic instruction, 2 = confident to perform with supervision/coaching, 3 = confident to perform with minimal consultation, 4 = confident to perform independently) across five areas focused on connection with patients and relational aspects of care. These included (1) assessing and understanding nonverbal cues in patients with SNI, (2) developing a personalized care plan for patients with SNI, (3) understanding the nonmedical needs of patients with SNI, (4) partnering with families of children with SNI, and (5) understanding what life is like outside the hospital for patients with SNI. Burnout was assessed using the validated Maslach Burnout Inventory, which includes subscales of emotional exhaustion, depersonalization, and personal accomplishment measured through 23 items on a 7-point Likert scale from “a few times a year” to “every day.” 25 Finally, meaningful work was assessed through the validated Work and Meaning Inventory, which includes positive meaning, meaning-making through work, and greater good motivations subscales, assessed using 12 items on a 5-point Likert scale from “absolutely untrue” to “absolutely true.” 26
Survey data were analyzed descriptively with means and standard deviations. The Pearson’s chi-square test was used to evaluate differences in baseline and follow up assessments. Significance was set to <0.05. No adjustments were made for multiple testing, as this was an exploratory study and was intended to be hypothesis-generating in terms of the tool’s impact on outcomes.
Results
Thirty-seven out of 42 eligible residents participated [25 interns (67%), 12 senior residents (33%)]. There were a total of 28 (76%) pediatric, 6 (16%) family medicine, 2 (5%) anesthesia, and 1 (3%) psychiatry residents. There was attrition over the course of the study, with 17 participants (53%) responding to one-month survey and 10 participants (27%) responding to three-month surveys.
Use of the SHINE tool
At one month, the majority of respondents reported that they felt that the tool was helpful (n = 5, 42%) or very helpful (n = 6, 50%) and were likely (n = 8, 67%) or very likely (n = 3, 25%) to continue using the tool. These numbers were similar at three months, with respondents reporting that the tool was helpful (n = 5, 63%) or very helpful (n = 3, 37%), and most reporting that they were likely (n = 3, 38%) or very likely (n = 2, 25%) to continue using the tool. All recommended teaching future residents about the tool at both the one-month (n = 16, 100%) and three-month (n = 8, 100%) timepoints. When taking into account overall response rates, at one month 30% (n = 11/37) of all enrolled residents found the tool helpful or very helpful and were likely or very likely to continue using the tool, and at three months, 22% (n = 8/37) of all enrolled residents found the tool helpful or very helpful and 14% (n = 5/37) were likely or very likely to continue using the tool.
