
Abstract
In the context of a globally aging society, the concept of a compassionate community—which links societal frameworks with palliative care—has gained increasing attention. We posited that compassionate community initiatives should be perceived as sustainable efforts that extend from healthy stages of life. This study is a scoping review designed to define and elucidate how compassionate communities are utilized and practiced IN the health care domain. A systematic search of Medline, the Cumulative Index to Nursing and Allied Health Literature, Cochrane, and PsycINFO was conducted using the keyword “Compassionate Community.” Articles were limited to those in English and published between 2015 and 2025. The Preferred Reporting Items for Systematic Reviews and Meta-analyses extension for scoping reviews guided data extraction and synthesis. A total of 27 articles were included. From these 27 articles, the concept of compassionate community in the health care domain was redefined. Additionally, eight functional aspects of a compassionate community were identified: Supporting, Connecting, Educating, Empowering, Empathizing, Cultivating, Surveying, and Lobbying. In this study, we restructured the concept of a compassionate community in the health care domain and categorized specific initiatives into eight functional aspects. Although the notion of compassionate community as an initiative that integrates society and palliative care aligns with previous research, this study clarified the specific activities required from a more practical approach. The results of our study may provide valuable insights for future research aimed at utilizing compassionate communities as a strategy for primary health care practice.
Keywords
Introduction
Citizens living with life-threatening illnesses, aging, grief, or bereavement, as well as those providing care at home to such individuals, are part of our communities. A compassionate community refers to a local community organized to assist and support all such citizens. 1 Kellehear, who first proposed this concept, identified key characteristics of compassionate cities, including the integration of compassion into local health policies, attention to vulnerable populations, respect for cultural diversity, access to supportive and palliative care services, and recognition of community loss and social inequities. 1 Recently, there has been a growing interest in Compassionate Communities, particularly in Europe and North America, with various regions undertaking initiatives.2,3 In these areas, Compassionate Communities are regarded as a new integrated care model that connects the public health approach with palliative and end-of-life care.
Recent reviews suggest that interventions by Compassionate Communities transform social and cultural attitudes towards death, dying, and bereavement. Compassionate Communities aim to enhance social capital through fruitful partnerships between public institutions, private enterprises, and the third sector, ultimately promoting volunteer-led activities to provide better care for individuals in the final stages of life. 4 Integrating societal frameworks with palliative care, as envisioned through Compassionate Communities, is expected to become an increasingly important concept.
Because they support those facing death and loss, compassionate communities have historically focused on palliative and end-of-life care. 5 However, in a globally aging society, compassionate communities should not be limited to initiatives near the end of life. They can also be understood as sustainable efforts that begin while people are still healthy and help them build relationships and connections within the community before crises occur. Although compassionate community initiatives have been implemented in various regions, their scope and practices vary widely. The concept is open to multiple interpretations. Therefore, to advance its application in health care, it is necessary to clarify compassionate communities as a more concrete practice concept. Previous studies have reported inconsistencies in the definition and implementation of compassionate communities. However, their concrete application within the health care domain has not been systematically understood. Therefore, this scoping review aimed to define compassionate communities in the health care domain and to elucidate the functions they serve in practice.
Methods
Compassionate communities are a concept that has not been clearly defined; therefore, we conducted a scoping review to clarify them.
Scoping reviews are suitable when the purpose is to identify knowledge gaps, scope a body of literature, and clarify concepts. 6 We used Arksey and O’Malley’s widely used methodological framework 7 for scoping reviews. We also followed the Joanna Briggs Institute Reviewer’s Manual, a standard guideline for scoping reviews. 8 Arksey and O’Malley’s framework includes five steps: identifying the research question; identifying relevant studies; study selection; charting the data; and collating, summarizing, and reporting the results.
Identifying the research question
Our purpose was to explore previous findings about compassionate communities in the health care domain and clarify who is being targeted and what kind of interventions are being used. Therefore, our main research question was: How are compassionate communities in the health care domain defined and practiced?
Identifying relevant studies
Data sources
The following databases were used for the literature search: Medline (PubMed), Cumulative Index to Nursing and Allied Health Literature, Cochrane, and PsycINFO. The keyword used was “Compassionate Community.”
Inclusion and exclusion criteria
The inclusion criteria included: the title or abstract included the words “Compassionate Community” or “Compassionate City,” the text defined the concept of compassionate community, and the text described specific applications or initiatives based on the concept of compassionate community.
