
Abstract
Suicidal ideation (SI) is a complex phenomenon occurring across populations and is especially prevalent among patients with serious illness. Palliative care (PC) clinicians often care for patients at elevated risk for SI and are well positioned to identify and respond to suicidality. Clinical encounters may require distinguishing passive wishes for death from active suicidal intent, addressing modifiable sources of suffering, and supporting patients and families through emotionally complex conversations. Practical, evidence-informed guidance can help clinicians approach these encounters with greater clarity and confidence. In this article, an interdisciplinary group of PC, psychiatry, psychology, social work, and chaplaincy clinicians shares ten tips for caring for patients with serious illness who experience SI.
Introduction
People living with serious illness face compounding physical, psychosocial, spiritual, existential, and financial stressors. These stressors place seriously ill patients at risk for the development or exacerbation of underlying major depressive and anxiety disorders, as well as other psychological conditions. 1 Seriously ill patients may also experience feelings of demoralization, isolation, and hopelessness, the last of which is strongly associated with suicidality.1–3
Suicidality—encompassing ideation, intent, and behavior—impacts patients with serious illness disproportionately. The global lifetime prevalence of suicidal ideation (SI) is thought to be around 9% in the general population versus 14–15% in those with serious illness.4–6 One study in older adults with serious illness found that they were three times more likely to report SI than those without serious illness. 7 Completed suicide rates are likewise higher in seriously ill patients (21.6–39.7 per 100,000 person-years) compared with the general population (14.2–16.7 per 100,000 person-years).8–11
Addressing suicidality can be challenging for a number of reasons. In many cultures, there is stigma associated with mental illness, and discussions of self-injury, suicide, and death are considered taboo.12–14 Additionally, clinicians may be concerned that asking patients about SI may worsen risk of suicide (see Tip #2), or they may feel undertrained to initiate such conversations. 15
Identifying patients at risk for suicidality can also be difficult. Depressive symptoms and suicidality have a strong bidirectional relationship, and psychiatric interventions can reduce suicidal thoughts and behaviors when patients receive appropriate care.16–18 However, suicidality should not be assumed to occur only in the setting of depression or another known psychiatric diagnosis, such as substance use disorders, personality disorders, psychotic disorders, or trauma-related disorders. Studies suggest that 12–20% of people who attempt suicide have no preceding psychiatric diagnosis. 19 Among patients with serious illness, suicidality may reflect multiple converging factors, including the stressors listed above, as well as psychiatric illness, uncontrolled physical symptoms, cultural context, and the burdens of illness itself.1–3,20,21 It is therefore important that clinicians assess suicidality directly rather than relying on depression screening or psychiatric history alone.
Given their expertise and care of seriously ill patients at heightened risk for SI, palliative care (PC) clinicians are uniquely positioned to identify suicidality and initiate appropriate support. In this article, we share our top ten tips for PC clinicians evaluating and caring for patients with serious illness who experience SI.
Tip 1: Patients with Serious Illness, Especially Cancer, Are More Likely to Experience Suicidality Compared to the General Population, Warranting SI Screening for All Patients Receiving PC
Patients with serious illness are at a several-fold higher risk of suicidality compared with the general population.4–11 Sub-populations at highest risk are those with malignancy of any kind, as well as other chronic gastrointestinal, hematological, pulmonary, and neurological conditions. Risk increases with disease comorbidity.22–26
Personal or family history of depression or suicide, trauma or adverse childhood experiences, substance use, and limited social support all increase suicide risk.27,28 These factors, when compounded with serious illness, leave this population particularly vulnerable to suicidality. 3 SI can emerge at any point in the course of a serious illness, though a particularly high-risk time is the six months following diagnosis. This is especially true for patients with cancer, where the risk of death is up to seven times higher during this period.10,11,29,30 SI may also persist through end of life. One study reported that, in a population of 88 veterans receiving home hospice, 34% were depressed and 14% experienced SI. 31
For these reasons, PC clinicians should screen for SI early and at clinically meaningful intervals, including after diagnosis, disease progression, major functional decline, uncontrolled symptoms, transitions in care, or expressions of hopelessness. Screening should include risk and protective factors such as connectedness, sense of purpose, social support, spiritual or cultural beliefs, prior trauma, substance use, and psychiatric history. Validated tools, including the Patient Health Questionnaire-9 (PHQ-9), can help identify coexisting depressive symptoms; however, depression screening alone is not sufficient to assess suicide risk. 32
Tip 2: Asking About SI is Critical and Saves Lives; Avoiding These Conversations Contributes to Stigma and At-Risk Patients May Not Receive Appropriate Care
A common barrier to SI assessment is the misconception that asking about suicide may trigger or worsen suicidal thoughts. Evidence does not support this concern. 15 Direct, calm, and nonjudgmental questions about SI can help identify patients who might otherwise remain silent. Many people with SI experience shame or difficulty seeking help. Fewer than half disclose SI or suicidal behavior to others, and disclosure rates are even lower among people who subsequently die by suicide. 33
PC clinicians can normalize the question while still asking it clearly. For example: “I sometimes hear from patients that they’re having thoughts about death, suicide, or not wanting to keep living. Has that been part of your experience?” Other patients may need a more direct question: “Have you had thoughts about ending your life?” Asking in this way communicates that suicidality is something the clinical team can hear, discuss, and address. Patients are more likely to disclose SI when clinicians are calm, empathic, and nonjudgmental. 34 Avoiding the topic can reinforce stigma and leave at-risk patients without appropriate support.
