
Abstract
Background:
Advance care planning has proven to be beneficial to medical care as it elicits patient preferences at the end of life, yet Indigenous populations have low rates of participation.
Objective:
This gap map scoping review serves to assess the current literature regarding the prevalence of advance care planning and palliative care characteristics in Indigenous populations of North America and Oceania.
Design:
Articles were identified from searches performed in five databases spanning the period from 2013 to 2023.
Results:
Twenty-eight articles met the inclusion criteria, representing studies conducted in the United States (n = 15), Canada (n = 2), New Zealand (n = 7), and Australia (n = 4). The included articles varied in study design, comprising qualitative (n = 16), observational (n = 7), mixed method (qualitative and quantitative) (n = 4), and interventional (n = 1). Two major findings endorsed across studies were (1) a high frequency of family involvement in end-of-life decision making and (2) awareness of culturally unsafe end-of-life services, creating hesitancy and mistrust.
Conclusions:
These results map the gaps in the existing research literature exploring the needs and preferences of Indigenous peoples in end-of-life decisions, palliative care, and advance care planning while highlighting a paucity of known effective interventions for Indigenous people.
Introduction
Advance care planning (ACP) is a process that allows patients to express their preferences for medical care when they are unable to speak for themselves. ACP is a beneficial, yet underutilized aspect of health care 1 that supports adults at any age or stage of health to ensure they receive medical care that is consistent with their values, goals, and preferences during serious illness. 2
Health care providers can use ACP as a tool to facilitate patient autonomy. Patients who complete ACP are less likely to report concerns with physician communication and are more comfortable with what to expect. 3 Conversely, poor quality of care at the end of life (EOL) can be attributed in part to a lack of ACP and discussions about preferences for care. 4
Internationally, differences in terminology and the legality of ACP documentation are well known. Australia’s ACP documentation primarily takes the form of advance care directives, which are recognized under legislation (statutory) or common law (nonstatutory).5,6 However, terminology differs by jurisdiction, and there is a lack of clarity regarding the legal standing of nonstatutory advance care directives. However, there remains growing support for standardizing and simplifying ACP and harmonizing legislation. 6 In comparison, New Zealand’s health agency, Te Whatu Ora Health (TWOH), offers comprehensive patient-centered guides that explore EOL preferences tailored to cultural values (www.myacp.org.nz). They also offer ethnic specific guides such as Whenua ki te whenua for Māori and Tōfā Fetāla’i for Samoans. These guides include headings such as “What matters to me” and “How I make decisions” to spark discussion and expand upon personal Indigenous values.
In the United States, only about 30% of adults had an advance directive in 2017. 1 This is also true in Australia, where a retrospective medical record audit among people with chronic diseases found that only 2.8% of the records had an advanced care directive, 3.9% had an enduring guardian, and 15.4% had documented resuscitation plans. 7 A New Zealand survey measuring different aspects of health, work, and retirement in older adults found that only 29.27% of participants had completed an enduring power of attorney document, 6.99% had completed a living will, and 3.98% had completed an advance care plan. 8 In a nationwide survey, 81% of U.S. physician participants felt they discussed ACP with their patients too late. 9 Having completed ACP is associated with a higher level of college education, higher socioeconomic status, older age, and a higher number of chronic illnesses. 10 Compared to Whites, ethnic minorities were less likely to have completed ACP.11,12 Common barriers cited include health literacy level, religion and spirituality, and health care system mistrust. 13 In Indigenous populations, ACP and EOL practices such as palliative care and hospice are underutilized. 14
The provision of care at EOL differs greatly between patients, each with particular needs for coping with illness. 15 Therefore, it cannot be treated with a singular, universal approach. A growing literature exists about patient values and EOL preferences, particularly those influenced by cultural understandings.16,17 Definitions of successful aging and what is perceived as a “good death” may differ between Indigenous populations and non-Indigenous populations. For example, Indigenous Australians have a strong connection to the land, so remaining “in country” is more important than life-sustaining treatment.16,18,19 Understanding the preferences of Indigenous populations at EOL and the facilitators and barriers to pursuing ACP will contribute to improving EOL outcomes among Indigenous populations. Literature reviews have synthesized research on issues in providing palliative and end-of-life care to Indigenous communities, highlighting the importance of providing culturally tailored care at the EOL.20–22 However, most reviews involve solely qualitative data, and little research has been done to synthesize both qualitative and quantitative research of multiple study designs among multiple Indigenous communities. Thus, this review aims to build upon this framework of knowledge and identify gaps in the current literature. The goal of this scoping review is to evaluate the existing literature about the prevalence and characteristics of ACP completion in Indigenous populations of North America and Oceania.
Methods
We performed two database searches to identify relevant articles. In search output 1, citations consisted of ACP completion in ethnic minorities overall (Supplementary Data S1). We searched PubMed and Google Scholar for articles published from September 2013 to October 2023 using search term keywords related to ACP (e.g., advance directive) and populations (e.g., ethnic minority). In search output 2, citation searches consisted of ACP completion specifically in Indigenous populations (Supplementary Data S1). We searched a wider range of databases, including PubMed, Google Scholar, PsycNet, Web of Science, and EBSCOhost, for articles published from September 2013 to October 2023 using search term keywords related to ACP and Indigenous populations (e.g., Native Hawaiian).
We exported search results into Zotero and removed duplicates. We screened titles and abstracts and, subsequently, with the remaining articles, conducted a full-text screening independently by two reviewers. We resolved disagreements by discussion and consensus. Included articles: (1) represented samples of Indigenous populations of North America and Oceania in entirety or in part; (2) were published in peer reviewed journals; (3) were published from September 2013 to October 2023; (4) addressed barriers to ACP, EOL care, palliative care, or POLST; (5) included adult participants (>18 years); and (6) were written in English. Excluded were articles that did not disaggregate data of multiple ethnic groups (Fig. 1).
