
Abstract
Background:
Nausea and vomiting are distressing symptoms in palliative care. Due to a heterogeneous population and limited evidence, clinical management remains challenging. Guidelines often recommend an etiology-based treatment approach, but supporting evidence is scarce, particularly for noncancer patients.
Objectives:
Evaluating the impact of a structured, etiology-based treatment pathway on nausea and vomiting burden and treatment quality in palliative care patients.
Setting/Subjects:
Single-center, before-after study in adult patients on a German tertiary palliative care unit, comparing symptom burden and treatment quality before (Phase 1, 15 months) and after (Phase 2, 12 months) implementation of the pathway.
Measurements:
Outcome measures were change in symptom burden score on day 3 (Integrated Palliative Care Outcome Scale ([IPOS]), treatment quality (quality indicator [QI]; burden reduction on IPOS), and duration of symptoms (days). Significance level was set at α < 0.01.
Results:
In Phase 1, 172/330 patients (52.1%) experienced 230 episodes of nausea/vomiting, versus 139/280 patients (49.6%) with 178 episodes in Phase 2. On day 3, symptom burden scores for nausea decreased to a greater extent in Phase 2 (p = 0.007); vomiting showed a nonsignificant reduction (p = 0.021). The QI (nausea) was met in 124/178 (69.7%) versus 129/156 (82.7%) (p = 0.0056), and the QI (vomiting) was met in 66/93 (71.0%) versus 81/95 (85.3%) (p = 0.0176) episodes. Symptom duration decreased from 3 (0–25) to 2 (0–23) days (p < 0.001).
Conclusions:
The systematic etiology-based pathway significantly improved cause identification and treatment quality. While benefits were more pronounced in cancer patients, this structured approach provides a robust framework for enhancing antiemetic management in the palliative care setting. Further studies should investigate antiemetic treatment in noncancer patients.
Key Message
This study investigates the impact of a structured treatment pathway on nausea and vomiting symptom control in palliative care, highlighting the effectiveness of a systematic approach over standard care, particularly in cancer patients. However, further research is needed to optimize tailored interventions for noncancer patients.
Introduction
Nausea and vomiting are common and burdensome symptoms in palliative care, with reported prevalence of nausea from 22% to 68%1–3 and vomiting from 20% to 40%.1,3 Patients describe even mild nausea as very distressing,2,4 with a great influence on their quality of life. The management of these symptoms remains challenging in clinical practice.2,5 The broad spectrum of antiemetics, heterogeneous patient population, and risk of adverse effects and interactions 6 require cautious, evidence-based treatment. Moreover, palliative care guidelines predominantly focus on patients with underlying malignancy7–10 and do not address the diverse needs of other diseases sufficiently. Yet, studies highlight that individuals with nonmalignant conditions also frequently suffer from nausea in palliative settings.11,12 This backdrop underscores the need for evidence-based treatment recommendations that comprehensively address both cancer and noncancer patients.
Current international guidelines mostly recommend an etiology-based approach for selecting the appropriate antiemetic treatment,7,8,13,14 with overall limited evidence. This approach depends on correct cause identification, yet studies found no underlying cause in 26–43% of cancer and noncancer patients.1,2 Additionally, the multifactorial symptom origin often complicates appropriate drug selection. 2 One study with cancer patients showed the etiology-driven treatment approach to be effective in 56% after one week, 15 which may be insufficient in this time-limited, vulnerable setting.
In response to these gaps, this study evaluates the impact of a structured pathway on the symptom burden of nausea and vomiting and the antiemetic treatment quality in patients admitted to a palliative care unit, regardless of their underlying disease.
Methods
Study design
A before-after observational study was conducted and reported according to the STROBE Guidelines. 16 First, the status quo of the treatment quality of nausea and vomiting on a German palliative care unit was evaluated (15 months, Phase 1, January 2021 to March 2022). During this period, antiemetic management followed standard care based on individual physician experience, with the German palliative care guideline available for consultation. Detailed results are reported elsewhere. 1 Second, the impact of a structured, etiology-based treatment pathway 17 on the treatment quality was investigated retrospectively (12 months, Phase 2, March 2023 to February 2024).
Participants and setting
All adult patients (inpatient stay ≥2 days) with advanced disease, consecutively admitted to the palliative care unit of a tertiary hospital, were included. When admitted to this unit, cancer patients typically did not receive further antitumor treatment.
Treatment pathway
The development of the pathway is reported elsewhere.17,18 It is based on recommendations of eight international palliative care guidelines,7,9,10,14,19–22 a noncomprehensive literature search (until November 30, 2022) and results from Phase 1. Given the palliative focus of this study, guidelines for chemotherapy-induced nausea/vomiting were not considered. Analogous to international guidelines, the pathway follows an etiology-based approach for managing nausea and vomiting. It supports cause identification and drug selection for seven palliative care scenarios. Furthermore, reassessment of the treatment is emphasized, including steps for therapy escalation and discontinuation. The pathway was developed by two palliative care pharmacists based on multiprofessional perspectives from experienced palliative care physicians. It consists of a treatment algorithm (Supplementary Fig. S1), a user’s guide, and information on prescribed drugs. 17 Implementation was facilitated through structured training and a formal standard operating procedure. To ensure the pathway served as a real-time clinical decision-support tool, it was integrated into the patient’s medical records and used for consultation during rounds.
Study endpoints and data collection
Demographic data and the Australia-modified Karnofsky Performance Status 23 (assessed by physicians) were extracted from patient records. The Charlson Comorbidity Index (CCI) 24 was based on documented diagnoses. Prescription charts provided medical data; the suggested etiology was documented with the pathway.