The exclusion criteria included: articles not written in English, COVID-19-related literature, education-related literature targeting students, and articles published before 2014. Therefore, the study was limited to the period from 2015 to 2025 (with the final search date being December 15, 2025) because the standard criterion for a systematic review is based on studies published in the past 10 years before the review. These screening steps were carried out independently by the first and second authors. If any of their interpretations varied, the issue was discussed with one or more of the other authors until consensus was reached.
Study selection
After removing duplicates from the searched literature, the following steps were taken to select studies that met the inclusion criteria: initial content evaluation and detailed evaluation.
In initial content evaluation, the titles and abstracts of each article were reviewed, and articles containing the words “Compassionate Community” or “Compassionate City” were selected. In the detailed evaluation, the 162 articles selected in the content evaluation phase were thoroughly read, and those that defined the concept of compassionate community in the text and described specific applications or initiatives based on the concept of compassionate community were selected.
Charting the data
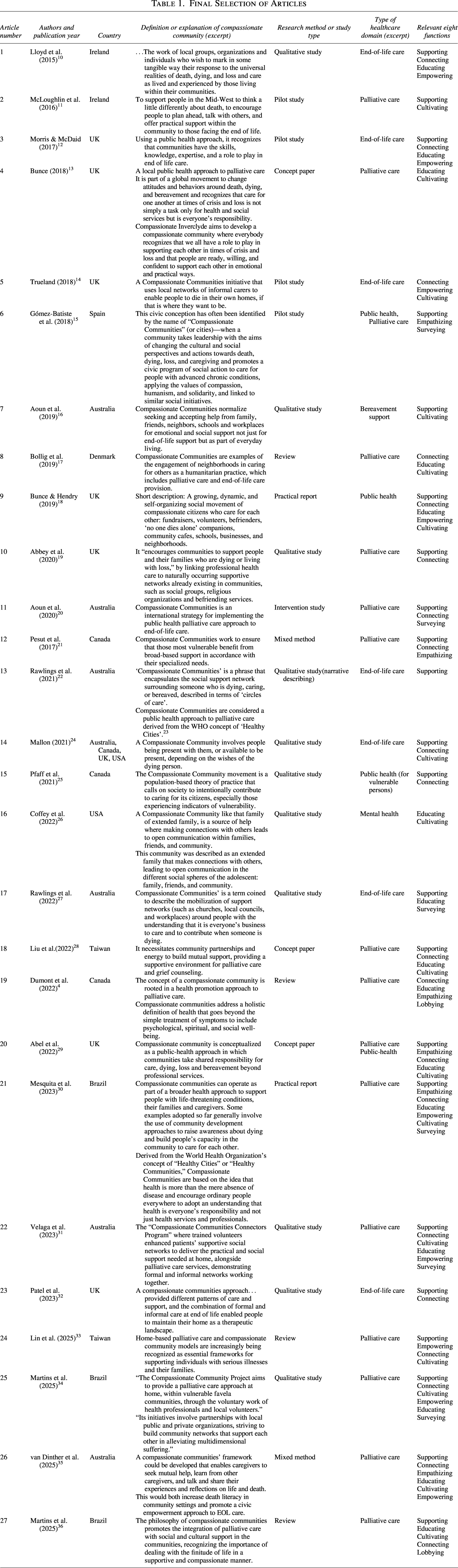
We constructed a study selection flowchart according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for scoping reviews guidelines (Fig. 1). 9 From the text of the final set of articles, we drew a data chart to compare the definitions and explanations of a compassionate community (Table 1). The chart included basic information about the articles, the definition or explanation of a compassionate community, the research method used, and the type of health care domain. The definition or explanation of a compassionate community was extracted from the text of the article. The research method described how the study was carried out. The type of health care domain explained the type of health problem the compassionate community catered to. In addition, the practical functions of compassionate communities in the health care domain identified from the findings of this study were incorporated into the table.