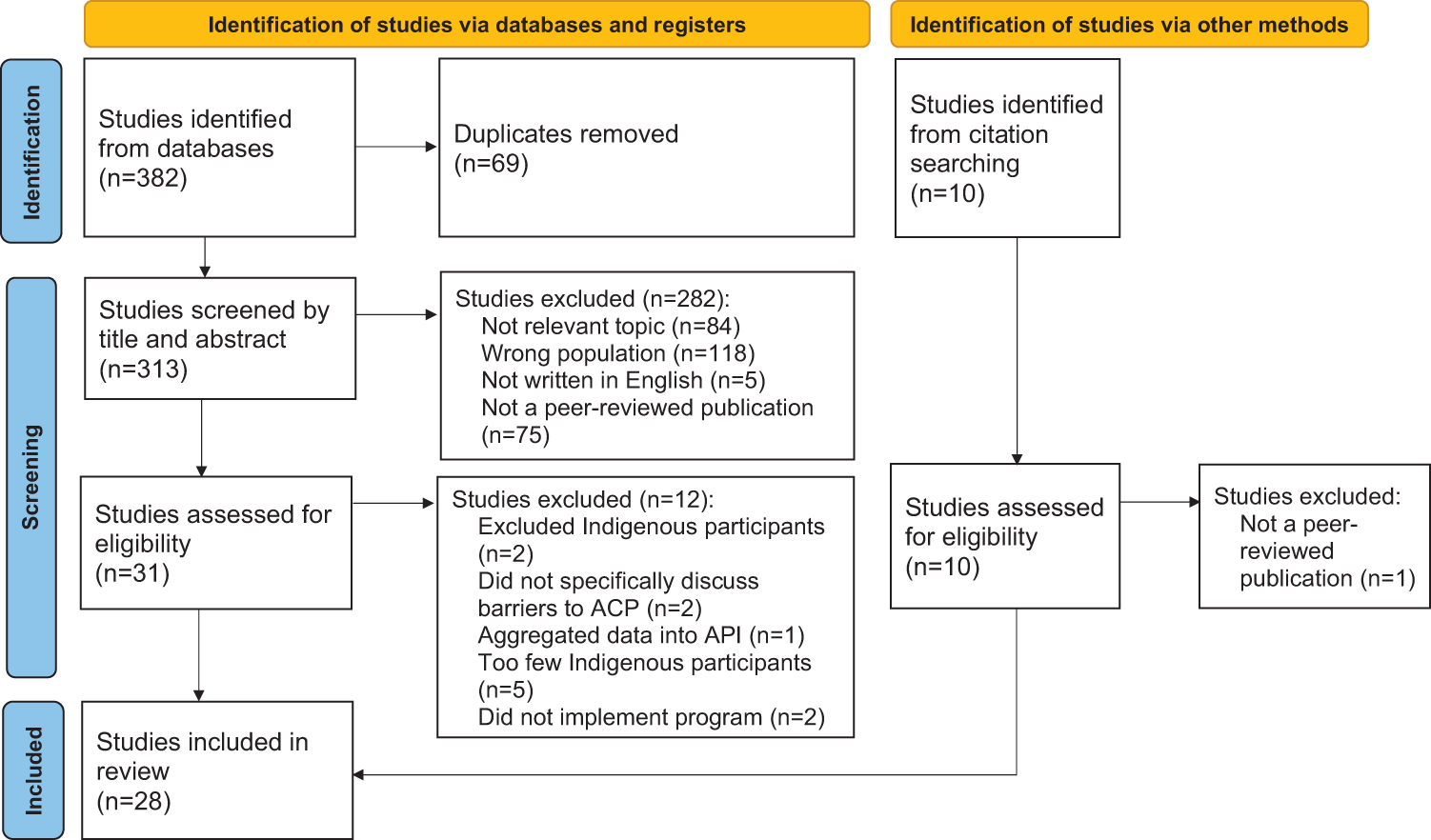
PRISMA flow diagram for selection of ACP publications of Indigenous People of North America and Oceania for Review.
Using a data charting form, two reviewers independently extracted relevant information from each included article and discussed and continuously updated the table in an iterative process. We grouped studies by design type, characteristics (e.g., country of origin, aim, study methods), population (e.g., number of Indigenous participants in the total sample), and main findings. Because this review integrates evidence from multiple study designs, we employed a data-based convergent synthesis approach to combine qualitative and quantitative findings. Following the approach described by Noyes et al., all included studies were analyzed using the same methods, and the findings were integrated and presented together to address a single review question. 23 One reviewer identified recurring topics and created inductive code categories. Two reviewers then discussed the categories and independently grouped the findings by category using Microsoft Excel. From these categories, we identified five overarching themes: (1) culture and spirituality, (2) location/place of death is highly valued, (3) family support and relationships, (4) health system improvements, and (5) access to ACP resources. Following the identification of the five overarching themes, coded data within each theme were reexamined to identify patterns of convergence and divergence. Related codes were clustered to form subthemes, which reflected more granular distinctions within each broader domain. Subthemes were iteratively refined through discussion until consensus was achieved.
Evidence and gap maps (EGMs) represent a novel approach for synthesizing and visualizing the existing evidence related to a specific research question. 24 EGMs are particularly valuable for identifying gaps within the current literature, as well as highlighting areas that have been extensively studied. The EGM for this review was developed using the same methodological framework as the review itself, including the formulation of a research question, conducting a comprehensive search, screening against predefined inclusion and exclusion criteria, and the systematic coding of included studies through thematic analysis. Figure 3 was produced using Evidence for Policy & Practice Information (eppi.ioe.ac.uk) (EPPI) Mapper (Version 2.4.5).
Results
Literature search results
In total, 28 citations met the inclusion and exclusion criteria (Fig. 1). The study designs were interventional (n = 1, Table 1), observational (n = 7, Table 2), qualitative (n = 16, Table 3), and mixed methods (n = 4, Table 4). Studies were conducted in the United States (n = 15), New Zealand (n = 7), Australia (n = 4), and Canada (n = 2) (Fig. 2).
