
Abstract
Objective:
This narrative review aims to summarize best practices in palliative care for patients undergoing evaluation for organ donation.
Background:
Palliative care clinicians are uniquely positioned to improve care for potential organ donors and their families. When ongoing life support is no longer consistent with the patient's/family's goals, inpatient palliative care clinicians should be able to recognize and advocate for the end-of-life (EOL) priorities of patients who are potential organ donors. This includes guiding communication during decision-making, as well as providing symptom management for patients and psychosocial support for patients and caregivers.
Methods:
We conducted a narrative review of published literature and policies relating to the role of palliative care in potential organ donors.
Results:
Families of organ donors report a high rate of satisfaction with the decision to pursue organ donation; however, family distress remains common. Moral distress is also common among clinicians caring for patients undergoing organ donation, which can stem from concern for under-treatment of symptoms, worries that medications for comfort are being used to hasten death, and lack of clear roles and expectations in managing the dDCD process.
Discussion:
We present strategies for supporting and communicating with patients and families prior to and during evaluation for organ donation. We also outline a framework for symptom management in the setting of potential dDCD, emphasizing that potential organ donors should always receive EOL symptom management in line with current best practices for withdrawal of life-sustaining treatments, though limited guidance exists for applying these practices in the context of anticipated dDCD. Finally, we discuss the role of palliative care in mitigating moral distress among medical teams and Organ Procurement Organization staff caring for patients who are potential organ donors.
Keywords
Introduction and Framing
The decision to be an organ donor upon one’s death constitutes a laudable altruistic gift made in the interest of helping others. Families can find it affirming to honor their loved one’s altruism by supporting their decision to participate in organ donation. 1 However, without careful planning and coordination by the care team, organ donation discussions and procedures may exacerbate the emotional distress experienced by surrogate decision makers at the end of a patient’s life.1–6
Palliative care teams, with their expertise in identifying patient/family distress and their specialized communication skill set around complex medical decision making, are uniquely positioned to provide support for patients, families, and care teams during this potentially distressing time. Palliative care involvement for organ transplant recipients is inconsistent and highly variable 7 ; there is also limited data regarding current practices in the use of palliative care for potential organ donors. In this narrative review, we provide an overview of the information and processes to help palliative care teams best support and respect their patients’ decision to participate in organ donation. We review the legal and policy context underlying the current organ donation landscape, emerging ethical issues in the organ donation process, and best practices for providing high-quality end-of-life (EOL) care for patients undergoing evaluation for organ donation and their families.
Narrative Review Methodology
This article presents a narrative review of literature relevant to EOL care for patients undergoing organ donation or evaluation for organ donation. The rationale behind this review was to synthesize existing literature on provision of high-quality EOL care for patients undergoing evaluation for organ donation, with an emphasis on communication around organ donation and symptom management at EOL for patients potentially undergoing dDCD. Our objective was to provide a concise, practical guide to EOL care for palliative care and other specialty providers taking care of patients undergoing evaluation for organ donation. We initiated our literature review via PubMed and Google Scholar index search utilizing the search terms “palliative care organ donors” and “end-of-life care for organ donors.” Titles and abstracts that were identified using the above search terms were reviewed for inclusion by the primary author. Inclusion criteria included broad applicability for adult organ donors within the U.S. organ donation landscape and those that contained conclusions or guidance relevant to palliative or EOL care for potential organ donors and their families. We chose to focus on articles applicable to the United States due to the importance of understanding the legal and policy frameworks guiding the donation process in a particular country; articles that discussed physiology, symptom management, and family support were included even if written outside of the United States. Articles were excluded if they solely discussed non-U.S. organ donation policy or if they focused primarily on biomedical interventions for organ optimization or on care of organ recipients. The bibliographies of identified papers were examined for further sources. Saturation was assumed when further bibliography review did not yield novel sources meeting inclusion criteria. Upon identification of the limited evidence base for symptom management at EOL for potential organ donors specifically, we expanded our search to include guidelines and best practices for EOL symptom management in general to provide practical guidance. All four coauthors reviewed the included sources for appropriateness and suggested additional articles for inclusion based on their areas of expertise.
As understanding the legal and ethical context behind the U.S. organ donation system is important for clinicians interacting with patients undergoing evaluation for organ donation, we also performed separate PubMed searches using the terms “ethical issues in organ donation” and “ethics of normothermic regional perfusion”; subsequently, we used a similar process to that described above to identify current relevant articles. Finally, we utilized the Organ Procurement and Transplantation website and relevant legal codes to better flesh out historical context and current policy within the U.S. organ donation system.
