
Abstract
Existential concerns are common in serious illness and may include confronting questions about meaning, purpose, and mortality. The salience of these issues can vary between patients and throughout illness, and can oscillate between existential suffering, demoralization, normative processing, and even existential growth. Through analysis of a clinical composite case, this article illustrates dimensions and cues of existential suffering during serious illness. Recognizing the sources and manifestations of existential distress can help expand therapeutic imagination in serious illness care. Guided by existential principles, we draw on the tenets of Intensive Caring and Dignity in Care to offer practical language and psychotherapeutically informed communication strategies for general palliative care practice. These techniques aim to ease existential suffering, strengthen relational connection, and support patients in living meaningfully through the end of life.
Keywords
Introduction
In the setting of serious illness, existential concerns related to meaning, purpose, and belonging often intensify and become salient as individuals confront the fragility and limits of life. 1 In palliative care settings, psycho-existential symptoms are common and may become distressing. 2 Although prevalence estimates vary depending on the constructs evaluated, existential suffering among people with serious willness is reported in approximately 13–35% of patients.2–5 Importantly, patients may move dynamically along a continuum from existential suffering to existential growth, with experiences that fluctuate over time with illness progression, psychosocial and spiritual factors, relationships, and care encounters. 6 Recognizing and responding to existential suffering is a core component of palliative care practice.
Written for frontline, interdisciplinary palliative care clinicians, this article uses a case-based approach to illustrate concrete, actionable serious illness communication (SIC) techniques for responding to psychological distress rooted in existential suffering. Existential suffering is conceptualized through the lens of existential therapy’s core struggles, with parallels drawn between existential suffering, personhood, and dignity in serious illness to deepen recognition of the sources and manifestations of distress and to expand therapeutic imagination in SIC. 7 These existential principles are adapted and operationalized for routine serious illness care rather than as specialist psychotherapeutic interventions. We highlight frameworks intentionally designed for everyday clinical practice—such as tenets of Intensive Caring 8 to enact Dignity in Care 9 — that align with underlying psychological needs. Together, these approaches aim to ease existential suffering, strengthen relational connection, and support patients with existential distress in living meaningfully through the end of life. This article is the fourth in a nine-paper series on psychotherapeutically informed SIC.
Case Description
Mr. B is a 72-year-old retired mechanic, father, and grandfather with a history of alcohol use disorder, now living with decompensated cirrhosis. His illness course has been marked by refractory ascites, requiring repeat paracenteses, recurrent hospitalizations for upper gastrointestinal bleeding, and progressive renal dysfunction. Although his family remains hopeful that he may be considered for a liver transplant, Mr. B has struggled to engage in conversations about his goals and preferences, becoming increasingly withdrawn. In a period of openness, Mr. B becomes tearful, saying, “I wanted to see my grandkids grow up.” Later that day, a nurse reports that while assisting him with a bedpan, Mr. B broke down, saying: “Going to the bathroom in a pan—it’s disgusting. I can’t even go to the restroom on my own anymore. I used to take care of everyone, and now I can’t even take care of myself. This just…isn’t a life.”