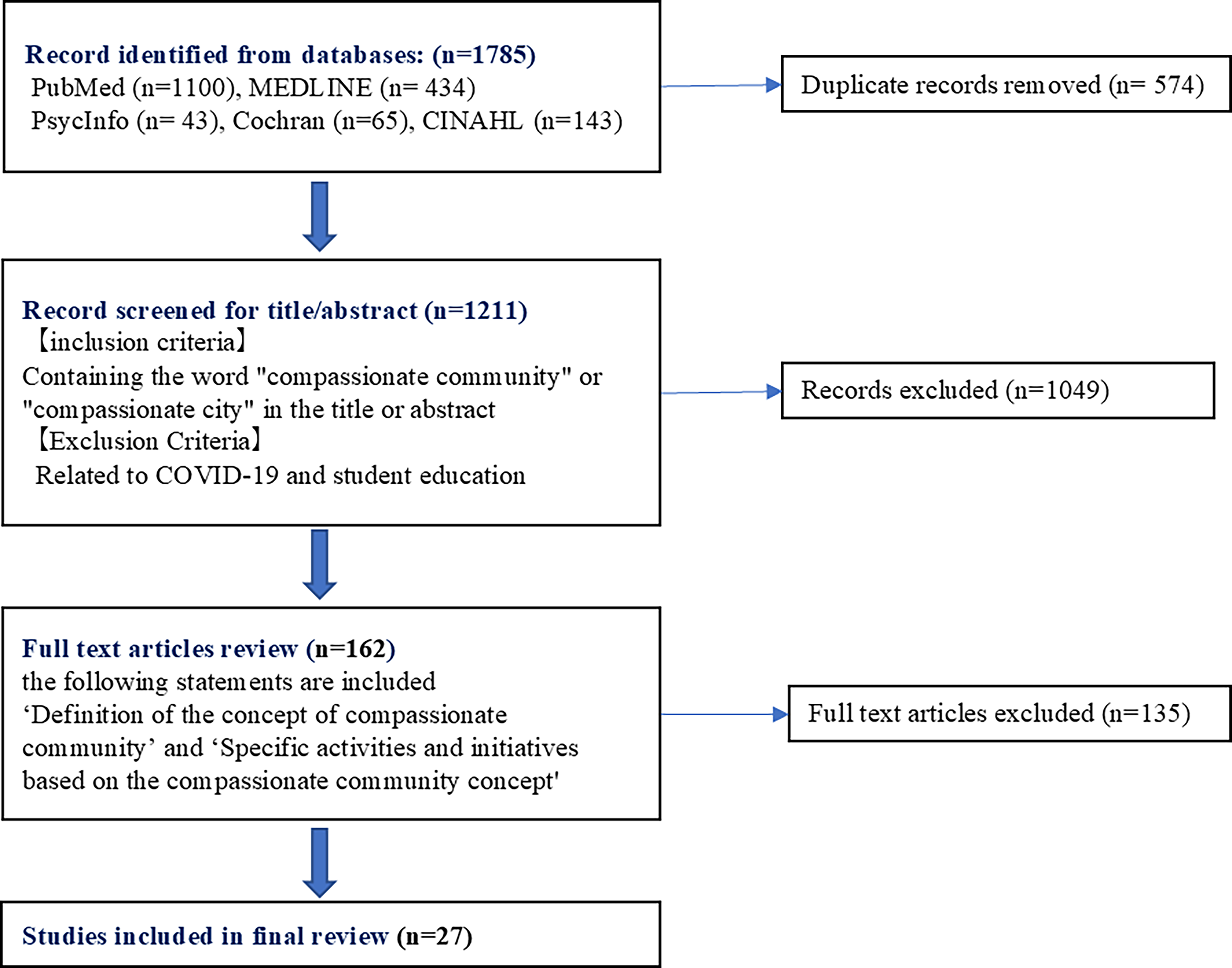
Flowchart of study selection according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Final Selection of Articles
Collating, summarizing, and reporting the results
We subdivided the extracts describing the definition or explanation of a compassionate community into smaller parts by meaning. We collated and categorized them into subthemes and then synthesized them into broader themes.
Results
Figure 1 illustrates the flowchart of study selection. A total of 27 articles met the eligibility criteria. Table 1 presents the final selected articles in chronological order, including the definition or description of compassionate communities and associated data. The included studies were conducted in the United Kingdom (n = 7), Australia (n = 6), Canada (n = 3), Brazil (n = 3), Ireland (n = 2), Taiwan (n = 2), the United States (n = 1), Spain (n = 1), Denmark (n = 1), and multiple countries (n = 1). Regarding study design, the included articles comprised qualitative studies (n = 11), pilot studies (n = 4), reviews (n = 4), a mixed-methods study (n = 2), an intervention study (n = 1), and other types of articles (n = 5).
