
Abstract
Dear Editor:
Withdrawal of mechanical ventilation (WMV) is a common end-of-life practice in intensive care units (ICUs) and is frequently associated with patient distress. 1 An important emerging trend is that organ donation after circulatory determination of death (DCD), as opposed to death by neurological criteria, is now the most common method of organ recovery. 2 This has major implications for palliative and end-of-life care in the ICU setting. There is limited evidence guiding symptom management and clinical processes for patients undergoing WMV in the context of DCD. 3 Notably, WMV for DCD often occurs in operating rooms rather than ICUs, with procedural differences—such as immediate extubation rather than rapid terminal weaning and patient positioning and draping—potentially influencing the recognition and management of distress.
To generate hypotheses for future research following this major shift in organ procurement, we conducted a retrospective analysis of patients planned for DCD within a larger prospective observational study (OBSERVE-WMV) performed across two academic centers (January 2021–July 2022). 1 Eligible patients were adults undergoing WMV following a transition to comfort-focused care. Distress was assessed by ICU nurses using validated instruments: the Critical Pain Observation Tool (CPOT), Respiratory Distress Observation Scale, 4 and Richmond Agitation-Sedation Scale. Distress was defined by thresholds indicating pain, agitation, or respiratory distress, and recurrent distress as three or more episodes.
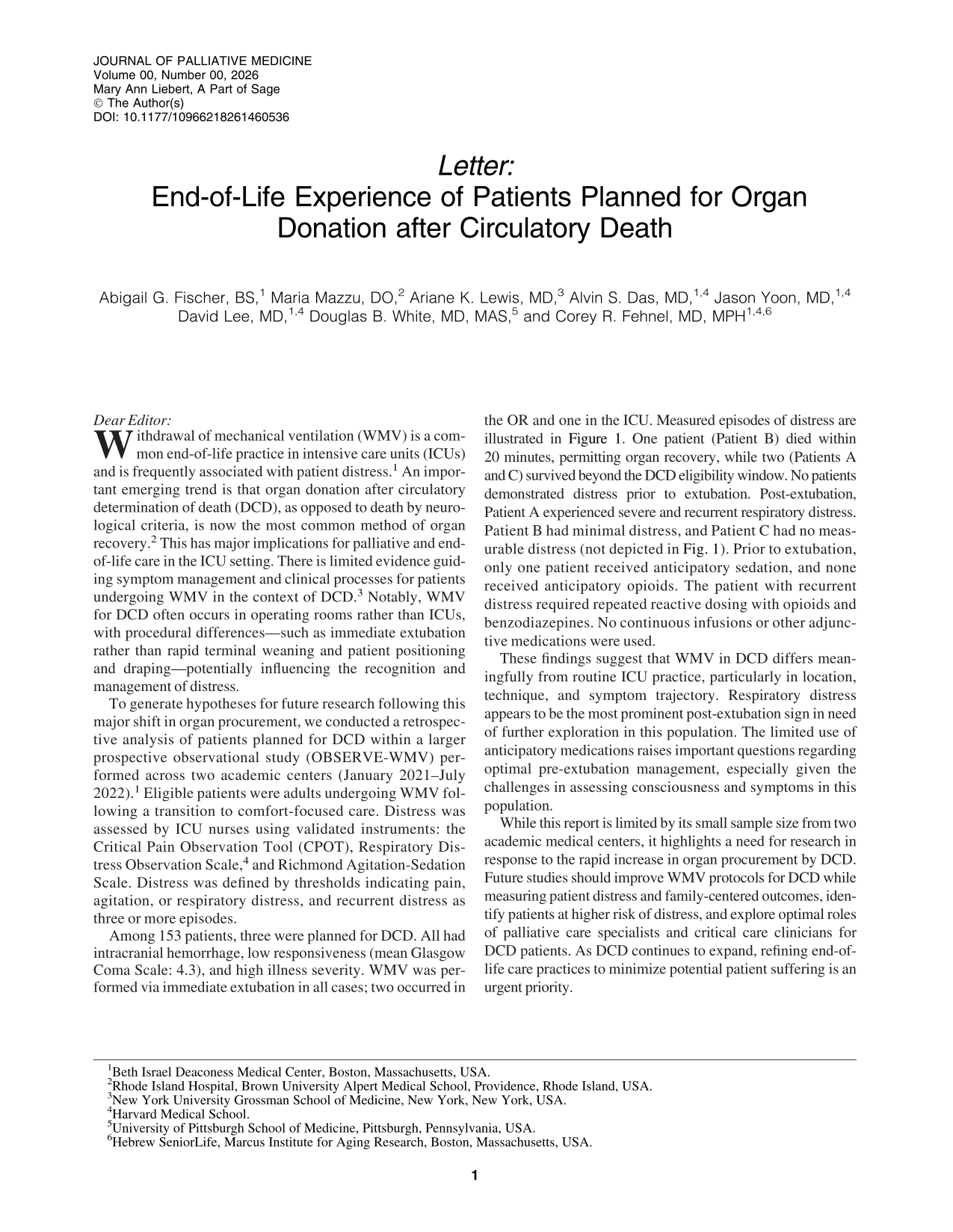