About half of respondents (one-month: n = 8, 50%; three-months: n = 6, 60%) reported being high users of the tool, reporting having used it once to twice a week within the preceding month. Similarly, about 40% percent of respondents (one-month: n = 7, 43%; three-months: n = 4, 40%) reported being low users of the tool, using the tool two times or less each month (residents who did not indicate usage frequency were excluded from this portion of the analysis).
Self-reported confidence
In evaluating self-reported confidence in caring for children with SNI, at baseline residents reported low confidence (mean: 2.08, standard deviation (SD) 0.84) (Table 1 and Fig. 2). Lowest ratings were for the areas of (1) developing a personalized care plan (mean: 1.81, SD: 0.81), (2) understanding the nonmedical needs of patients (mean: 1.92, SD: 0.69), and (3) understanding life outside the hospital (mean: 1.81, SD: 0.84). After one month, respondents reported significant improvements across all areas (mean increase: 0.55, SD: 0.15, p value <0.001). One resident shared, “Twice… families have said that they appreciated me listening and being present. It felt like parents appreciated me asking about who their child is.”
Confidence Caring for Children with Severe Neurological Impairment at Baseline, One Month, and Three Months
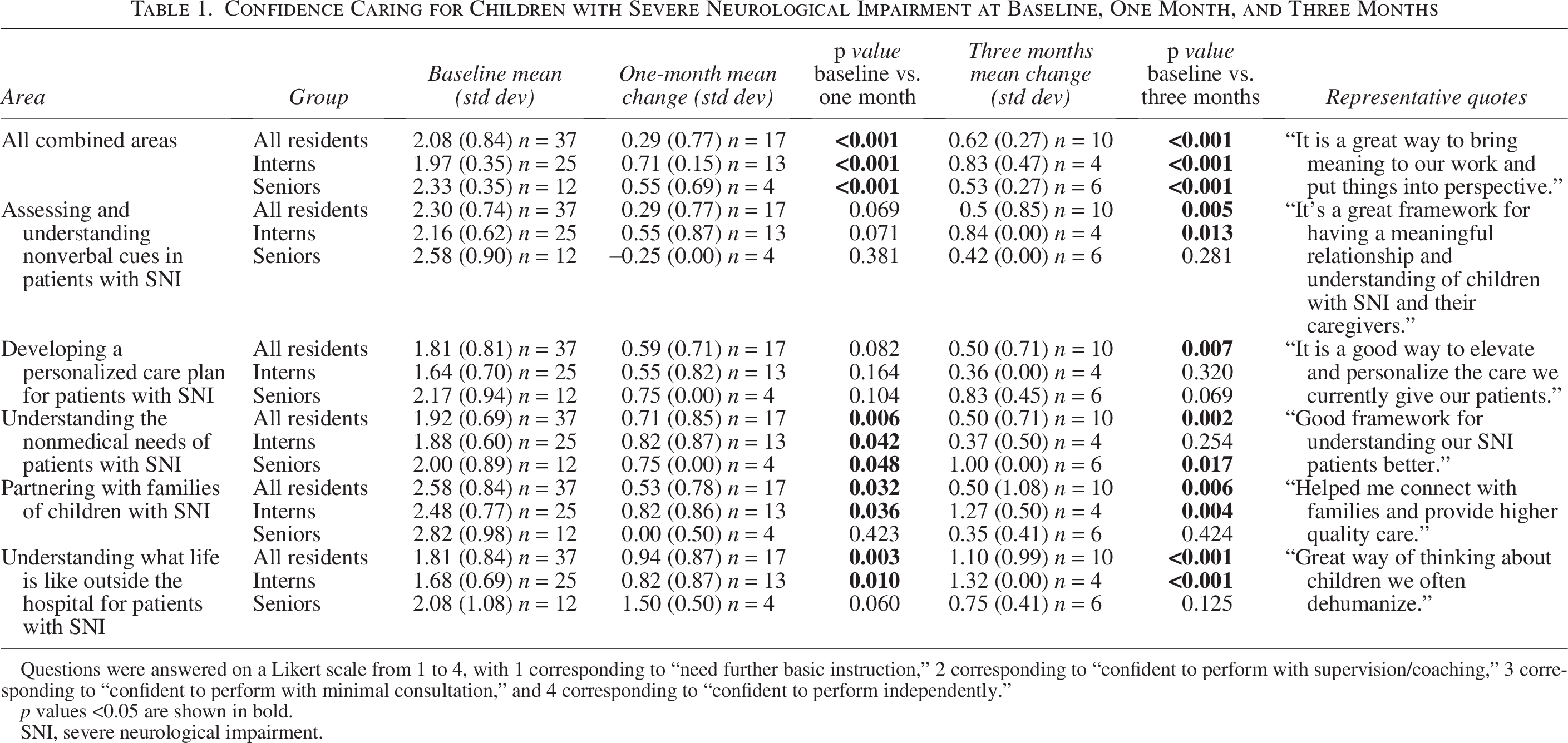
Questions were answered on a Likert scale from 1 to 4, with 1 corresponding to “need further basic instruction,” 2 corresponding to “confident to perform with supervision/coaching,” 3 corresponding to “confident to perform with minimal consultation,” and 4 corresponding to “confident to perform independently.”
p values <0.05 are shown in bold.
SNI, severe neurological impairment.
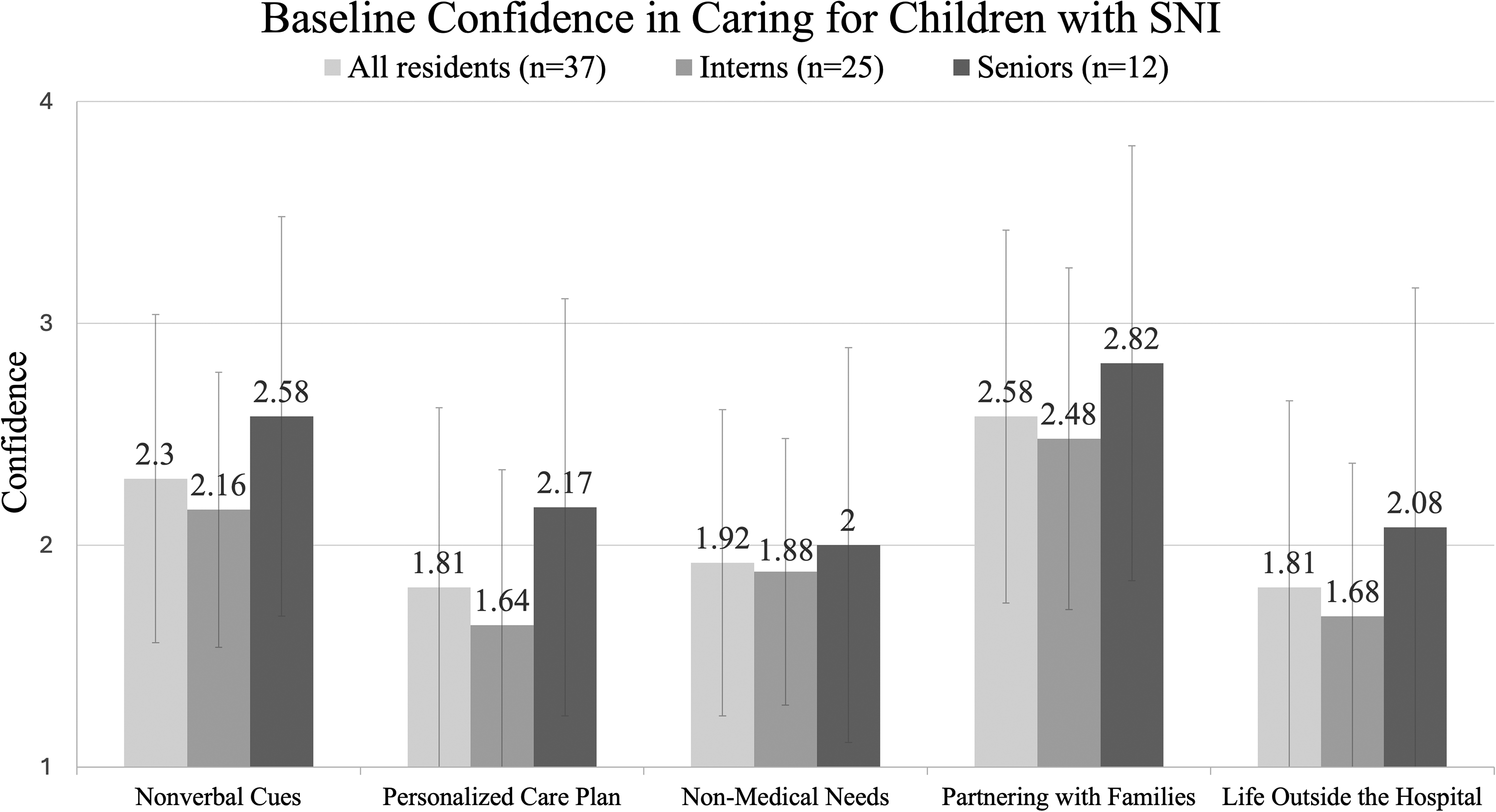
Baseline confidence in caring for children with SNI. Mean baseline values are depicted for intern and senior residents across five measured areas. Questions were answered on a Likert scale from 1 to 4, with 1 corresponding to “need further basic instruction,” 2 corresponding to “confident to perform with supervision/coaching,” 3 corresponding to “confident to perform with minimal consultation,” and 4 corresponding to “confident to perform independently.” SNI, severe neurological impairment.
