
Abstract
Background:
Palliative care research encompasses varied topics, disciplines, settings, populations, and diseases. The National Institutes of Health (NIH) is a major funder of palliative care research and researcher career development.
Aim:
To characterize 10 years of NIH-supported palliative care research and identify research gaps and opportunities that could improve access, use, and quality of palliative care for individuals with serious illness.
Design:
We used keywords to identify new palliative care awards and publications from 2014 to 2024. We screened titles and abstracts using NIH iSearch tools for eligibility, yielding 899 awards and 1703 publications, then abstracted and analyzed research type, population, setting, and National Consensus Project for Quality Palliative Care (NCP) domain.
Results:
Palliative care research awards nearly doubled from 2014 to 2024 across 17 NIH institutes. Over 40% included clinical trials, and nearly 30% were career development or training awards. Most addressed the NCP domains of Structure and Processes (35.3%) and Physical Symptoms (20.4%). Publication influence was above average, measured by relative citation ratio. Most articles reported on data collection (36.9%) or secondary analysis (37.9%); few reported clinical trials (9.2%). Over 80 articles leveraged NIH-funded infrastructure. Few awards (7.8%) or publications (6.3%) addressed health disparities.
Conclusions:
NIH investment in palliative care research increased over the period of interest. Increased support for the breadth of palliative care research beyond end-of-life care, clinical trials and intervention development, studies focused on caregivers and palliative care for persons living with Alzheimer’s and related dementias, research and data infrastructure, and inclusion of palliative care-relevant content in large center and network awards are clear successes. While many 2004 NIH research priorities were addressed, gaps remain. Sustained investment with increased coordination could systematically accelerate translation of high-quality palliative care into widespread real-world practice.
Introduction
Evidence indicates a significant health span-lifespan gap in the United States, 1 meaning Americans are living longer but not necessarily with healthy longevity or quality of life, thereby increasing the need for palliative care services. Palliative care is an interdisciplinary specialty focused on improving the quality of life for people with serious illnesses and their care partners. Key elements of palliative care include treating symptoms and alleviating suffering (e.g., pain, nausea, or psychological distress), understanding and addressing the patient’s or family’s goals for care, and facilitating care coordination.2,3
Palliative care can be provided at any point along the trajectory of serious illness, even alongside curative treatment, and it includes end-of-life care. A serious illness is “a health condition that carries a high risk of mortality and either negatively impacts a person’s daily function or quality of life or excessively strains their care partners”, 4 examples include cancer; advanced heart, pulmonary, or kidney disease; Alzheimer’s disease and related dementias (ADRD); older adults with frailty or multiple serious chronic conditions; and children with medical complexity.5,6 The National Academies of Science, Engineering, and Medicine have identified multiple research gaps and opportunities including addressing health care system barriers to providing high-quality serious illness care; understanding and addressing disparities in care; and developing approaches and interventions to address the high prevalence of physical, psychological, and financial burden for persons with serious illness and their caregivers while providing care that is concordant with their wishes.7,8 As Americans live longer with serious illnesses across the lifespan, we need a breadth of palliative care research to build a high-quality evidence base that addresses gaps and opportunities that, if addressed, may improve access, use, and quality of palliative care for all individuals with serious illness.
After helping define the field and shape future directions through a National Institutes of Health (NIH) State-of-the-Science Conference Statement on Improving End-of-Life Care in 2004,9–11 the NIH increased support for palliative care research projects, research infrastructure, and career development and training. One notable example is the Palliative Care Research Cooperative, supported and managed by the National Institute of Nursing Research (NINR) from 2010 to 2023.a,12–17 Multiple NIH- and U.S. Department of Health and Human Services (DHHS)-funded systematic and other reviews have defined the science of palliative care, addressing areas such as the effectiveness of palliative care models and interventions, measures, quality improvement, implementation science, and qualitative research,5,11,16,18–22 and informed U.S. palliative care clinical care, policy, and guidelines.3,23
This scoping review aims to characterize the past 10 years of NIH-supported palliative care research and identify remaining research gaps and opportunities that, if addressed, may improve access, use, and quality of palliative care for all individuals with serious illness. We will describe NIH-supported palliative care research and career development awards between 2014 and 2024; provide an overview of NIH-funded palliative care-relevant research articles published during this same 10-year timeframe; and identify key research gaps and opportunities.
Methods
We used NIH Research, Condition, and Disease Categorization (RCDC), MeSH keywords, and additional keywords and phrases to define parameters for palliative care competing awards and NIH-funded publications from 2014 to 2024 in NIH iSearch. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews guided our methods for reviewing the resulting set of awards and publications. Using eligibility criteria based on the Population, Intervention, Comparisons, Outcomes, Type of Study, Setting, and Timing Framework (Table 1), we screened awards and publications for eligibility and abstracted and analyzed data on award and research type, population, content, setting, and National Consensus Project for Quality Palliative Care (NCP) Clinical Guidelines domain and adapted subdomain. The original subdomains were framed for clinical use and required adaptation to incorporate palliative care research concepts for this and similar palliative care scoping reviews. 24 The study team reviewed and confirmed record exclusions at regular meetings. Figure 1 illustrates the conceptual framework guiding the scoping review, including working definitions, NCP domains, adapted key subdomains, and research characteristics of interest.3,5,24
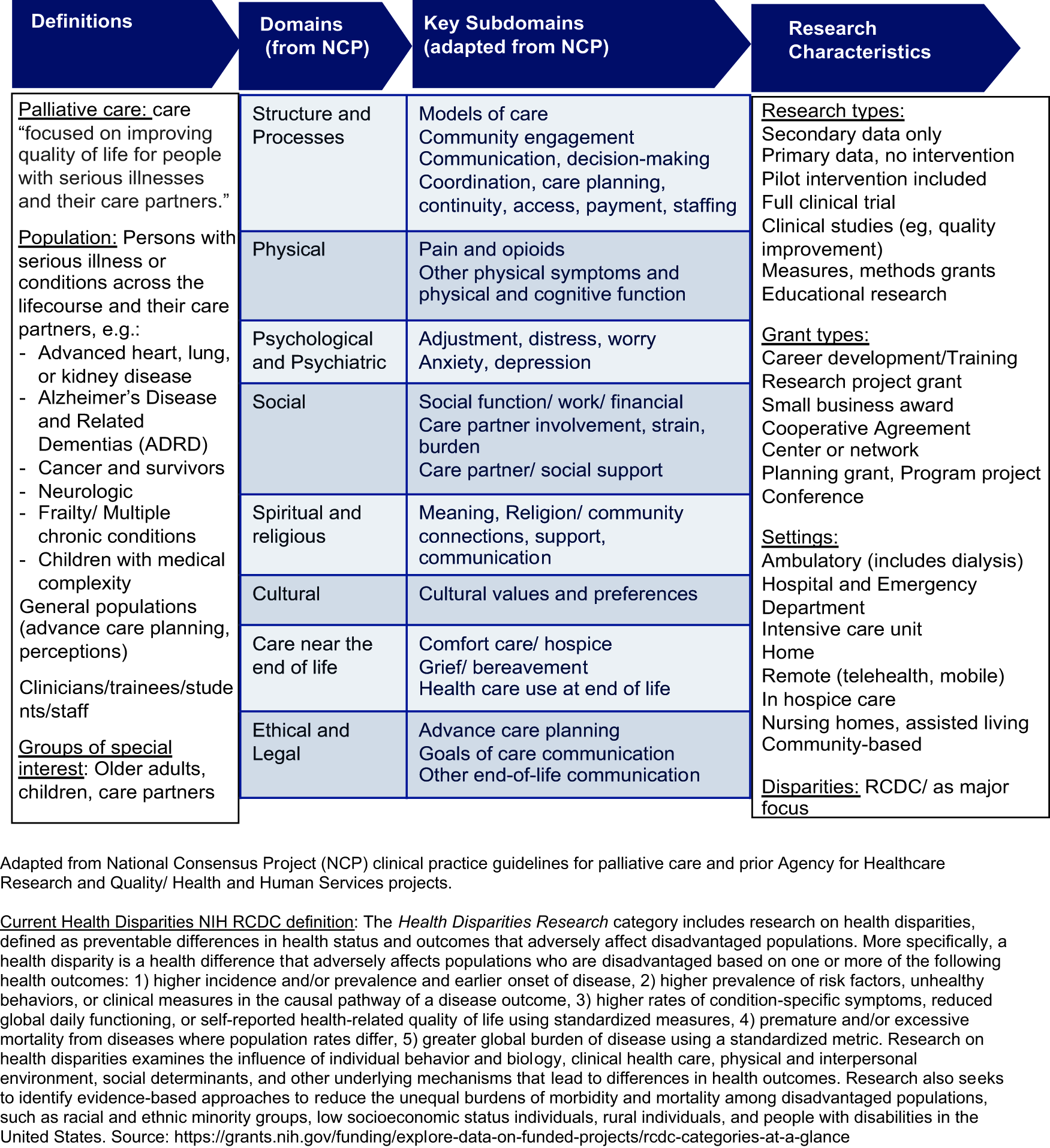
Conceptual framework (introduction).