Among 153 patients, three were planned for DCD. All had intracranial hemorrhage, low responsiveness (mean Glasgow Coma Scale: 4.3), and high illness severity. WMV was performed via immediate extubation in all cases; two occurred in the OR and one in the ICU. Measured episodes of distress are illustrated in Figure 1. One patient (Patient B) died within 20 minutes, permitting organ recovery, while two (Patients A and C) survived beyond the DCD eligibility window. No patients demonstrated distress prior to extubation. Post-extubation, Patient A experienced severe and recurrent respiratory distress. Patient B had minimal distress, and Patient C had no measurable distress (not depicted in Fig. 1). Prior to extubation, only one patient received anticipatory sedation, and none received anticipatory opioids. The patient with recurrent distress required repeated reactive dosing with opioids and benzodiazepines. No continuous infusions or other adjunctive medications were used.
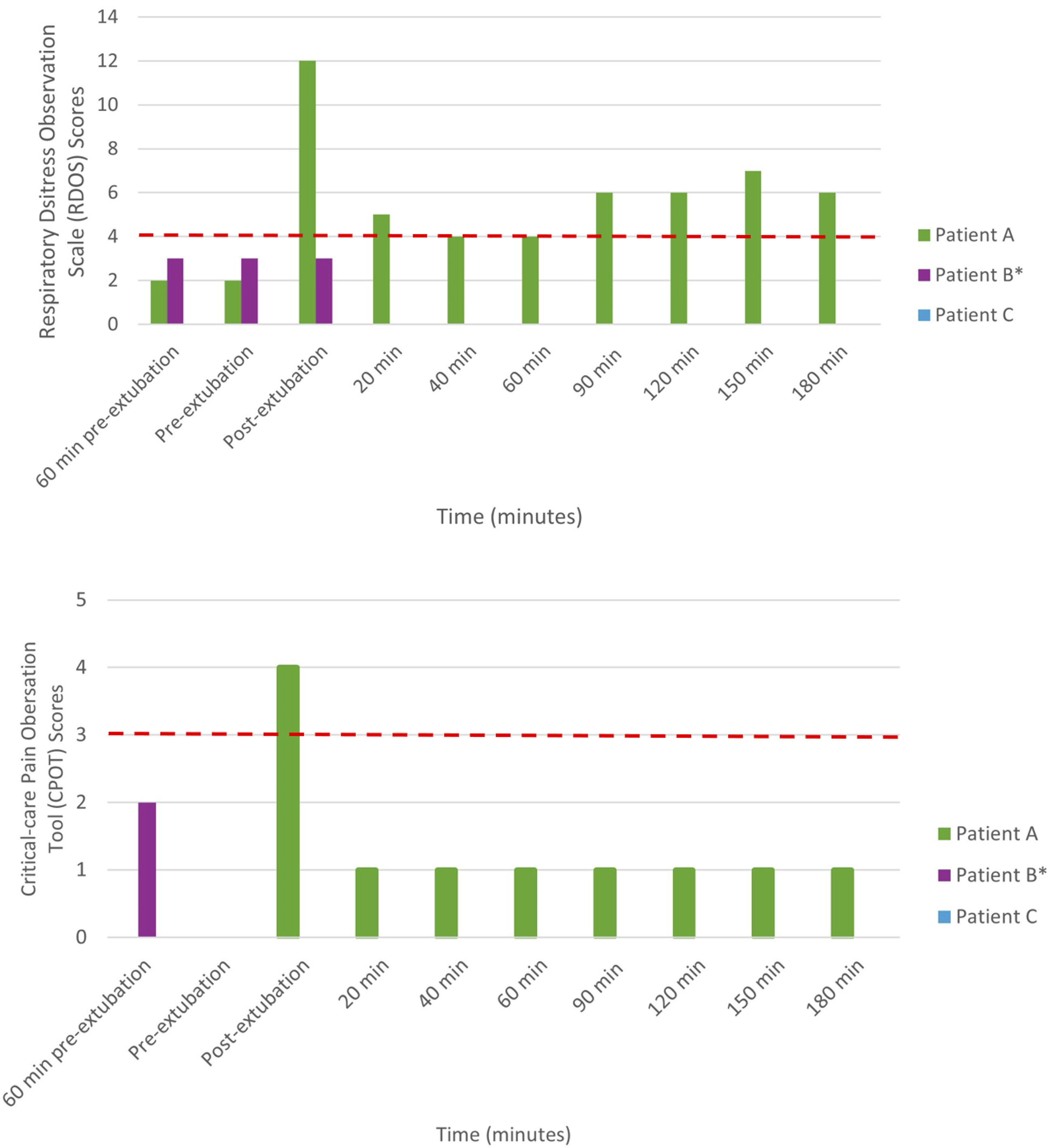
Respiratory Distress Observation Score (RDOS) (upper panel ) and Critical Care Pain Observation Tool (CPOT) (lower panel) assessments of patients undergoing withdrawal of mechanical ventilation planned for organ donation after circulatory death. Pain was measured using CPOT (range: 0–8; scores of 3–4 indicate moderate pain, and scores of 5–8 indicate severe pain). Respiratory distress was assessed with the RDOS (range: 0–16; scores of 3 or less indicate mild distress, scores of 4–6 indicate moderate distress, and scores of ≥7 indicate severe distress). Distressful episodes were defined as a CPOT score >2 and/or RDOS >3. The dashed red line indicates the threshold for a defined episode of distress. Recurrent distress was defined as three or more episodes of distress. Patient B died <20 minutes after extubation (denoted with an asterisk). Patient C had no measurable distress.