At three months, residents retained the gains from one-month timepoint, with respondents reporting increases across all areas (mean increase of 0.83, SD: 0.15, p value <0.001) (Table 1, Fig. 3). Interns showed ongoing gains as compared to the one-month timepoint, with the largest increases in the areas of (1) assessing and understanding nonverbal cues (mean increase of 0.84, SD: 0.82, p value = 0.013), (2) partnering with families (mean increase of 1.27, SD: 0.50, p value = 0.004), and (3) understanding life outside the hospital (mean increase of 1.32, SD: 0.00, p value <0.001). Senior residents showed the biggest gain in the area of understanding the nonmedical needs of patients with SNI (mean increase: 1.00, SD: 0.82, p value = 0.017).
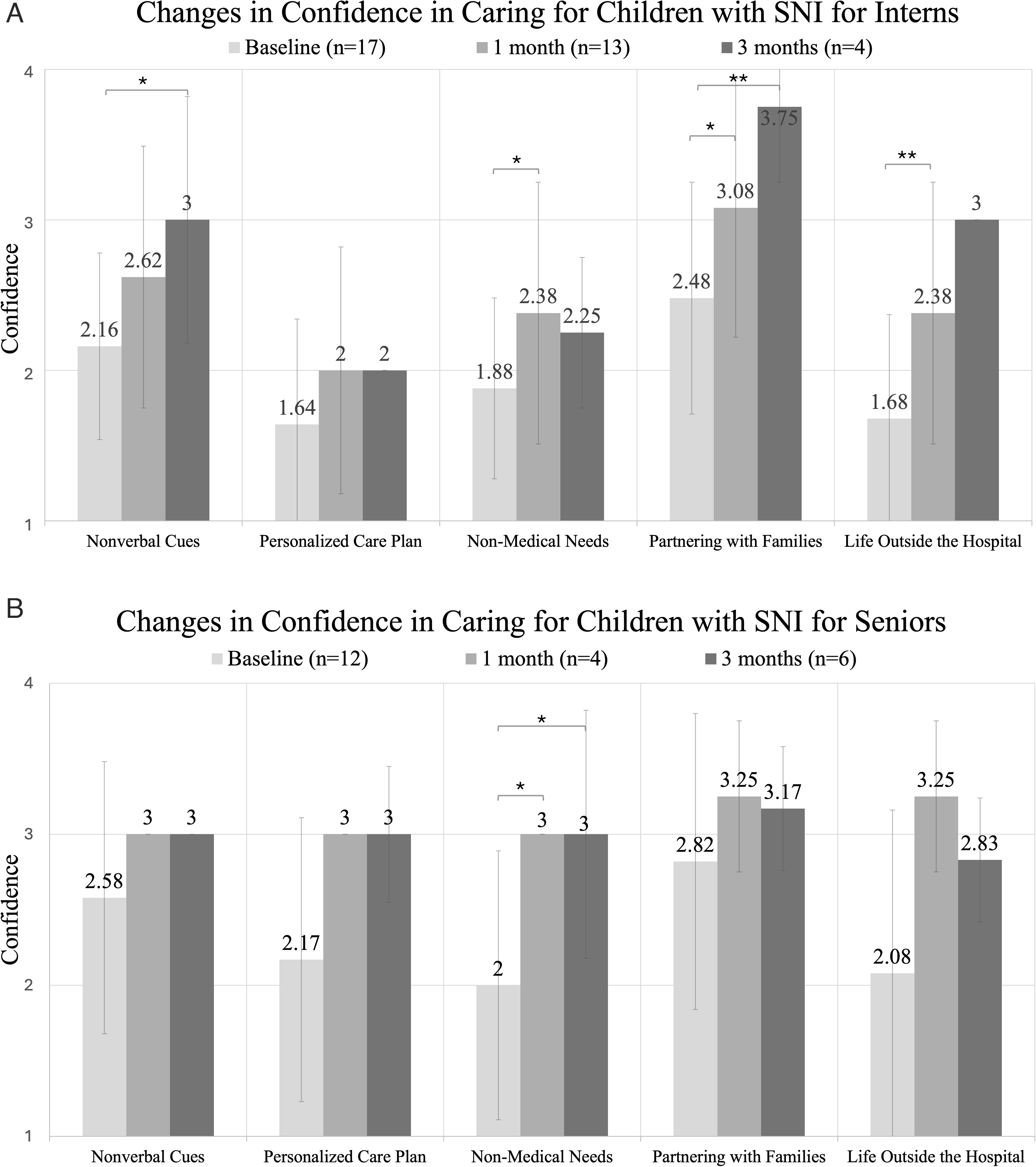
Changes in confidence in caring for children with SNI for interns
Senior residents also reported higher baseline confidence compared to interns (mean: 2.33, SD: 0.35 for seniors; mean: 1.97, SD: 0.35 for interns, p value = 0.007; Table 2 and Fig. 3). At the one-month timepoint, both senior residents and interns showed significant gains in confidence, with seniors showing a trend toward greater gains (mean increase: 0.77, SD: 0.34 for seniors; mean increase: 0.52, SD: 0.13 for interns, p value = 0.004). At three months, senior residents showed more significant gains than interns in the areas of (1) developing a personalized care plan for patients (mean increase: 0.83, SD: 0.45 for seniors; mean increase: 0.36, SD: 0.00 for interns, p value = 0.012) and (2) understanding the nonmedical needs of patients (mean increase: 1.00, SD: 0.82 for seniors; mean increase: 0.37, SD: 0.50 for interns; p value = 0.005).