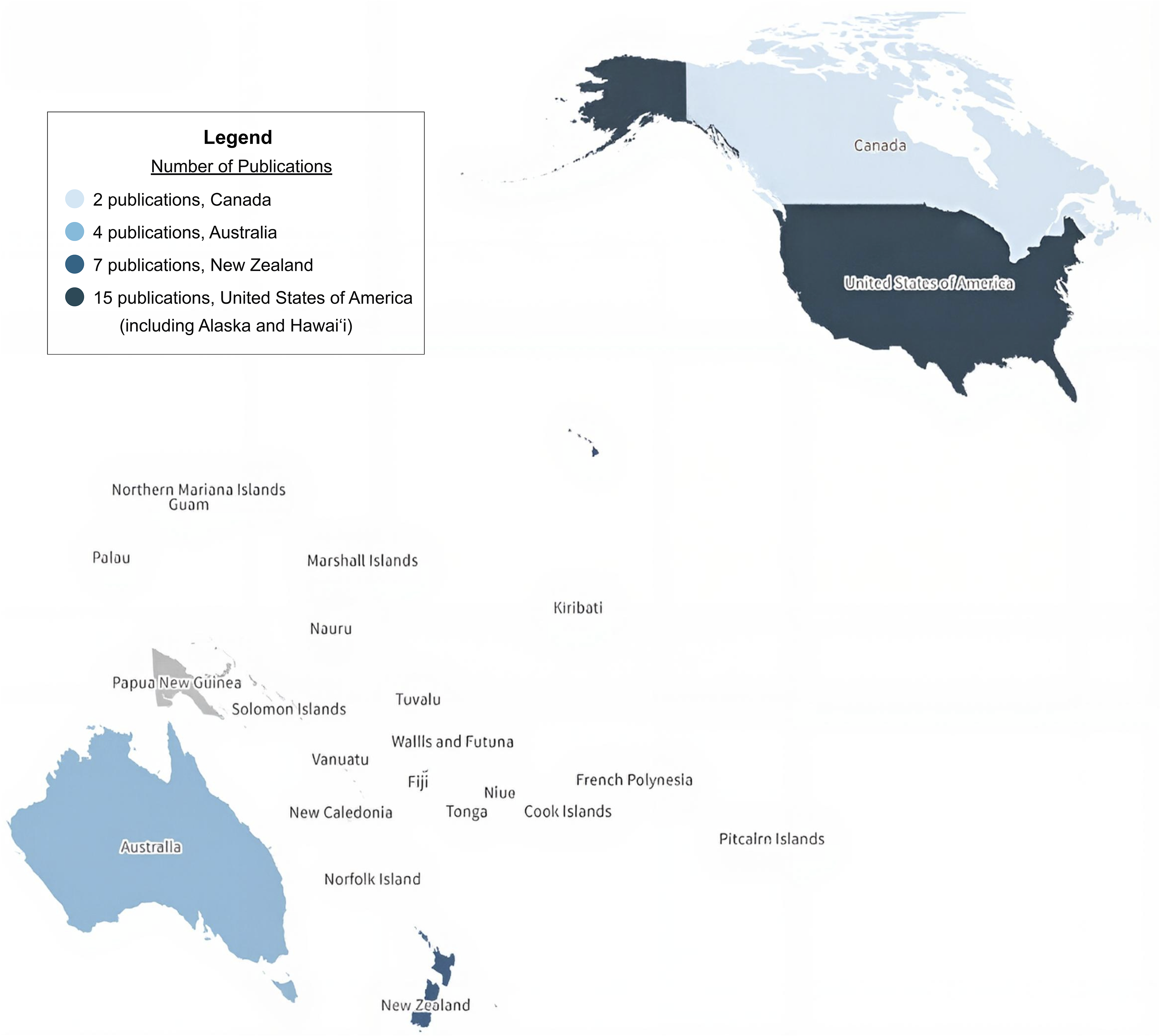
Geographic distribution of ACP publications by country.
Included Experimental Studies (n = 1)
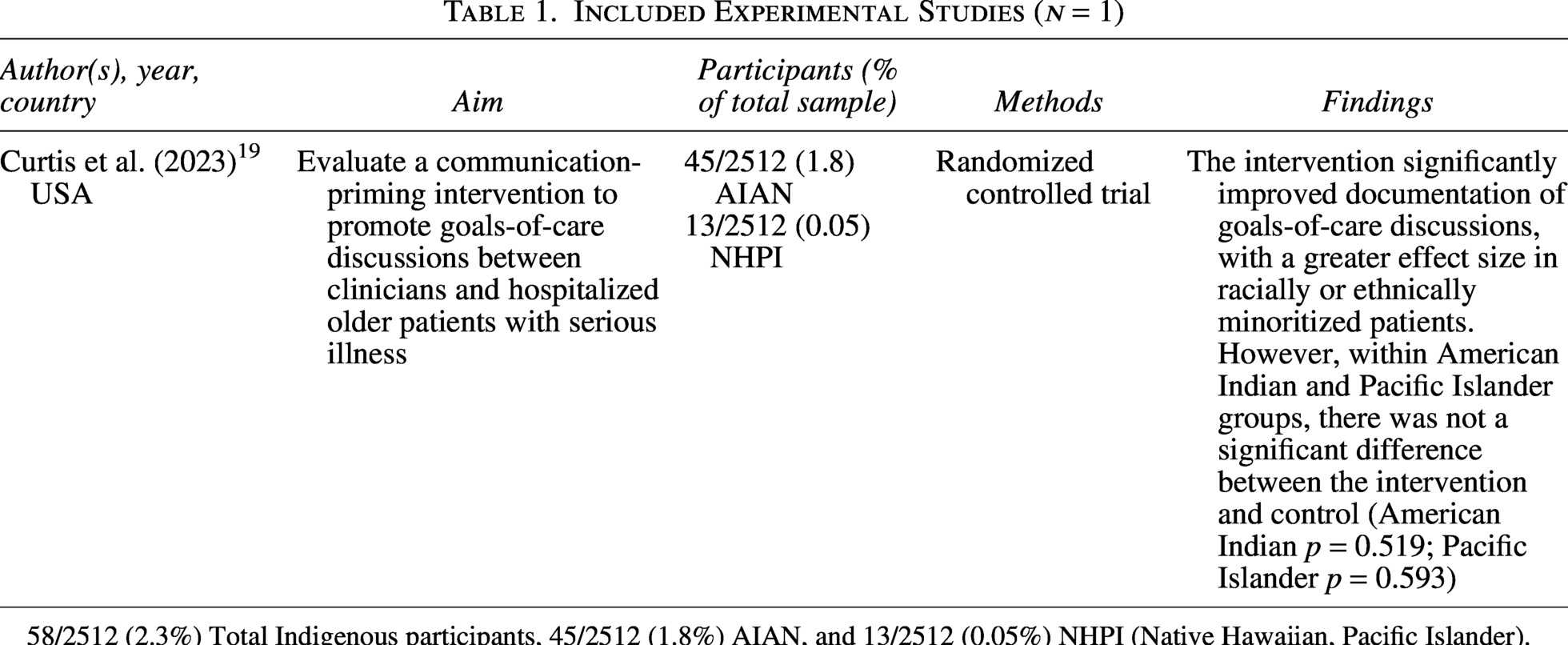
58/2512 (2.3%) Total Indigenous participants, 45/2512 (1.8%) AIAN, and 13/2512 (0.05%) NHPI (Native Hawaiian, Pacific Islander).
