
Abstract
Background:
Opioids are widely used for cancer-related pain but are associated with serious adverse events, making appropriate prescription auditing essential. In Japan, most outpatient opioid prescriptions are dispensed at community pharmacies, where pharmacists play a key role. However, the content and clinical significance of opioid-related prescription audits have not been fully elucidated.
Objectives:
To evaluate the content, clinical significance, and impact of prescription inquiries by community pharmacists on outpatient opioid prescriptions.
Designs:
This single-center retrospective cohort study analyzed prescription inquiries related to outpatient opioid prescriptions issued by the National Cancer Center Hospital East between September 2023 and March 2025. Inquiry contents were classified according to drug therapy problems related to efficacy and safety.
Measurement:
Pharmacist interventions were evaluated using established rating instruments for medication-order error severity and clinical value.
Results:
During the study period, 184,688 prescriptions were issued; 10,153 (5.4%) involved inquiries from community pharmacies, including 391 (0.2%) related to opioids, of which 341 (87%) resulted in prescription modifications. Inquiries related to efficacy and safety accounted for 48%, with dosage errors (23%) and treatment duration errors (23%) most common. Overall, 180 cases (46%) were classified as potentially lethal, serious, or significant medication-order errors, and 46% of pharmacist interventions were rated as significant or higher, most frequently involving dosage errors with high severity and clinical value.
Conclusions:
These findings highlight the critical role of community pharmacists in ensuring safe and appropriate opioid therapy and underscore the importance of collaboration between hospital and community pharmacists in outpatient cancer care.
Key Message
Community pharmacists play an essential role in outpatient opioid safety through prescription audits. In this study, 87% of opioid inquiries prompted prescription changes, and nearly half revealed potentially serious errors. High-value interventions corrected dosing or duration problems, underscoring the need for pharmacist–physician collaboration in safe cancer pain management.
Introduction
Cancer incidence is increasing, and the annual number of new cancer cases worldwide is projected to reach 35 million by 2050. 1 Cancer-related pain affects 44% of patients and is more prevalent during and after treatment, particularly in advanced cancer.2,3 Although opioids are widely used for cancer pain, they are associated with adverse events including constipation, nausea, respiratory depression, and dependence;4–6 therefore, appropriate management is essential to ensure safe use.
In Japan, physicians typically issue prescriptions, and opioids are primarily dispensed to patients at community pharmacies.7,8 Community pharmacists are therefore responsible for verifying the appropriateness of prescriptions, assessing patient background, providing medication counseling, and monitoring adverse events.9–11 When questions arise regarding a prescription, community pharmacists contact the prescribing physician for clarification, and the medication is dispensed to the patient after the issue has been resolved. 12
However, the actual status of prescription audit for opioid prescriptions in community pharmacies has not been fully elucidated. In particular, prescription inquiries may serve as an indicator to identify potential problems in opioid prescriptions, yet few studies have systematically analyzed inquiry contents to evaluate community pharmacists’ interventions.
Therefore, this study aimed to evaluate the content, level, and intervention effects of prescription audit conducted by community pharmacists through a detailed analysis of prescription inquiries from community pharmacies.
Methods
Study design and setting
This study is a single-center retrospective cohort study. The objective of the study was to categorize the content of prescription audit inquiries, to establish the detailed categories of inquiries from community pharmacies, and to clarify the level of pharmacist interventions. Consequently, interventions and reports from community pharmacists related to telephone follow-up and tracing reports, which were not considered to be part of prescription auditing, were excluded from the study. The subjects of this study were records of inquiries made by community pharmacies regarding outpatient prescriptions issued by the National Cancer Center Hospital East between September 1, 2023, and March 31, 2025.
Flow for queries regarding doubts
At the National Cancer Center Hospital East, more than 90% of paper prescriptions issued each day are dispensed at community pharmacies. After receiving a prescription from a physician, patients submit it to a community pharmacy to receive their medications. Community pharmacists perform prescription audit during dispensing and contact the hospital when questions arise regarding the prescription.
When inquiries are received from community pharmacies, hospital pharmacists first review and categorize the inquiry content and, if necessary, consult the prescribing physician before providing feedback to the community pharmacist. The inquiry content, medications involved, whether the prescription was modified, and the feedback provided are documented in the electronic medical record. Therefore, at our institution, all prescription inquiries from community pharmacies are recorded in the electronic medical record by hospital pharmacists, and these records were used as the data source for this study.
