
Abstract
Background:
Serious illness conversation (SIC) is a structured conversation framework designed to improve shared decision making and promote goal-concordant care with patients anticipating end-of-life care decisions.
Objective:
Examine reach, timeliness, and quality of SIC implementation across a health system after implementation of a SIC Program (SICP). Examine factors associated with SIC completion for eligible patients.
Design:
Retrospective observational cohort study of decedents eligible for SIC from 2022 to 2024 in a large health system in the United States.
Measurements:
Proportion of eligible patients with a documented SIC, demographic and clinical characteristics, timing of SIC relative to eligibility and death, number, and quality of SIC sessions.
Results:
About 7424 patients met the inclusion criteria, and half (49.5%) of those had SIC documentation. Of those, mean number of SICs was 3.6 (SD 5.56). First documented SIC included defined quality components 31.1% of the time. Factors associated with SIC included palliative care visits (OR 2.26, 95% CI 1.84, 2.78), a primary care provider in the system (OR 1.77, 95% CI 1.59, 1.96), and an inpatient admission with discharge to home care (OR 2.36, 95% CI 2.07, 2.70). Patients with dementia (OR 0.58, 95% CI 0.51, 0.66) were less likely to have SIC.
Conclusion:
Systemwide implementation of an SICP engaged half of eligible patients; many of those had multiple documented conversations prior to death. More work is needed to engage eligible patients, especially those with dementia, and to improve conversation quality.
Key Message
Implementation of an SICP with an Electronic Health Record (EHR)-based SI score to identify patients in an integrated health system resulted in identification of a large population of seriously ill patients, with documentation of at least one conversation in nearly half of that group. Implementation occurred across the inpatient and outpatient settings.
Introduction
Serious illness (SI) is defined as a health condition that carries high-risk of mortality and negatively impacts a person’s daily functioning, quality of life or excessively strains caregivers. 1 Patients with SI often do not receive care near the end-of-life that is concordant with their goals and preferences for treatment.2–5 As a foundational element of goal-concordant care, communication to identify goals is often lacking, with fewer than one-third of seriously ill individuals reporting having had a conversation about their most important goals with their clinician. 6 When conversations do occur, they tend to occur late in the course of illness and focus more on technical aspects of treatment than on the goals that seriously ill individuals consider most meaningful. 7
Clinician barriers to implementing timely and effective communication about SI include a lack of skill and motivation to have potentially challenging conversations, inadequate education on prognostication, insufficient time, and misaligned incentives.8,9 Systemic barriers include goals-of-care conversations not being embedded in routine care, difficulty identifying patients at high risk of death, difficulty finding conversation documentation in the EHR, lack of role definition for clinicians during course of disease, and lack of institutional commitment.8–12 Serious illness conversation (SIC), a structured conversation framework, was created to guide conversations around goal-concordant care.8,13 SIC is a component within a program (SICP) aiming to address the above clinician barriers, as well as systemic barriers.8,13
Research on SICPs to date has focused on feasibility, acceptability, and quality of life measures14–16 with limited research on implementation experience17–21 or outcomes.14,22–25 Several studies and pilots have examined feasibility and uptake of a comprehensive SICP through randomized trials in varied settings including oncology,14,16 primary care, 17 and a hospital. 18 Implementation findings are generally positive, with increased SIC occurrence in the intervention group, provider and patient satisfaction with the process and tools, and improved content and quality of the conversations.14–18 Limited information has been shared about implementation of an SICP across an entire health system rather than in the context of randomized trials or pilots in limited settings.20,21 Among studies documenting SIC implementation at the health system level, both are exclusively inpatient. Gonzalez et al. reported conversation completion rates for patients with an ICU stay of 5 days or more, and nonobstetric adult hospitalized patients. 21 Oo et al. described implementation of a machine learning algorithm to identify hospitalized patients at high and intermediate risk for mortality with the aim of increasing goals of care conversations with these patients. 20
This study describes process outcomes of the implementation of an SICP at a large integrated health system, across both the inpatient and outpatient settings. Specific questions addressed include: (1) What proportion of eligible patients had a documented SIC? (2) Which patients were most and least likely to have a documented SIC? (3) For patients with a documented SIC, how timely was the SIC? What elements of the SIC were most frequently documented? How many conversations did each patient have? And which clinical roles conducted the SIC?
Methods
Setting
This study takes place in a large midwestern integrated health system. The system includes critical access, community, and quaternary care hospitals, urgent care centers, primary care clinics, and postacute care services including home health and hospice, as well as a large multispecialty medical group, which includes palliative care.