Differences in Confidence Caring for Children with Severe Neurological Impairment Between Senior and Intern Residents
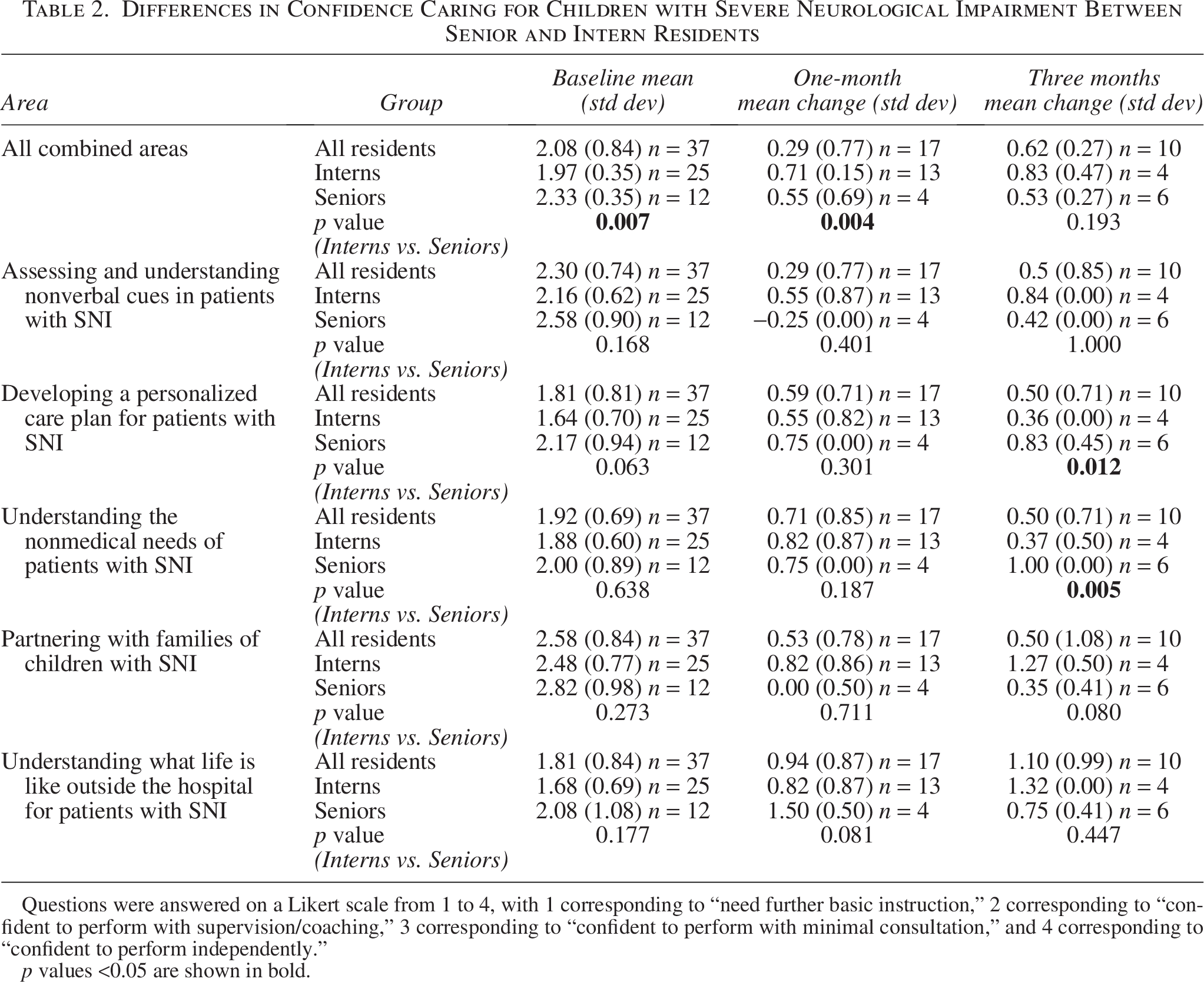
Questions were answered on a Likert scale from 1 to 4, with 1 corresponding to “need further basic instruction,” 2 corresponding to “confident to perform with supervision/coaching,” 3 corresponding to “confident to perform with minimal consultation,” and 4 corresponding to “confident to perform independently.”
p values <0.05 are shown in bold.