Surveyed opioids and data sources
This study focused on oral and transdermal opioid medications. The opioids included in this study were selected because they represent the major oral and transdermal opioids approved and commonly used for cancer pain management in Japan. These agents cover the standard opioids recommended in Japanese clinical practice guidelines for cancer pain. The opioids included in the study were fentanyl, oxycodone, morphine, tapentadol, methadone, opium tincture, hydromorphone, and codeine phosphate hydrate. In this study, we retrospectively extracted all records of inquiries regarding these opioids during the study period and investigated the content of inquiries during prescription audits and the level of pharmacist intervention.
Classification of inquiry content and intervention level
The content of inquiries from community pharmacies was categorized based on the framework described by Barnett et al. (2009), 13 with drug therapy problems classified from the perspectives of efficacy and safety (Supplementary Table S1). This classification framework, although not specific to opioids, was applied to categorize opioid-related prescription inquiries by mapping clinically relevant issues such as dosing errors, treatment duration, and safety concerns to the corresponding categories. The level of pharmacist intervention was assessed using the rating instrument reported by Overhage and Lukes (1999), 14 and interventions were analyzed according to the severity of medication-order errors and the value of pharmacist clinical services (Supplementary Tables S2 and S3). The severity of medication errors was assessed based on the potential clinical consequences if the error went undetected and classified as potentially lethal, serious, significant, or minor. The clinical value of pharmacist interventions was evaluated independently according to the framework by Overhage and Lukes and categorized as extremely significant, very significant, significant, somewhat significant, or having no clinical significance. Although