PICOTS: Inclusion and Exclusion Criteria for Grants and Publications
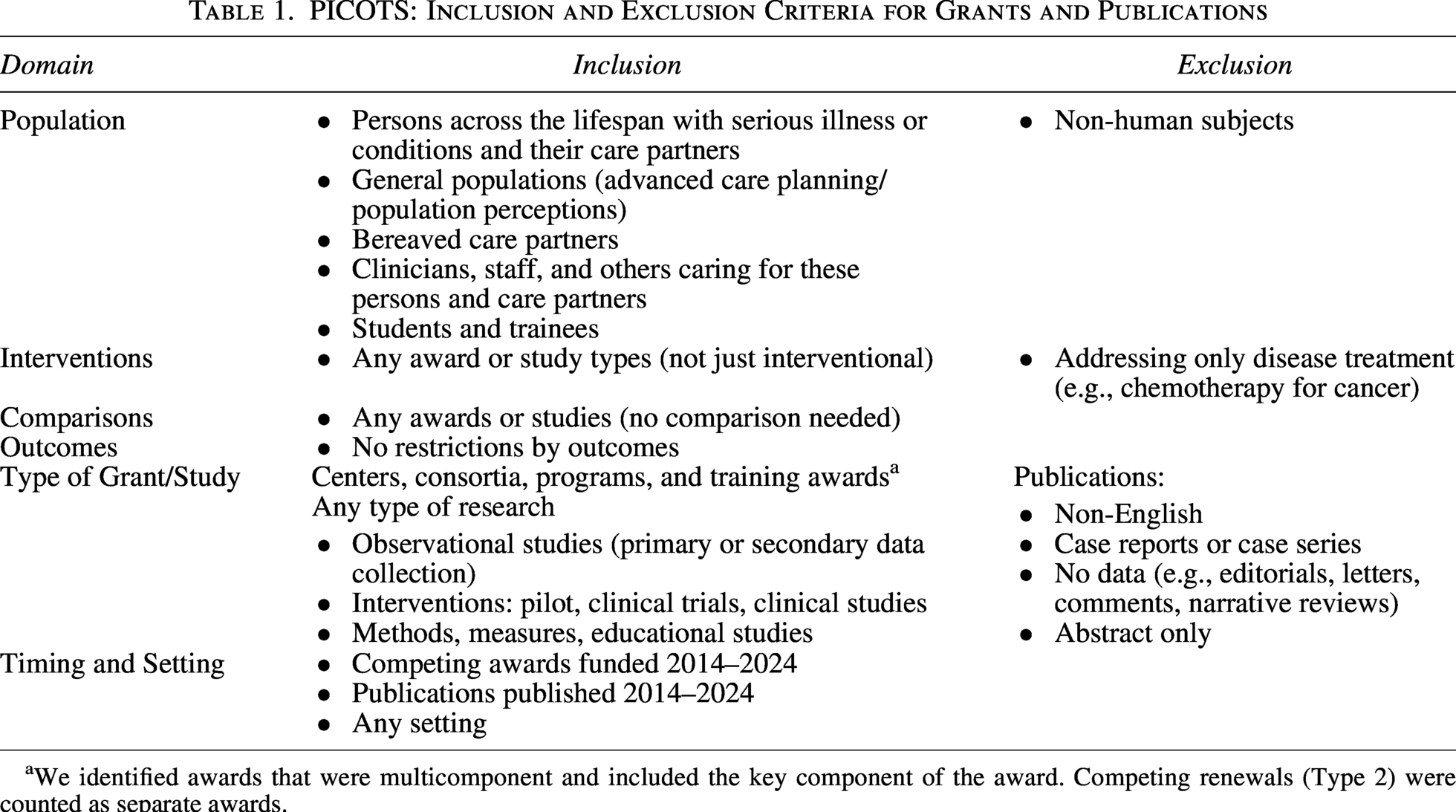
We identified awards that were multicomponent and included the key component of the award. Competing renewals (Type 2) were counted as separate awards.
Award search strategy
We used internal NIH iSearch portfolio analysis tools to identify unique palliative care awards (Table 2). First, we identified all new (competing) awards, including subprojects, made in fiscal years 2014 through 2024 that were assigned to the palliative care RCDC category. We included competing awards only (types 1 and 2) to restrict to unique projects. Because the RCDC category is broadly inclusive, we next removed any awards that lacked one or more specific palliative care keywords or phrases in the title, abstract, or specific aims. Finally, we reviewed each grant number, project title, abstract, and specific aims. We removed any awards that were duplicates; not human subjects; a non-related subcomponent of an overall award; focused on curative treatment; or otherwise not relevant to palliative care (e.g., management of chronic pain but not in the context of serious illness or palliative care). We identified 1055 competing awards, of which 899 (85.2%) met inclusion criteria (Fig. 2).
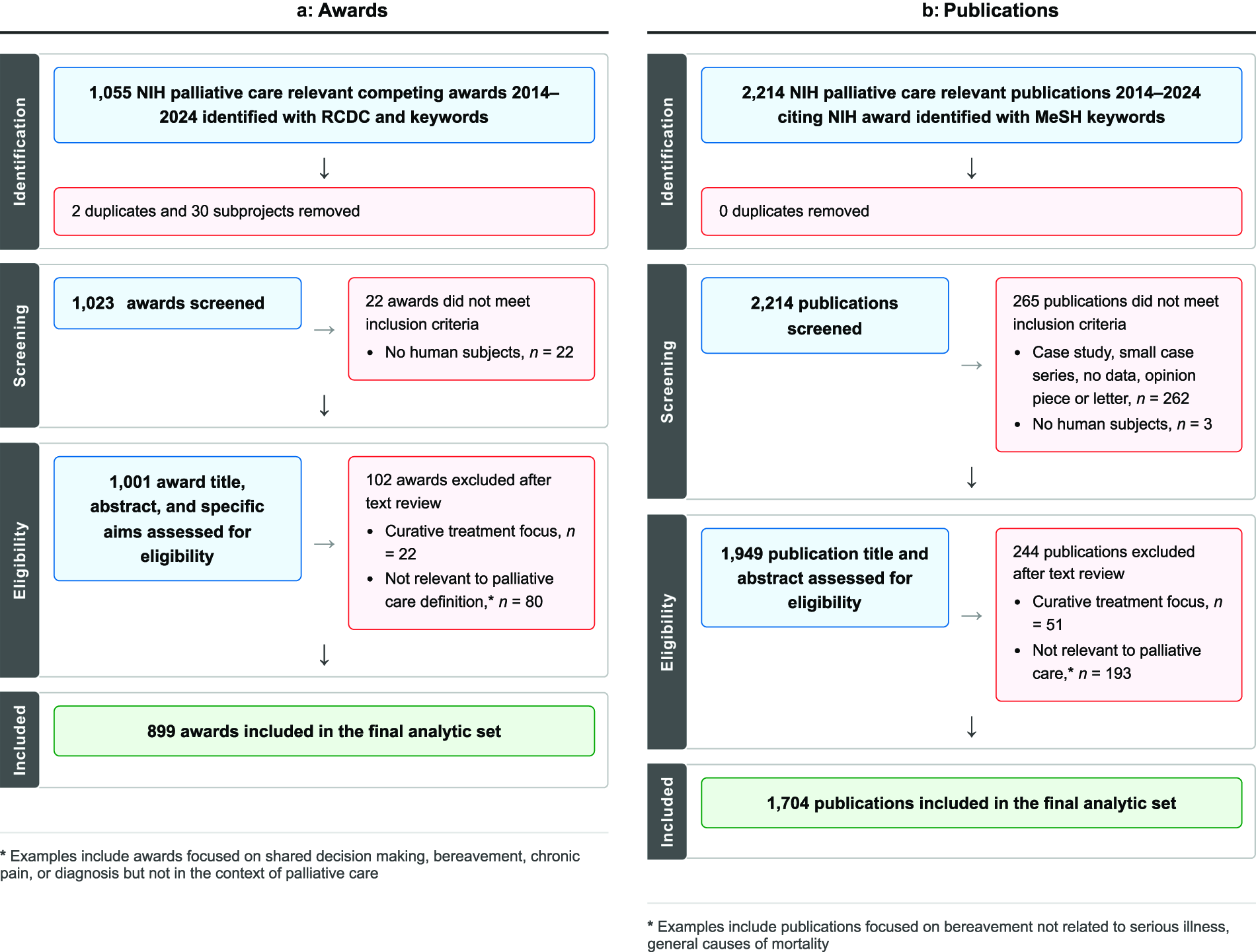
PRISMA diagram (methods).