Legal and Logistical Overview of Organ Donation
Legal history and role of Organ Procurement Organizations
In 1968, the Uniform Anatomical Gift Act was composed by the Uniform Law Commission (ULC) and adopted by all U.S. states to allow for organ donation with either the prior authorization of an individual—often through registries managed at the state level—or the authorization of their legal next-of-kin.8,9 In the United States, authorization for organ donation is obtained via an “opt-in” approach, in contrast to some European countries where agreement to organ donation is implied unless an individual has specifically opted out. 9 The Dead Donor Rule, which states that organ donors must be dead prior to vital organ procurement, is codified into the laws regulating the organ donation system. 10
The National Organ Transplant Act (NOTA) of 1984 authorized the creation of the Organ Procurement and Transplantation Network (OPTN) to oversee the organ transplant system which encompasses the procurement of organs, maintenance of the transplant waitlist, and allocation of organs. NOTA also established the United Network for Organ Sharing, a nonprofit entity that manages the OPTN. The OPTN is subdivided into 58 Organ Procurement Organizations (OPOs) that cover different geographic regions. 8 OPOs determine an individual’s eligibility for organ donation, discuss organ donation with the patient or family, manage the process of organ procurement, and provide support for families after organ donation occurs. 11 Per CMS (Centers for Medicare and Medicaid Services) regulation, hospitals must support OPOs in informing families of each potential donor of the option to donate. 12
Legal standards and professional practices have established a protocol of separation between the medical team providing clinical care to the patient prior to death and the team conducting organ procurement after death. U.S. Department of Health and Human Services policy requires that only OPO representatives or trained individuals approach families to explain donation options and make the request for donation. 13 In addition, OPTN policy states that organ recovery must not be performed by the same clinician or team that declares the patient’s death to limit potential conflicts of interest. 14 These policies are critical to avoid misunderstandings or missed opportunities for donation that can occur when untrained individuals approach families to discuss organ donation, as well as to avoid undermining the trust that families have in the medical team to act in accordance with the patient’s best interest rather than with the goal of organ procurement.
Types of organ donation
Organ donation includes both solid organs (including but not limited to kidneys, liver, pancreas, heart, lungs) and tissues (cornea, bone, skin). Some organs and tissues can be donated viably from living donors (e.g., single kidney, skin), while others must come from deceased donors. 15 Organ donation by a deceased donor can occur through one of two pathways: donation after death by neurological criteria (dDNC) and donation after circulatory death.
dDNC, colloquially referred to as “brain death,” is currently the most common method of deceased organ donation in the United States. 16 Death by neurological criteria is defined as the irreversible cessation of all brain function, including brainstem reflexes, for example, after a patient suffers severe traumatic or anoxic brain injury. 9 This definition was proposed in the ULC’s 1981 Uniform Determination of Death Act as a legal form of death equivalent to circulatory-respiratory death. 17 Death by neurological criteria is recognized as a legal form of death in all states, though state laws vary in terms of religious accommodations, management of surrogate objection, and standards for testing. 18 In 2023, the American Academy of Neurologists issued updated diagnostic criteria and recommendations for management to support consistent practice. 19
Donation after determination of circulatory death (dDCD) is a newer pathway to organ donation that has been used to expand the pool of potential donors. 20 dDCD represented 36% of organ donors in 2023. 20 dDCD may be considered if a patient is not likely to progress to death by neurological criteria but has a severe, irreversible injury and is likely to cease circulatory function following withdrawal of life-sustaining therapies (WOLST) within an amount of time such that organ donation would remain a viable option. This may occur in cases of severe brain injury (that does not result in death by neurological criteria), cardiovascular compromise, high spinal cord injuries, or reliance on circulatory support like extracorporeal membrane oxygenation (ECMO). 16 For patients deemed appropriate for dDCD consideration, if the surrogate may be considering the removal of life-sustaining therapies in line with what they feel to be the patient’s goals, the OPO representative may then approach to present the option of dDCD.
During dDCD, life-sustaining therapies are discontinued under the care of the patient’s existing medical team, often in the operating room setting. When death occurs within an acceptable time frame for organ viability (generally 60–120 minutes), death is declared by the patient’s medical team, a mandatory “hands-off” period is observed (usually 5 minutes), and the organ procurement team will proceed with organ procurement. 21 Should the patient not progress to death within an acceptable time frame, the patient may return to the ICU where the medical team will continue comfort-focused management, including possible transition to hospice.
Notably, unlike dDNC, the traditional process of dDCD subjects the patient’s vital organs to time without oxygen perfusion after LST is removed, known as “warm ischemia” time, potentially causing damage to the organs. 21 The development of normothermic regional perfusion (NRP) as a technique for organ recovery addresses this concern and has been the subject of significant ethical and legal deliberation, as will be discussed in the subsequent section.