Residents who reported higher use of the tool experienced the largest gains across all groups at the one-month timepoint (mean increase: 0.65, SD: 0.25 for high users; mean increase: 0.39, SD: 0.33 for low users, p value = 0.002) (Table 3 and Fig. 4). No difference was seen at the three-month timepoint. While residents who reported high usage of the tool at one month did have higher baseline confidence as compared to residents reporting low usage of the tool (mean: 2.30, SD: 0.38 for high users; mean: 1.96, SD: 0.50 for low users), this difference was not significant (p value = 0.850).
Differences in Confidence Caring for Children with Severe Neurological Impairment Between High and Low Users
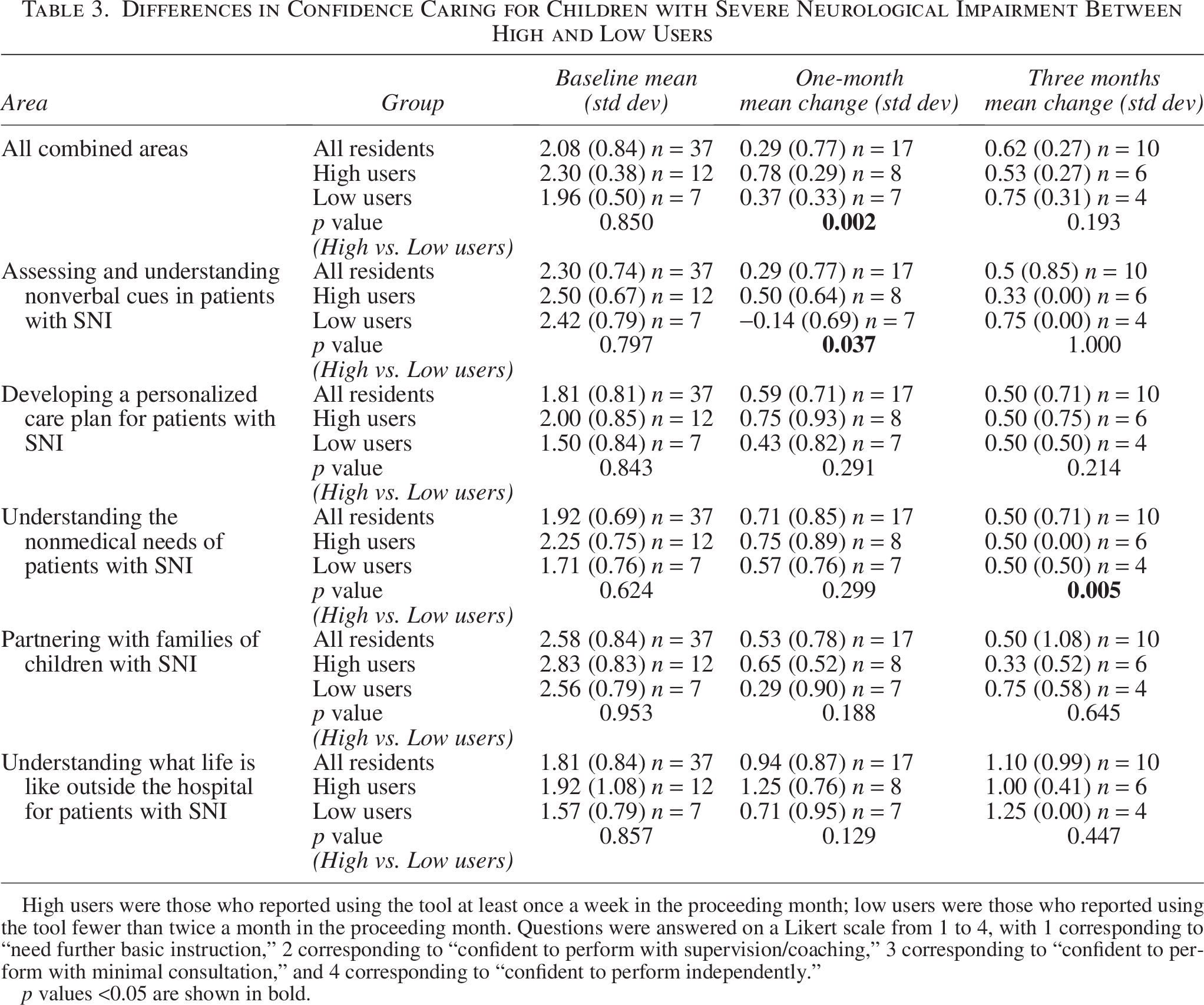
High users were those who reported using the tool at least once a week in the proceeding month; low users were those who reported using the tool fewer than twice a month in the proceeding month. Questions were answered on a Likert scale from 1 to 4, with 1 corresponding to “need further basic instruction,” 2 corresponding to “confident to perform with supervision/coaching,” 3 corresponding to “confident to perform with minimal consultation,” and 4 corresponding to “confident to perform independently.”
p values <0.05 are shown in bold.