The primary endpoint was the change in symptom burden scores for both nausea and vomiting on day 3 after treatment initiation. Symptom burden was assessed daily with the Integrated Palliative Care Outcome Scale (IPOS) (0: no burden, 4: highly affected), 25 primarily via proxy reports (medical staff) and patient reports when possible.
Secondary endpoints included duration of nausea and vomiting symptom burden (days; ended after complete resolution according to IPOS) and a predefined quality indicator (QI) for both symptoms, calculating the proportion of patients for whom the symptom burden decreased by ≥1 point on IPOS on days 3 and 6 of a treatment episode. This reduction was considered clinically meaningful. A treatment episode began with symptom onset or initiation of continuous antiemetic therapy and ended when nausea/vomiting resolved or no antiemetics were given for three consecutive days. Continuous treatment was defined as a scheduled administration of antiemetics according to their duration of action, as opposed to administration as needed. The QI analysis was restricted to episodes with an initial IPOS >0; episodes with missing data or without symptom burden at baseline were excluded.
Statistics
Statistical analyses were conducted comparing patient characteristics and study endpoints. Normality was tested with the Shapiro–Wilk test. Descriptive statistics were used to summarize continuous variables (median, range) and categorical variables (frequencies, percentages). For group comparison, the Wilcoxon rank-sum test (primary endpoint, duration of symptom burden) and chi-squared test (QI) were used. Pearson’s chi-squared test compared categorical variables. A one-sided Wilcoxon rank-sum test was performed to compare improvement regarding symptom burden. Analyses were conducted using R (version 4.4.1 2024-06-14). The significance level was set to α < 0.01, accounting for multiple testing.
Ethics approval
The study was approved by the local research ethics committee of the Medical Faculty at LMU Munich (No. 24-0616).
Results
A total of 389 (Phase 1) and 316 (Phase 2) patients were screened, of whom 330 and 280 met the inclusion criteria (Fig. 1). Around half of the patients experienced symptoms in each group, of which more than half of the patients suffered from nausea only (96/172, 55.8% vs. 74/139, 53.2%) (Fig. 1).
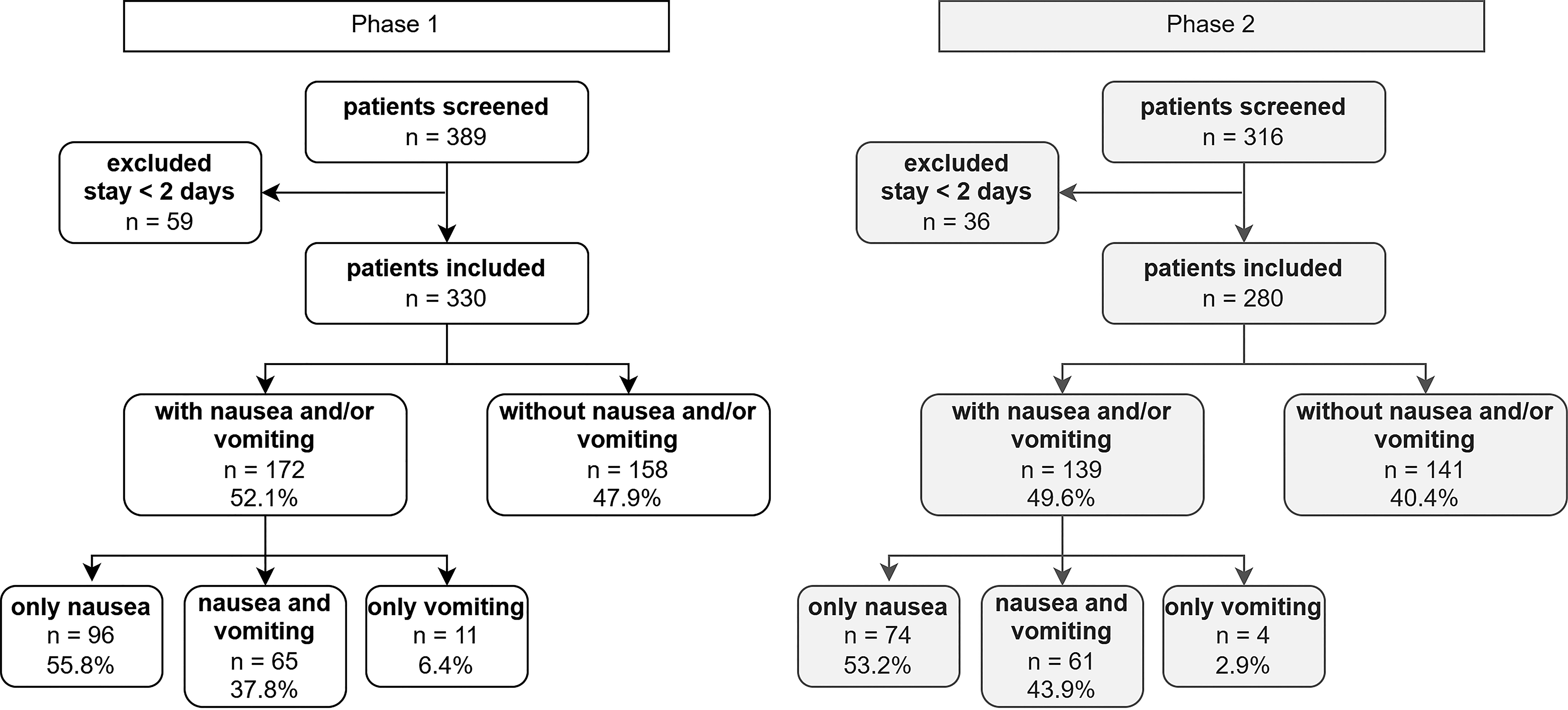
Patient flowchart.