these represent distinct concepts, corresponding relationships were observed between severity and intervention value categories. The assessment of severity was performed subjectively by the evaluators based on the potential clinical consequences if the error went undetected, taking into account patient-specific factors such as opioid tolerance, dosing regimen, and concomitant medications. “Potentially lethal” errors were defined as those with a high risk of life-threatening harm, such as respiratory depression. All cases were independently reviewed by two pharmacists authors (K.I. and S.S.), and final classifications were determined by consensus.
Study outcomes
The primary outcomes were the detailed classification of inquiry contents related to prescription auditing by community pharmacies and the evaluation of pharmacist intervention levels. As this study aimed to descriptively characterize these outcomes, no statistical analyses were performed.
Results
Number of cases included in the analysis
The total number of prescriptions issued during the survey period was 192,841. Of these, a total of 391 opioid-related inquiries were included in the analysis (Fig. 1).
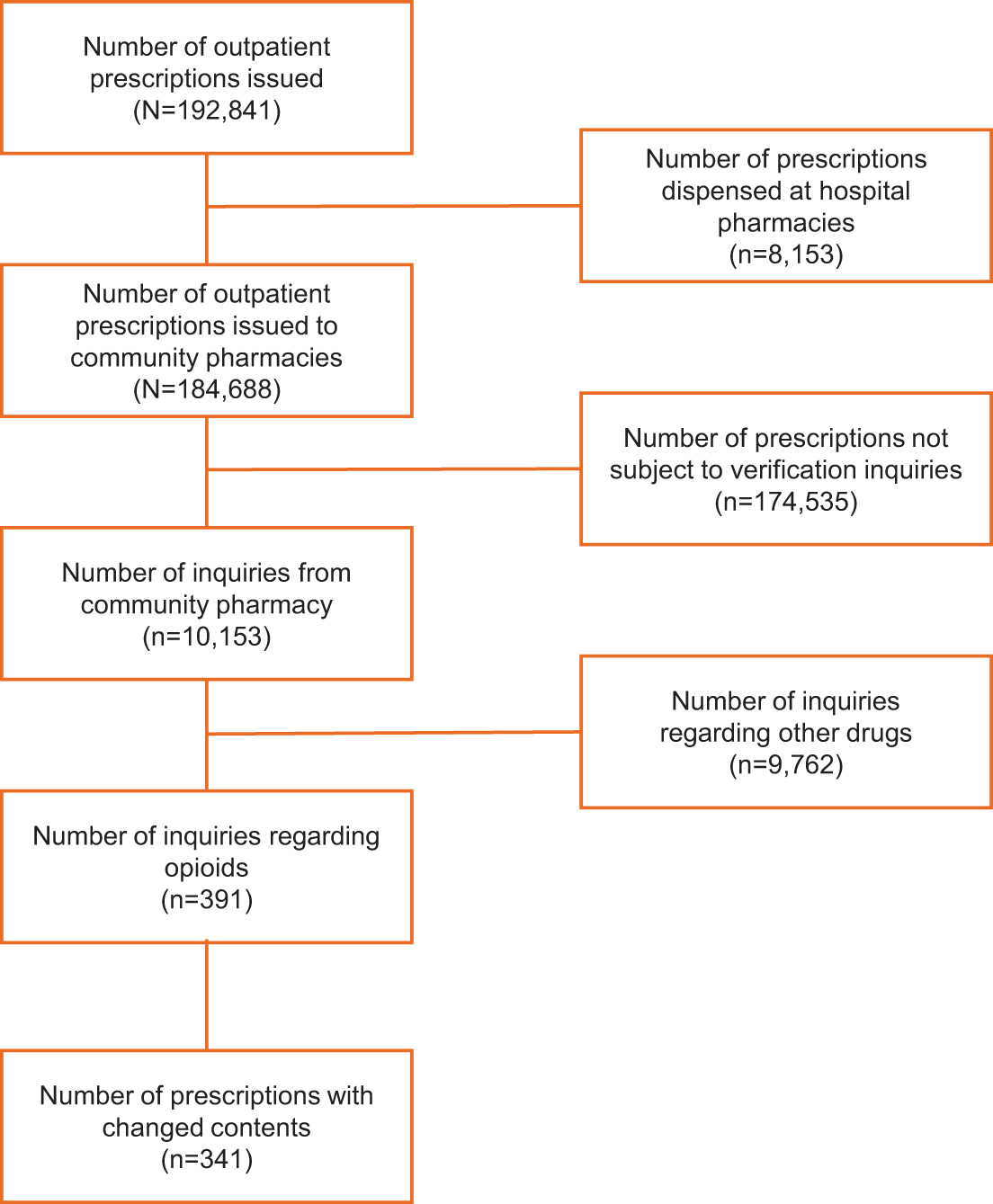
Flow diagram of extracted inquiry cases.
Oxycodone was the most frequently queried opioid, accounting for 247 cases (63%) (Supplementary Table S4). This was followed by fentanyl in 49 cases (13%), codeine phosphate hydrate in 32 cases (8%), morphine in 24 cases (6%), and hydromorphone in 19 cases (5%). Prescription modifications were made in 341 of the 391 cases (87%) following inquiries.
Details of inquiry content
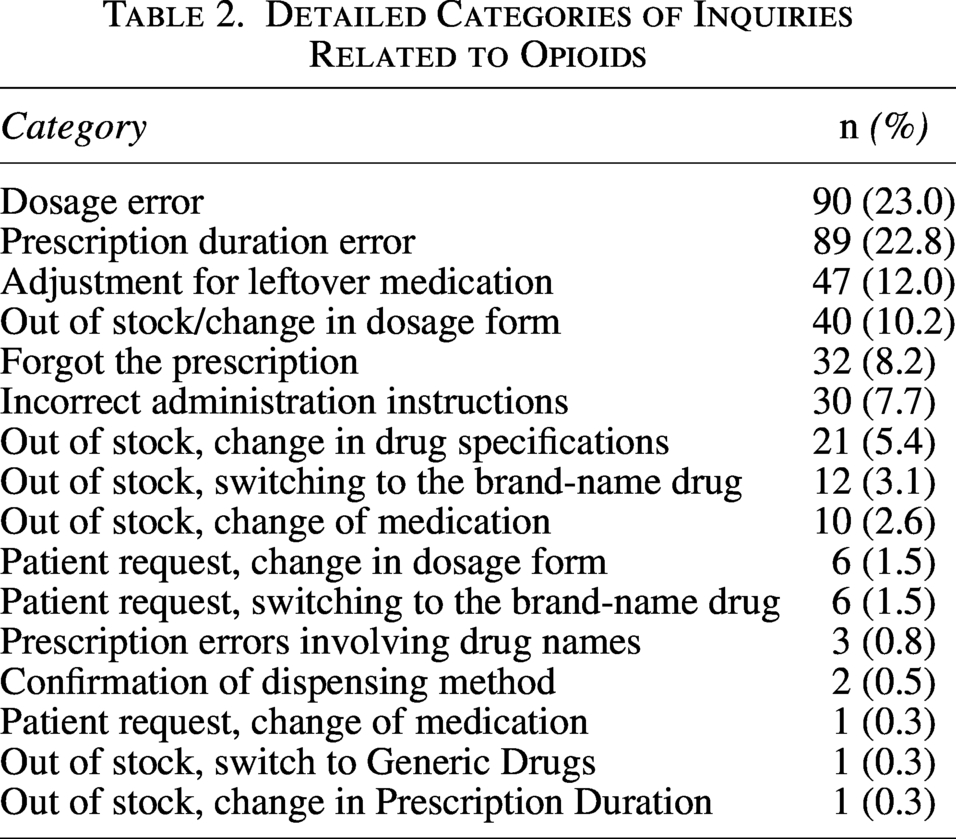
Inquiries were mainly related to drug therapy, efficacy, and safety, each accounting for approximately one-quarter of cases (Table 1). A detailed breakdown of inquiry categories is presented in Table 2. The most common inquiry type was dosage errors (90 cases, 23%), followed closely by treatment duration errors (89 cases, 23%) and adjustments for leftover opioids (47 cases, 12%).