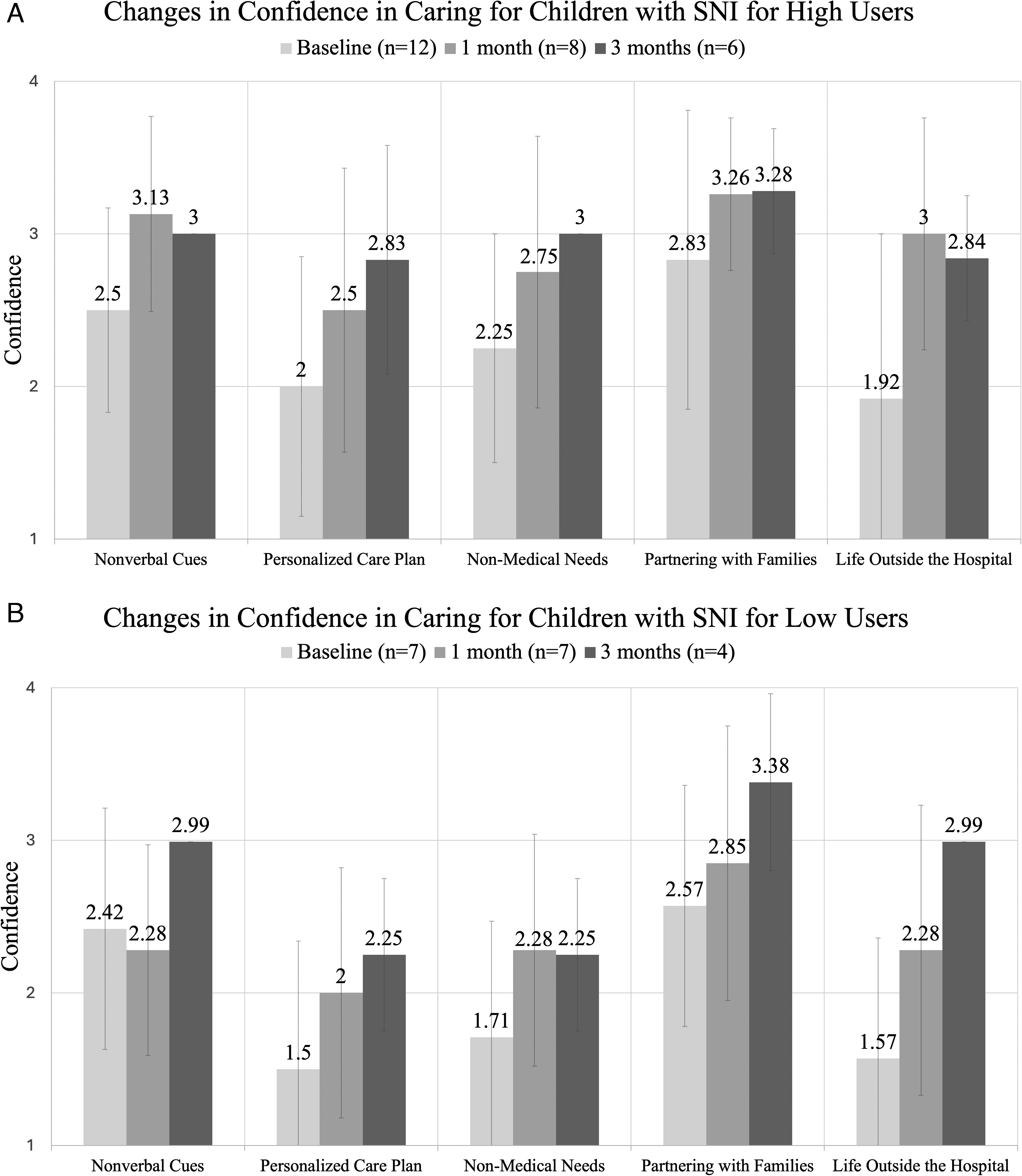
Changes in confidence in caring for children with SNI for high users
Burnout
For burnout, residents in the study reported high levels of burnout, especially on the emotional exhaustion (EE) subscale (Table 4). Burnout was similar for interns (mean: 37.68, SD: 10.86 for EE, mean: 16.64, SD: 5.51 for depersonalization [DP], and mean: 36.08, SD: 6.16 for personal accountability [PA]) and senior residents (mean: 41.25, SD: 8.61 for EE, mean: 16.50, SD: 6.36 for DP, mean: 36.67, SD: 3.85 for PA). Although burnout scores were slightly lower on follow-up surveys at one month (mean decrease: 1.88, SD: 5.18 for EE, mean decrease: 1.13, SD: 3.52 for DP, mean decrease: 0.06, SD: 3.87 for PA) and three months (mean decrease: 2.00, SD: 7.20 for EE, mean decrease: 2.70, SD: 4.30 for DP, mean increase: 0.60, SD: 4.55 for PA), no significant differences were found from baseline scores.