Demographic data and disease characteristics of symptomatic patients are shown in Table 1.
Demographic Data and Characteristics of the Patients with Nausea/Vomiting
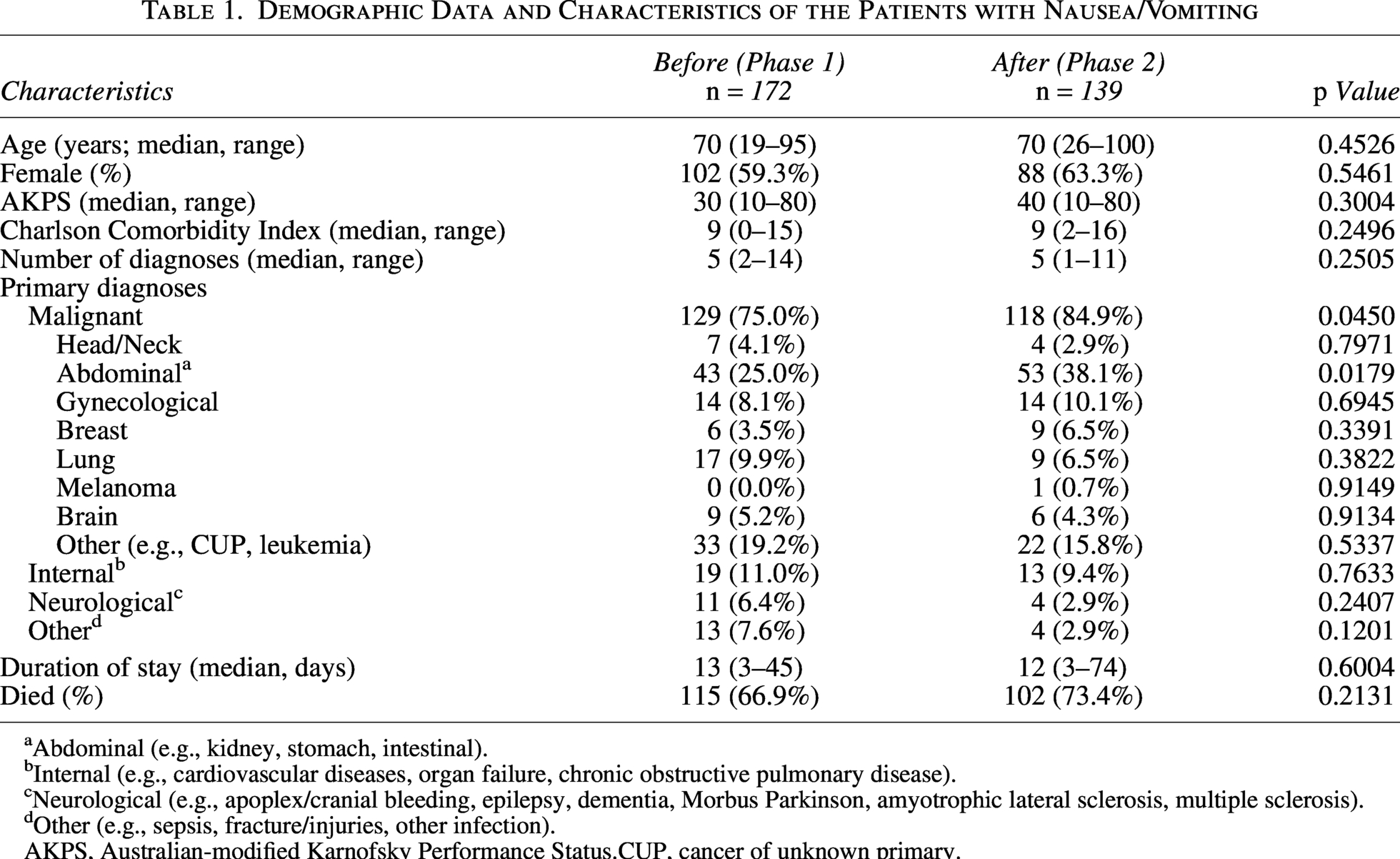
Abdominal (e.g., kidney, stomach, intestinal).
Internal (e.g., cardiovascular diseases, organ failure, chronic obstructive pulmonary disease).
Neurological (e.g., apoplex/cranial bleeding, epilepsy, dementia, Morbus Parkinson, amyotrophic lateral sclerosis, multiple sclerosis).
Other (e.g., sepsis, fracture/injuries, other infection).
AKPS, Australian-modified Karnofsky Performance Status.CUP, cancer of unknown primary.
In both groups, the median age was 70 years, with a median CCI of 9. The majority of symptomatic patients were female and had an underlying malignancy. No significant differences were found between the two phases regarding demographic and clinical parameters. The developed pathway was utilized in 104/139 patients (74.8%, only Phase 2). Nonuse mainly occurred during short stays or around weekends/holidays, likely due to physicians’ time constraints. Overall, 230 treatment episodes were documented in 172 patients in Phase 1 (median 1 per patient), compared to 178 episodes (139 patients) in Phase 2 (median 1, p = 0.5163). Complete data on symptom burden were documented for 178/230 versus 156/178 episodes, respectively.