Details of Inquiry Content
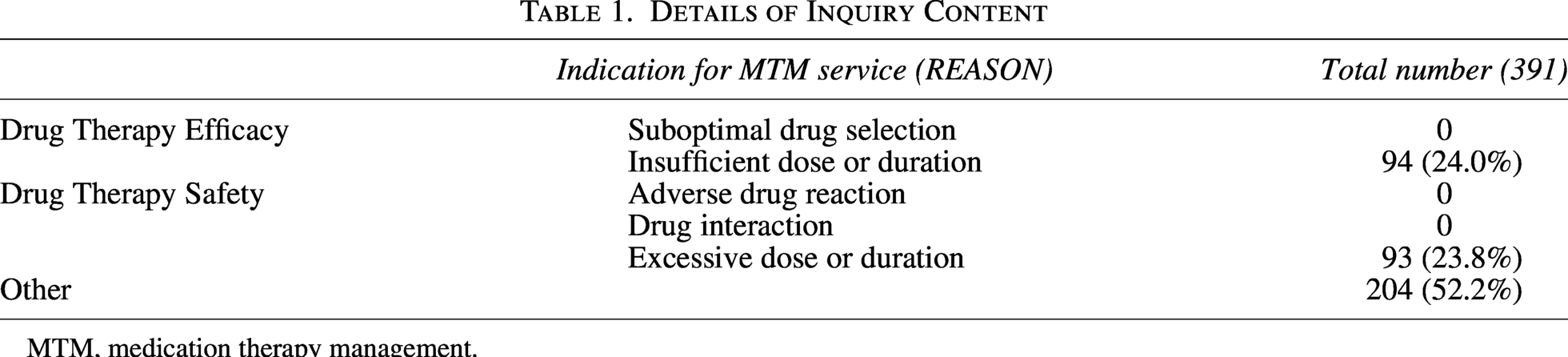
MTM, medication therapy management.