Included Observational Studies (n = 7)
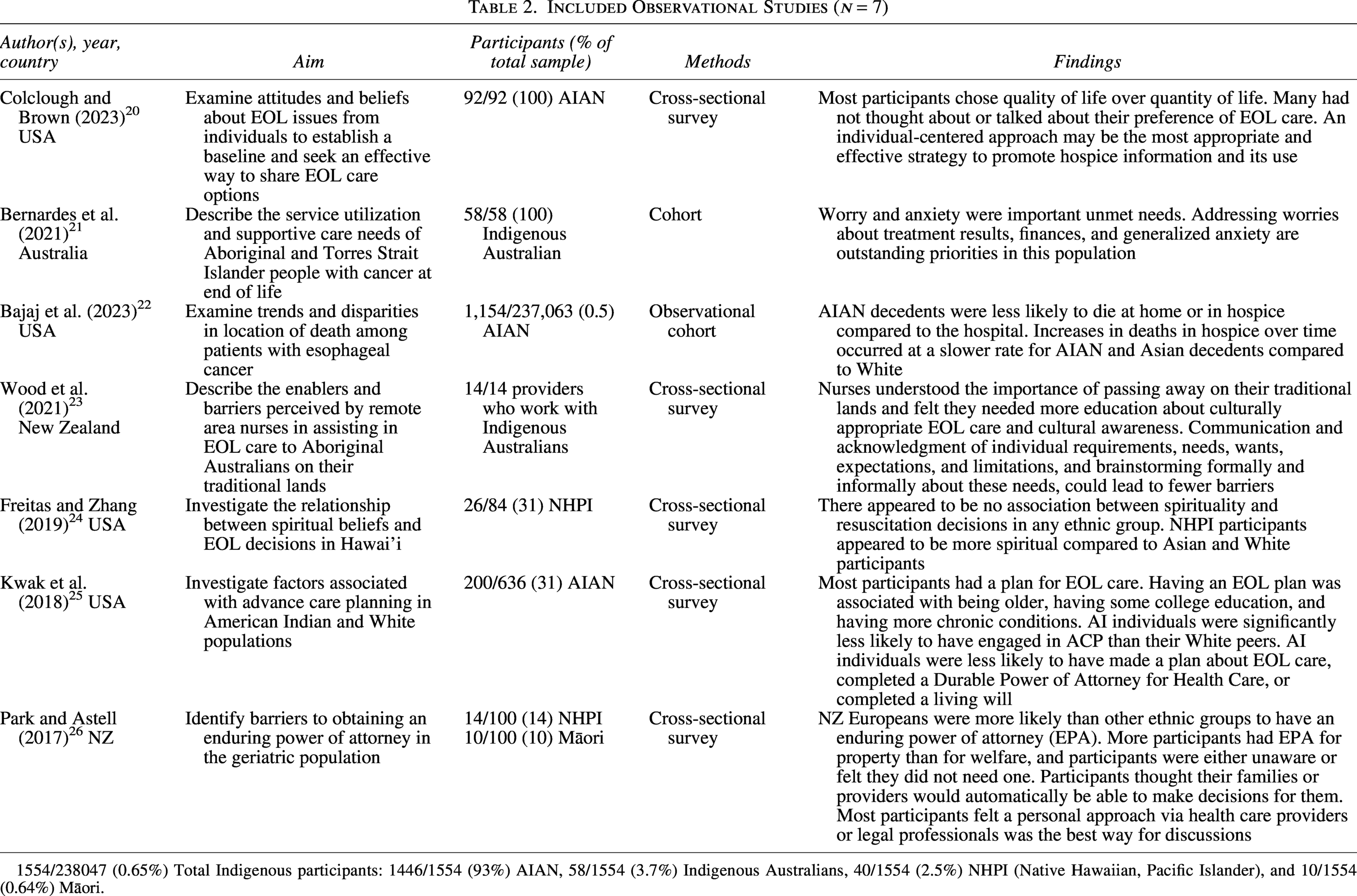
1554/238047 (0.65%) Total Indigenous participants: 1446/1554 (93%) AIAN, 58/1554 (3.7%) Indigenous Australians, 40/1554 (2.5%) NHPI (Native Hawaiian, Pacific Islander), and 10/1554 (0.64%) Māori.
Included Qualitative Studies (n = 16)
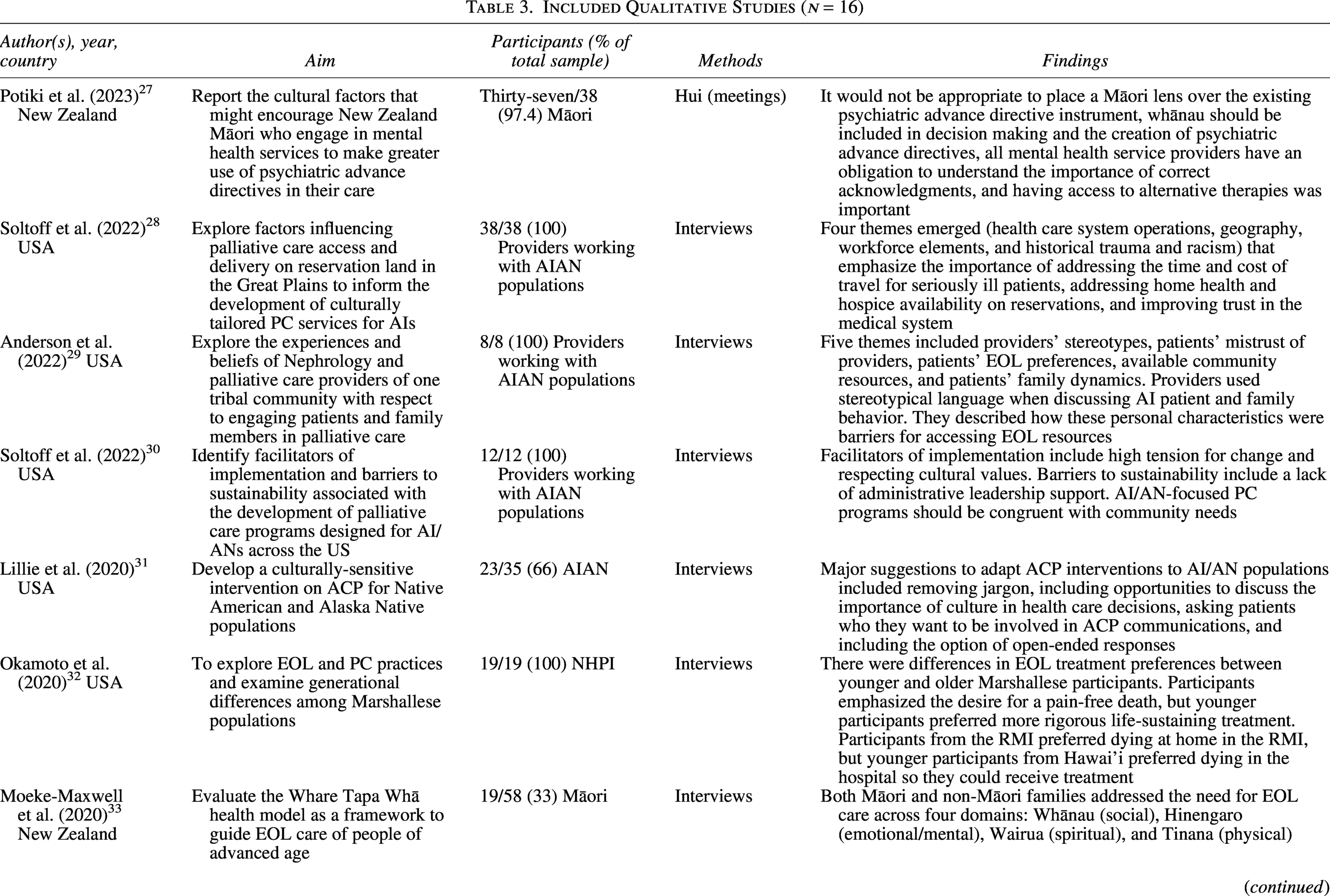
221/431 Total Indigenous participants (51%): 77/221 (35%) Māori, 55/221 AIAN (25%), 46/221 (21%) NHPI (Native Hawaiian, Pacific Islander), and 43/221 (19%) Indigenous Australian, RMI (Republic of the Marshall Islands).