Emerging Ethical Considerations
Trust and transparency in OPOs
Public support for organ donation is high, and public trust plays an important role in the success of the organ donation and transplantation system.22,23 There is substantial variation in trust and perspectives of organ donation, 24 including evidence of decreased willingness among Black individuals to agree to organ donation on behalf of their next-of-kin and concerns that health care professionals engage in unethical organ recovery. 24
In 2020, the CMS approved new performance metrics for OPOs, including requirements to report rates of procured organs and successful transplantations to maintain their certification. 25 There is growing concern that these new requirements incentivize OPOs to pursue organ procurement in ways that stand to undermine public trust in donation. 26 To maintain trust in this life-saving system, it is crucial that potential donors and their families experience respectful and optimal treatment throughout the donation process and that procured organs are allocated fairly and effectively. 27 As discussions around the trustworthiness of the organ procurement system continue, the Health Resources and Services Administration has released a proposal for public feedback and revised policies for OPTN transparency and accountability in dDCD. Proposed policies include standardizing protocols and communication practices among OPOs and creating a required mechanism for stakeholders to call a pause if they have any concerns regarding the appropriateness of moving forward with dDCD. 28
Ethics of first-person authorization
Organ donation does not require informed consent as it entails the disposition of a body upon death and does not stand to confer benefits or harms to the deceased person. Further, members of the public often lack a detailed understanding of the organ donation process when signing up to be an organ donor, meaning registering would not constitute informed consent. 29 All U.S. states have implemented first-person authorization (FPA) laws, wherein prior agreement of an individual to be an organ donor (e.g., by joining a registry when obtaining a driver’s license) constitutes a binding legal gift of their body upon death. FPA is sufficient to proceed with organ donation upon their death without obtaining additional authorization from that person’s surrogate. 30
In practice, FPA primarily applies to patients who are declared dead by neurological criteria, as successful dDCD requires testing and interventions while the patient is still living, for which consent must be obtained from the patient’s surrogate. 31 The frequency at which donation occurs without family agreement is likely quite low; one 2016 study did not find an increase in organ donation rates after the establishment of FPA laws, 32 and one survey of OPOs found that the majority (89%) estimated that the frequency of family objecting to organ donation in cases of registered donors was <10%. 33 While the absolute number of cases may be low, it is important that use of FPA over family objections not be a barrier to trust in the organ donation system. Even when an individual patient has registered as an organ donor, discussions between OPOs and families should be respectful of family needs and preferences regarding donation to avoid worsening family distress and to preserve the trustworthiness of the organ transplant system.
Normothermic regional perfusion
NRP is an emerging option for dDCD that may improve transplant success and graft outcomes.34,35 During NRP, perfusion is re-established in situ after death is declared by clamping the brachiocephalic arteries to occlude blood flow to the brain and using an ECMO machine to maintain organ perfusion, either solely to the abdominal cavity (A-NRP) or to the thoracic and abdominal cavities (TA-NRP), which allows for procurement of the heart and lungs. 36 Most OPOs use NRP for at least some of their cases; however, in one survey, 47% of OPOs that used NRP did not have a specific policy surrounding its use. 37 Of OPOs surveyed, 95% thought that standardized guidance documents would be helpful. 37
Ethicists and clinicians are divided as to the appropriateness of NRP: On one hand, it increases the supply of viable organs in a way that is consistent with the current practice to allow for complete cessation of circulatory functions prior to procurement; on the other hand, by restoring circulation with ECMO, opponents to NRP feel that the criteria by which the patient was initially declared dead are then no longer met at the time of procurement—thus violating the Dead Donor Rule.36,38 It is important to consider whether individuals (when signing up for a donation registry) and surrogates (when authorizing donation on behalf of someone else) are aware of the potential role of NRP and if that awareness is a necessary component of authorizing organ donation.36,38
There is a small but growing amount of information regarding public opinion of NRP. Participants in one survey expressed similar levels of willingness to participate in organ donation with TA-NRP as with dDNC. 25 Another study identified perspectives of various parties (donor families, organ recipients, and providers) regarding NRP; participants were largely reassured by the concept that all brain activity had ceased after the 5-minute waiting period and did not feel that restarting the heart undermined trust in death declaration. 24
Of note, minimal research has explored this important question of whether the brain becomes re-perfused by collateral circulation during the course of NRP. One very small study (eight donors undergoing A-NRP and two undergoing TA-NRP) found that measurement of mean intracranial arterial blood pressure remained the same after initiation of NRP as compared to the time of circulatory death. 39 Overall, NRP remains a controversial subject with variations in practice across regions and institutions, and it is important for clinicians to be familiar with the practices and policies at their own institution.
Support for the Patient and Family Prior to Decision for Organ Donation
OPO referral: Understanding which patients are potentially eligible for organ donation
Any patient who is undergoing evaluation for death by neurological criteria or whose family plans WOLST as a component of EOL care should be referred to the OPO. It is important to note that referral to the OPO does not necessarily mean the patient will be eligible to proceed to donation. In addition, the patient’s condition may improve, such that organ donation is no longer a consideration. Nevertheless, timely referral to the OPO supports optimal planning, communication, and outcomes should the patient’s condition support eligibility for organ donation. 16
Each OPO has specific clinical criteria that should trigger a referral for evaluation, and hospitals are required to alert the OPO when patients meet these triggers. 40 It is helpful to be aware of these criteria for your institution to facilitate prompt referral, which is important to enable the OPO to have time to evaluate the patient for eligibility. The OPO is responsible for evaluating the patient for donor eligibility; thus, it is important to refer all patients who meet the clinical triggers, even those with medical factors that may limit eligibility. 16 For patients who are undergoing assessment for death by neurological criteria or for any patient for whom WOLST is being considered, early proactive dialogue with the OPO regarding the patient’s eligibility for donation can help guide the approach to EOL communications.
Family communication prior to discussion of donation
Communication with families regarding the patient’s diagnosis and prognosis should be clear, compassionate, and direct. It is also vital to ensure that the patient has been given enough time for potential clinical recovery, particularly for clinical situations (e.g., traumatic brain injury) in which early prognostication is difficult. Palliative care teams should collaborate closely with the ICU team and OPO to understand whether a patient may be eligible for organ donation. 16 Once the ICU team has shared with the surrogate that a patient is likely to fit the criteria for death by neurological determination, teams should collaborate with the OPO to assist the OPO in determining optimal timing to approach the surrogate. Palliative care teams are often most familiar with family dynamics and evolving emotional readiness and thus can be the most appropriate members of the medical team to guide timing of OPO approach. 41 For patients who are receiving life-sustaining therapies and are potentially eligible for dDCD, goals of care conversations should be held without discussion of organ donation as for any other patient. If continuation of life-sustaining therapies is inconsistent with goals of care, then surrogates should be provided the opportunity to meet with the OPO (see next section).