Detailed Categories of Inquiries Related to Opioids
Level of intervention
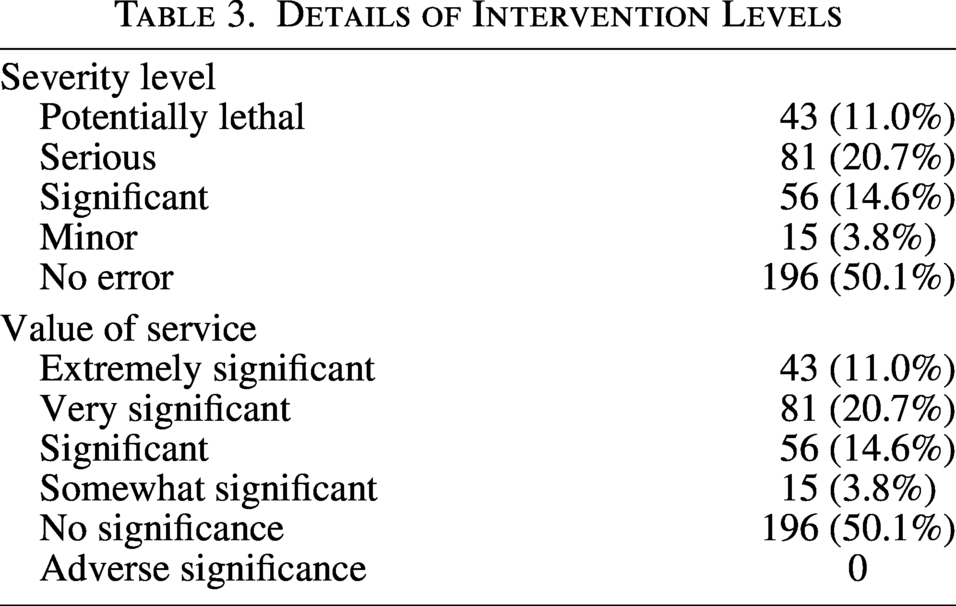
The severity of medication-order errors and the value of pharmacist interventions were assessed for all 391 cases. In terms of error severity, 195 cases (50%) involved medication-order errors ranging from potentially lethal to minor, in which pharmacist intervention was required (Table 3). Furthermore, 180 cases (46%) were classified as potentially lethal, serious, or significant medication-order errors. Representative examples of pharmacist interventions varied according to the severity level of medication-order errors. Potentially lethal cases included excessive opioid prescriptions, such as an unintended 10-fold increase in oxycodone dosage. Serious cases involved insufficient prescription duration following opioid dose escalation, which could have resulted in interruption of pain management. Significant cases included incorrect prescription durations without dose changes, whereas minor cases mainly involved clarification of administration instructions. Cases classified as no error primarily involved formulation changes due to medication stock availability. Regarding the value of pharmacist interventions, 43 cases (11%) were rated as extremely significant, 81 cases (21%) as very significant, and 56 cases (15%) as significant. Overall, 180 cases (46%) were assessed as having a value of service of significant or higher.
Details of Intervention Levels
When inquiry content was analyzed by intervention level, dosage errors were the most frequent category among cases classified as potentially lethal and extremely significant (33 cases), followed by prescription omissions (7 cases) and incorrect treatment duration (1 case) (Table 4). Among cases classified as serious and very significant, dosage errors were again the most common (35 cases), followed by incorrect administration instructions (16 cases) and incorrect treatment duration (15 cases). In cases classified as significant, incorrect treatment duration was the most frequent category (21 cases), followed by dosage errors (17 cases). Representative examples included prescriptions in which the treatment duration was insufficient to cover the period until the patient’s next scheduled visit, such as a fentanyl transdermal patch prescription that was mistakenly issued for 1 day instead of the intended 14 days and subsequently corrected following pharmacist inquiry.
Details on Severity and Value of Interventions
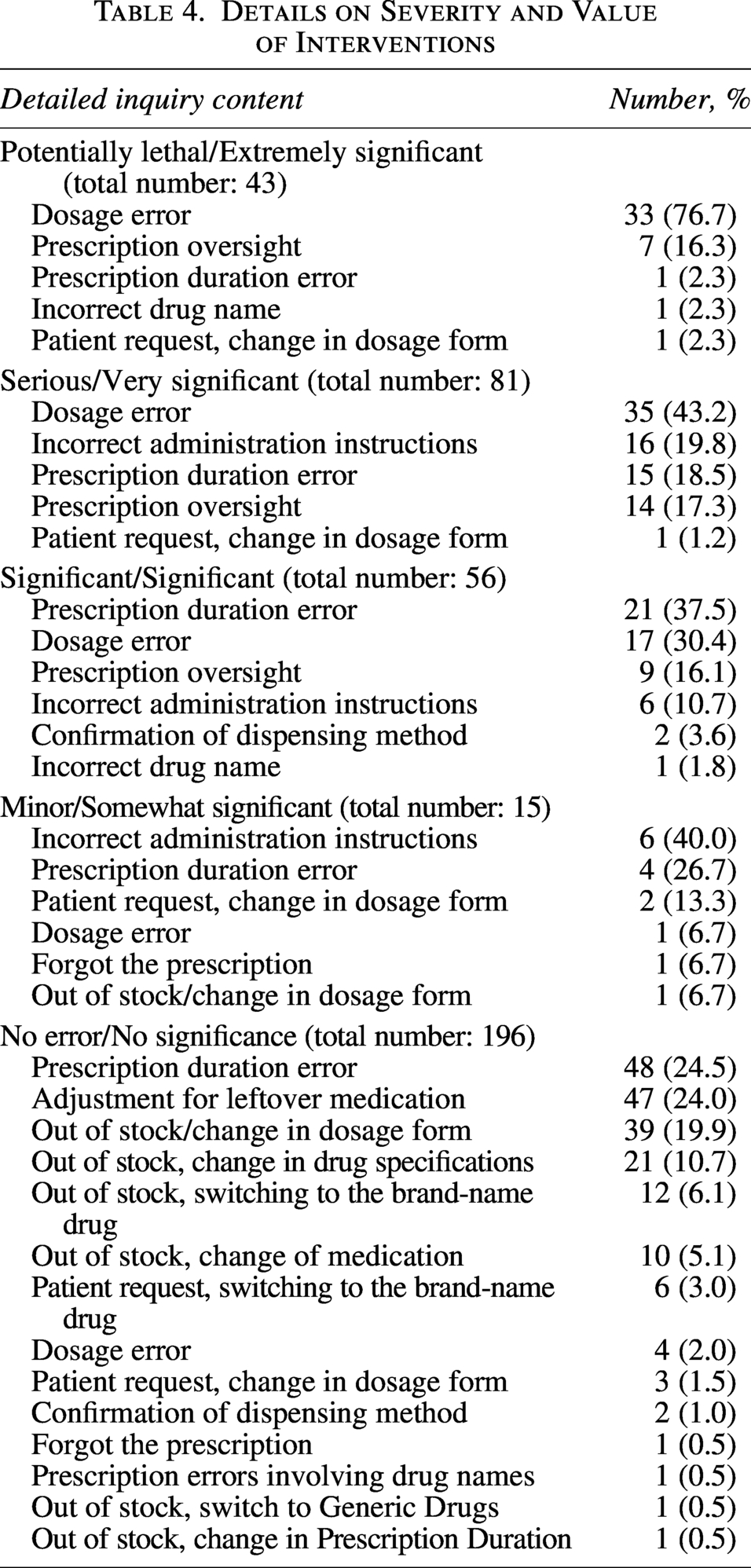