Discussion
Mr. B’s withdrawal, inability to engage meaningfully in care, and tearful expressions of multidimensional loss suggest that he is struggling to cope with existential suffering caused by his serious illness experience. To accompany Mr. B in his existential suffering, clinicians can first consider the core struggles underlying his distress using foundational principles of the existential therapy framework. We can then respond with SIC techniques that align with his psychological needs, such as the tenets of Intensive Caring 8 to enact Dignity in Care. 9
Principles of existential therapy as a framework for understanding existential distress
Existential therapy emphasizes a set of core tensions arising from the fundamental condition of human existence. Among the most widely articulated frameworks, existential psychiatrist and psychotherapist Irvin Yalom described four central existential struggles: aliveness versus finitude; freedom versus responsibility; isolation versus connection; and meaning versus meaninglessness. 10 Existential suffering arises when individuals confront these fundamental conditions of existence without sufficient internal or external resources to cope; it is distinguished from normative existential concern by its intensity and all-encompassing nature. 11
Existential suffering in the context of serious illness can manifest in a wide array of potential distressing thoughts or emotions in a given patient— feelings of hopelessness; loss of meaning and dignity; regret, grief, and loneliness; worries of burdening others; fears of dying; questions about whether life remains worth living. 12 For some, it may manifest as demoralization, marked by profound hopelessness and helplessness arising from a loss of purpose or meaning in life.4,13
In serious illness, suffering has been conceptualized as a fracturing of personhood, occurring when illness disrupts identity. 14 These experiences are relationally embedded and shaped by connections with family, caregivers, and clinicians.15,16 Disease-related changes in cognition, communication, or function may evoke diminished or invisible personhood, sometimes described as a form of “social death,” as patients become increasingly marginalized within their social and clinical worlds. 15
Examining Mr. B’s experience through Yalom’s core existential challenges illuminates multiple sources of suffering (see Table 1). 10 Overt conversational cues reflect deep existential concerns, such as direct confrontations with death (“I wanted to see my grandkids grow up”), shifts in daily routines that threaten freedom and identity (“I can’t even go to the restroom on my own anymore”), changing relationships that raise concerns about belonging and isolation (“I used to take care of everyone”), and questions about what makes a meaningful life (“This just…isn’t a life”). Conversational cues may also be more subtly expressed within conversation; speech patterns and markers of disfluency may suggest difficulty conveying the gravity of one’s emotional response to the current situation. 17
Mapping Core Existential Struggles to Psychologically Aligned SIC Strategies
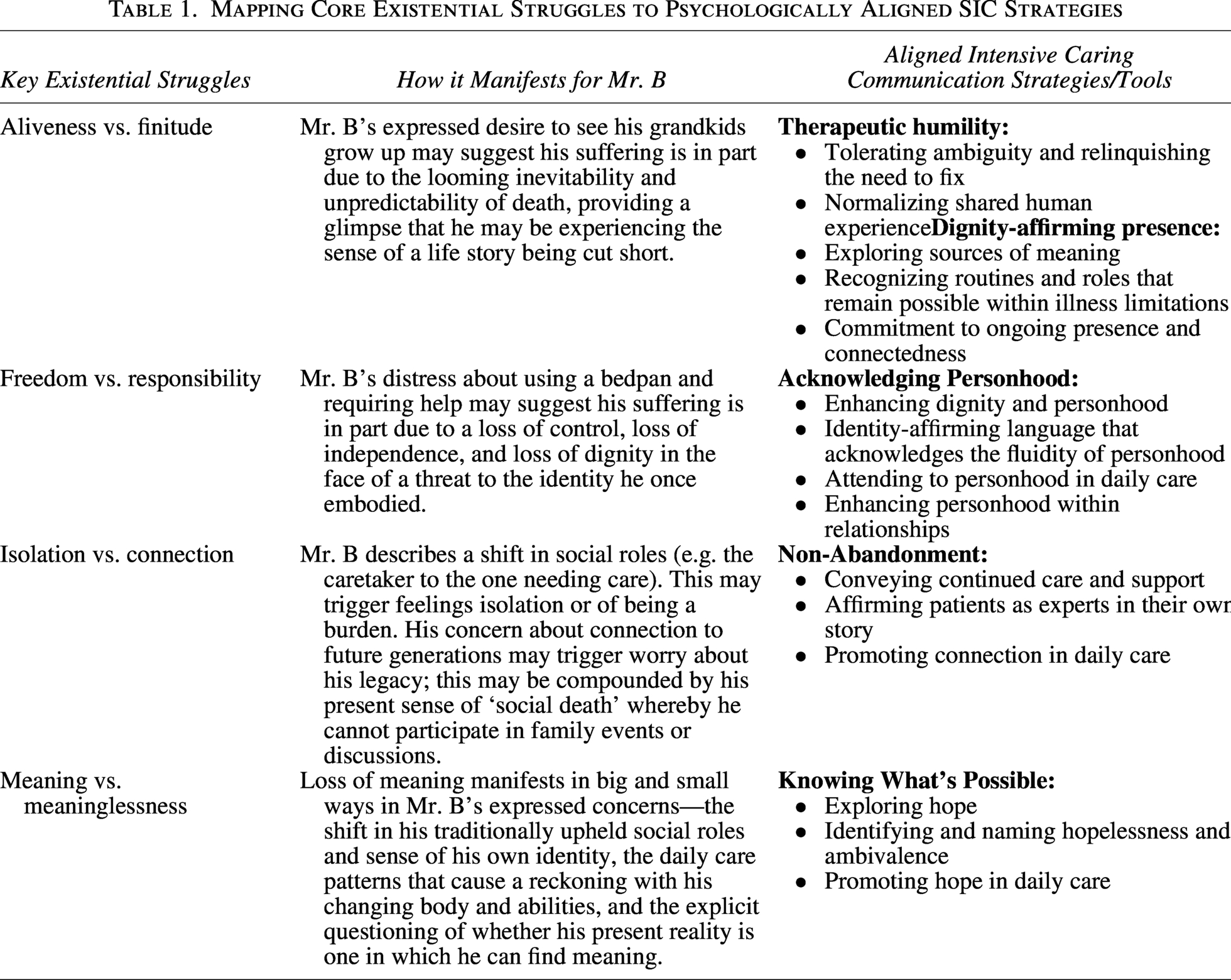
Viewed through the lens of fractured personhood, Mr. B’s reflections on who he once was suggest a profound disruption of personhood. His statement, “This just…isn’t a life,” signals he may be questioning whether his current state of existence remains meaningful or worthwhile.