Included Mixed Method Studies (n = 4)
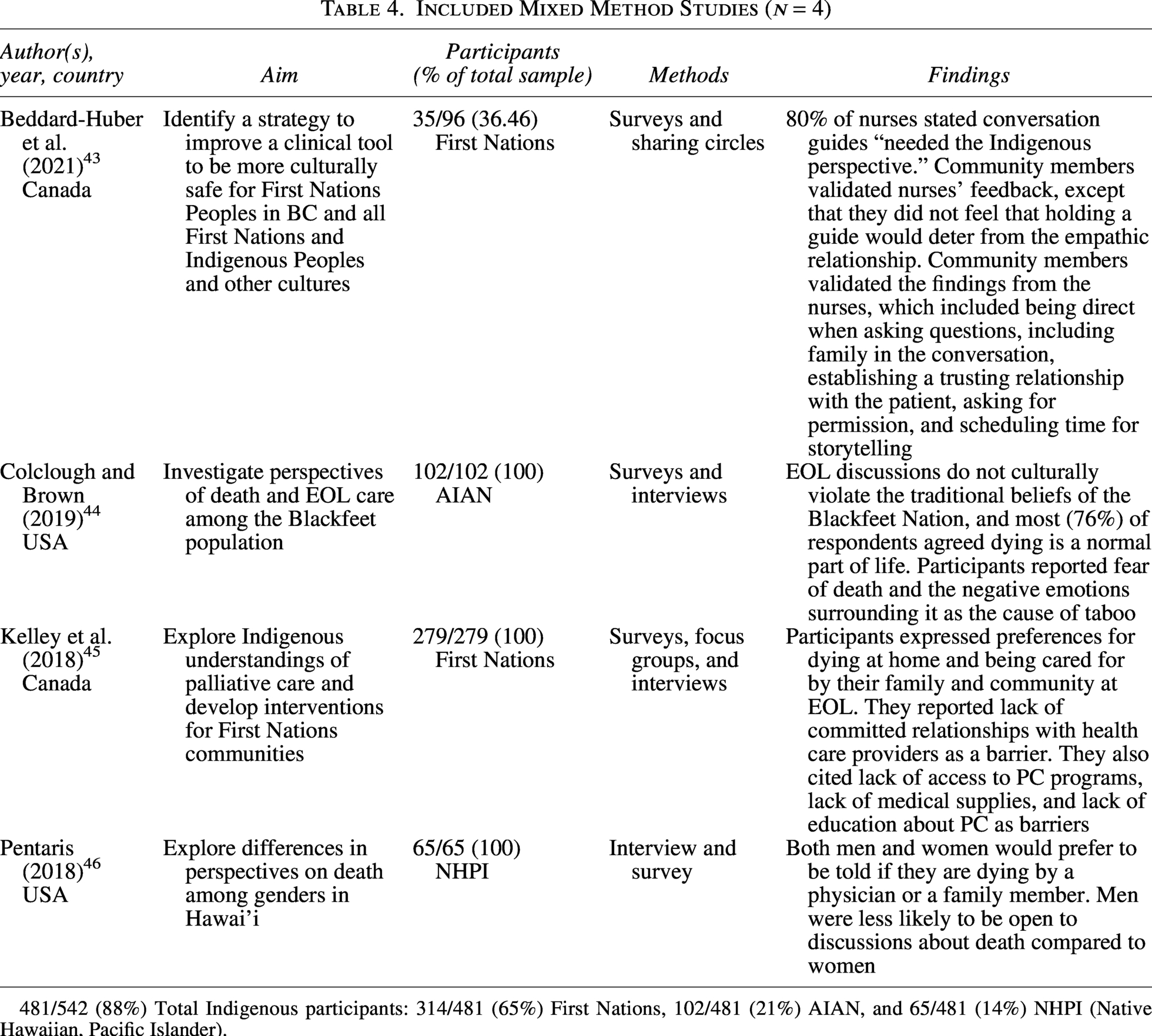
481/542 (88%) Total Indigenous participants: 314/481 (65%) First Nations, 102/481 (21%) AIAN, and 65/481 (14%) NHPI (Native Hawaiian, Pacific Islander).
Based on the evidence gap map, the most frequently reported findings were family support and relationships (n = 20), followed by culturally unsafe services creating hesitancy and mistrust (n = 16), access to ACP resources (n = 16), and lack of funding and resources for EOL programs (n = 15) (Fig. 3). By country, the United States reported family support and relationships the most, New Zealand reported culturally unsafe services create hesitancy and mistrust the most, and Australia reported location/place of death being highly valued, family support and relationships, and lack of funding for programs the most. It was difficult to determine which findings were most frequent in Canada since only two studies were included.
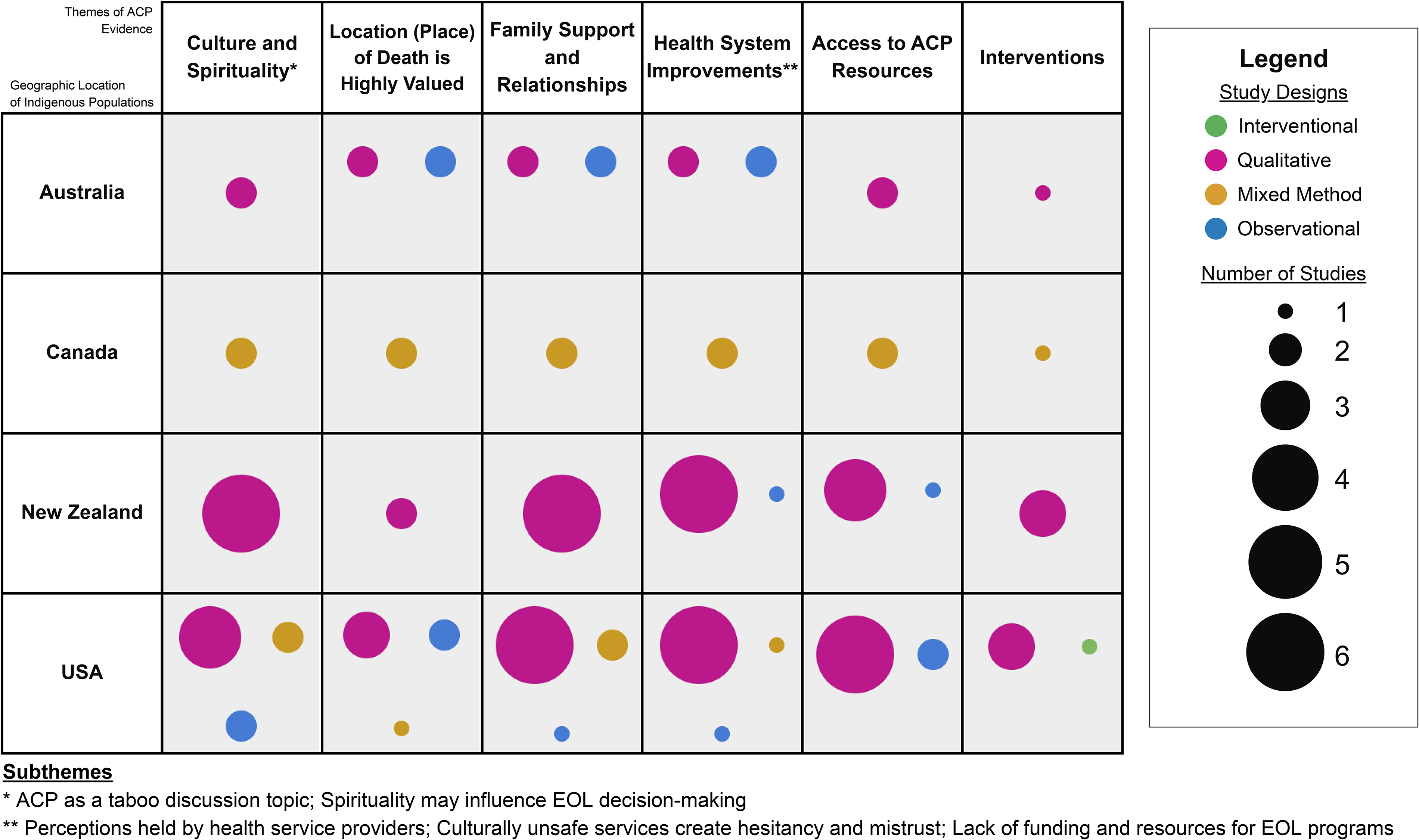
Thematic gap map of ACP in Indigenous populations of North America and Oceania.