Award and Publication Search Strategies a
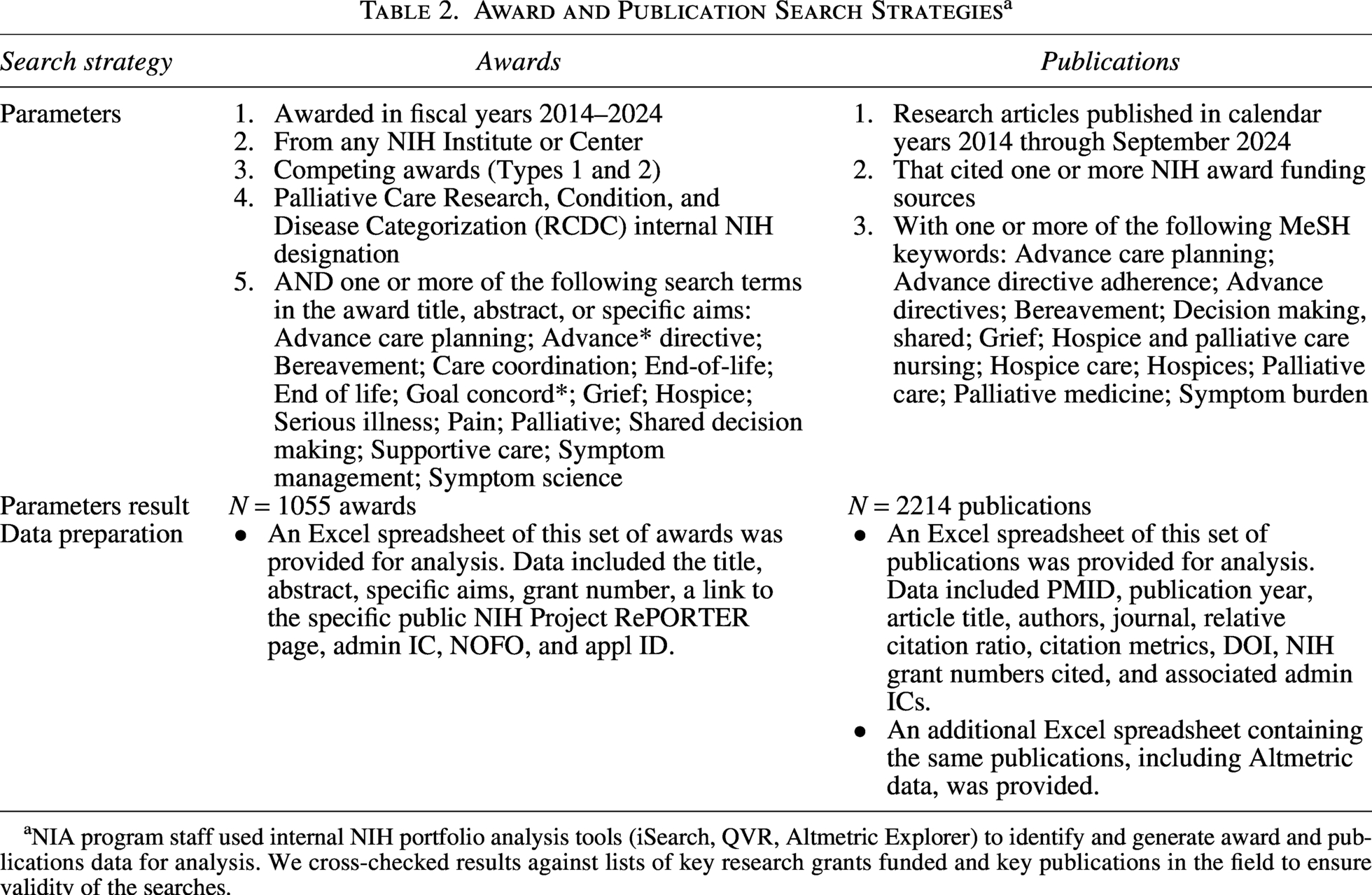
NIA program staff used internal NIH portfolio analysis tools (iSearch, QVR, Altmetric Explorer) to identify and generate award and publications data for analysis. We cross-checked results against lists of key research grants funded and key publications in the field to ensure validity of the searches.
Publication search strategy
Rather than restrict the universe of NIH-funded publications to those that cited the awards identified in the analytic set, we searched for palliative care-relevant articles among all NIH-funded publications (i.e., citing any NIH award) published from 2014 to 2024 (Table 2). We chose this approach because not all publications citing a palliative care-relevant award may be focused on palliative care; awards not identified as focused on palliative care may generate palliative care-relevant articles, and to accommodate the delay in time from completion of an award to publishing final results (i.e., many awards made in the 10-year time frame would not have had time to publish final results in the same time frame). First, we identified all NIH-funded publications with palliative care-related MeSH keywords. Next, we reviewed each article’s metadata, title, and abstract. We removed any that were not research articles, not reporting on human subjects, focused on curative treatment, or otherwise not relevant to palliative care (e.g., bereavement but not in the context of palliative care). We identified 2214 unique publications, of which 1703 (77.0%) met inclusion criteria (Fig. 2).