Change in Measures of Burnout and Meaning in Work One Month and Three Months
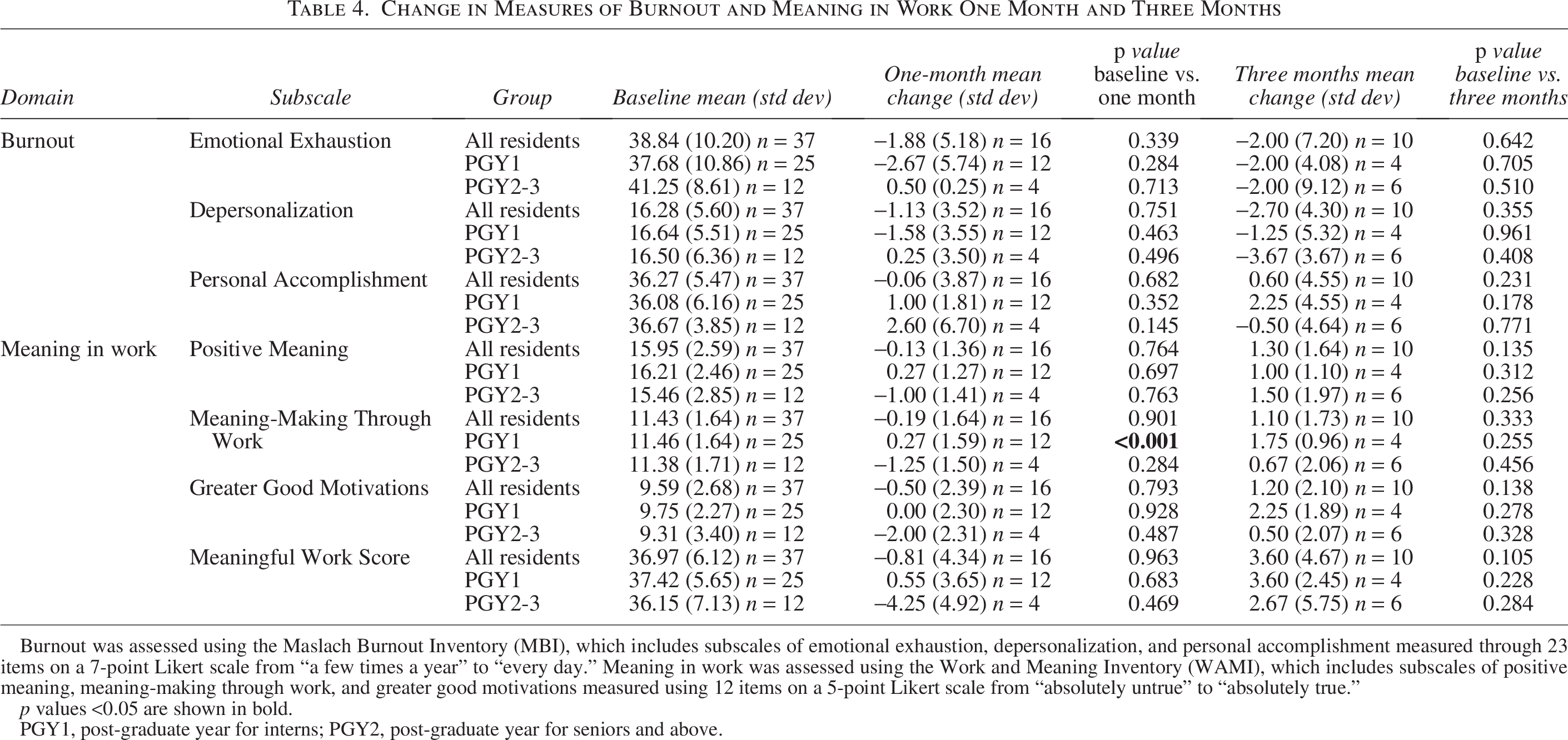
Burnout was assessed using the Maslach Burnout Inventory (MBI), which includes subscales of emotional exhaustion, depersonalization, and personal accomplishment measured through 23 items on a 7-point Likert scale from “a few times a year” to “every day.” Meaning in work was assessed using the Work and Meaning Inventory (WAMI), which includes subscales of positive meaning, meaning-making through work, and greater good motivations measured using 12 items on a 5-point Likert scale from “absolutely untrue” to “absolutely true.”
p values <0.05 are shown in bold.
PGY1, post-graduate year for interns; PGY2, post-graduate year for seniors and above.
Meaningful work
For meaningful work, residents reported moderate scores (mean: 36.97, SD: 6.12), which were similar for interns (mean: 37.42, SD: 5.65) and senior residents (mean: 36.15, SD: 7.13) (Table 4). No significant difference was seen in meaningful work from baseline to follow-up surveys at one month (mean difference: −0.81, SD: 4.34) and three months (mean increase: 3.60, SD: 4.67). Despite this, residents did report subjective impacts on meaningful work, with one participant sharing, “I used the tool at the beginning of a patient’s stay in the hospital and it made a huge difference building excellent rapport and a foundational relationship with the family. It also helped me understand the patient so much more… I found this really fulfilling for myself.”
Discussion
In this study, the personal history tool SHINE was a way for residents to elicit information from children with SNI and their families about their communication style, personhood, and individualized care needs. Although SHINE did not improve resident reports of burnout or meaningful work, those who self-reported higher use of the tool also reported more gains in confidence in their care for children with SNI. Residents reported that using the tool was beneficial for improving the quality of care they provide for patients, improving connection, and building rapport with families.