Program description
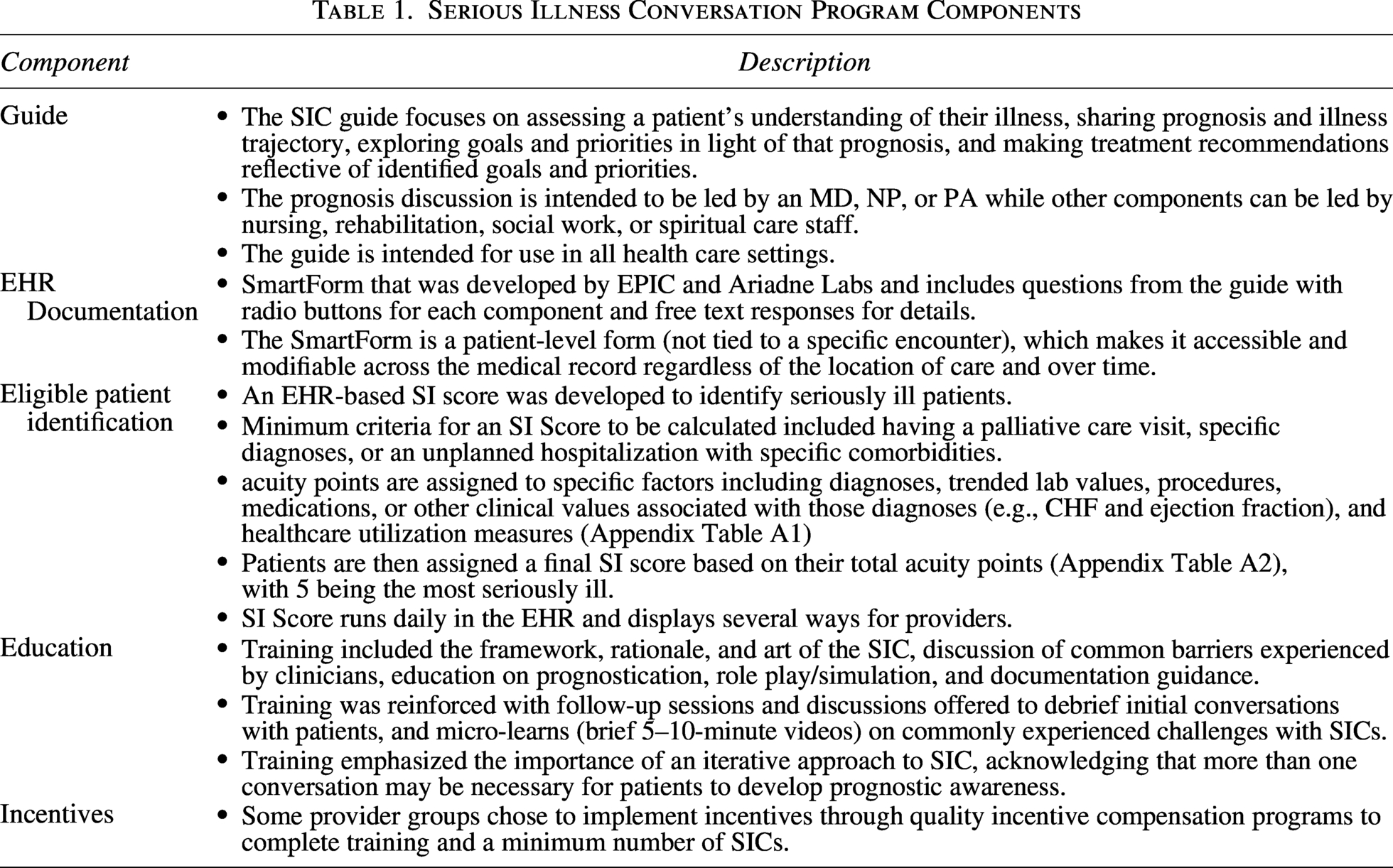
The program utilizes the standard components of the SICP developed by Ariadne Labs: the SIC Guide, EHR standard documentation tools, interdisciplinary team education and system engagement. In addition, our program includes clinician training on prognostication, use of an EHR-based SI score with clinician prompts, and aligned provider incentives.8,13 Components are defined in Table 1.
Serious Illness Conversation Program Components
Patients Eligible for SIC Who Died Prior to End of Study Period (2022–2024), Stratified by SIC Documentation Status (n = 7,424)
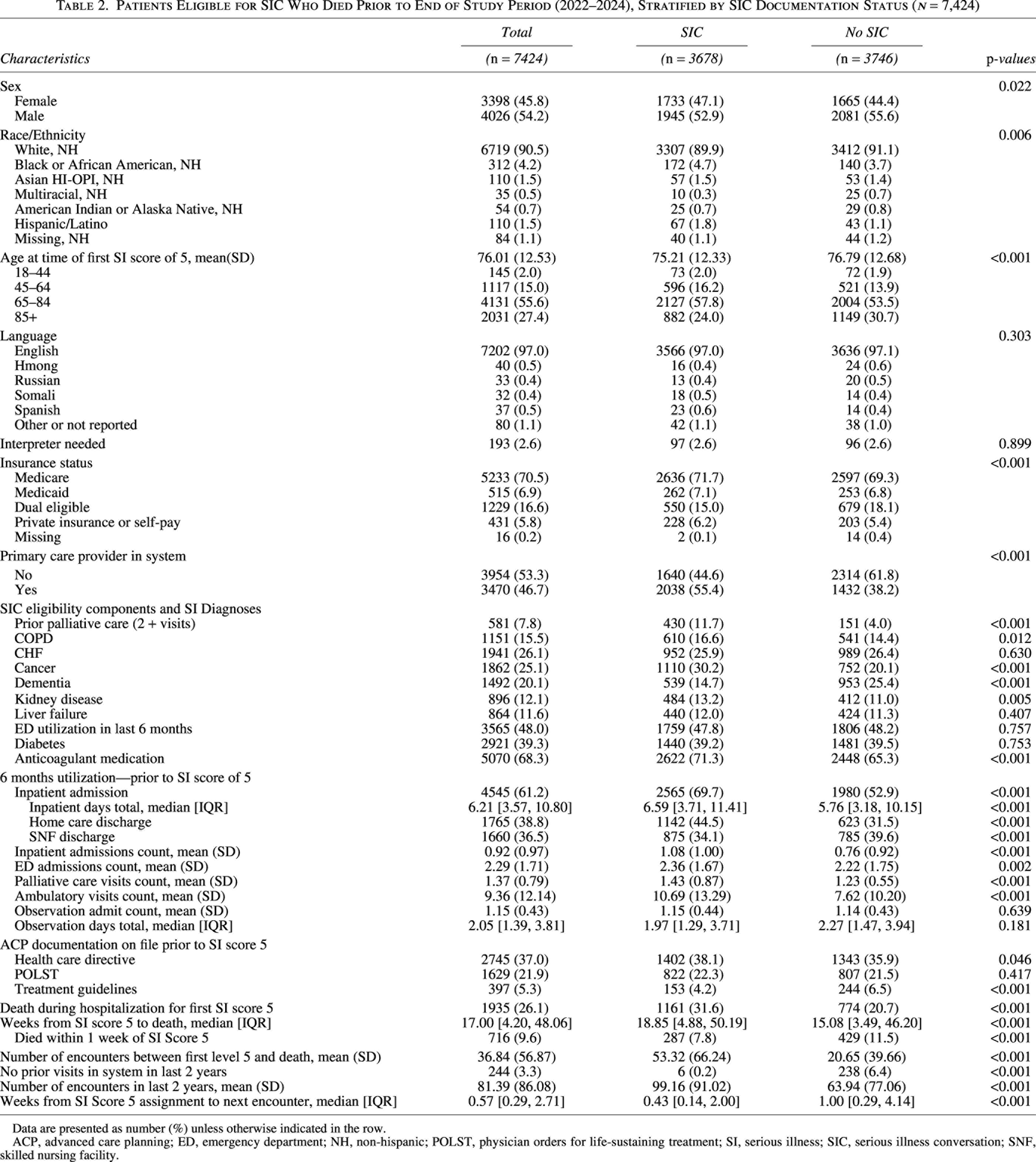
Data are presented as number (%) unless otherwise indicated in the row.
ACP, advanced care planning; ED, emergency department; NH, non-hispanic; POLST, physician orders for life-sustaining treatment; SI, serious illness; SIC, serious illness conversation; SNF, skilled nursing facility.
Oversight for implementation and training related to the SICP is run by the palliative care department. To develop our SI score, we referenced evidence-based studies to identify triggers for palliative care interventions. We used those triggers and clinical expertise to create score components (Appendix Table A1) to identify patients suitable for palliative care interventions, including hospice eligibility. We assigned values to each component and used an iterative chart review process to determine total point cut-offs (Appendix Table A2) corresponding to different levels of illness severity. While we were unable to do a validation study for these specific outcomes (palliative care appropriateness and hospice eligibility), we were able to identify that among patients hospitalized who received an SI score of 5 (highest), 35% died within 6 months, and 41% died within 12 months.
The score prompts providers and clinicians in several ways with variation by clinic or hospital setting. These include a best practice alert, a score column in the census report, discharge huddles, a banner, a specific EHR advance care planning navigator, patient lists, and population-based reports. Though patients with an SI score of 5 are the priority population for a SIC, care team members are encouraged to use their clinical judgment with patients at lower levels and consider if they are appropriate for a SIC.