Data extraction—awards
Extracted data elements included application identification number (appl ID), grant number, activity code, fiscal year, administering institute or center, contact principal investigator name, title, abstract, specific aims, RCDC codes, and clinical trial status (yes/no). An award is defined as having a clinical trial consistent with the NIH definition of a clinical trial at the time of award. We extracted and coded additional information after reviewing the titles, abstracts, and specific aims of each award, including the primary serious illness or condition and NCP domains and their adapted subdomains (Fig. 1). We categorized primary study populations (children, adults, older adults, and care partners), care settings, and research types. We evaluated secondary analysis use of data sets funded by NIH. Using the internal NIH iSearch portfolio analysis tool, we coded awards identified with one or more health disparities research-related RCDC category “yes” for health disparities (except for 2014 and 2015 awards, for which the health disparities RCDC categories were not available in iSearch). Then we read titles, abstracts, and specific aims to determine whether at least one aim addressed a health disparities research question. b
Data extraction—publications
Extracted data elements included PMID, publication year, title, author(s), abstract, MeSH keywords, condition, NIH Relative Citation Ratio (RCR), 25 citations, DOI, and NIH grant number(s) cited. We extracted and coded additional information after reviewing the title and abstract, including population, serious illness or condition, setting, research type, health disparities focus (yes/no), clinical trial or pilot intervention development without a clinical trial, and NCP domain and adapted subdomains. A publication was determined to include a clinical trial based on review of the abstract; this determination was not contingent on whether the award(s) cited in the publication included an NIH-defined clinical trial. We also reviewed recent palliative care clinical practice guidelines, health care professional association documents, and systematic reviews for the use of evidence from NIH-funded publications.3,5,23,26
Data analysis
After screening and abstraction, we used a shared Excel workbook to derive variables from extracted data (award type based on activity code, subprojects to multicomponent awards, health disparities RCDC yes/no), populate variables coded by hand after review of each record (NCP domain, NCP adapted subdomain, research type, population, illness or condition, setting, health disparities relevant focus), and create cross tabs, pivot tables, and data visualizations to summarize the data.
Results
The final analytic set included 899 competing awards made and 1703 research articles published between 2014 and 2024 (Fig. 2). Table 3 provides characteristics of awards and publications, including primary setting, population, serious illness or condition, and research type.
Characteristics of Awards and Publications
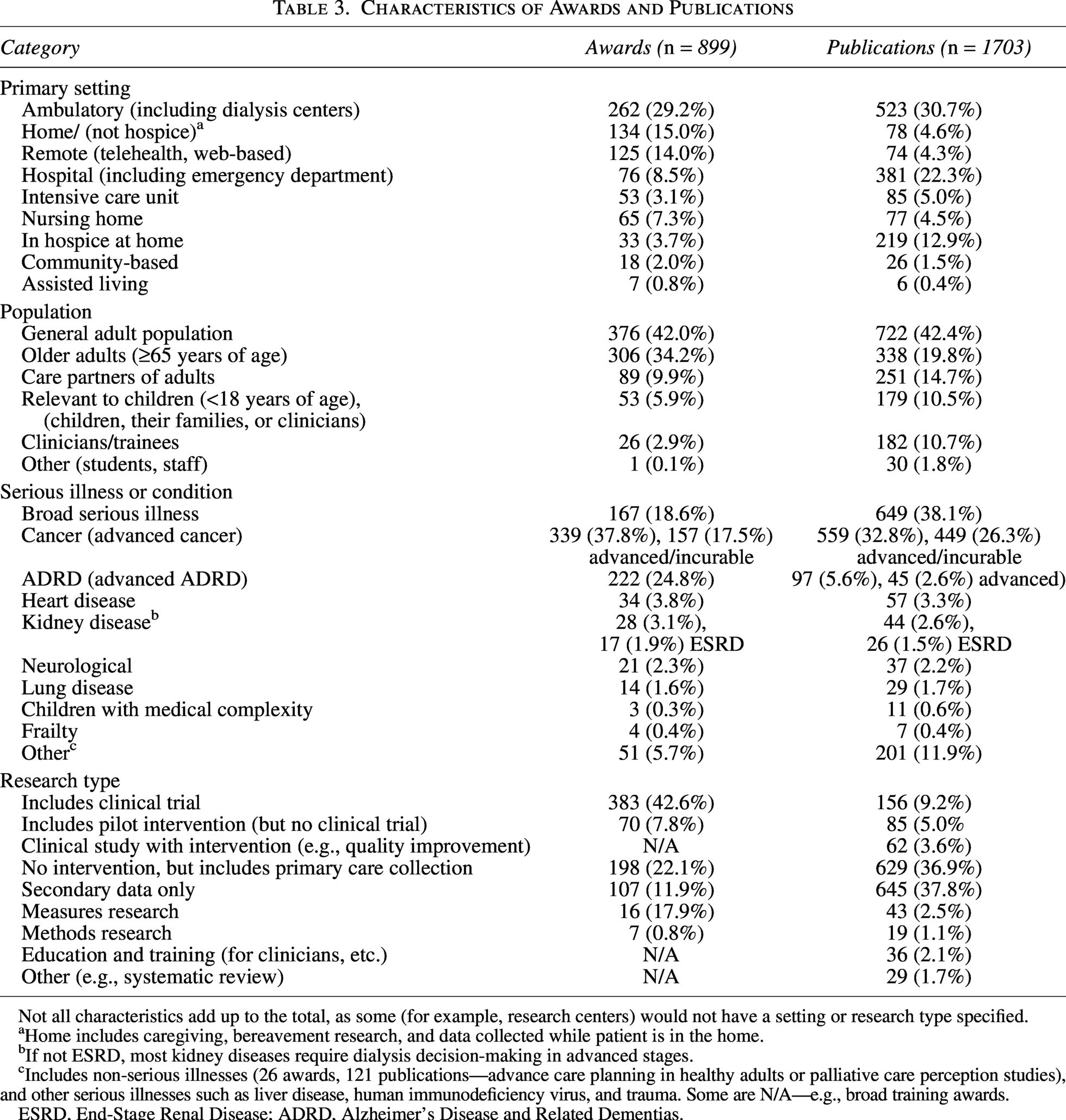
Not all characteristics add up to the total, as some (for example, research centers) would not have a setting or research type specified.
Home includes caregiving, bereavement research, and data collected while patient is in the home.
If not ESRD, most kidney diseases require dialysis decision-making in advanced stages.
Includes non-serious illnesses (26 awards, 121 publications—advance care planning in healthy adults or palliative care perception studies), and other serious illnesses such as liver disease, human immunodeficiency virus, and trauma. Some are N/A—e.g., broad training awards.
ESRD, End-Stage Renal Disease; ADRD, Alzheimer’s Disease and Related Dementias.
Awards
Between 2014 and 2024, the number of new palliative care research awards in a single year increased by 91% from 53 to 101 (Fig. 3). Over the same time period, the number of all NIH competing awards grew 9.5% from 18,979 in 2014 to 20,574 in 2024. Although there was modest growth in the share of palliative care research relative to all new NIH awards in that timeframe, palliative care continued to represent less than 1% of NIH’s extramural portfolio (0.28% of all NIH competing awards in 2014 and 0.49% of all NIH competing awards in 2024). The 899 NIH awards administered across 17 different Institutes and Centers were mostly research project grants (53.7%) or career development or training awards (29.5%). More than 40% of the awards included one or more clinical trials (42.6%), as defined by the NIH in the year the award was made, and 7.8% include pilot intervention studies without a full clinical trial. Almost 5% of the projects included were large center or network awards that were not entirely focused on palliative care but had a relevant component. The National Institute on Aging (NIA) (40.7%), National Cancer Institute (NCI) (27.6%), and NINR (18.9%) administered most awards. In contrast, 7 of the 17 institutes and centers administered fewer than 5 awards during this period (Fig. 4). Of all the institutes, NINR awarded the highest proportion of palliative care research (11.9%) among NINR’s competing awards during this time; NIA had the next-highest proportion at 2.3%. Using NIH RePORTER to determine total competing and non-competing costs, we estimate NIH’s financial investment in these 899 unique awards totaled $3.6 billion from fiscal year 2014 to 2024, with a 12% average annual increase.