Prevalence of ACP completion
Indigenous populations had less frequent ACP completion than other ethnic groups, as reported in four studies. In a cross-sectional survey, American Indians were significantly less likely to have engaged in ACP compared to Whites. 31 In another survey, in New Zealand’s Counties Manukau Health, Europeans were more likely to have an enduring power of attorney than other ethnic groups (including Māori and other Pacific Islanders). 32 Among Blackfoot Indians in the United States, most (78%) did not have an advance directive in place and only about one-third thought of their EOL medical care preferences or had talked to their family about these preferences, according to a cross-sectional survey. 26 In a cohort study in Australia, only a small portion of Indigenous Australians with cancer received palliative care, despite most of them dying in a hospital. 27
Challenges to ACP completion
Culture and Spirituality
ACP as a taboo discussion topic
Twelve articles described ACP and discussions about death and dying as taboo, which was identified as a barrier in engaging with these discussions in the health care setting. These articles were predominantly qualitative, with interviews being the most common method. This theme was described by Indigenous participants from all four countries, as well as health care providers who worked with American Indian patients. This theme often came up in how participants described their communication with health care providers. For example, Frey et al. described a “shyness” driven by cultural norms in Māori and other Pacific Islander patients that prevents them from asking for help, as well as being reluctant to speak to providers from different cultural backgrounds. 47
Multiple reasons were cited for this taboo. While Blackfoot peoples in the United States had individual differences, Colclough and Brown reported that the majority pointed out a fear of death. 48 Negative life events like sickness and death can break the living spirit, so talking about death and EOL is difficult due to loss and its associated emotions. 48 Other reasons were not wanting to “give up” on their elders (e.g., providers mentioned Polynesian families prefer full code because they feel an obligation to do everything possible to care for their elders 46 ) and not “jinxing” death (e.g., Native Hawaiians suggested their will to live can slow down their death, and they can sense that their death is imminent). 49
However, EOL discussions were not always taboo topics. A study of Blackfoot Elders in the United States found most respondents strongly agreed that dying is a normal part of life, and discussions about care among families were not against tribal tradition. These discussions were necessary to provide care and combat feelings of powerlessness and should take place in a culturally comfortable environment. 48 Ojibwe Elders in the United States had a similar perspective, with almost all being open to discussions about death. 40 A lack of formal planning did not necessarily indicate a resistance to ACP. 40 EOL care discussions are also becoming more normalized in Indigenous communities. Sinclair et al. reported that discussions about death among Indigenous Australians were taboo in the past, yet funeral and burial planning discussions have led to more overall acceptance. 44
Spirituality may influence EOL decision making
Eleven articles discussed spirituality as playing a significant role in EOL decisions. Indigenous participants from all four countries emphasized the central role of spirituality in EOL care, influencing cultural practices, family experiences, and ACP decisions. As an example, Dembinsky et al. recognized the importance of specific ceremonies and practices surrounding death and acknowledged the cycle of life–death–life as a continuum in the belief system of Indigenous Australians. 45 In Māori communities, Moeke-Maxwell et al. discuss the importance of the Wairua (spiritual) domain, which includes the delivery of cultural and spiritual health care and the ability of patients to conduct spiritual customs at EOL. 39 Attending to these spiritual needs brought comfort to their families. 39 This is also true for constructing informational materials such as brochures, as described by Simpson et al. 42 Participants highly valued spiritual imagery and recognized the importance of spirituality in EOL discussions. 42
The role of spirituality also has some impact on ACP decisions. Dennis and Washington found that leaving decisions up to Creator and trusting that things will “work out” results in people finding little need for making formal plans. 40 There was also a belief that the Creator would show signs that death is imminent, so people would know when they would die rather than viewing death as a sudden or unexpected event. 40 However, participants acknowledged the importance of planning for after-death to ensure implementation of their cultural and spiritual wishes. 40 In surveys measuring the spirituality of Native Hawaiians, they were found to have higher levels of spiritual and religious beliefs than Caucasian participants; however, Freitas and Zhang noted there was no association between spirituality and resuscitation decisions. 30
Location (Place) of Death Is Highly Valued
The location (place) of dying was cited by 14 articles as being an important factor in EOL planning (Fig. 3). Across these studies, preferences around place of death were closely tied to cultural values, family presence, and connection to home and land. According to Dembinsky et al., a major concern among Yamatji is not being able to die “in country.” 45 This is also discussed by Sinclair et al., where discussions revealed a desire to be buried in their home country, surrounded by family. 44
Multiple articles also reported wishes to die at home, surrounded by family. Kelley et al. reported that most (87%) respondents preferred to receive palliative care (PC) at home in their First Nations communities. 50 Pentaris discussed how all Native Hawaiian participants desired a natural death at home. 49 Māori and Polynesian patients were recognized by providers for having a strong need for having a large space to be surrounded by family.39,51 Ojibwe elders in a United States study by Dennis and Washington desired a peaceful death at home and expressed that some medical interventions were not compatible with a peaceful death. 40 Blackfoot Indians in the United States also desired a peaceful and painless death at home, but they wanted some type of hospital treatment when dying. 26 Interestingly, Okamoto et al. found that among Marshallese participants, participants (both from the U.S. and the Republic of the Marshall Islands) were more concerned with the burial of the body being at home than with the location where the death occurred. 38
Family Support and Relationships
The role of family and the community is highly valued in EOL care, and decision making was a recurring theme in 20 articles, making it the most frequently mentioned theme overall (Fig. 3). These articles consistently highlighted a shared emphasis on collective care, family presence, and relational decision making at the EOL. Although cultural and spiritual beliefs varied among Indigenous peoples, there was still a shared importance of caring for dying community members. 50 In one study, Pentaris reported that Native Hawaiians appeared to experience death and grieving collectively. 49 Moeke-Maxwell et al. found that family involvement in health care planning initiatives, decisions about physical care, and having the space to gather near their loved ones satisfied the Tinana domain in the Te Whare Tapa Whā model of well-being, making it an essential component to providing care. 39 All Māori participants in Potiki et al. emphasized that involving families in the decision-making process is essential, describing the concepts of whakawhanaungatanga (establishing and building relationships) and manaakitanga (respect, generosity, and care for others). 33 The importance of family involvement was also observed by health care providers who work with Indigenous patients. For example, in Canada, nurses described holding a conversation without family present as culturally unsafe in First Nations communities. 52
High family involvement in EOL care among Indigenous peoples may result in a decreased need for ACP. Sinclair et al. reported that Indigenous Australians have a sense of trust in their family to make medical decisions on their behalf, so there was no need for formal documentation. 44 However, Sinclair et al. also found that Indigenous Australians with complicated family relationships prefer more formal planning in their care. 44 Similarly, Goff et al. described how differing types of patient-family/friend interactions could potentially affect ACP discussions. 43