We began SIC training in 2019, starting with hospitalists, followed by primary care and specialties (nephrology, palliative care, geriatrics, critical care, oncology, cardiology, cardiothoracic surgery). Initially, training was focused on physicians and advanced practice providers but was later expanded to other disciplines in home health, and care management. We also required training for new employees, although it was open to all care team members.
Study design and sample
A retrospective cohort study was used to report on process measures for the implementation of the SICP. Patients were included if they received a SI Score of 5 for the first time after January 1, 2022, and they died prior to December 31, 2024. This study period was chosen as it aligned with the completion of clinician training and implementation of tools across the system. Patients were excluded if they received an SI Score of 5 prior to 2022 or had a documented SIC prior to 2022. Patients without consent on file for the use of their EHR data for research were also excluded. The data used for this article were part of a larger research initiative that included the aim of examining end-of-life care utilization related to SIC. This influenced the decision to include only deceased patients. This also allowed us to examine the course of SIC implementation over the course of a patient’s end of life. This study was determined to be not human subjects research by the Allina Health IRB.
Measures
All study data were extracted from the EHR. Patient measures included demographics, whether their primary care provider was in our system, and disease categories from the SI Score (Appendix Table A1). Utilization measures were collected for 6 months prior to receiving a SI Score of 5: inpatient admissions, inpatient days (total), discharges to a skilled nursing facility (SNF) or Home Care, emergency department visits, palliative care visits, observation visits, hospice enrollment, and number of ambulatory visits. We also assessed if ACP documentation was on file prior to SI Score of 5 [health care directive, disease-specific treatment guidelines, Physician Orders for Life-Sustaining Treatment (POLST)]. We also measured time from assignment of an SI score of 5 to death, and from the next appointment to assess amount of time and opportunities for an SIC to occur.