Based on the descriptions extracted from each article, compassionate community was redefined as follows: In the health care domain, a compassionate community is defined as a local community that supports individuals facing life-threatening illness, aging, grief, bereavement, or caregiving responsibilities. This concept is grounded in the principle that health and well-being are not merely professional obligations but collective communal responsibilities. Within such communities, those experiencing crises, loss, or terminal illness, along with their families, receive emotional and social support from family, friends, neighbors, schools, workplaces, and local organizations as an integral part of everyday life. Furthermore, compassionate communities aim to transform cultural and social attitudes toward death, dying, and care, thereby strengthening community relationships, enhancing local resources, and contributing to the development of practical policies.
In Table 2, the specific initiatives of compassionate communities in the health care domain were categorized based on their similarities. The initiatives of compassionate communities were categorized into the following eight functions: supporting, connecting, educating, empowering, empathizing, cultivating, surveying, and lobbying (Table 2).
Attributes of a Compassionate Community
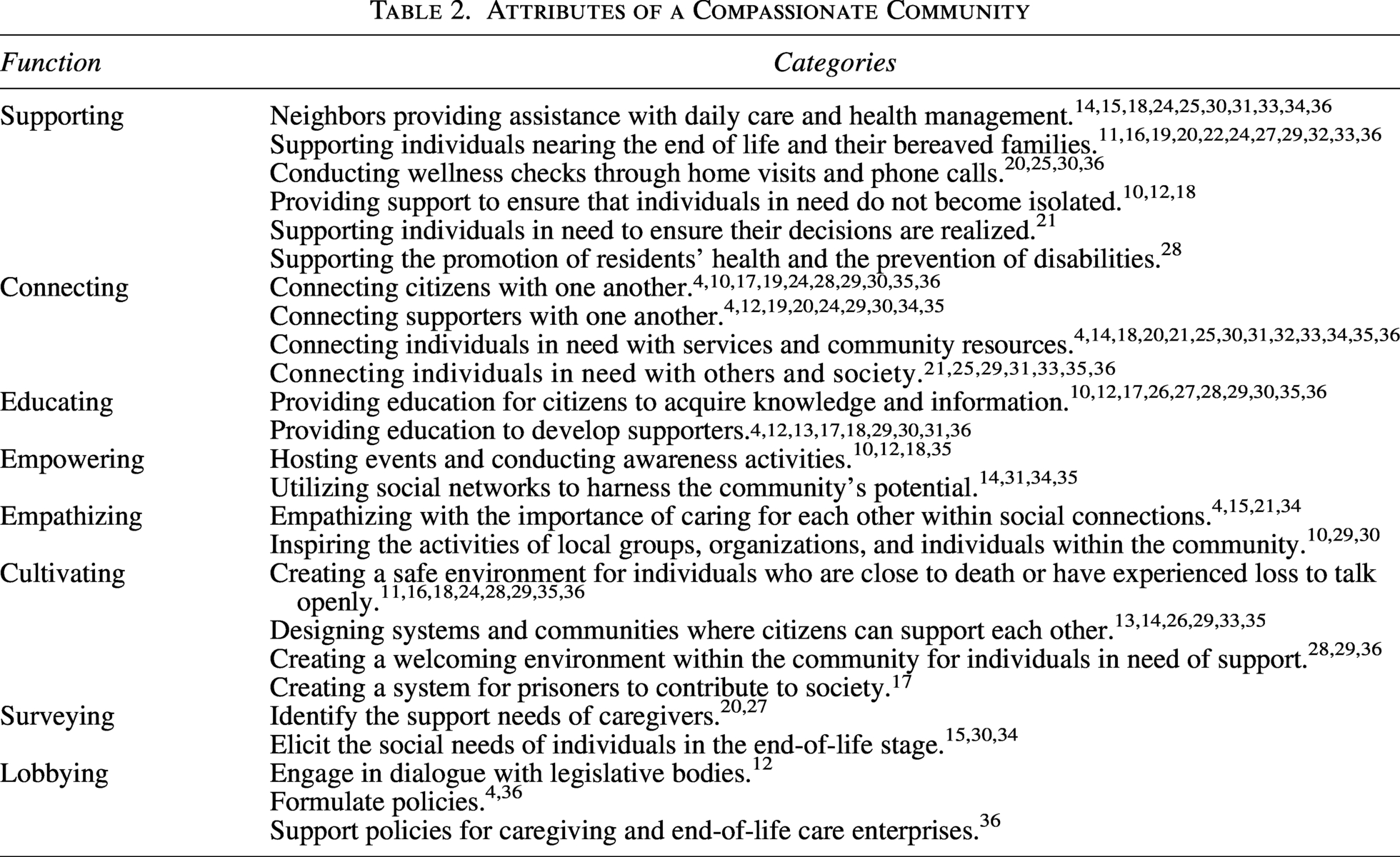
In the “Supporting” category, compassionate communities were characterized by not only professionals supporting those nearing the end of life and their bereaved families but also residents providing daily life support to each other. Specific activities included cleaning, laundry, shopping, pet care, medication management, and wellness checks. In the “Connecting” category, efforts included not only person-to-person connections among supporters and residents, but also linking individuals in need of support with community services, resources, and social networks. The “Educating” category encompassed education for citizens and training for professional supporters. In compassionate communities, education and human resource development were aimed at enabling mutual support among volunteers and local residents, rather than relying solely on professionals for support. The “Empowering” category involved supporting and encouraging participating citizens through events and awareness activities, as well as fostering community capacity by supporting social networks. The “Empathizing” category involved initiatives to enhance the values of compassion and solidarity and foster empathy within the community. In the “Cultivating” category, efforts were made to create environments where residents in need of support could exist safely and to design organizations that enabled mutual support among citizens, thereby enhancing community capabilities. The “Surveying” category included identifying the needs of individuals requiring support and investigating the support needed by caregivers. The “Lobbying” category involved promoting the compassionate community approach through discussions with legislative bodies and policy formulation from a social perspective.
Based on the above findings, we integrated the eight functional aspects of compassionate communities identified in this study (Table 2) to create a conceptual framework for compassionate communities in the health care domain (Fig. 2).

Eight functional aspects of a compassionate community.
Discussion
Definition of compassionate community in the health care domain
Kellehear, who first proposed the concept of compassionate community, outlined nine characteristics that define a compassionate city. 1 These characteristics include local health policies that recognize compassion as an ethical imperative; attention to the needs of older adults, people with life-threatening illnesses, and people living with loss; respect for social and cultural differences; and the inclusion of grief and palliative care services in local government policy and planning. They also include access to supportive experiences, interactions, communication, and palliative care services; reconciliation with Indigenous people and remembrance of other important community losses; consideration of economically disadvantaged groups, including rural and remote populations, Indigenous people, and homeless people; and preservation of the community’s spiritual traditions and storytellers.