With the high involvement of families in EOL care, conflicts among family members over goals of care can create hesitancy to engage with planning. Frey et al. reported that patients withhold wishes from their families to preserve harmony. 46 Instead, they defer to the judgment of health care providers. 46 Isaacson reported that the eldest child is typically designated as the primary spokesperson for the elder, but may not always represent their true wishes. 41 Participants in this study also recognized that changing the designated spokesperson through formal planning can ensure wishes are followed through. 41
Health System Improvements
Perceptions held by health service providers
Perceptions of Indigenous people by health care providers create a barrier to EOL care engagement, as reported by 10 articles (Fig. 3). These perceptions often reflect stereotypes and assumptions that negatively shape provider–patient interactions and limit engagement in EOL care. Anderson et al. reported the use of stereotypical language to describe American Indian attitudes toward PC, such as fatalistic and nihilistic. 35 Some attributed the lack of engagement in PC to the patient’s shortcomings, like not wanting help, being noncompliant, difficult to reach, or being overall uninterested. 35 They also describe families as being disjointed and high emotion, making their care challenging. 35 Some had the misperception that American Indian patients have access to many health resources since their tribe pays for everything. 35 These harmful perceptions can be a barrier to information provision and lead to providers playing a “gatekeeper role” in planning engagement. 47
Relationships between patients, their families, and staff were repeatedly identified in 10 articles. Beddard-Huber et al., Kelley et al., and Sinclair et al. discussed the importance of establishing a relationship between the provider and patient before beginning the conversation due to the difficulty of EOL discussions.44,50,52 According to Moeke-Maxwell et al., relationships between health care professionals and patients fall into the domains of whānau (social well-being) and hinengaro (mental and emotional well-being) in the Te Whare Tapa Whā model of well-being. 39 Māori participants valued connections with staff, providers taking an interest and having empathy, and shared ties with the local community. 39 These values were also shared by Māori participants in another study, who explained that whakawhanaungatanga (establishing and building relationships) helps to address mistrust and willingness to ask for help. 47 Without these relationships, patients are less likely to discuss their goals of care with providers. In interviews conducted at a dialysis center by Goff et al., patients and their caregivers desired more connection with their nephrologist and staff, and a lack of rapport with staff is likely to impact their ACP decisions. 43
Culturally unsafe services create hesitancy and mistrust
Incompatibility between Western health care systems and Indigenous EOL practices may create barriers to care, as described in 16 articles. These challenges often arise when Western health care practices fail to reflect Indigenous cultural values, histories, and lived experiences. Dembinsky et al. describe how Australian hospitals did not accommodate Yamatji culture at the EOL. 45 For example, physical limitations of hospital space prevented families from gathering, behaviors such as crying, wailing, or not eating were frowned upon by providers, and there was a lack of privacy for passing on sacred information, which is an important practice at EOL. 45
Racism, medical mistrust, and generational trauma in Indigenous patients play a role in pursuing health care. Mistrust of health care due to historical trauma in American Indian patients was found to negatively impact the ability to build relationships with providers and hold effective discussions. 34 This mistrust was further reinforced by ongoing poor continuity of care and racism. 34 Some health care providers also acknowledged the negative impacts of history and the lack of cultural sensitivity education on providing EOL care to American Indian patients. 35 Perceived power differentials between doctors and patients were also cited as a potential threat to trust in American Indian patients. 43
Provision of information may not be culturally appropriate. For example, when assessing the ability of PC brochures to meet Māori cultural needs, participants pointed out a lack of local landscapes, a lack of Māori people, a lack of younger generations, a lack of understanding of cultural values by brochure authors, and images that conflicted with the values being expressed in the text. 42 It was also recognized that it is not sufficient to simply place an Indigenous lens over a non-Indigenous practice. In examining a psychiatric advance directive instrument, Potiki et al. reported that participants acknowledged the instrument might be useful, but simply putting a Māori lens over it without a deeper understanding would lack the cultural considerations that would make it effective. 33 As one participant explained, “It’s a good concept, but why do we still have to justify ourselves being Māori to a Pākehā system?” 33
Lack of funding and resources for EOL programs
Fifteen of the included articles frequently mentioned a lack of funding and resources in PC, hospice, and other EOL areas of care. These studies consistently pointed to systemic and structural constraints that limit access to timely and adequate EOL care for Indigenous populations. Challenges such as resource gaps, staffing shortages, a lack of services, and a lack of support for families make it difficult to provide quality care at EOL.34,35,50 These challenges are pronounced in rural areas. Soltoff et al. noted issues with the availability of hospice and home health services for patients living on reservations. 26 Three other studies also described similar challenges, with travel issues like transportation, money, and gas being significant challenges.29,34,41,45 Three studies specifically described challenges with EOL care with the Indian Health Service.34,35,41 Kelley et al. paint a similar picture for health care systems in First Nations communities, 50 and Potiki et al. describe this issue in Māori communities as well, with systemic shortcomings and a lack of Māori leadership being the cause of fragmented services. 33
Financial concerns of patients also pose a barrier to pursuing EOL care and planning. Health care providers noted that limited financial resources create a reluctance to engage in PC. 35 In a survey by Colclough and Brown, more than half (57%) of participants expressed an interest in receiving hospice care, but many (42%) felt they could not afford it. 26 While not directly related to ACP, financial burdens of the funeral and burial process were also a cause of tension in EOL planning, further contributing to a reluctance to have discussions. 44
Access to ACP Resources
Limited understanding of the services available at EOL among patients was reported as a barrier in 16 articles (Fig. 3). Participants often had a limited understanding of PC versus hospice, a limited understanding of what services were available to them, and an unawareness of how these practices can be adjusted to meet cultural and spiritual needs.35,45,47,51 Multiple studies reported a general openness to discussions about ACP, but participants did not pursue it because they were unaware or had not previously given it much thought.31,40,43,44,50
Health literacy was reported to be a barrier to accessing information about EOL planning and care in five articles. Together, these articles suggest that limited awareness, health literacy challenges, and language barriers restrict engagement with ACP. In the PC brochures presented in a study by Simpson et al., Māori participants did not appreciate the use of jargon and wordy sentences. 34 This was shared by participants in Beddard-Huber et al., where both nurses and community members identified wording as an issue in interventions, and more direct, plain language was needed. 41
Language barriers were also a significant challenge in providing care in seven articles. The translation and interpretation of discussions were barriers to holding conversations about ACP for both providers and patients.32,35,46,47 There was also a reported reluctance to use interpreters for discussing death, and the availability of interpreters was of concern.41,47
Interventions
Several studies explored strategies aimed at improving engagement in end-of-life planning, focusing on both provider-facing tools and community-based approaches. These interventions were designed to support more effective communication, documentation, and access to information.