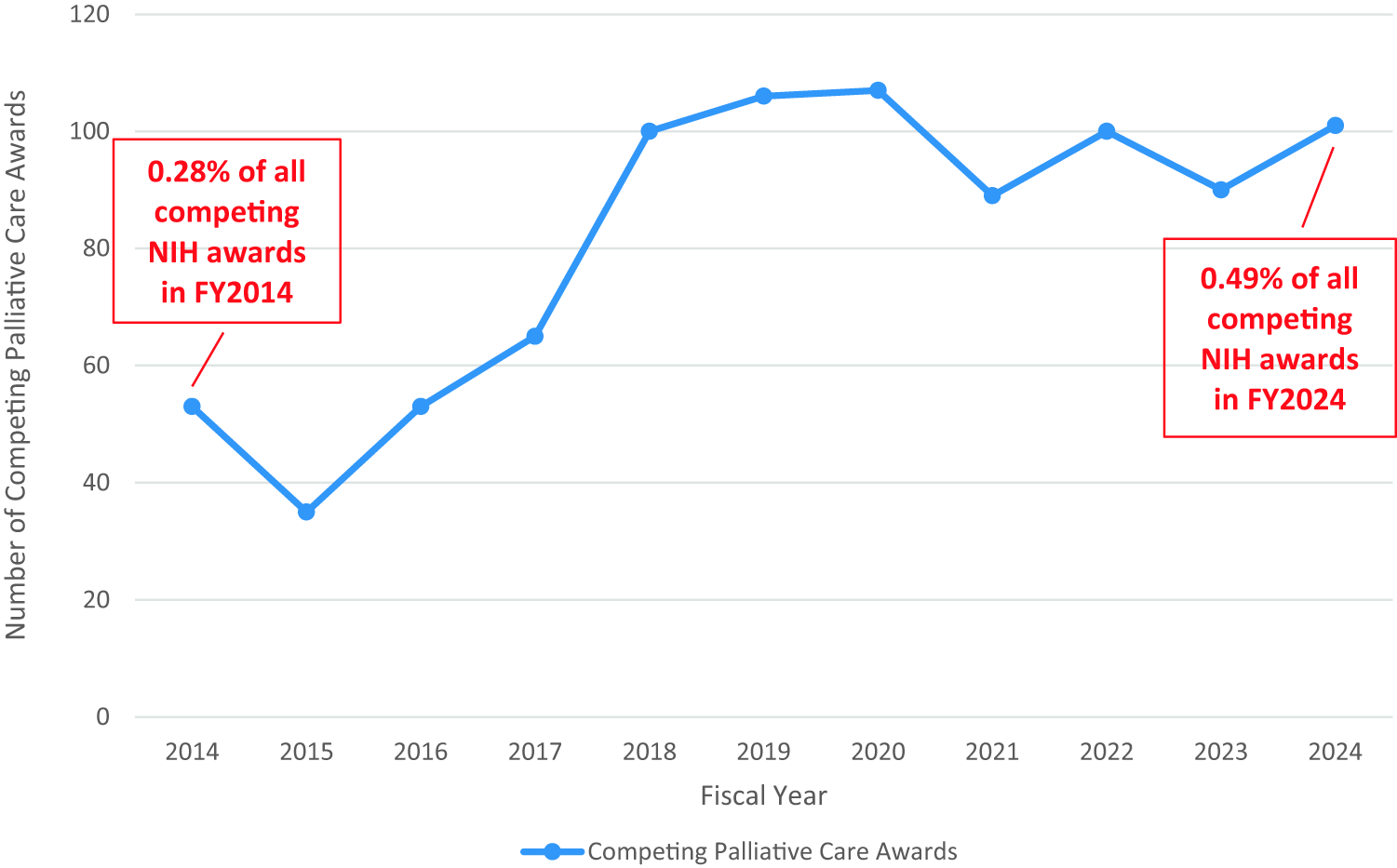
Time series of awards (results).
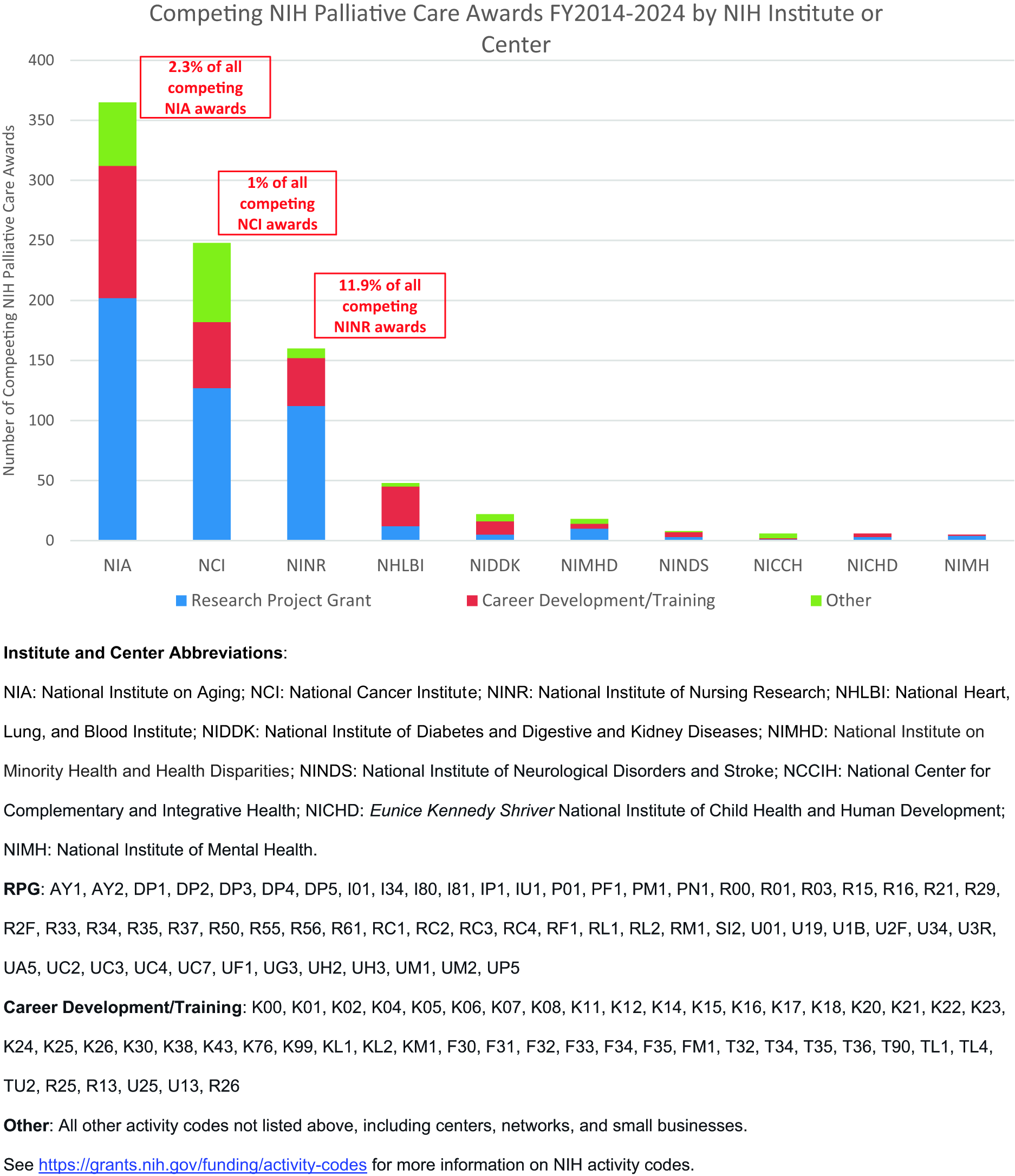
Awards by IC and activity group (results).
Nearly one-third of the awards were career development or training-related, including 163 career development awards, 53 pre- or postdoctoral fellowship awards, 15 pathway-to-independence awards (K99/R00), 15 research education or short-course awards, 12 institutional training awards, and 6 dissertation awards. This count did not include indirect support for palliative care scientific research workforce development from other NIH-funded research infrastructure, such as large consortia or center grants.
About 7.8% of all awards and 3.4% of awards with a clinical trial included one or more specific aims focused on disparities in palliative care access, use, or quality. Most studies took place primarily in ambulatory settings (29.4%), in the home (excluding hospice at home) (15%), or via telehealth or web-based modalities (14%). Fewer studies took place in hospitals (8.5%), nursing homes (7.3%), or hospice at home (3.7%). More than half of the studies were specific to persons with cancer (55.3%), and about one-quarter were focused on persons living with ADRD (24.8%). Most projects focused on the general (42%) or older adult (34.2%) population, and comparatively fewer focused on care partners of adults with serious illness (9.9%) or on children younger than 18 (5.9%).