While formal psychotherapy would be outside the scope of general palliative care practice, existential principles can inform therapeutic communication techniques in the face of existential distress, as illustrated below. Patients with severe or complex existential distress may additionally benefit from increased interdisciplinary support and clinicians with specialized expertise in psychological, psychiatric, or spiritual care.
SIC techniques aligned with existential principles
The concept of suffering, and strategies to address the various dimensions of suffering, are central concerns across health care disciplines, both as clinical challenges and as a moral imperative.
18
The Dignity in Care model, developed and disseminated by Harvey Max Chochinov, highlights how clinicians’ attitudes, behaviors, and systems of care have the potential to uphold (or erode) patient dignity. Informed by existential principles, Chochinov developed the tenets of Intensive Caring to describe a relational posture that operationalizes dignity in everyday clinical work. Below, we explore the application of five core elements as actionable SIC techniques: nonabandonment, acknowledging personhood, knowing what’s possible, dignity-affirming presence, and therapeutic humility.
8
Table 1 maps Mr. B’s existential struggles onto dignity-conserving strategies
19
embedded within the tenets of Intensive Caring.
For Mr. B, whose statements suggest existential loneliness and isolation,
20
clinicians can convey their continued care and support:
I know you’re used to taking care of others, and it sounds like right now, it’s a big change for you to accept help. I don’t know what will make this easier, however, I want to keep talking about it together. Our care team will keep showing up and working with you to make this feel more bearable for you.
Mr. B’s team may affirm his expertise and agency in his own story with statements such as:
What has helped you through adversity and hard times in the past? What can we do to support you accessing those resources now?
Mr. B’s team may also promote connection in daily care by inviting family participation as desired and pausing to create moments of deliberate slowness to foster connection within busy clinical settings.
For Mr. B, whose illness appears to threaten his identity, clinicians may ask the PDQ:
23
What do I need to know about you as a person to give you the best care possible?
Importantly, identity can evolve as patients adapt to illness, reorder priorities, and prepare for death. Mr. B’s team can affirm enduring values while also supporting the myriad ways that patients adjust to progressive illness
15
with language that acknowledges the fluidity of personhood: Even with illness, I still hear the problem-solving mechanic in you. I can see how painful it is to not be there for your grandchildren, which shows how deeply you care about your family.
Mr. B’s team can recognize aspects of care that he finds most undignified and ask questions that will guide strategies for supporting preferences, when possible, and preserving dignity:
What about your body or privacy feels most important to you right now? How would you like to be seen or known, despite the things that are happening to your body?