Suspected etiology and respective treatment
In Phase 1, no etiology was documented in 26% of patients, whereas this proportion decreased to under 10% in Phase 2 (p < 0.001). The most frequently suspected etiologies were gastrointestinal causes, namely malignant intestinal obstruction or hypomotility (Table 2A). Multifactorial causes were not documented in Phase 1; however, in Phase 2, a multifactorial nature was suspected as the etiology in 17/178 cases (9.6%). As patients did not receive further chemotherapy after admission to the palliative care unit, chemotherapy-induced nausea and vomiting (CINV) played an insignificant role and were only suspected in very few cases, potentially due to delayed nausea/vomiting.
Suggested Etiology (A) and Prescribed Continuous Treatment (B) for Nausea and Vomiting
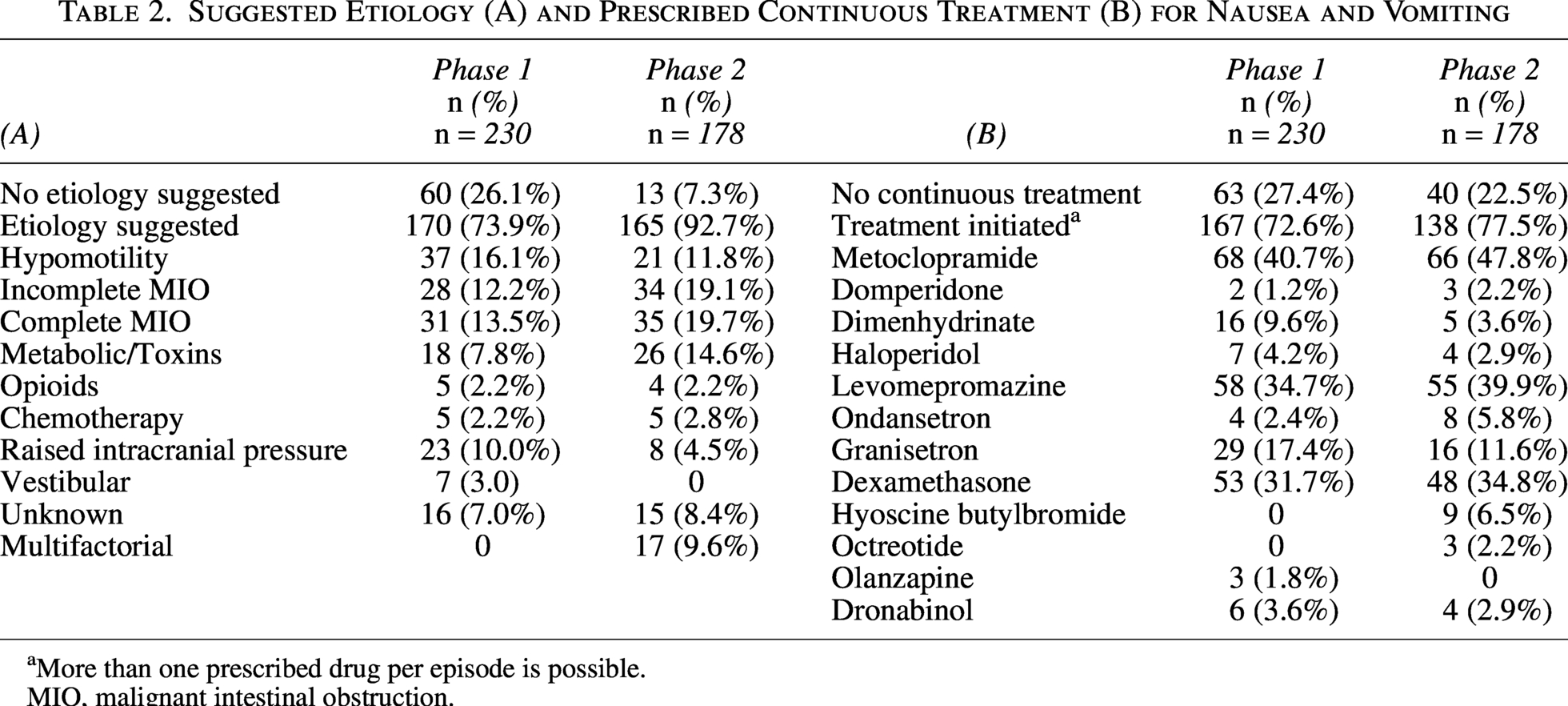
More than one prescribed drug per episode is possible.
MIO, malignant intestinal obstruction.
Table 2B describes the initiated antiemetic treatment. In Phase 1, at least one antiemetic was prescribed in 167/230 episodes (72.6%), increasing slightly to 138/178 patients (77.5%, Phase 2). Of those receiving antiemetic treatment, combination therapy with more than one antiemetic at a time was required in 96/167 (57.5%) and 68/138 (49.2%) episodes, respectively (p = 0.1523). Metoclopramide was the most commonly prescribed, followed by levomepromazine and dexamethasone, each administered to approximately one-third in both groups. Notably, the use of dimenhydrinate (equivalent to cyclizine) decreased in Phase 2. Additionally, antisecretory agents (hyoscine butylbromide and octreotide) were used exclusively in Phase 2 as antiemetics, while olanzapine was not prescribed there.
Guideline adherence significantly differed between the two phases. In Phase 1, the prescribed antiemetics matched the suspected etiology in 113/167 episodes, with continuous treatment (67.7%) according to the German palliative care guidelines. This increased to 128/138 episodes (92.8%) in Phase 2 (p < 0.001), compared to the etiology-based pathway. Rescue medication also showed improved adherence, with guideline-concordant prescribing in 127/221 (57.5%) versus 142/176 (80.7%) episodes (p < 0.001).