The pause: Providing family with the opportunity to meet with the OPO representative
Once a patient’s surrogate medical decision maker is aware of the patient’s condition and future expectations with ongoing life-sustaining therapies, the discussion may shift to a comfort-focused approach in which teams and families determine the logistics and timing for WOLST. If the patient is potentially eligible for organ donation, it is important to pause before final decision making to allow the surrogate to speak with an OPO representative. This pause ensures that surrogates are fully informed in making decisions most consistent with the patient’s values and preferences prior to solidifying a timeline or location for WOLST. The pause also helps to mitigate the distress that can be caused to families by backtracking from what they perceive to be an already established plan of care. Palliative care clinicians are often already familiar with family dynamics and preferences and thus can play an important role in guiding teams and families regarding the timing of this pause and subsequent communication (Fig. 1).
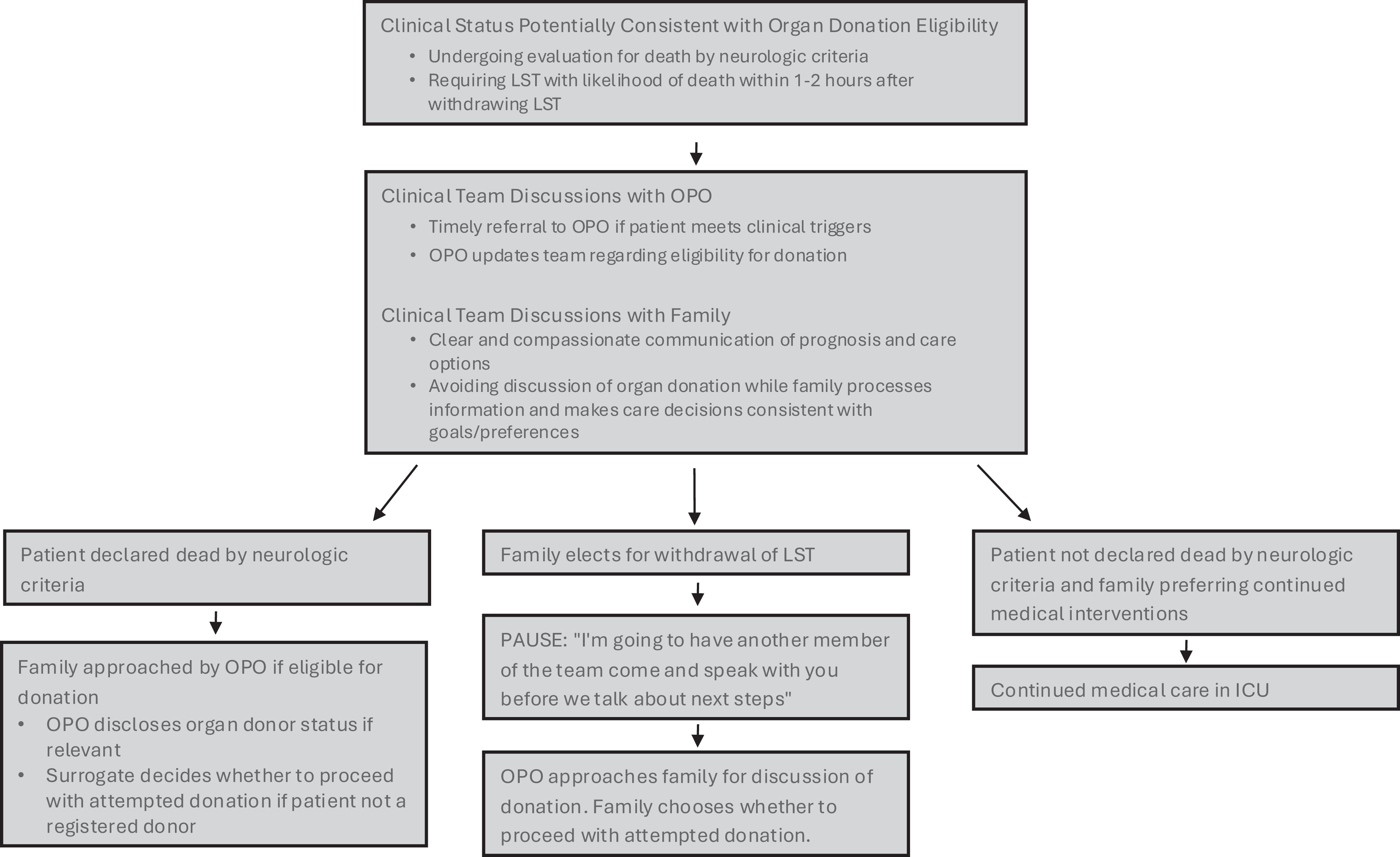
Algorithm for engaging in shared decision making with families of patients who are potential organ donors.