While families provide the backbone of care for children with SNI throughout their lifetime, barriers exist to incorporating their perspectives into hospital care.27,28 The existing literature substantiates these challenges as families report feeling that their expertise is not valued by clinicians, that they have to “fight” in order for their child to receive the care they need, and that clinicians underestimate the quality of life of their child.12,29–31 Families report that clinicians have been indifferent to their child’s recovery, made them feel unwelcome in the hospital, or lacked a positive impression of their child’s full life. 10 In a recent national study involving >100 participants, families and clinicians noted the need for more humanistic and connected care for children with medical complexity, including those with SNI. 32
Similarly, clinicians report feeling overwhelmed and unprepared to care for children with SNI.13,18 In studies among pediatric residents and their training programs, many lack opportunities for residents to see children with complex medical needs outside of the hospital setting.3,13,33 Studies also suggest that misjudgments regarding quality of life are common, with residents and clinicians underrating quality of life compared to families and children themselves.9,17,34 These barriers not only negatively impact care for children with SNI but also contribute to burnout and distress among clinicians.18,35 Specifically, clinicians report struggling to care for children when cure is not possible, when there is considerable uncertainty regarding the child’s health trajectory, and when they do not know how to communicate directly with the child to understand their experiences. 13 These are critically important barriers to address not only to appropriately and effectively care for children with SNI but also to improve clinicians’ experience and meaning in their work.
The personal history tool, SHINE, was codeveloped to start to address this need through easy-to-implement training and EHR techniques. Participants from this study indicated that use of the SHINE tool improved their confidence in connecting with families and their understanding of their patients’ nonmedical needs and lives outside the hospital. A subset of participants also reported durable improvements, which persisted three months after learning about the tool, as well as ongoing high usage overall.
In this study, interns reported lower baseline levels of confidence compared to senior residents in caring for children with SNI, and overall senior residents showed greater improvements over time. Additionally, those who reported higher use of the tool reported larger gains in confidence over time as compared to those who reported low use of the tool. While residents shared in open-ended feedback that they felt positive impacts on their engagement with their work, no measurable impact on burnout or meaningful work was seen in this study. Given the inclusion of residents from several training programs, the low response rates, and diverse work environments residents were in at the time of the one- and three-month follow-up surveys, any measurable impact on burnout and meaningful work may have been difficult to assess and perhaps obscured.
There are a number of limitations to this study. This was a small, single-site study limiting generalizability. Enrollment was limited to residents on the inpatient service, with plans to enroll more of the residency program in the future. This study did not have a control group and relied on measures of self-report rather than objective measures of experience. Given the limitations of retrospective self-reporting, no causative conclusions can be drawn about the direct impact of tool use on confidence. Additionally, SHINE required teaching time with residents, and we experienced challenges in recruitment related to on-service residents being unavailable due to patient care needs. There were low rates of return on follow-up surveys. This may be because residents are frequently asked to participate in surveys without protected time for completion, and available funding did not allow for participant incentives. While responding residents reported an overall high likelihood of continuing to use the tool and the helpfulness of the tool, it is possible residents who did not return follow-up surveys were less likely to find the tool helpful overall, and thus positive responses may have been overrepresented.
Since the conclusion of the study, work has begun to integrate the SHINE tool into daily inpatient care, including teaching SHINE during inpatient orientation, incorporating it into standard inpatient templates, and continuing education around SHINE through Grand Rounds and Healthcare Equity Rounds at the children’s hospital. Next steps will include incorporating SHINE into care plans for children with SNI and other forms of medical complexity. We also plan to elicit families’ and caregivers’ perspectives on incorporation of SHINE into their child’s care. As we move toward hospital-wide use of the tool, we also plan to track SHINE usage via data collection from the EHR as an objective measure of use and documentation. Finally, we will be working with other children’s hospitals to incorporate SHINE at other sites nationally, including adaptation for home-based palliative teams and home hospice teams.
Conclusion
The personal history tool, SHINE, may be a promising way to improve residents’ self-reported confidence in relational aspects of care for children with SNI.
Authors’ Contributions
Conceptualization: P.A.W. (lead), A.X. (supporting), D.O. (supporting), I.D. (supporting), K.W. (supporting). Formal analysis, funding acquisition, and project administration: P.A.W. Investigation: P.A.W. (lead), A.X. (equal), D.O. (supporting), I.D. (supporting), K.W. (supporting). Supervision: P.A.W. (lead) and J.F.B. (supporting). Writing—original draft: P.A.W. (lead) and J.F.B. (equal). Writing—review and editing: P.A.W. (lead), J.F.B. (equal), A.X. (supporting), D.O. (supporting), I.D. (supporting), and K.W. (supporting).
Ethical Considerations
This study received IRB approval from the Seattle Children’s IRB (STUDY00004055) on January 19, 2023, and the University of Washington IRB (STUDY00016920) on December 15, 2022.
Consent to Participate
Participants provided written informed consent to participate at the time of enrollment via REDCap.
Consent for Publication
This publication does not include data from any individual participants.
Footnotes
Acknowledgments
The authors thank the many families, residents, and other trainees who participated in this project. They also thank members of the Seattle Children’s complex care, palliative care, hospital medicine, neurology, and general medicine teams for providing feedback and allowing them to incorporate this study into clinical care. Finally, they would like to thank Lucy Colville, MD, Rachel Caron, MD, and Anna Janecek, MD, for their work in recruitment as well as resident education around the SHINE tool.
Disclosure Statement
J.F.B. has received grants for unrelated work from the National Institutes of Health Eunice Kennedy Shriver National Institute of Child Health and Human Development, the National Palliative Care Research Center’s Kornfeld Scholars Program, the Cambia Health Foundation, the Seattle Children’s Research Institute, and the Lucile Packard Foundation for Children’s Health. J.F.B. has a collaboration through Seattle Children’s Hospital with mejo (mymejo.com) and is on the medical advisory board for Hope for HIE (hopeforhie.org).
The remaining authors have declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
This work was supported by the University of Washington’s Housestaff Quality and Safety Committee grant.
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.