The awards included a range of NCP domains and subdomains (Table 4). Most projects addressed the NCP domains of structure and processes of care (35.3%) and physical aspects of care (20.4%). Structure and processes of care include clinical communication and decision-making, care coordination and continuity, care access, staffing, and payment models. About 7% of awards focused on care for the patient nearing the end of life, and 10.9% focused on ethical and legal aspects of care, including advance care planning and broader discussions and planning for the care of the patient nearing the end of life.
NCP Domains and Adapted Subdomains of Awards and Publications
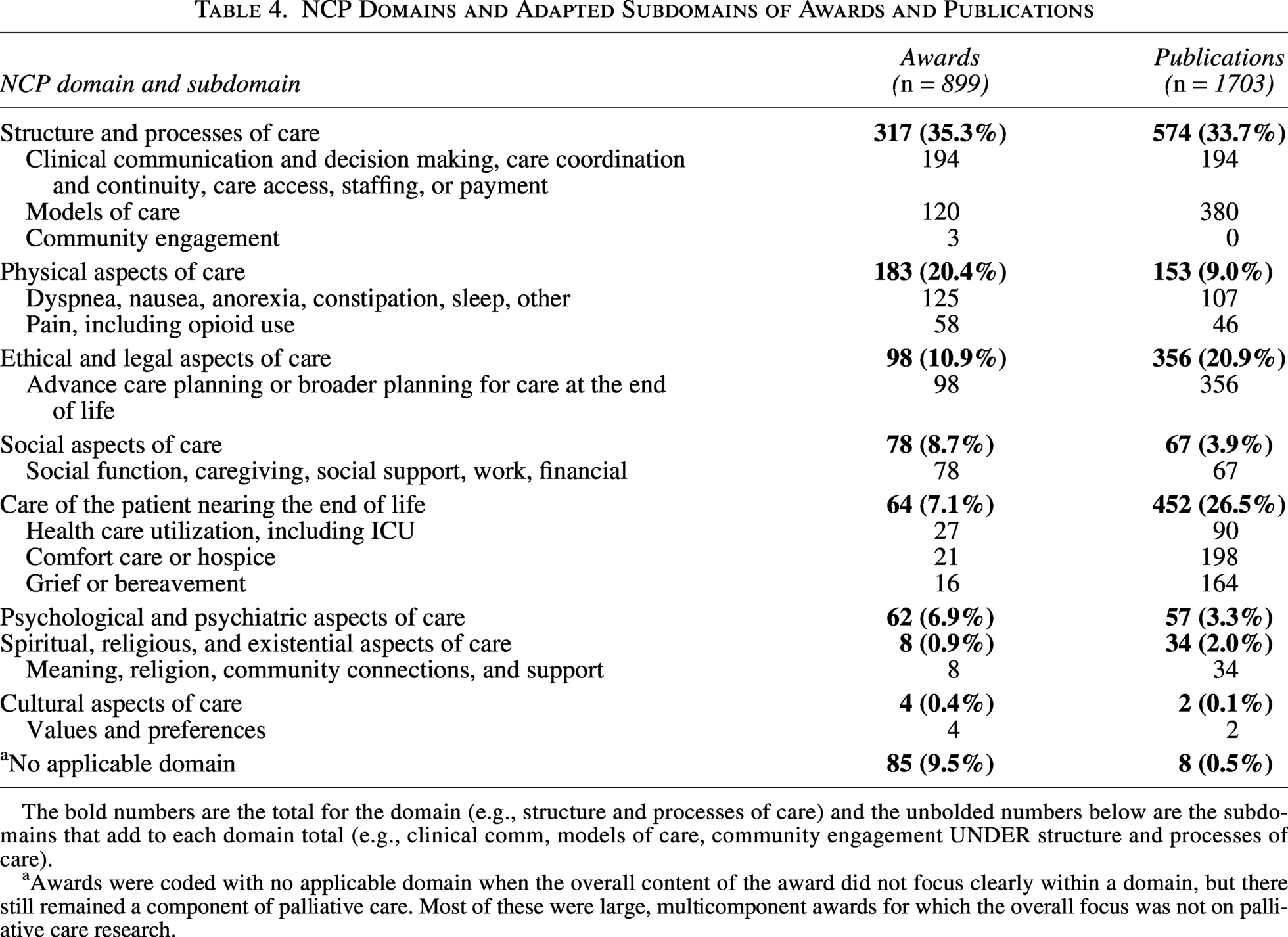
The bold numbers are the total for the domain (e.g., structure and processes of care) and the unbolded numbers below are the subdomains that add to each domain total (e.g., clinical comm, models of care, community engagement UNDER structure and processes of care).
Awards were coded with no applicable domain when the overall content of the award did not focus clearly within a domain, but there still remained a component of palliative care. Most of these were large, multicomponent awards for which the overall focus was not on palliative care research.
Publications
We used NIH’s iCite tool to obtain basic bibliometric metrics for the analytical set of 1703 research articles. c , 27 The majority of publications (1477) had been in the field long enough to be assigned an RCR, a citation-based measure of scientific influence normalized to citations per year for NIH-funded publications in the same field and year. 25 Of the articles with a calculated RCR, the mean RCR was 1.84, which means this set of publications had a greater-than-average influence in the academic literature than other NIH-funded publications in the same fields (an RCR of 1.0 would mean the set has, on average, the same number of cites per year as the median NIH-funded paper in its field, and an RCR of 2.0 would mean the set has received twice as many). Almost 300 (17.6%) of the articles were considered clinical articles, and 928 (54.5%) were cited by clinical articles, both indicators of potential clinical impact. The 20 most influential papers, as measured by RCR, included topics such as advance care planning or goals-of-care planning, aggressive care at the end of life, timing of palliative care, quality of care, patient and caregiver distress, and defining the serious illness population (Table 5).