Once a surrogate decides to proceed with organ donation, they may have further questions about what the process looks like. Having a supportive relationship with the OPO representative allows the team to direct these questions to the OPO and facilitate answers in a timely manner. In addition, clinical teams can act as advocates for the patient and their family preferences during the donation process. As palliative care teams are often familiar with typical EOL clinical/symptom trajectories as well as protocols/procedures surrounding EOL care at their individual institutions, they are poised to advocate for surrogate preferences for EOL rituals and provide symptomatic support during WOLST. 42
Providing emotional support for family
Families of organ donors describe the importance of empathetic communication and support from ICU team members and OPOs, as well as clear anticipatory guidance regarding the donor process. Best practices include providing multimodal communication (e.g., supplementing conversations with visual information guides), having family meetings in the appropriate setting (i.e., in a private setting, in-person when possible, with all relevant decision makers and team members present, and with sufficient time to address concerns or questions), and having a support person available. 6 In their assessment of patients and families, palliative care teams can play an important role in mitigating family distress and the development of post-traumatic stress symptoms by identifying and responding to family distress in the moment, as well as by anticipating distressing moments and appropriately involving the interdisciplinary team for support.41–43 See Table 1 for specific examples of potential precipitants of family distress and recommended approaches for prevention and management.
Recommendations for Management of Potential Points of Family and Team Distress
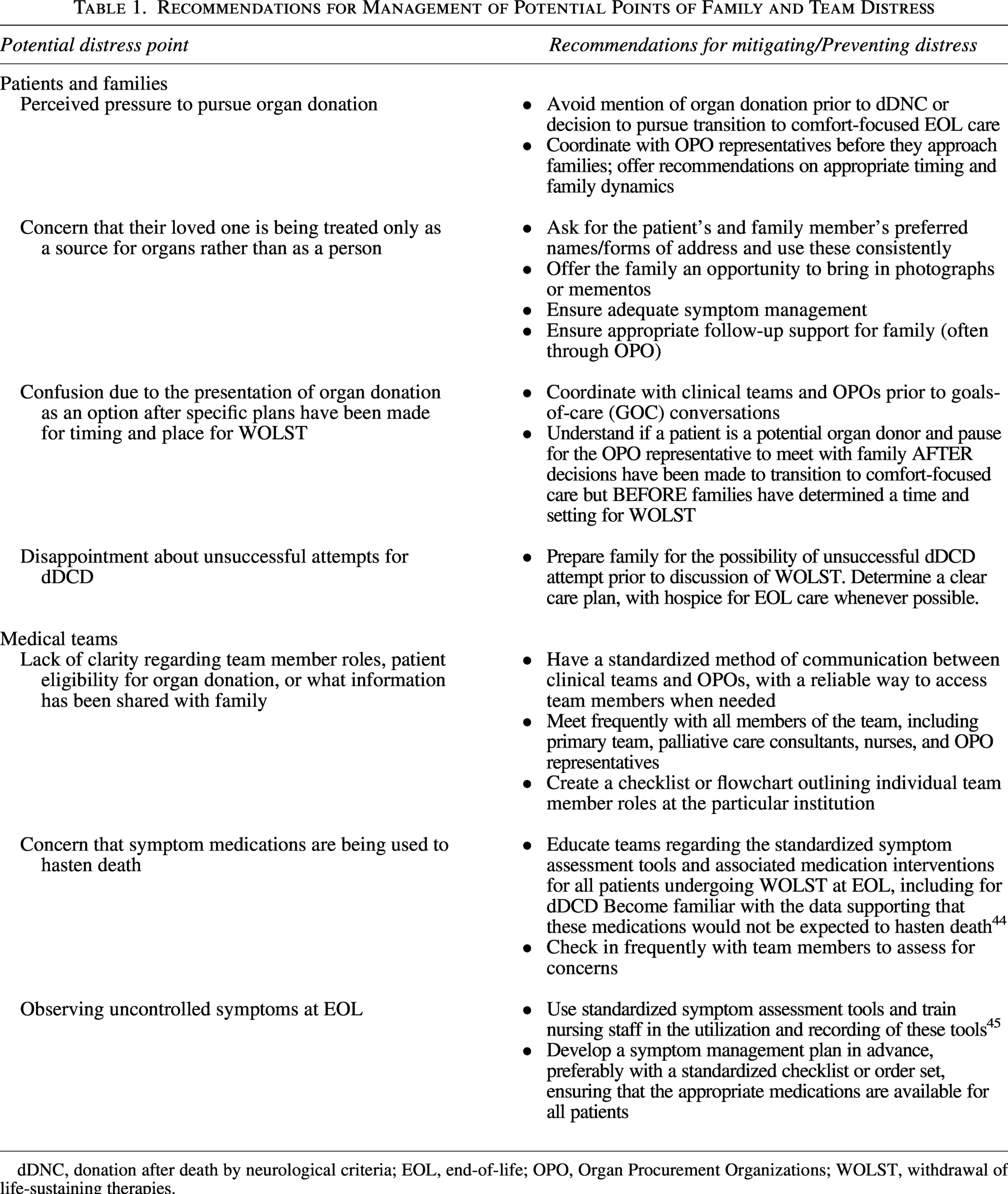
dDNC, donation after death by neurological criteria; EOL, end-of-life; OPO, Organ Procurement Organizations; WOLST, withdrawal of life-sustaining therapies.