Mr. B’s team may leverage the relational dimension of his life to enhance personhood:
Are there special or important roles in your life that you would like to talk about? Are there lessons from your life you hope to pass on? Are there words of guidance or advice you would like to share with people you love or care about?
Clinicians also can affirm personhood within families by guiding care partners toward conversations that foster connection, comfort, forgiveness, and goodbyes, which may support both patients’ dignity and families’ grief and bereavement.
25
Dignity Talk
26
is a question framework designed to facilitate conversations between patients and their family members without the support of a therapist. These types of dignity-conserving conversations can include reminiscence, affirmation of the importance of a person’s story, and fostering narrative integrity.
27
I hear that your family is hopeful about transplant, and I share that hope. At the same time, I wonder if we can think together about what else you might be hoping for right now. Given everything you’re facing, what does hope look like for you today, even if it’s different from what you hoped for before?
Clinicians should be mindful that hope and hopelessness often coexist.
1
Mr. B’s team may explicitly name hopelessness or the dilemma involved in seeking hope during times of despair, thereby opening additional space for exploration:
28
People who tell me they feel hopeless often say they feel that nothing matters. I’m wondering if we can talk about what matters to you now, or what has mattered to you in the past?
Clinicians can promote hope in daily care by fostering meaningful connections, identifying near-term events patients may look forward to, gathering meaningful symbols such as photographs, music, letters, or poems, imagining alternate hopes centered on comfort or connection, and inviting reflection on wishes for loved ones in the future.
29
Dame Cicely Saunders observed, “If we can come not only in our professional capacity but in our common vulnerable humanity, there may be no need of words on our part, only for concerned listening”. 30
For Mr. B, whose statements reflect a sense of meaninglessness, clinicians might respond with communication strategies that affirm dignity through open-ended, exploratory questions that invite reflection on meaning, drawing from dignity therapy and meaning-centered psychotherapy approaches.9,31 His team may ask:
What gives you a sense of purpose right now? When have you felt most alive or connected? What do you hope people remember most about who you are?
Mr. B’s team may support him by upholding a sense of meaning in his days by recognizing activities of daily living as “Accomplishments of Disabled Life,”
32
supporting valued “normal” routines and roles in whatever ways are possible within his current limitations.
29
Relational care practices that uphold dignity are rooted in continued presence and an unwavering commitment to connectedness.
Conversations may therefore move between seemingly opposing ideas, such as supporting living well while acknowledging dying or holding space for meaning and security, uncertainty and grief.16,33 Allowing these dialectics to coexist, rather than attempting to resolve them prematurely, can create opportunities for existential growth. 16 Insights from other therapeutic contexts suggest that non-directive, supportive approaches that trust individuals’ intrinsic capacities may help patients transform their relationship to suffering, reconciling previously conceived paradoxes, even amid intense emotional states.34,35
For Mr. B, clinicians can model tolerating ambiguity and relinquishing the need to fix with statements such as:
It seems like you are grappling with how to live fully, even now.
Mr. B’s team can normalize shared human experience through statements such as:
Despite being very ill, I wonder what part of you feels strongest right now? Many people in your situation experience both grief and gratitude, or a desire for both solitude and connection. What do you think about that?
Conclusion
Suffering has been described as being experienced by persons, not merely by bodies, arising from threats to the intactness of the person as a complex psychological and social being.35 The relief of suffering has long been recognized as the central aim of palliative care. The core existential struggles described in existential therapy can provide clinicians a lens through which to recognize and consider the nuanced manifestations of existential suffering. 10 When existential distress emerges as a central driver of suffering, SIC techniques grounded in existential principles and adapted for routine clinical care, such as Intensive Caring, 8 may be particularly helpful in upholding patient dignity and addressing underlying psychological needs. Integrating these approaches—along with systems-level practice changes that prioritize time, training, and interdisciplinary support for relational and meaning-centered serious illness care—can help clinicians respond more skillfully to existential suffering while promoting dignity, connection, and meaning through the end of life.
Author Disclosure Statement
All cases presented in this series are hypothetical composites developed for illustrative and educational purposes. They do not represent real patients, and, therefore, consent to publish was not required. No competing financial interests exist.
Funding Information
No funding was received for this article.