An SIC was defined as occurring if any of the SIC components were documented. Measures relevant to timing of the SIC included if the SIC was completed prior to or after receiving the SI Score of 5, the time between SI Score identified as 5 and first SIC, and the time between first SIC and death. Characteristics measured for the first SIC included the documenting provider type, location, and inclusion of quality components: (1) sharing prognosis with the patient, (2) patient goals discussion, and (3) recommendations. If all three components were documented, the SIC was classified as meeting minimum quality standards.
Analysis
We characterized the sample using descriptive statistics such as frequencies, means with standard deviations, and medians with interquartile ranges for categorical, continuous, and time measures, respectively. Patients with a documented SIC were compared with patients without documented SIC using bivariate tests (chi-squared, t-test or Wilcoxon).
To assess factors associated with SIC engagement, we used logistic regression with Akaike Information Criterion (AIC) backward elimination. 26 This approach balances model fit and complexity by penalizing the inclusion of unnecessary variables, thus helping to determine the most relevant independent covariates.
Descriptive analysis assessed measures related to the quality of SIC documentation, namely the timing of the conversation in relation to the SI score, the number of conversations documented and which of 11 elements of the SIC were documented as having been discussed and the practitioner involved. Additionally, within this group we conducted a sub-analysis comparing patients who received their first SIC prior to a SI Score of 5 versus those who received their first SIC after a SI Score of 5.
All analyses were carried out in R 27 Version 4.1.2 and used the stepAIC function from the MASS package. 28
Results
During the study period, 7424 patients met SIC eligibility criteria (Table 2). The sample was 54.2% male, 90.5% white, non-Hispanic, 97.0% English speakers, average age of 76 (SD 12.53). Most (70.5%) were insured by Medicare. The most common SI diagnoses were CHF (26.1%), Cancer (25.1%), and Dementia (20.1%). Just over half of eligible patients (53.3%) did not have a primary care provider assigned in the study health system. In the 6 months prior to receiving a SI Score of 5, 61.2% had an inpatient admission, with 36.5% of those patients discharged to an SNF and 38.8% to a home care program.