The classifications of severity and intervention value were fully aligned across all categories, with each severity level corresponding directly to a specific category of intervention value (i.e., potentially lethal/extremely significant, serious/very significant, significant/significant, minor/somewhat significant, and no error/no significance), and no discrepancies were observed.
Discussion
This study is the first report in Japan to analyze prescription inquiries from community pharmacies regarding outpatient opioid prescriptions and to evaluate the detailed content of these inquiries and the clinical significance of pharmacist interventions. We found that 48% of inquiries were related to drug therapy efficacy and safety, and 46% were classified as interventions of significant or higher level. These findings suggest that clinically important prescribing issues exist in outpatient opioid therapy and that prescription audit by community pharmacists plays a critical role in identifying and correcting potential prescribing errors.
Approximately half of outpatient opioid prescriptions in this study were classified as potentially lethal, serious, or significant medication-order errors. In recent years, increasing opioid use and diversification of prescribing patterns across regions and health care settings have contributed to greater complexity in opioid management.15,16 Under these circumstances, ensuring the safe and effective use of opioids requires collaboration not only among physicians but also between hospital pharmacists and community pharmacists. Community pharmacists, in particular, are responsible for comprehensive medication management, including concomitant drugs, and therefore require advanced prescription audit skills. In this study, community pharmacists identified many clinically significant errors, and prescription modifications were made in 87% of cases following inquiries, indicating that prescription audit by community pharmacists leads to meaningful changes in real-world practice.
The most frequent inquiry categories were dosage errors and treatment duration errors, together accounting for approximately half of all cases. These categories were also predominant among cases with higher intervention severity and value. Opioid dosing must be individualized based on patient-specific factors such as pain severity, prior opioid exposure, renal function, and concomitant medications. 17 In addition, treatment duration may vary according to treatment response or temporary interruptions. Errors in dosage or duration may therefore result in serious clinical consequences, including overdose, inadequate analgesia, or treatment interruption. Our findings indicate that community pharmacists actively identify these high-risk issues during prescription audits.