Twenty Most Influential Papers Citing NIH Funding as Measured by Relative Citation Ratio
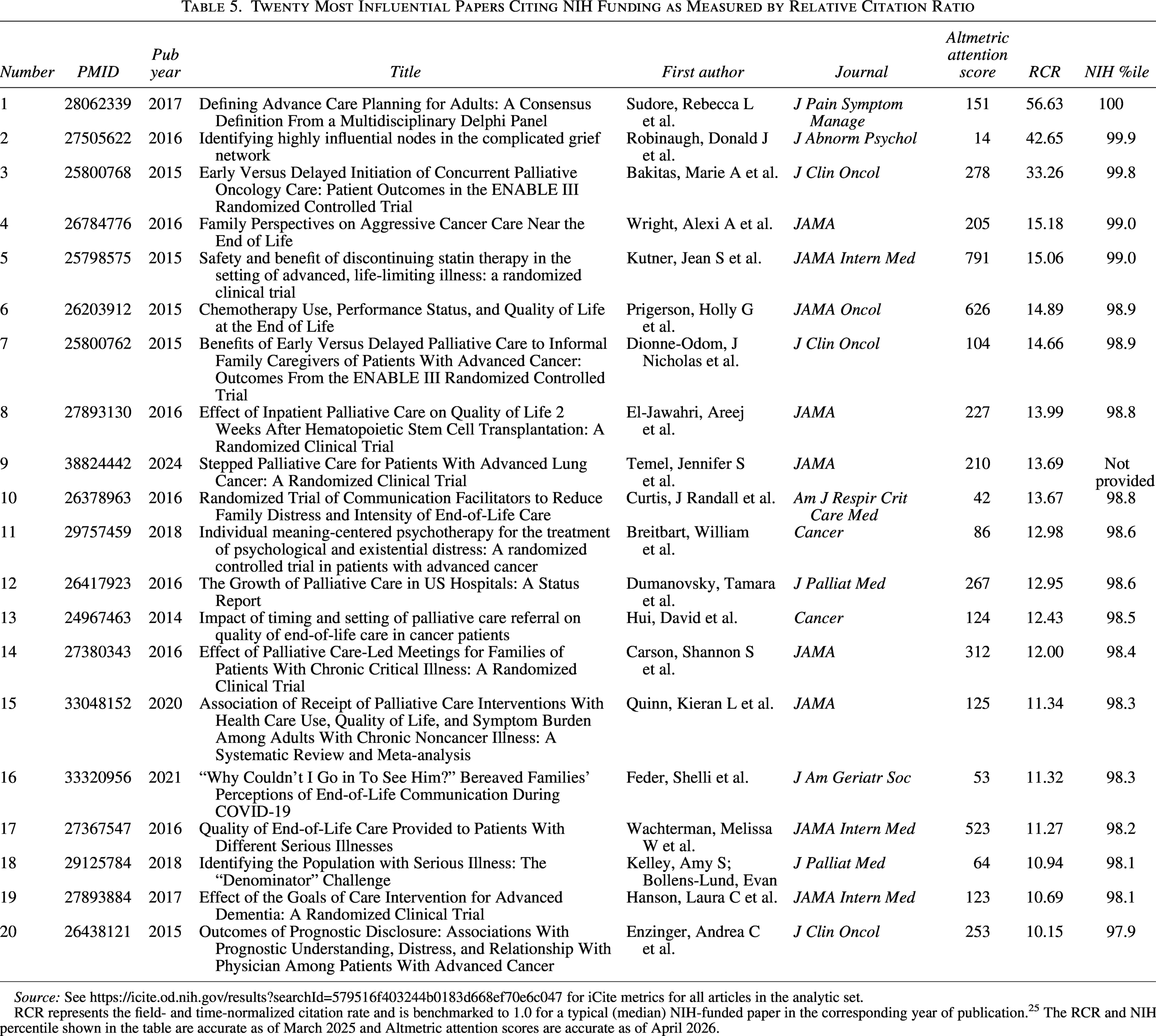
Source: See https://icite.od.nih.gov/results?searchId=579516f403244b0183d668ef70e6c047 for iCite metrics for all articles in the analytic set.
RCR represents the field- and time-normalized citation rate and is benchmarked to 1.0 for a typical (median) NIH-funded paper in the corresponding year of publication. 25 The RCR and NIH percentile shown in the table are accurate as of March 2025 and Altmetric attention scores are accurate as of April 2026.
Assessing the impact of research and clinical publications on real-world practice was more challenging than basic bibliometrics. Ways of measuring influence included citations or mentions in policy documents, clinical guidelines, clinician professional organizations, or patents. Recent palliative care clinical practice guidelines,3,26 American Medical Association policies, d and systematic reviews5,28 cited NIH-funded publications. According to Altmetric, a tool that generates metrics of influence beyond traditional bibliometrics, the analytic set of publications received 266 mentions in policy documents, 176 in clinical guidelines, and 17 in patents. Approximately 16% of the analytic set publications that appeared in Altmetric are considered within the top 5% of all research outputs scored by Altmetric.
Several articles reported on studies that leveraged other NIH- or DHHS-funded research or data infrastructure. Thirty articles used NCI’s Surveillance, Epidemiology, and End Results-Medicare linked data; 37 articles used NIA-funded Health and Retirement Study data (some also linked to Medicare claims data); and 19 articles used data from the NIA-funded National Health and Aging Trends Study and its sister study, the National Study of Caregiving. Based on a high-level scan of abstracts, approximately 200 articles used Centers for Medicare and Medicaid Services (CMS) datasets, including Medicare, Medicaid, Outcome and Assessment Information Set (home health care), Minimum Data Set (nursing home care), or Hospice Quality Reporting Program data.
The 1703 publications primarily reported on studies of persons with cancer (59.1%) or on serious illness generally (38.1%). Only 8.2% reported on persons with ADRD as the primary population. A modest portion of publications focused on children (10.5%) and caregivers (14.7%), while most involved adults generally (42.4%) or adults age 65 and older (19.8%). More than a third of the publications reported on studies involving non-clinical trial-related primary data collection (36.9%) or secondary data analysis (37.8%), while only 9.2% reported on a clinical trial. Most articles focused on ambulatory settings (30.7%), hospital settings (22.3%), or hospice at home (12.9%), while only 4.5% reported studies conducted in nursing homes. Only 6.3% of publications identified health disparities as a key objective, and 3.5% addressed special populations (e.g., rural health). Fewer than 3% of articles focused on measures development.
Like the set of awards, most publications reported on studies focused on the NCP domains of structure and processes of care (33.7%), including care planning and coordination, communication and decision-making, payment, staffing, quality, and models of care, or ethical or legal aspects of care (21.0%), most of which was focused on advance care planning. Unlike the awards, about one-quarter of the publications focused on care near the end of life (26.5%), including comfort care and hospice, grief or bereavement, and health care utilization.
Discussion
It is notable that between 2014 and 2024, the number of NIH-funded competing palliative care research-related awards grew 91%, while the number of all NIH-funded competing awards grew 9.5 percent. Although the share of NIH research that is palliative care relevant remains small (less than 1%), it seems likely that efforts among program staff at NIH, early calls to action within and outside of NIH, and readiness in the field have influenced this significant growth in NIH’s portfolio.
The 2004 NIH State-of-the-Science Conference Statement on Improving End-of-Life Care identified as priority research areas developing and testing of consistent and validated measures; enhancing methodological rigor of intervention development and clinical trials research; developing strategies to translate efficacious interventions into practice in real-world settings; understanding and characterizing patient, caregiver, and health care system influences on patient and family outcomes; supporting and leveraging retrospective representative cohort data that include variables relevant to palliative care; and facilitating collaboration and coordination among research funders, agencies, and public-private partnerships. Palliative care research is broad and interdisciplinary, and while research in these areas has grown significantly, the quality of the evidence base is varied. A systematic review to inform the fourth edition of the NCP clinical practice guidelines concluded the evidence base to be of limited quality due to inconsistency of study findings, the lack of precise effect estimates to support the effectiveness of interventions, and large variation in study designs, with few randomized controlled trials that allow strong evidence statements. 23 Another review concluded that increasing methodological rigor to inform health policy and practice should be a top priority for palliative care research. 29 Other assessments of palliative care research priorities included the need for systematic individual- and dyad-level intervention development; systems-level palliative care practice and capacity research; understanding the societal context for palliative care, including health systems, economic, payment model, health, and health care policy research; and addressing disparities in palliative care access and quality.7,8,30–35
NIH support of palliative care research suggests the field has evolved from an early focus on cancer, end-of-life, pain, and hospital settings to increasingly address other conditions, including ADRD, more upstream care in cancer survivorship and early dementia, broader symptom management, and ambulatory settings and web-based interventions.9–11,16 At the time of the NIH state-of-the-science conference in 2004, the focus in the field was on end-of-life care. Although care at the end of life remains a critical part of palliative care, the proportion of awards focused on other domains of care suggests a shift toward supporting a broader scope of palliative care science.
NIH awards focused on the domain of physical symptoms through broad screening and feedback programs, with little attention to mechanisms and to novel nonpharmacological and pharmacological interventions for important symptoms such as dyspnea or delirium. Multimodal pain management with opioid sparing was addressed only in a set of awards NIH solicited for end-stage renal disease. Some key domains received less focus among the awards or publications, indicating opportunities for further attention in future research, including the psychological and psychiatric, social, cultural, and spiritual and meaning-making aspects of palliative care.