Symptom burden
Patients in both phases showed similar initial symptom burden (p = 0.4538 and 0.508 for nausea and vomiting, respectively). Figure 2 shows the change in nausea burden for all symptomatic patients with complete data. Distinct differences emerged between day 1 and day 3: In Phase 2, a higher proportion of patients shifted from higher to lower symptom burden, with many more achieving complete nausea resolution compared to the baseline period. Conversely, improvements in Phase 1 were less frequent and less pronounced. These patterns align with the statistical results, demonstrating significantly greater improvement in nausea in Phase 2 (p = 0.007). For vomiting, the difference did not reach the significance level (p = 0.021, α = 0.01), although the trend was consistent with the hypothesized direction, suggesting greater improvement in Phase 2.
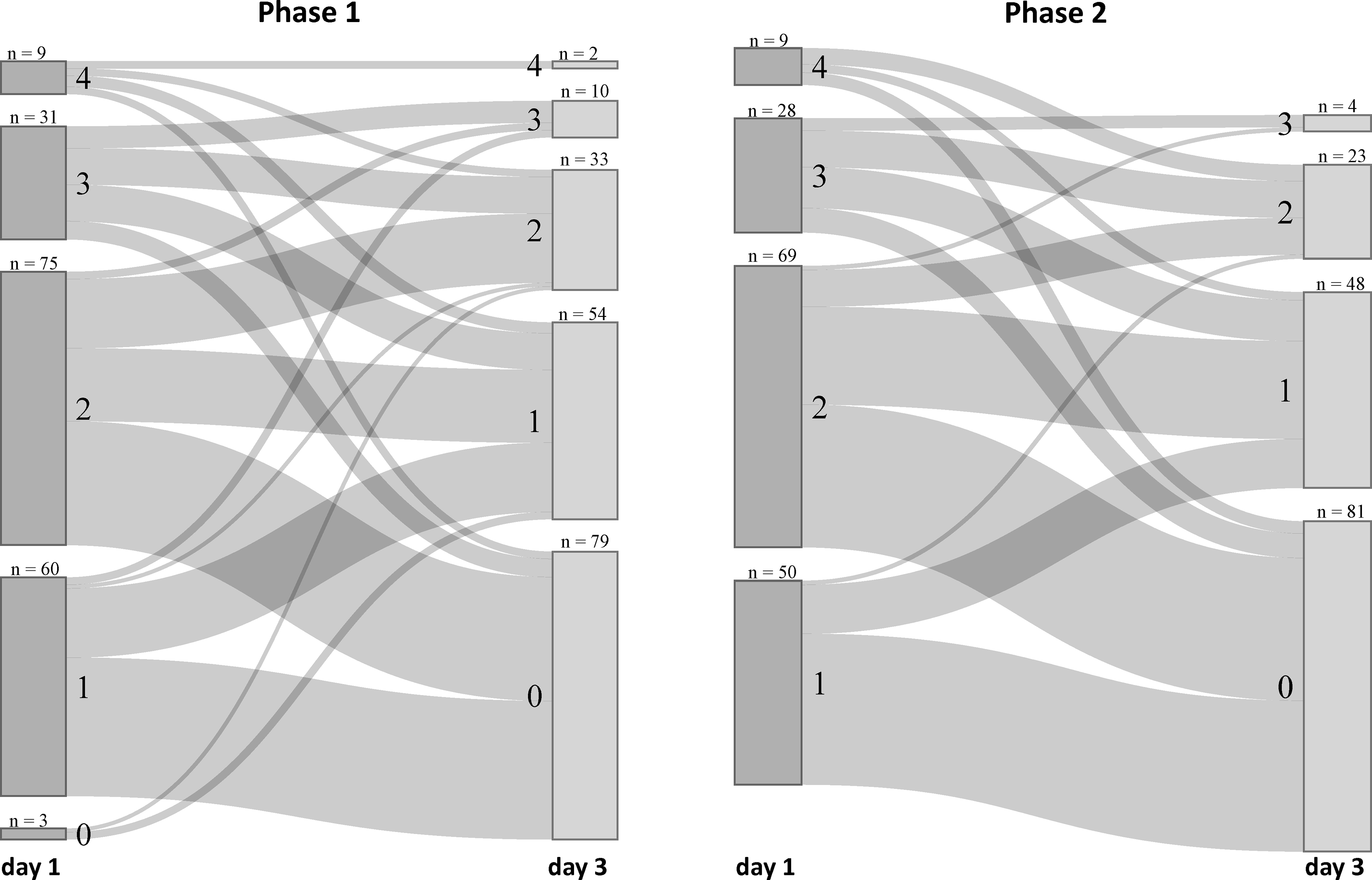
Changes in nausea symptom burden (IPOS) from day 1 to day 3 for Phase 1 (n = 178) and Phase 2 (n = 156). IPOS—0: no symptom burden, 4: highly affected by symptom. IPOS, Integrated Palliative Care Outcome Scale.
QI and duration of symptom burden
The QI showed a significant improvement for nausea between the phases after three and six days (Table 3). This improvement is mainly reflected in the subgroup of cancer patients (p = 0.0046), whereas no difference was observed for noncancer patients (p = 0.7020). For vomiting, the observed improvement after three days was not statistically significant (p = 0.0176; Table 3B).