Of eligible patients, 3678 (49.5%) had at least one SIC documented prior to death (Table 2). Compared with patients with no SIC, patients with SIC were more likely to have a primary care provider in the system (55.4% vs. 38.2%, p < 0.001); to have had 2 + palliative care visits (11.7% vs. 4.0%, p < 0.001); to have an SI diagnosis of cancer (30.2% vs. 20.1%, p < 0.001), COPD (16.6% vs. 14.4%, p = 0.012), or kidney disease (13.2% vs. 11.0%, p = 0.005); and to be on anticoagulation medication (71.3% vs. 65.3%, p < 0.001). Patients without SIC documentation were more likely to have an SI diagnosis of dementia (25.4% vs. 14.7%, p < 0.001). Eligible patients were equally likely to have a POLST on file with small differences in the presence of health care directives or disease-specific treatment guidelines. Utilization measures of inpatient, emergency department, palliative care, and ambulatory visits in the 6 months prior to the SI score of 5 were all significantly higher in the group with SIC documentation.
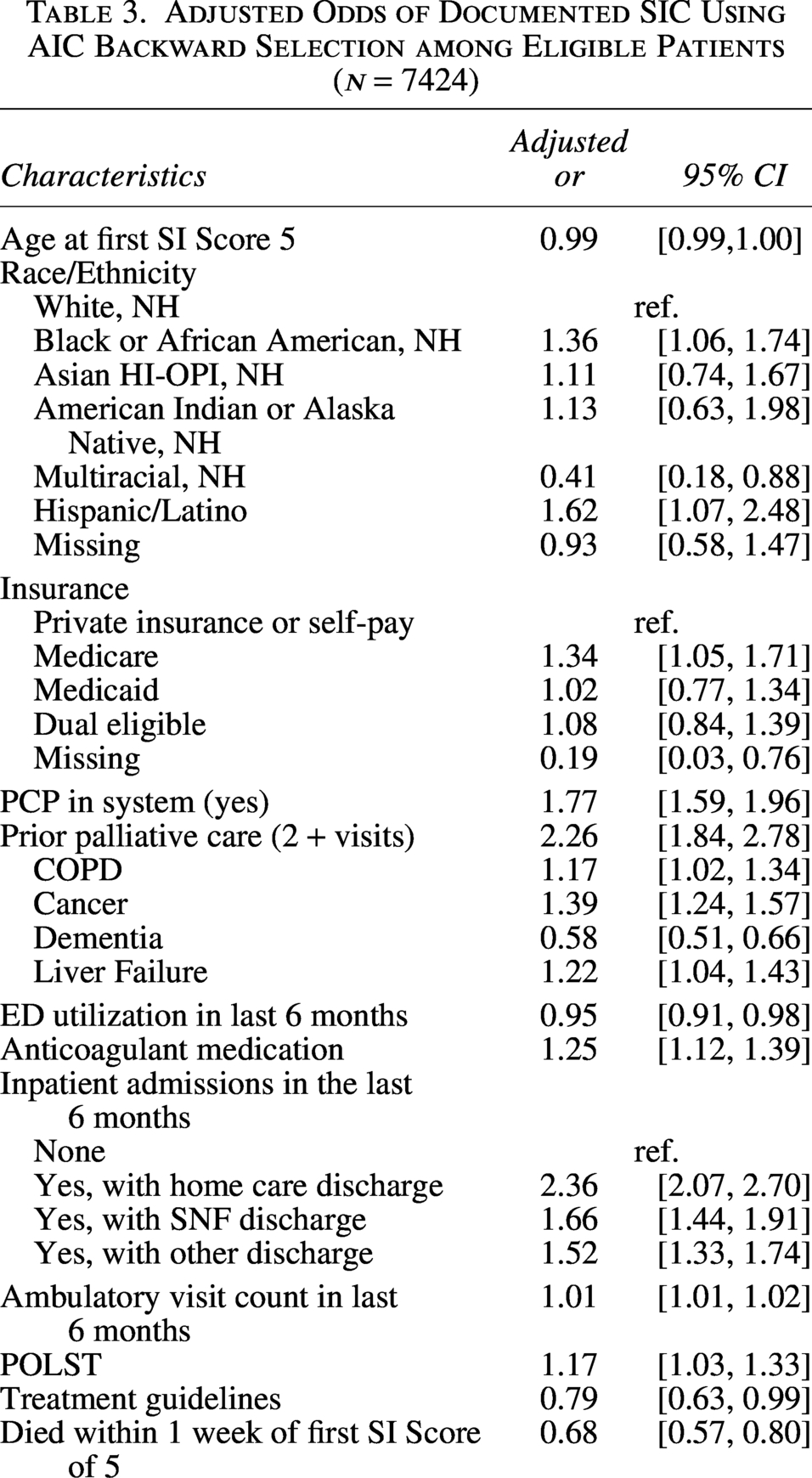
In the multivariate logistic regression model (Table 3), factors associated with increased odds of SIC included having 2+ palliative care visits (OR 2.26, 95% CI 1.84, 2.78), a primary care provider in the system (OR 1.77, 95% CI 1.59, 1.96), a prior inpatient admission with discharge to Home Care (OR 2.36, 95% CI 2.07, 2.70), and SI diagnosis of cancer (OR 1.39, 95% CI 1.24, 1.57). Additionally, both Hispanic/Latino (OR 1.62, 95% CI 1.07, 2.48) and Black (OR 1.36, 95% CI 1.06, 1.74) patients were more likely than White patients to have SIC documentation. Factors associated with reduced odds of SIC included dementia (OR 0.58, 95% CI 0.51, 0.66), disease-specific treatment guidelines present (OR 0.79, 95% CI 0.63, 0.99), as well as ≤1 week between level 5 and death (OR 0.68, 95% CI 0.57, 0.80).
Adjusted Odds of Documented SIC Using AIC Backward Selection among Eligible Patients (n = 7424)
Nearly half (45.3%) of the 3678 patients who had a documented SIC had the SIC prior to receiving an SI Score of 5 (Table 4). For these patients, the median time from conversation to SI Score of 5 was 1.89 weeks. For patients with the SIC after a score of 5, the median time between that score and the SIC was 8.97 weeks. Median time from first documented SIC to death was 12.75 weeks (IQR 3.6, 35.6 weeks). Most first SICs occurred during an inpatient admission (63.4%) and were documented by a physician (60.2%).
Characteristics and Content of SIC Intervention among Those Patients with SIC (n = 3678)
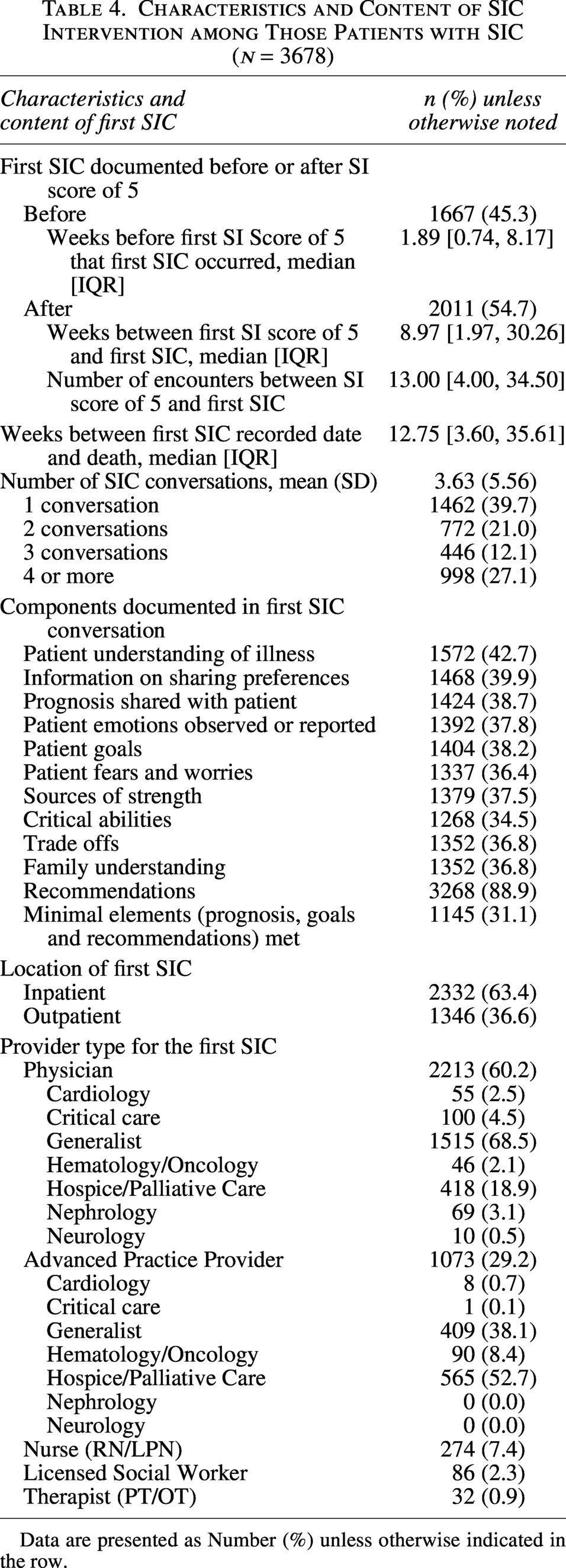
Data are presented as Number (%) unless otherwise indicated in the row.