These findings suggest that WMV in DCD differs meaningfully from routine ICU practice, particularly in location, technique, and symptom trajectory. Respiratory distress appears to be the most prominent post-extubation sign in need of further exploration in this population. The limited use of anticipatory medications raises important questions regarding optimal pre-extubation management, especially given the challenges in assessing consciousness and symptoms in this population.
While this report is limited by its small sample size from two academic medical centers, it highlights a need for research in response to the rapid increase in organ procurement by DCD. Future studies should improve WMV protocols for DCD while measuring patient distress and family-centered outcomes, identify patients at higher risk of distress, and explore optimal roles of palliative care specialists and critical care clinicians for DCD patients. As DCD continues to expand, refining end-of-life care practices to minimize potential patient suffering is an urgent priority.
Ethical Approval and Informed Consent Statements
The study was approved by the Institutional Review Board at Beth Israel Deaconess Medical Center, including a waiver of informed consent for patient participants.
Conflicts of Interest
C.R.F. serves as Treasurer for the Neurocritical Care Foundation, and a consultant for Aneuryst, Inc. Remaining authors report no relevant disclosures.
Footnotes
Funding Information
C.R.F. is supported by the National Institute on Aging (K23AG066929). D.R.W. is supported by the National Heart Lung and Blood Institute (K24HL148314).