Support of the Patient and Family During and After Organ Donation
High-quality EOL care for potential organ donors
Potential organ donors must receive high-quality EOL care that is consistent with established best practices. 45 A consistent protocol for WOLST in the setting of dDCD can confirm that all patients receive high-quality care (Fig. 2). While there is little direct evidence regarding symptom control during DCD, 46 Healey et al. outline a set of best practices for WOLST in the setting of dDCD. 45 These best practices emphasize the importance of validated symptom assessment tools as well as rigorous and standardized medication administration to optimize symptom control. 45
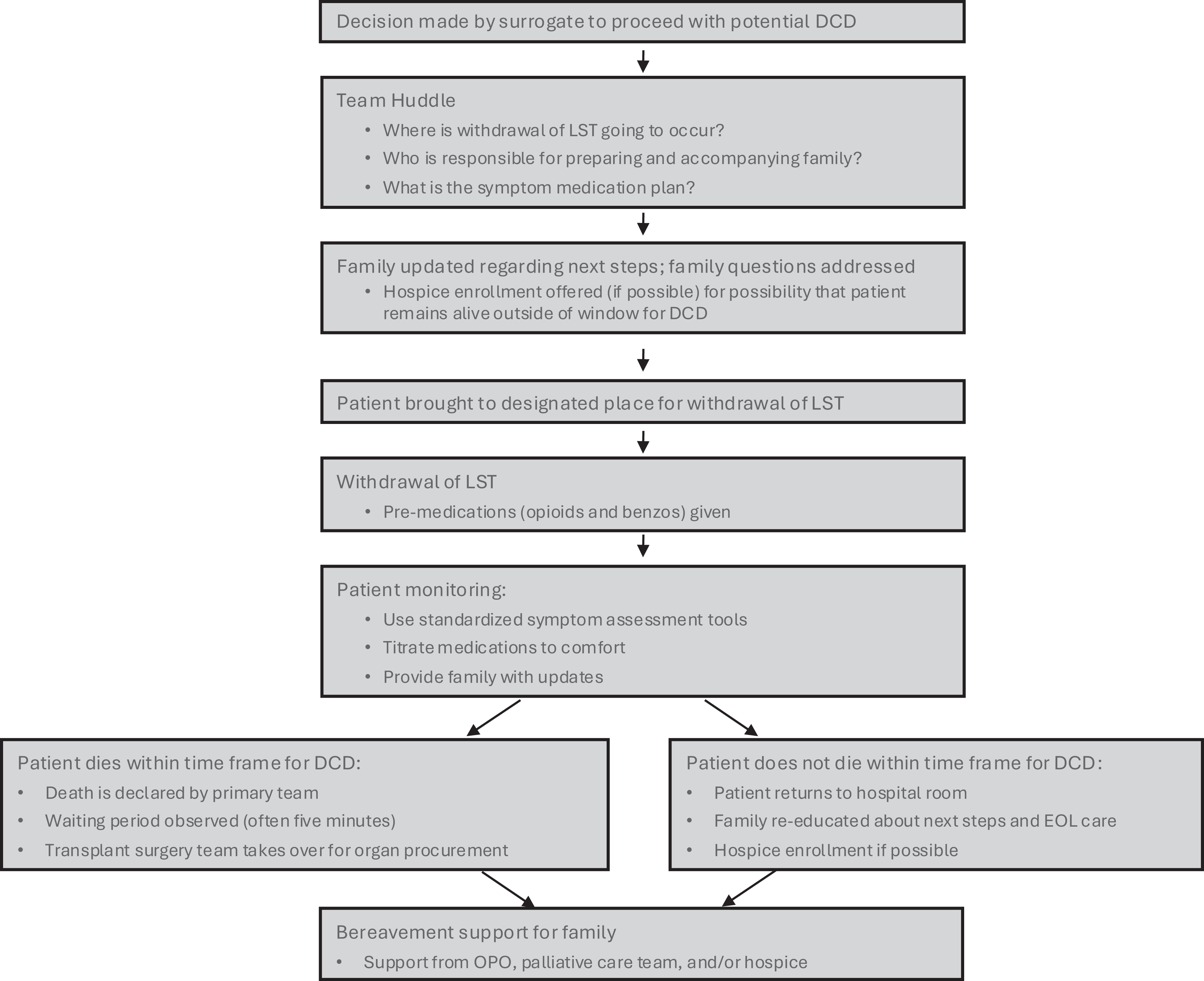
Algorithm for providing best practices in EOL care for patients undergoing WOLST for potential DCD.