Patients with a documented SIC had on average 3.6 conversations (SD 5.56), with 39.7% of patients having documentation of 1 SIC, 21.0% had 2 SICs, 12.1% had 3, and 27.1% had 4 or more (Table 4). For the first SIC, the most common component documented was recommendations (88.9%), followed by patient understanding of illness (42.7%) and information on sharing preferences (39.9%). The least prevalent component was critical abilities (34.5%). Just under one-third (31.1%) of first SICs documented contained all three of the defining components of a quality conversation.
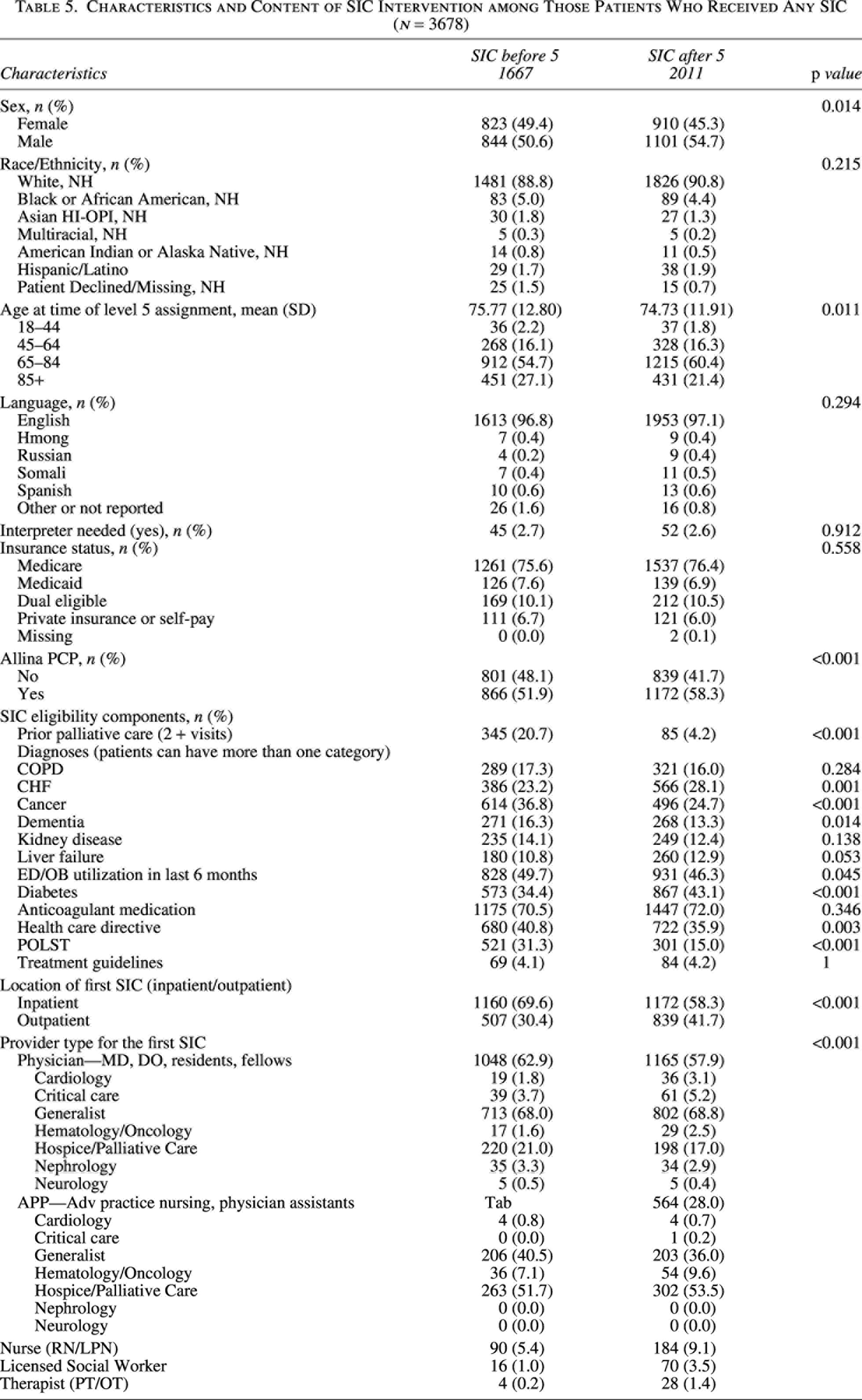
In the sub-analysis, patients with an SIC documented prior to an SI Score of 5 were more likely to have had prior palliative care visits (20.7%) compared with those with an SIC after an SI score of 5 designation (4.2%), p < 0.001 (Table 5). They were also more likely to have an SI diagnosis of cancer (36.8% vs. 24.7%, p < 0.001) and to have the first SIC conducted in the inpatient setting (69.6% vs. 58.3%, p < 0.001). These patients were more likely to have a first SIC completed by a physician (62.9% vs. 57.9%) or APP (30.5% vs. 28.0%), whereas those for patients with a conversation completed after an SI score of 5 were more likely to be documented by a nurse, social worker or therapist.