The definition of compassionate community derived from the results of our current study aligns with Kelleher’s definition of compassionate city in that it aims to ensure that vulnerable individuals and their families, who face situations of isolation, death, and loss, can connect with society and receive support in circumstances where compassion is needed by the community.
Kelleher’s definition is a holistic concept based on the World Health Organization’s (WHO) definition of a healthy city. 23 Although the overarching concept aligns with the definition in this study, Kelleher’s definition is considered abstract for implementing a compassionate community within local societies. In this study, we identified eight functional aspects of a compassionate community, which we believe indicate specific actions necessary to implement a compassionate community. Hence, this may serve as a useful resource for future compassionate community implementation.
Practice of compassionate community in the health care domain
The practice of compassionate communities in the health care domain was examined based on eight functional aspects.
First steps towards creating a compassionate community
Previous studies have described compassionate community initiatives not as a concept focused solely on end-of-life palliative care, but as a broader concept aimed at meeting the needs of people living with chronic diseases and life-limiting illnesses, caregivers, and bereaved families. 37 The results of this study also indicate that the scope of a compassionate community is not limited to end-of-life events and issues such as life-threatening diseases and bereavement, aligning with previous studies.
In the “educating” aspect of compassionate community, initiatives included encouraging citizens of different generations to learn from each other through empathy and the exchange of life experiences and promoting literacy on death and loss across all age groups and organizations. Additionally, “empathizing” activities involved sharing values and creating empathy through solidarity, enabling community members to work towards a common direction. Building community networks requires involving, empowering, and educating local people to act for their benefit. The accumulation of such practices transforms cultural and social views and behaviors regarding death, dying, and loss, leading individuals of all ages to participate in cultivating communities as local resources from a healthy stage. This serves as a first step for community members to prepare and take concrete actions toward creating a compassionate community.
A compassionate community is created by citizens
Previous studies have shown that compassionate community initiatives have been conducted by health care and social welfare professionals, individuals with experience and expertise in building social networks, and the volunteer sector. 38 Furthermore, leadership in these initiatives often involved health care service institutions and professionals. 4
However, the results of our study suggest that, while “Empowering” citizens to take initiative, efforts were also made to “connect” citizens with one another and resources, thereby “Cultivating” communities that serve as valuable assets to the local society. This indicates that those who provide support in a compassionate community are not limited to professionals. The creation of a compassionate community is a collective responsibility of the community, and it can be argued that the essential element of a compassionate community lies in the active engagement of its members.