Quality Indicator a over All Treatment Episodes
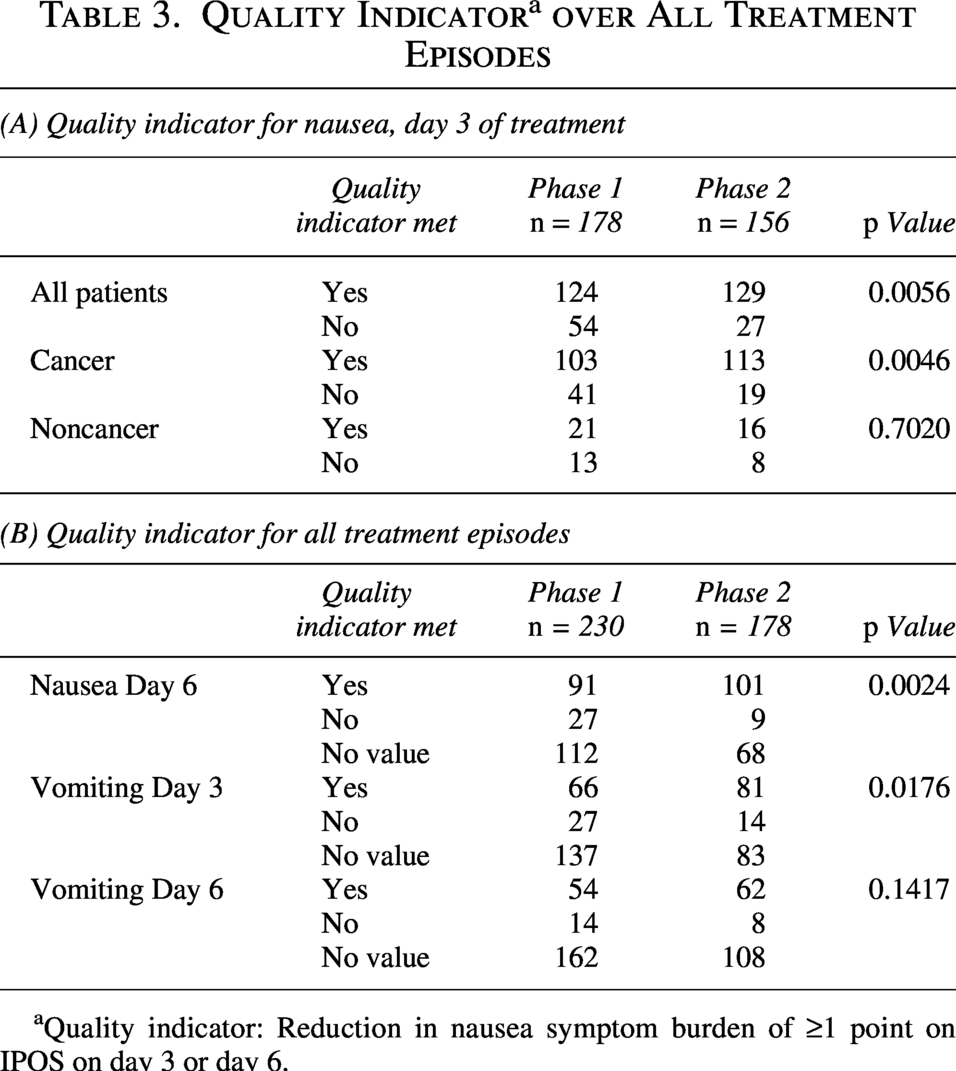
Quality indicator: Reduction in nausea symptom burden of ≥1 point on IPOS on day 3 or day 6.
In Phase 2, patients experienced a significantly shorter symptom duration for both nausea and vomiting (median 2 days vs. 3 days in Phase 1, p < 0.001, Fig. 3). Additionally, cases with prolonged episodes (>5 days) were significantly reduced (p = 0.0012). Subgroup analysis revealed a significant reduction in symptom duration for cancer patients (p < 0.001). For noncancer patients, the difference was not significant (p = 0.0582).