Characteristics and Content of SIC Intervention among Those Patients Who Received Any SIC (n = 3678)
Discussion
The results presented demonstrate the impact of a multi-year effort to implement an SICP in a large, integrated health system. In contrast to most other implementation studies, we introduced the SICP in both the hospital and outpatient settings. Notably, 30% of the first SICs were completed in the outpatient setting. Studies in the past few years have typically focused on one or the other setting. A primary care model found 63% of patients receiving SIC after provider training in six clinics, 17 another found a range of completion from 25% for patients identified as intermediate risk of mortality to 64% for high-risk patients in a hospitalized population, 20 or 65% or more for patients in the ICU 21 and another pilot found 13.5% among high-risk patients in an oncology setting. 23
Approximately half of our eligible patients received an SIC prior to death. This high percentage may be due to several factors. First, implementation of the SI score was concurrent with standardization of SIC documentation within the medical record. The SI score was visible across outpatient and inpatient settings and identified a large population of eligible patients. Additionally, incorporating training on the score, documentation tools, and the conversation technique gave clinicians adequate tools and confidence to enact conversations within the flow of patient care visits. Systemwide implementation across primary care, hospitalists, specialists, and interdisciplinary professionals with a focus on joint accountability and each patient touchpoint as an opportunity for a conversation enhanced buy-in over time from clinicians.
Concurrent training of providers from multiple disciplines, combined with allowing discussion time during training sessions to discuss implementation barriers in different clinical settings, resulted in several important outcomes, which may benefit implementation in other institutions. In one instance, we were able to create a new clinical visit type on the basis of provider feedback at a training session, which led to smoother scheduling, patient preparation, and documentation in the primary care setting. Additionally, documentation of completion in the hospital or recommendation for SIC completion after discharge from the hospital was built into standard transition documentation used by the hospitalists to communicate to primary care. Finally, the use of the SI score allowed for quantification of a seriously ill population. Documentation of the SI conversations in a standard template allowed for measurement of conversation completion and population penetration estimation. This measurement capability facilitated quality metric development for serious illness conversation performance, which was subsequently used for provider incentive measurements and pay-for-performance contracts within provider-payer contracts.
While our SICP prioritized patients with an SI score of 5, nearly half of the patients in our study had their first SIC before reaching that threshold. This finding suggests that clinician judgment was active in the identification of patients whose scores may not have accurately identified the severity of their illness, or clinicians may have engaged patients in SIC sooner. Similarly, an inpatient pilot of a similar SICP found that providers with training were more likely to have conversations substantially earlier than those without the training. 18
Our training strategy emphasized the importance of iterative conversations. We emphasized documentation of care goal discussions even if “incomplete” relative to the SIC guide. This is reflected in the finding that patients had multiple conversations (average 3.6) documented prior to death and partial conversation documentation. Average number of conversations was studied at smaller scale previously29,30 with multiple conversations also observed, though fewer overall (average 1.7–2.1 conversations over 2–3 years). Documentation within the SIC guide was often only partial with each element used in 30–40% of conversations, except for recommendations documented in >80% of conversations. Only 31.1% of conversations met our defined quality completion threshold. While our program encouraged the use of the SIC SmartForm for documentation of partial conversations, defining and reporting a quality threshold provides a measurement for conversation integrity. It also provides a framework for future study of conversation impact based on conversation quality.
A limitation of our current work is that we analyzed only the presence or absence of documentation in each section of the SIC conversation module, as opposed to the specifics of the text in the note sections. Two studies31,32 have suggested variability in what providers document in standardized conversation forms and the concordance between patient and provider recall of what was discussed. Analysis of the content of SIC documentation and the patterns of which elements are documented will likely be a direction of future research.
Initial analysis showed differences between patients who did and did not receive SIC based on disease process, with increased likelihood of SIC in conditions typically felt to represent more serious illness (cancer, renal failure). However, in multivariate analysis, specific care delivery associations including number of palliative care visits, having a primary care provider within the system and having been discharged from the hospital to home care, were more strongly correlated than individual patient diagnoses or factors. Primary care, hospitalists, palliative care, and home health clinicians were among the earliest groups where the program was implemented, which likely increased completion by providers and clinicians in these settings. Oo et al. 20 also found care delivery factors of hospital LOS and ICU admission within a hospitalization correlated with SIC more strongly than diagnosis.
In addition to care delivery factors, a dementia diagnosis correlated strongly with not having a documented SIC, both in the initial and multivariate analyses. Communication barriers frequently present in dementia including speech limitations and availability of proxies may contribute to reduced documentation of SIC. It may also be related to the challenges in identifying individuals with earlier-stage dementia using EHR data.
The restriction of inclusion criteria to decedents limits our ability to assess provider engagement in the SIC process among all patients identified as seriously ill during the study period. This decision was to enable examination of SIC engagement over the course of the end of life as well as utilization of care at the end of life (for another study aim). From a process implementation perspective, a limitation is that we were not able to provide a time series to assess the rate of uptake among all eligible patients after provider training, or rate of implementation of providers as they received training during a roll-out period.