The use of validated symptom assessment tools to assess respiratory distress, pain, and agitation can help guide appropriate medication dosing and titration; these tools should be used before, during, and after WOLST, with adjustments to symptom medications if scores exceed the target. Examples of validated symptom assessment tools include the Respiratory Distress Observation Scale (RDOS) for respiratory distress, the Nonverbal Pain Scale for pain, and the Richmond Agitation Sedation Scale for sedation.47–50 While there is no evidence for the use of any particular symptom assessment tool in dDCD, the RDOS is a validated, commonly used tool for assessing dyspnea at EOL for patients who cannot self-report their symptoms. 48
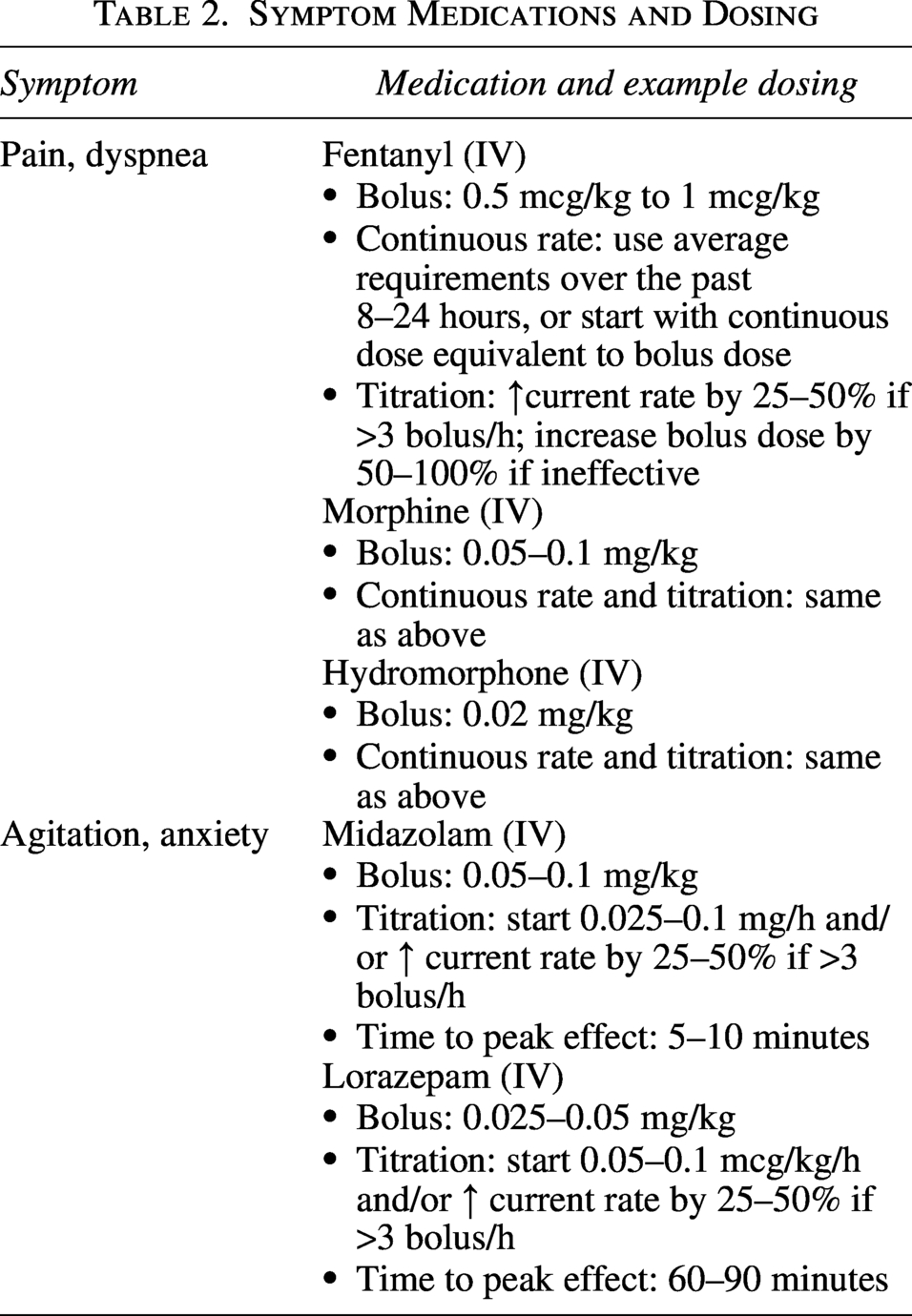
Medications for symptom management are also essential. More than 30% of all patients undergoing WOLST at EOL may experience respiratory distress, highlighting the importance of adequate symptom control. 51 Premedication with opioids before WOLST is associated with improvements in symptom control. 51 While there is limited evidence regarding selection and dosing of symptom medications, opiates are preferred agents for pain and respiratory distress, and benzodiazepines have the best evidence for anxiety and agitation at EOL. 47 Medications should be titrated until the symptom burden is minimal. In one study, the use of the RDOS as part of an algorithmic approach to management of respiratory distress at EOL was associated with a significant reduction in respiratory distress after WOLST. 49 Standardized order sets with medication indications and dosing instructions can be developed to ensure that all individuals undergoing DCD receive optimal symptom management. 45 We have included a list of example medications and dosing strategies (Table 2); this table only provides rough guidance due to the limited evidence for specific dosing or protocols.