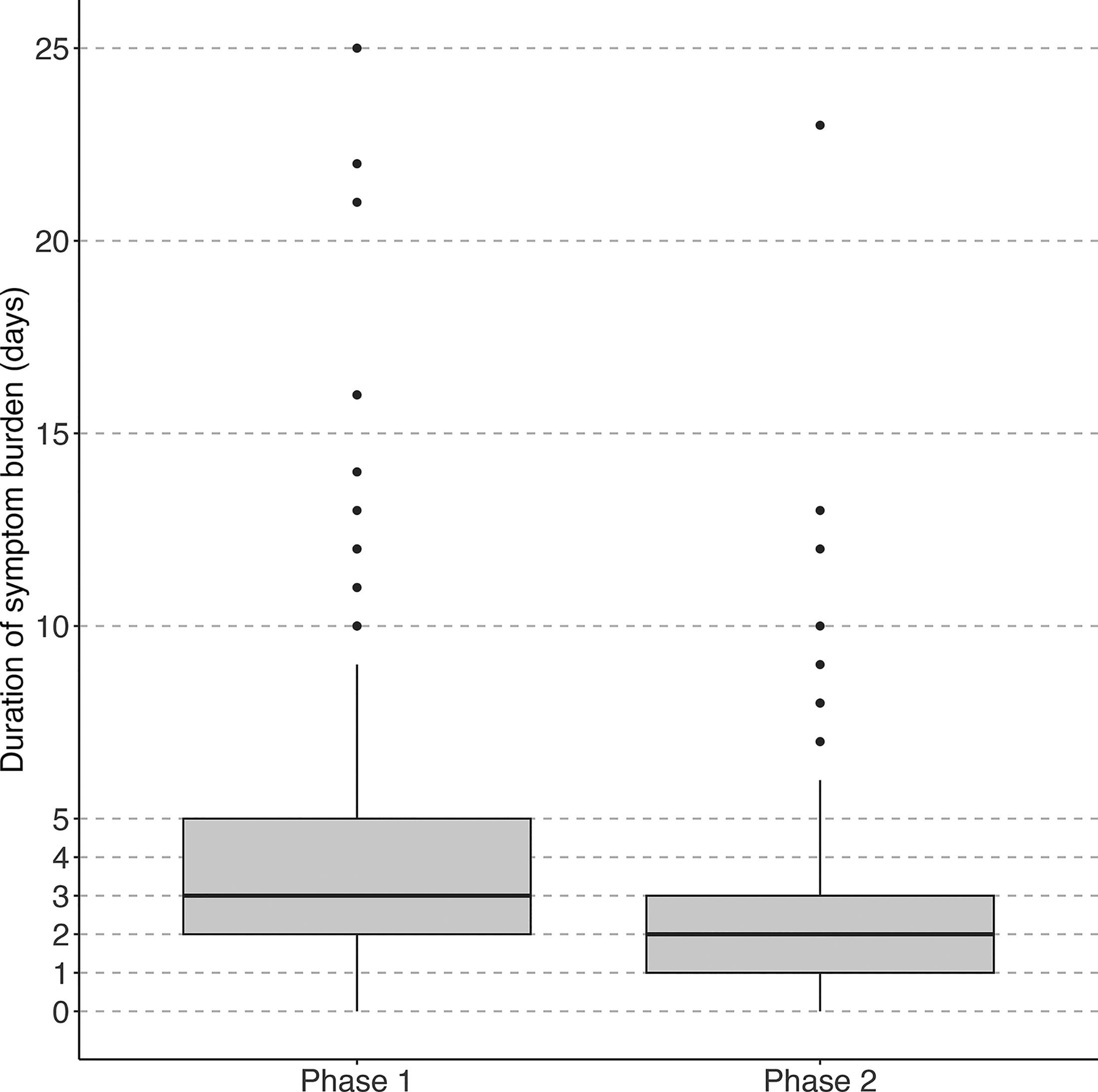
Duration of symptom burden (nausea and/or vomiting) in days (Phase 1 vs. Phase 2) for all patients.
Discussion
This study investigates the effect of a structured pathway on the treatment quality of nausea and vomiting in palliative care patients. Results indicate that the pathway is potentially superior to standard care, particularly for nausea. For vomiting, the observed improvement was not statistically significant. This approach was more effective in cancer patients.
Comparability of study groups and antiemetic treatment context
The study population was comparable to other palliative care studies regarding sociodemographic characteristics26,27 and proportion of symptomatic patients.2,12 However, these studies predominantly include cancer patients only.
Patients in both phases experienced similar nausea and vomiting burden at treatment initiation, supporting group comparability. Initial burden was consistent with previous findings, 2 where most patients were moderately affected. Even mild nausea can be very bothersome, 4 highlighting the need for rapid and effective treatment. Once again, these studies only included cancer patients, underscoring the evidence gap for noncancer patients. However, cancer patients and also females appear once more to be particularly prone to experiencing nausea and vomiting.1,2,26 Overall, the similarities between the groups ensure a valid comparison.
The pathway should be contextualized within palliative care, which differs from oncology-led prevention of CINV. Because patients in this study were no longer receiving chemotherapy, CINV-specific protocols and agents like neurokinin-1 (NK-1) receptor antagonists were not included. For CINV, the pathway referred to the current German guideline on supportive therapy. 28 Recommended drugs reflected the limited evidence base, guideline availability through late 2022, and local availability. Olanzapine is not yet established as an antiemetic in palliative care in Germany, where levomepromazine is often preferred due to lower cost and greater clinical experience. 29 As evidence grows for non-CINV palliative scenarios, 30 olanzapine and other emerging agents represent important candidates for future pathway updates.
The medication profile aligns with another study on guideline-based treatment effectiveness in patients with advanced cancer. 15 This study presented here does not assess antiemetic safety; this is discussed elsewhere. 31 However, potential safety risks remain relevant. For example, metoclopramide use often exceeds the recommended five-day limit in clinical practice. 32 Although this study did not assess treatment duration of single drugs, the pathway’s emphasis on reevaluation and de-escalation may reduce unnecessary treatment and therefore enhance drug safety.
Impact of the pathway
The pathway was completed in almost three-quarters of symptomatic patients. Because it may have influenced physicians’ decisions even without documentation, no subgroup analysis by pathway completion was conducted.
Identifying the underlying cause of nausea and vomiting can be challenging.1,2,33 The etiology-based pathway helped to address this gap. The significantly lower proportion of episodes without documented etiology in Phase 2 suggests that its structure supported physicians in identifying the underlying cause. Notably, in Phase 2, a multifactorial cause was suspected in a relevant number of cases, although this is lower than other studies have suggested.2,15 Current palliative care guidelines rarely explicitly address the management of multifactorial causes and often imply a single etiology.7,9,34 Additionally, no clear evidence-based guidance exists for effective drug combinations, leaving physicians without structured support in these complex cases. The pathway acknowledges this gap and offers a practical approach by providing treatment options that also account for multifactorial causes.