Conversation guides for health care providers were explored as a potential method for improving documentation in two articles. In a randomized controlled trial evaluating a communication-priming intervention in the United States, the intervention led to a significant increase in the documentation of goals of care discussions, with greater effects seen among patients of ethnic minority populations. 25 However, no significant differences were found between intervention and control groups within American Indian or Pacific Islander participant groups (American Indian p = 0.519, Pacific Islander p = 0.593). 25 In a study evaluating the effectiveness of the Serious Illness Conversation Guide in First Nations and Indigenous Peoples in British Columbia, some nurses felt that holding a conversation guide might come off as impersonal and disrespectful to Indigenous patients, but community members did not feel it would deter them from maintaining an empathetic relationship. 52 Their suggestions for improving this tool included being direct with asking questions, asking permission before beginning discussions, and adjusting terminology following the patient’s health literacy. 52
To improve the accessibility of information about planning, outreach events were recommended to engage with the community in seven articles. Participants in the study by Sinclair et al. appreciated being able to receive information about ACP from a person they are familiar with in a comfortable and relaxed environment, like a community event. 44 Although face-to-face communication is preferred by most, it may not always be possible, so brochures and videos may suffice as an alternative. 42 Technology was also suggested as a way to reach younger generations. 44
Discussion
This scoping review synthesizes current knowledge on ACP in populations Indigenous to North America and Oceania. Studies incorporated perspectives of patients, their families, and providers from the United States, Canada, New Zealand, and Australia. This topic was explored more frequently in the United States, which had more articles compared to New Zealand, Australia, and Canada. We found a paucity of EOL research involving Indigenous groups in Canada, with only two articles meeting the inclusion criteria. The included articles were diverse in study design but were predominantly qualitative. There is a need for more intervention designs or experimental research about ACP and for evaluating potential intervention programs within Indigenous communities.
Although Indigenous communities are known to be diverse, the literature review identified common needs and preferences. Our findings suggest Indigenous peoples have specific EOL preferences and are generally open to discussions about ACP, but there needs to be systemic changes for ACP interventions to be developed and implemented widely. Improving cultural competence in EOL care is one of the biggest areas of improvement discussed in the included articles. One proposed method is increased training of providers on how to provide culturally competent care. Education on topics such as the impact of the cultural history of an Indigenous population, cultural awareness in EOL care, and more training in EOL care overall were mentioned as areas of improvement.29,34,41,50 Translating resources and documents and connecting them with cultural values was suggested as a way of addressing concerns about cultural safety in potential interventions. According to Potiki et al., providers must understand and respect the language, especially with people’s names. 33 Isaacson also emphasized the need for more interpreters and for workers within the Indian Health Service to learn the language to provide effective care to elders. 41 Simpson et al. found that community members endorsed the use of te reo, Māori language, and Māori images in symbols in PC brochures to connect with cultural identity needs. 42 Formal planning has the potential to be a helpful tool to ensure wishes are carried out, yet engagement continues to be low. There was also a call for providing culturally competent care by including family in the process, interpreting documents, and integrating the community in developing interventions for improving engagement. It is also not enough to put an Indigenous graphic image over a non-Indigenous tool; it needs to be redefined from within the community so that it can address and meet their specific needs.
Despite growing attention to EOL care and ACP among Indigenous populations, several gaps remain. Most studies are qualitative with small samples, and there is a lack of larger studies with appropriate representation to ensure that thematic saturation has been appropriately established. In addition, existing studies are cross-sectional glimpses at the underlying issues that intersect with EOL care. Longitudinal research studies have the potential to identify and differentiate between phenomena such as temporal trends, demographic cohort effects, or the influence of community-based and/or health system initiatives to provide more generalizable insights. 53 Many Indigenous communities, particularly those in rural or underrepresented regions, also have limited representation in the literature.53,54 Finally, there is insufficient evaluation of culturally adapted health systems or community-based interventions, including conversation guides, educational materials, community-based outreach, or community health worker-facilitated programs to improve engagement in ACP.37,53–56
Limitations
This review offers an Indigenous perspective on EOL planning; however, there are several limitations to consider. These populations are underrepresented in research involving ACP, so the scope of this review is limited to what has been published. There are also a few studies that aggregate data (e.g., grouped into API or “other”), which makes it difficult to generalize the findings of each article to these populations.
This review also incorporates multiple Indigenous populations from multiple countries. Although they share similar histories of colonization and marginalization, each group has its own unique experiences. Not all beliefs about death are shared between communities, and even individuals within communities have conflicting beliefs. Each country has its laws and policies regarding ACP and EOL planning, as well as its systems for addressing the health of its Indigenous populations. Each process has its respective differences, but incorporating multiple processes will help to paint a larger picture of Indigenous experiences and existing barriers to the EOL process.
Conclusion
Based on the citations identified in this scoping review, there are several influences in ACP discussions and planning for the EOL in Indigenous populations. These include the role of culture and spirituality, family support and relationships, health care facilitators, and access to ACP resources. ACP interventions that recognize factors identified as important by patients, family members, and health care providers may have the potential to increase ACP documentation and ultimately improve EOL care and experiences among Indigenous populations.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The following funded grants was received for this article: National Institutes of Health (NIH), The National Institute of Nursing Research (NINR); 5R01NR018400.
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.