In the study by Overhage and Lukes, the severity of medication-order errors was shown to be associated with the clinical value of pharmacist interventions, and high-value interventions could occur even in the absence of prescribing errors. 14 In contrast, in the present study, most interventions were associated with clinically important prescribing issues. This difference may be attributable to the focus on opioid-related prescription inquiries, many of which involved prescribing problems requiring clinical correction. While this likely reflects the clinical nature of pharmacist interventions in this setting, the evaluation was based on subjective clinical judgment and may therefore introduce some variability despite efforts to ensure consistency through consensus. Despite demonstrating high prescription audits capability and intervention value, community pharmacists face several challenges. In Japan, electronic medical records are rarely shared between hospitals and community pharmacies, forcing community pharmacists to rely primarily on prescription information and limited patient interviews. 18 Although many community pharmacists involved in palliative care recognize the importance of opioid management, approximately half do not provide patient counseling. 19 In contrast, educational programs to enhance communication skills and palliative care expertise among community pharmacists have been implemented in Australia and the United States.20,21 In Japan, assessing educational needs and providing structured training programs may improve information sharing and enhance community pharmacists’ intervention capabilities.
Although hospital pharmacists can also perform prescription audits and patient management, limited staffing may make it difficult to provide comprehensive oversight of all outpatients’ opioid prescriptions. In this context, the role of community pharmacists in supporting appropriate opioid use has become increasingly important. Our findings highlight the value of collaboration between hospital pharmacists and community pharmacists in ensuring opioid safety. Furthermore, strengthening collaboration through not only paper-based prescriptions but also the use of technology such as shared electronic medical records and electronic prescription systems, as well as closer communication between hospital pharmacists and community pharmacists, may further enhance cooperative patient care and opioid safety.
This study has several limitations. First, as a single-center study, the generalizability of the findings is limited. Second, the analysis was based on inquiry records documented in electronic medical records, and inquiries managed through other channels may not have been captured. Also, because the total number of opioid prescriptions could not be determined, the frequency of pharmacist inquiries relative to all opioid prescriptions could not be evaluated. In addition, because the evaluations were conducted by pharmacist authors, the possibility of evaluation bias cannot be excluded. Third, we did not assess the clinical experience of community or hospital pharmacists. Because electronic medical records are not shared between hospitals and community pharmacies in Japan, variability in pharmacist experience may have influenced prescription review quality and introduced potential bias. In addition, the level of palliative care training and clinical experience among community pharmacists may influence the quality of prescription inquiries and interventions. However, this study did not assess pharmacist characteristics, and further research is needed to evaluate how pharmacist education and expertise affect intervention quality.
Despite these limitations, this study provides real-world evidence that prescription inquiries from community pharmacies frequently identify clinically important opioid prescribing issues and that community pharmacists contribute substantial value to medication safety. Strengthening information sharing and collaboration between hospitals and community pharmacies may further improve the safety and quality of outpatient opioid therapy.
Conclusion
This study demonstrated that prescription inquiries from community pharmacies regarding outpatient opioid prescriptions frequently addressed clinically significant prescribing issues. Nearly half of the inquiries were classified as having high clinical significance, and prescription modifications were made in many cases following pharmacist interventions. These findings indicate that community pharmacists play a crucial role in identifying and correcting potential prescribing errors through prescription audits.
Authors’ Contributions
K.I., Y.S., and S.S. designed this study and provided critical revisions. K.I., Y.S., and S.S. were involved in analyzing and writing this article. K.I. and Y.S. contributed equally to this work. All authors approved the final version of the article.
Ethics Approval
This study was approved by the Review Committee of the National Cancer Center (Research Project No. 2025-140).
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
sj-docx-1-plm-10.1177_10966218261460520 — Supplemental material for Prescription Inquiries From Community Pharmacies Regarding Outpatient Opioid Prescriptions: A Retrospective Analysis of Content and Clinical Significance
Supplemental material, sj-docx-1-plm-10.1177_10966218261460520 for Prescription Inquiries From Community Pharmacies Regarding Outpatient Opioid Prescriptions: A Retrospective Analysis of Content and Clinical Significance by Keito Ikou, Yuma Shibutani, Shinya Suzuki, Sayaka Nakajima, Akiko Hashimoto, Azumi Sakou, Yasuaki Ryushima, Naoko Kumazawa, Masahito Yonemura, and Naoki Kondo
Footnotes
Author Disclosure Statement
The authors have declared no conflicts of interest.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.