With the pathway, patients experienced pronounced and clinically meaningful improvements regarding symptom control. This is reflected in the rapid reduction of nausea within the first days of treatment. The systematic approach more frequently provided a reliable route to total symptom resolution, even where statistical significance was not met. The clinical trend strongly favored the intervention group, showing a greater burden reduction and an increased proportion of patients meeting the QI in Phase 2. The overall symptom duration decreased significantly and reached clinical meaningfulness, which was particularly pronounced for cancer patients.
The number of cases with an undocumented symptom burden also decreased significantly, suggesting that the systematic nature of the structured pathway encourages consistent reflection and documentation, even with multiple physicians involved in patient care. This improves management clarity and ensures that antiemetic drugs are purposefully aligned with the suspected cause. This approach helped to decisively reduce the symptom burden, representing a clear enhancement in the quality of care provided. This, although not directly measured, is likely to have improved overall well-being.
Areas for improvement
Despite the overall positive impact of the pathway, this study leaves some questions. Although the vomiting burden decreased, the change was not statistically significant. Vomiting can fluctuate, and occasional appearance may distort the results when assessed at a predetermined point in time. Furthermore, vomiting may not be resolved by pharmacological measures alone, and physical causes (e.g., obstructions) should be considered, 35 particularly for intestinal obstruction. Early evaluation for nasogastric decompression may be beneficial, although there is little supporting evidence. 36 In cases without substantial clinical improvement, further investigation into underlying causes remains necessary, as promoted by the pathway.
The relatively low rate of multifactorial etiology suggests a need for more sensitive diagnostic triggers within the tool, to ensure no contributing factors are overlooked. Some patients with intractable symptoms may experience total nausea, a concept mentioned more often only recently,1,37 where nausea is severely impacted by psychosocial and spiritual distress. This potentially explains cases of particularly long symptom duration resisting pharmacological management. The pathway offers two key benefits for these cases: First, frequent reassessment may help the interprofessional team to address individual needs earlier. Second, specific recommendations for treatment selection, including pharmacodynamically sensible drug combinations, also provide decision-making aid for complex situations.
So far, mostly employed in cancer patients,15,33 the etiology-based approach showed no significant benefits for noncancer subgroups beyond a slight trend in symptom duration. This may reflect the small subgroup size, where cancer patients had a greater impact on the overall results. Additionally, the pathway may overlook specific factors unique to noncancer patients. Since most studies focus exclusively on palliative care cancer patients, factors contributing to symptom burden in noncancer patients remain poorly understood. Tailored research is needed for this growing population.
Strength and limitations
A major strength of this study is the low risk of selection bias, supporting realistic representation of palliative care patients in a German tertiary hospital. Crucially, the inclusion of noncancer patients broadens the evidence base for this under-researched population. Regarding limitations, the choice of a before-after design over a randomized controlled trial helped prevent knowledge contamination among the clinical staff, ensuring that Phase 1 truly represented the status quo. Furthermore, as a single-center study conducted in an inpatient setting, the findings may not be directly transferable to the community setting, where close monitoring—as promoted by the pathway—and consecutive treatment adaptation might be challenging. This requires follow-up projects, investigating the effectiveness in this setting. Additionally, the retrospective design limits data accuracy, which depends heavily on the documentation quality. To address this, treatment decisions were recorded directly on the pathway, promoting consistent and reliable data capture. Although the use of proxy-reported outcomes in some cases is a challenge, strict separation of patient- and proxy-reported data in the evaluation ensured the precision of the IPOS.
Conclusion
This study demonstrates that a systematic, etiology-based approach greatly improves the treatment quality for nausea and possibly vomiting, leading to faster symptom relief. While such an approach is favored by most international guidelines, it has also been questioned. A study comparing a single-agent approach using levomepromazine versus haloperidol found symptom reduction in palliative cancer patients in nearly 70%, 38 and when comparing haloperidol to a guideline-driven treatment, no differences were found after 72 hours. 33 Additionally, one study reported that 43% of patients had no identified nausea etiology, yet 70% experienced symptom relief after 5–9 days. 2 The three studies, however, only included patients with far-advanced cancer. This raises important questions: Is identifying the etiology really essential or could a simpler, single-agent approach be a more practical alternative in clinical settings? To the authors’ knowledge, no further published studies have explored this approach. Future research should compare etiology-based and simplified single-agent treatment strategies while also investigating tailored interventions for noncancer patients. Until then, individualized treatment and sound knowledge of antiemetic pharmacology remain essential.
Ethical Considerations
The study was approved by the local research ethics committee of the Medical Faculty at LMU Munich (No. 24-0616).
Consent to Participate
Due to the retrospective nature of this study, participants did not need to consent. This was approved by the research ethics committee.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Authors’ Contributions
J.M.B.-S., C.B., and C.R. planned the study. J.M.B.-S. carried out the data collection with support of T.A. J.M.B.-S. and A.B.-S. carried out the data analysis. The article was written by J.M.B.-S., proof-read by C.B. and C.R., and approved by all coauthors.
Footnotes
Acknowledgments
The authors would like to thank Sophia Austermann, MD; Christina Hepperle, MD; Clemens Wittmann, MD; and Hamid Akifi, MD, for their professional advice during the development of the pathway and their support while implementing it in the study setting. Furthermore, they want to acknowledge the support of the Doctoral Program Clinical Pharmacy by the Stiftung Patient und Klinische Pharmazie, Munich, Germany.
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
This research received no funding/grant from any funding agency in the public, commercial, or not-for-profit sectors.