Conclusion
Our implementation of SICP in an integrated health system resulted in the identification of a large population of seriously ill patients, with documentation of at least one conversation in nearly half of that group, 30% of which first occurred in the outpatient setting. Further work is needed to enhance the quality of completion documentation of conversations, to continue to increase the proportion of eligible patients with a documented conversation, and to more actively engage individuals and proxies of patients with dementia.
Authors’ Contributions
G.V.: Conceptualization, funding acquisition, writing—original draft, writing—review and editing; A.S.: Conceptualization, funding acquisition, methodology, data acquisition, supervision, writing—original draft, writing—review and editing; K.H.: Conceptualization, funding acquisition, writing—original draft, writing—review and editing; S.C.-P.: Methodology, formal analysis, data acquisition, writing—original draft, writing—review and editing; J.R.: Conceptualization, funding acquisition, writing—review and editing; E.D.: Conceptualization, funding acquisition, methodology, supervision, writing—original draft, writing—review and editing.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest.
Funding Information
This study was determined to be not human subjects research by the Allina Health IRB. This study was partially funded by the Allina Health Foundation Grant #: 2024-09-P08.
Appendix
Serious Illness Score Cut Points and Interpretation
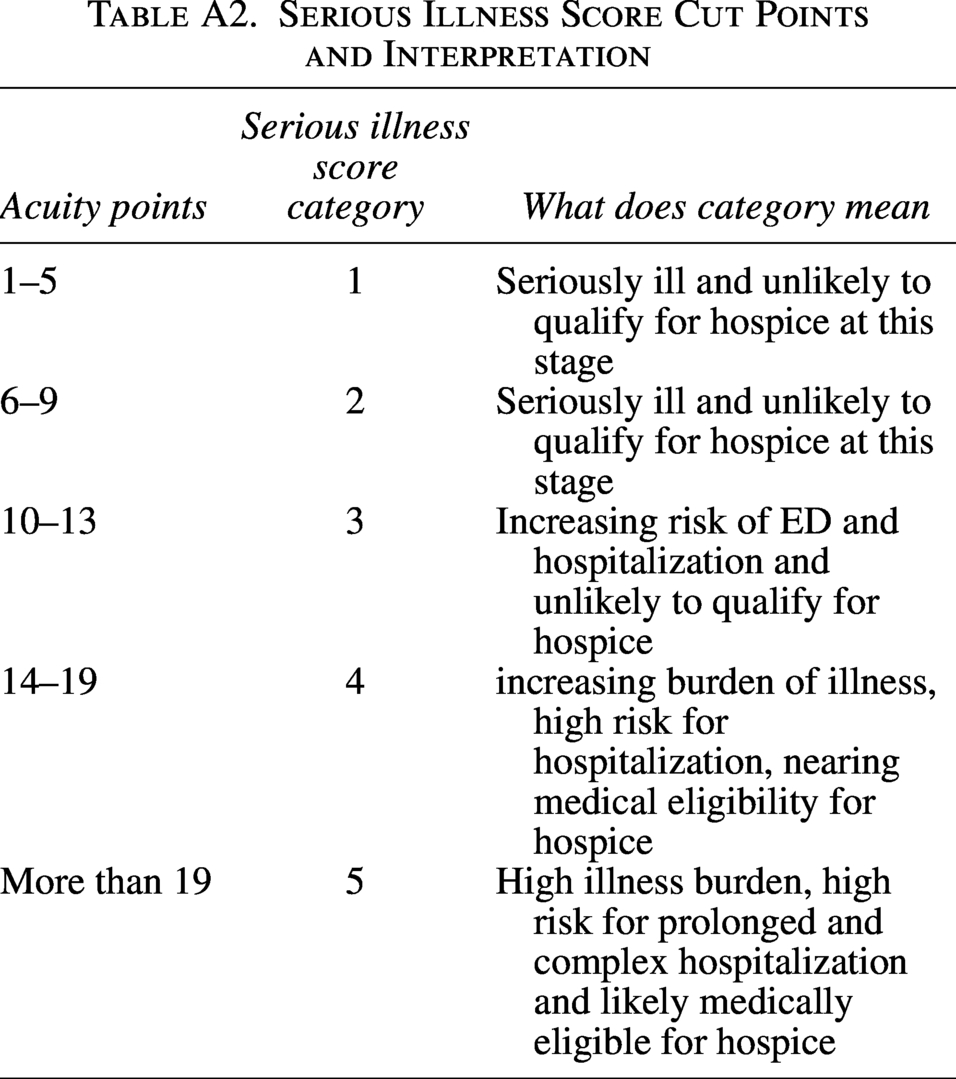
| Acuity points | Serious illness score category | What does category mean |
|---|---|---|
| 1–5 | 1 | Seriously ill and unlikely to qualify for hospice at this stage |
| 6–9 | 2 | Seriously ill and unlikely to qualify for hospice at this stage |
| 10–13 | 3 | Increasing risk of ED and hospitalization and unlikely to qualify for hospice |
| 14–19 | 4 | increasing burden of illness, high risk for hospitalization, nearing medical eligibility for hospice |
| More than 19 | 5 | High illness burden, high risk for prolonged and complex hospitalization and likely medically eligible for hospice |