Additionally, the “Supporting” activities conducted by residents included everyday life assistance such as meal preparation and cleaning, as well as checking on neighbors. This highlights that compassionate communities involve community members in daily mutual support.
While citizens spend only about 5% of their time receiving care from professionals, they spend 95% of their time with family, friends, and neighbors in their daily lives. 39 Therefore, compassionate community initiatives should move beyond dependence on professional services alone. A community-driven approach that promotes continuous learning and mutual support is essential in local societies.
This approach aligns with the concept of social prescribing advocated by the WHO, which is defined as “a means of connecting patients to a range of nonclinical services in the community to improve their health and well-being.” 40 It emphasizes the creation of a support system where community members mutually support each other, alongside formal health care services.
Thus, these findings suggest that compassionate communities are a valuable strategy for the practice of primary health care.
Implementation of compassionate community
The results of our study revealed that a compassionate community is not solely focused on the end-of-life stage but is a mutual and continuous initiative where local people can connect with society when they need support and utilize community-built resources as needed. Kelleher stated that compassion involves sharing in another’s suffering and forms the foundation of social empathy. 1 This implies that a compassionate community involves fostering a community that learns and supports each other through social interactions, making it a significant strategy as a public health approach.
However, there has been no verification of how a compassionate community impacts the health status and lifestyles of community members. The articles reviewed in this study did not provide evaluations or verifications of ongoing compassionate community initiatives. Dumont reported that most evaluations remain at the individual level rather than assessing community- or group-level changes. 4 Considering the definition of a compassionate community, it is necessary to promote research that evaluates the development and improvement of communities as organizations, rather than focusing solely on individuals.
Additionally, Kelleher emphasized that within compassionate communities, it is essential for community members—not professionals or service providers—to experience a sense of control over their own lives. 41 One method to achieve this is through advance care planning (ACP). ACP should be positioned as a means to support individuals in expressing how they wish to live within their community, enabling them to express their will autonomously and feel a sense of control over themselves. By adopting this approach, community members can collectively share and support the individual’s expressed wishes. The accumulation of such interactions is believed to contribute to the cultivation of a compassionate community, and efforts to implement ACP at the community level can be regarded as a crucial starting point for promoting compassionate communities.
Limitations and Recommendations
This study had a few limitations. First, at the time of the literature search, there were few studies evaluating interventions related to compassionate communities, and the available resources for assessing outcomes were insufficient. For future implementation, it is necessary to evaluate and verify such interventions, particularly focusing on processes and outcomes at the community level rather than at the individual level.
Second, our review revealed a lack of research on compassionate communities, particularly in Asia, where population aging is rapidly progressing. In Japan, a frontrunner in addressing the challenges of a super-aging society, concepts such as the community-based integrated care system and community-based inclusive society exist. However, their relationship to the concept of a compassionate community has not been sufficiently explored. To implement a compassionate community within society, it is essential to identify initiatives that align with this concept and to continue examining their connections with similar frameworks.
Conclusion
This scoping review has restructured the concept of a compassionate community within the health care domain, categorizing specific initiatives into eight functional aspects. The results of our study clearly indicate the necessary actions to realize a compassionate community. These findings may provide valuable insights for future research aimed at applying compassionate communities as a strategy for primary health care practice.
Authors’ Contributions
Conceptualization: Mad.N. and H.N. Methodology: Mad.N. and H.N. Investigation (e.g., literature search and selection): Z.T., A.Y., M.A., and K.C. Data curation (e.g., organizing and managing references): Mad.N., May.N., and A.Y. Writing—original draft: Mad.N. Writing—review and editing: Mad.N., H.N., and May.N. Visualization (e.g., figures, tables): Mad.N. Supervision: H.N. Project administration: H.N. All authors have read and approved the final article.
Date Sharing Statement
The data that support the findings of this study are available from the corresponding author, Mad.N., upon reasonable request.
Footnotes
Acknowledgments
Part of this article was presented at the 18th World Congress of the European Association for Palliative Care.
Author Disclosure Statement
The authors declare that there are no conflicts of interest.
Funding Information
This work was supported by the Japan Society for the Promotion of Science (JSPS) KAKENHI (grant number: 23K24686).