Few awards addressed common patient and caregiver issues, such as feeding and incontinence; grief and bereavement; broader care planning for needs beyond advance care planning; and spiritual and religious issues, such as legacy and meaning. Some serious illnesses and conditions, such as pulmonary and hepatic disease, frailty, and multiple chronic conditions, or children with medical complexity, received little attention in the awards and publications. Many awards and publications focused broadly on developing or testing different palliative care models, but there was less attention to the implementation and dissemination of those models in the real world. Very few NIH-funded publications focused on measurement research or development (2.5%) or reported studies addressing health disparities in palliative care (6.3%), both of which have been identified as high priorities for palliative care research. 16
The use of NIH-supported data infrastructure being leveraged for palliative care research is a promising finding that indicates palliative care-relevant data elements and variables are being collected and shared in publicly available data resources that are not singularly focused on palliative care. Continuing this support and identifying additional opportunities to use existing data infrastructure for secondary data analysis can shed light on the changing palliative care landscape and help identify possible approaches or interventions to address remaining gaps. NIA, for example, supports multiple nationally representative cohort studies and manages the NIA Data LINKAGE Program to facilitate secure data linkages to CMS and other administrative data, which may be of further use to palliative care researchers. e
Overall, the number of new awards with clinical trials increased from 15 in 2014 to 46 in 2024. However, the spread across NIH institutes, variety of topics and populations, and lack of synthesis or coordination among them suggest limited opportunities to systematically build an evidence base positioned that can translate into real-world practice. Only 9.2% of the NIH-funded palliative care-relevant articles published in these 10 years reported on a clinical trial. Since we did not limit the publication search strategy to those citing the awards in the award analytic set, the low number of articles reporting clinical trials is not due to a lack of time for later-funded studies to publish. Further, the proportion of palliative care clinical articles is extremely low when compared to all NIH-funded clinical articles during this period. There were 294 palliative care clinical articles in our analytic set of publications out of a total of 63,662 NIH-funded clinical articles published during the same period, 2014–2024, which is 0.46%. f Continued concerns about the methodological rigor of palliative care intervention research and its translation into the literature and into real-world practice must be addressed. 23 Nonpharmacological interventions often do not move beyond efficacy to effectiveness and implementation studies (i.e., the “implementation cliff”), and the NIH Stage Model provides a set of best practices to facilitate that pipeline. g ,36
The NIH has recently undertaken efforts to improve coordination of palliative care research across its institutes, centers, and offices, and to support the next generation of palliative care research infrastructure. In 2023, the NIH designated NIA as the lead institute for palliative care research. NIA, under the leadership of Dr. Amy Kelley, convened a multi-institute palliative care research workgroup. h This workgroup convenes regularly to share palliative care activities and projects across the institutes, centers, and offices; identify high-priority palliative care research projects for funding; and discuss and generate initiatives. The Workgroup was instrumental in developing a request for applications for a multicomponent cooperative agreement award to support a broad range of research and career development to leverage synergies, coordinate efforts, develop the scientific workforce, and address remaining gaps in the field. i NIH awarded the Advancing the Science of Palliative Care Research Across the Lifespan (ASCENT) Consortium in August 2025. 37 NIA, NCI, NINDS, NINR, NICHD, and NIMH are co-funding the project. The Consortium award aims to develop a national scientific infrastructure needed to advance palliative care research; create new research knowledge and develop research methodologies; foster the career development and impact of the palliative care research workforce through small research project awards, training, mentorship, and access to methodological consultations; disseminate palliative care research findings; and facilitate implementation in real-world settings. A focus in the project on using the NIH Stage Model to guide intervention development holds promise for developing interventions that can eventually move beyond the implementation cliff. In partnership with the NIH, this project has the potential to leverage the progress made by the PCRC; further broaden the scope of palliative care research; increase the quality, rigor, and coordination of research efforts; and catalyze the field more broadly to contribute to meeting current research gaps and opportunities, particularly in the earlier stages of career development and the research pipeline.
Limitations
This scoping review has several limitations that must be acknowledged. We have been transparent about our search strategies to identify awards and publications, but alternative search strategies would likely have yielded different results. Using the citation of an NIH grant number in a publication likely missed some relevant articles or included less relevant articles because of under- and overciting funding sources. It was beyond the scope of this review to fully characterize the meaning and implications of alternative metrics of publication influence. Future work would be improved by a deeper analysis of publications cited in policy documents and clinical guidelines as defined by Altmetric and how these metrics should be interpreted relative to other bodies of work.
Although all authors participated in the conceptual framework, discussion of coding principles, and adjudication of difficult coding decisions, we did not have a second coder review each record. The coding of awards was based on the original application abstract and specific aims, which may not reflect exactly what occurred during the grant period, particularly because a pandemic occurred during this timeframe, impacting the conduct of much research. Although of tremendous interest, it was beyond the scope of this review to assess the quality of research, synthesize research findings, delve more deeply into assessing impact on real-world practice, or assess the career trajectories of recipients of palliative care career development or training awards. Finally, this review was intentionally restricted to NIH-funded research, which excludes the depth and breadth of palliative care research supported by other entities during this period.
Conclusion
NIH investment in palliative care research, career development and training awards, and publications has increased considerably over the last 10 years. Support for a breadth of palliative care research beyond end-of-life care, clinical trials, and intervention development; studies focused on caregivers and palliative care for persons living with Alzheimer’s and related dementias; research and data infrastructure; and inclusion of palliative care-relevant content in large center and network awards are clear successes. While many topics and research priorities identified in the 2004 NIH State-of-the-Science Conference Statement on Improving End-of-Life Care are included in the examined body of work, several research gaps and opportunities remain, including better coordination across the varied nature of palliative care research; work on ameliorating disparities in care access, use, and quality; measures and measurement development; and improving the rigor and translation of interventions. NIH-supported palliative care research spans multiple institutes, topics, disciplines, settings, populations, and diseases. There is evidence that NIH-funded palliative care research articles are influential in academic literature, but it is unclear to what extent promising findings are translating into practice. Sustained investment and increased coordination and collaboration have the potential to facilitate the systematic development of a cumulative body of science that can accelerate translation of high-quality palliative care into widespread real-world practice. The newly funded Advancing the Science of Palliative Care Research Across the Lifespan (ASCENT) Consortium is a significant and critical next step.
It is a fact that we will all die, and most of us will experience serious illness—either for ourselves or as a caregiver. Preparing palliative care researchers and supporting the development of an evidence base that can be translated into widespread real-world practice will benefit all individuals with serious illness and those who care for them. The breadth and depth of the palliative care research field need to grow commensurate with this universal need and continue to improve in its rigor and coordination.
Authors’ Contributions
All authors had full access to the study data and are responsible for the integrity and accuracy of the data analysis. Concept and design: All authors. Acquisition of the data: C.K. Screening, abstraction, and analysis of the data: S.D. and C.K. Interpretation of data: All authors. Drafting of the article: C.K. and S.D. Critical review of the article for important intellectual content: All authors. Administrative, technical, or material support: S.D. Project Management: C.K. Artificial intelligence was not used in any part of the conduct of the scoping review or writing of the article.
Statements and Declarations
The participation of Drs. Alexis Bakos, Elena M. Fazio, Basil A. Eldadah, and Chandra Keller, or the materials used, should not be interpreted as representing the official viewpoint of the U.S. Department of Health and Human Services, the NIH, or the National Institute on Aging, except where noted. The National Institute on Aging employed Dr. Basil A. Eldadah through April 2025. Dr. Sydney Dy worked on this scoping review in partnership with the other authors through an Intergovernmental Personnel Act agreement; no NIH funds were used to support her time and effort on this project.
Ethical Considerations
This article does not contain any studies with human or animal participants.
Consent to Participate
This article does not contain any studies with human or animal participants.
Data Availability
The authors are committed to transparency and to addressing bias in the conduct and writing of this scoping review. The data and related scoping review materials are available upon request to the corresponding author.
Footnotes
Acknowledgments
The authors would like to acknowledge input provided by the NIH Palliative Care Research Workgroup on the conceptualization of this scoping review.
Author Disclosure Statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
None of the authors received funding for this scoping review.