Symptom Medications and Dosing
Support of the family during and after the donation process
Families often report high satisfaction with the decision to pursue donation; 1 however, they also express distress related to the donation process itself. Much of the existing literature focuses on optimizing successful organ transplants, with little focus on family support or symptom management in dDCD.5,6 The evidence that is available indicates that families are at high risk for experiencing traumatic memories of the course of ICU treatment, organ donation approach, and organ donation process, 4 with post-traumatic stress symptoms commonly reported. 2 Post-traumatic stress symptoms are common among family members of any patient dying in the ICU, and family members who have participated in EOL decision making may be at even higher risk. 3 These trends likely also apply to families of organ donors. Person-centered (rather than organ-centered) communication from teams may help to mitigate post-traumatic stress symptoms and distress. 4
Emotional and spiritual support for families is vital. Families report the importance of their loved one being treated as a human rather than simply a potential donor; this can be facilitated by bringing pictures of their loved one into the hospital or sharing stories about their loved one. 6 The palliative care interdisciplinary team, with established expertise in providing support and highlighting the individuality of the patient as a person, can play an important role in this process. Other best practices include having a support person who has been through a similar experience available during key moments, allowing families to walk their loved one to the OR (the “honor walk”) and be present for WOLST, and informing families about rituals to recognize donors. 5 Families also often express appreciation for follow-up and updates from the OPO (e.g., which organs were successfully recovered and if those organs were matched with a recipient). 6
Support of the patient and family in unsuccessful dDCD
Quality EOL care for patients and family support is essential when the patient does not progress to death within an acceptable time frame for dDCD. Up to one-third of patients who begin the dDCD process remain alive beyond 2 hours after withdrawal of LST and are not eligible for dDCD. 52 The mean time to death after WOLST for those not eligible for donation is 33 hours. 52 When patients return from the OR after unsuccessful DCD, they may require titration of symptom medications to ensure adequate symptom management.
Families will also need continued support, as they may not be emotionally prepared for a prolonged dying process. In these situations, some families express feeling a “second loss” or a sense of disappointment that donation was not able to occur. 6 In one study, families participating in focus groups described feeling distressed by the inability to honor their loved one as an organ donor and struggling to find meaning in the death. 53 Family members also reported a feeling of prolonged agony while waiting for death to occur and to learn if organs were useable, as well as regret over the “waste” of organs that were not able to be transplanted. 53 If the hospital caring for the patient has a mechanism by which inpatients can be enrolled with hospice services, the hospice agency can provide immediate symptom management after the patient returns from the operating room. In addition, while 54 OPOs are required to offer continued support and connection with donor families regardless of donation outcome, 16 hospice agencies can also provide an additional level of support through their mandated 13 months of bereavement care.16,42
Support of Clinical Teams
Taking care of critically ill patients, particularly those undergoing evaluation for potential organ donation, can cause distress for clinicians. To best support clinical teams, it is important to be aware of common causes of distress and how this distress may be mitigated. See Table 1 for a description of potential sources of team distress and recommendations for prevention and mitigation.
Witnessing uncontrolled symptoms at EOL can be a source of substantial distress for nurses. 55 Minimizing symptom distress before, during, and after WOLST by using standardized symptom assessment tools and medications as discussed above can help to reduce this distress. In addition, clear communication, consistent hand-offs, and identification of the roles played by each time (medical team caring for patient prior to death, nursing team, OPO, and transplant surgeons) can reduce the distress that comes from unclear roles/expectations and lack of transparency 47 ; palliative care teams are often well-equipped to promote this clear communication and clarity of roles, given their familiarity with EOL situations and high-stakes communication. 41
Team members may also experience moral distress if they believe that life-sustaining therapies are being inappropriately withdrawn or that death is being hastened to facilitate successful dDCD. As in any other WOLST, it can be helpful to discuss the concern in terms of the ethical principle of respect for autonomy: a patient or their surrogate has the right to refuse life-sustaining therapies if they are no longer aligned with the patient’s goals of care, even if cessation of intervention will lead to expected death. Intentional education of clinical teams, including nurses who are responsible for administering medications, can be helpful in reducing misconceptions that medications are being used to hasten death. First, explicit discussion of the intended purpose of medications to control symptoms, alleviate discomfort, and prevent suffering during an expected dying process helps to promote understanding and support for appropriate medication administration. Second, using standardized clinical tools as described above can reassure all team members that medications are being titrated to provide symptom control rather than to hasten the dying process. There is empirical evidence that opioids and benzodiazepines, when administered for symptom treatment and titrated to symptom relief, do not lead to hastened death 44 ; sharing this evidence when concerns arise can help to mitigate distress. In addition to providing general guidance and education, clinicians should address any concerns raised by team members regarding potentially inappropriate WOLST or medication administration directed toward hastening death. Any change in the patient’s condition warrants reassessment of dDCD eligibility to confirm that parameters for level of consciousness and ventilatory support remain met.
Moral distress among OPO representatives
OPO representatives can be overlooked as members of the clinical team. They have to navigate balancing the needs of donors and families with the pressures to obtain as many viable organs for transplant as possible. This dual set of obligations can place OPO representatives at higher risk of developing moral distress. OPO representatives must also communicate with families in difficult situations, such as when a patient is a registered donor but their legal next of kin may be unaware or not share this preference. Clinical teams should recognize the potential for distress among OPO representatives and acknowledge the potential need for supporting these members of the care team. 11
Conclusion
Palliative care teams play an essential role in promoting patient autonomy and supporting family decision making by creating space for all possible EOL goals. By applying expert communication skills and developing familiarity with the OPO staff and process for organ donation in a particular hospital, palliative care teams can facilitate clear communication between clinical teams and OPOs, promote goal-concordant EOL care regardless of donation preference, and hold OPOs accountable for respectfully and compassionately navigating conversations with families. As for any other dying patient, rigorous symptom control and family support are essential for patients undergoing dDCD; standardized assessment tools and consistent use of symptom control medications can help to ensure that each patient and family has access to quality EOL care.
Footnotes
Author Disclosure Statement
None of the authors have conflicts of interest to report.
Funding Information
No funding was received for this article.