Tip 3: Differentiate Between Active SI, Passive SI, and the Expression of Suffering, as This Distinction Will Change the Clinical Management Plan
Patients with serious illness may express thoughts about death in different ways, and the distinction has important implications for assessment and care (Table 1). A passive death wish refers to a desire to be dead or for suffering to end, without thoughts of causing one’s own death. Patients may say they are “ready for this to be over” or, for those with religious beliefs, they may express hope that “God will take me home.” These statements may reflect existential distress, demoralization, uncontrolled symptoms, or acceptance of approaching death, but they do not necessarily indicate suicidal intent.
Summary of Relevant Terms Regarding Suicidal and Self-Injurious Thoughts and Behaviors
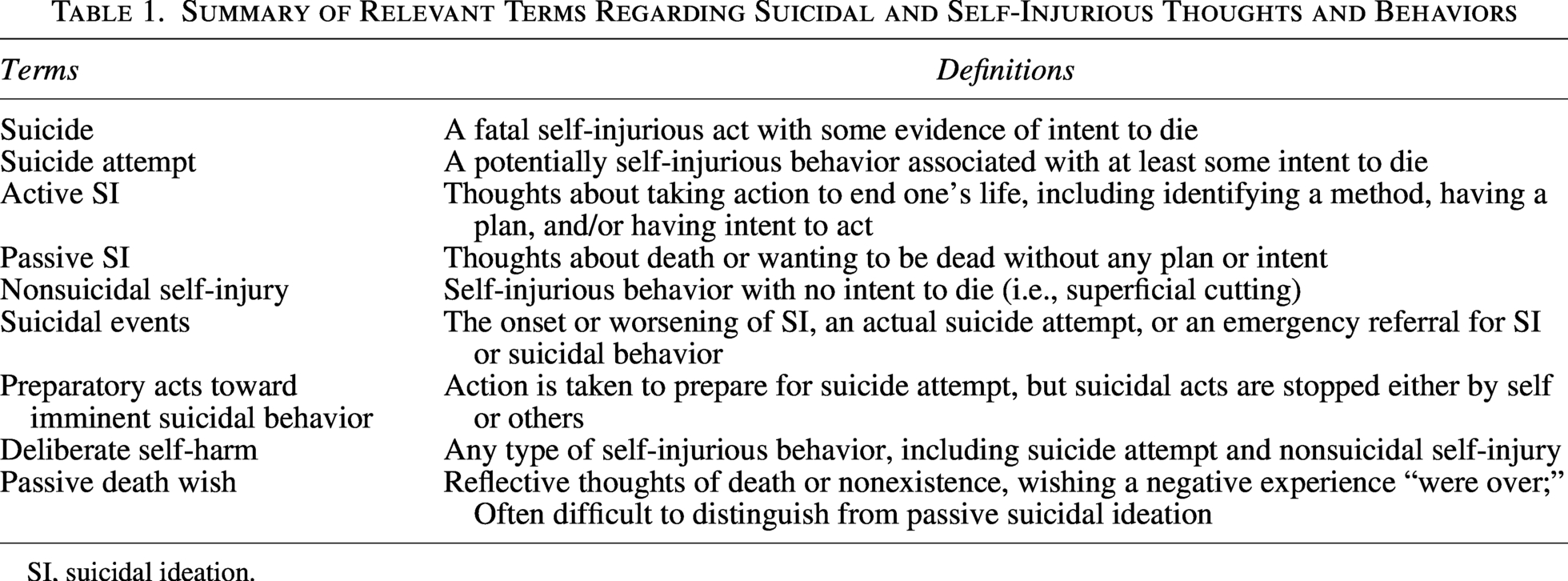
SI, suicidal ideation.
Passive SI goes a step further. It involves thoughts of killing oneself or causing one’s own death, but without a specific plan, preparatory behavior, or intent to act. Active SI involves thoughts of suicide with some combination of method, plan, intent, access to means, or preparatory behavior. Clinicians can clarify acuity by asking directly: “Have you thought about ending your life?” “Have you thought about how you would do it?” “Do you feel at risk of acting on these thoughts?” and “Have you taken any steps to prepare, such as gathering medications, writing a note, or giving things away?”
This distinction guides the clinical response. Active SI generally requires urgent safety assessment, means restriction, close supervision, crisis services, and, in some cases, psychiatric hospitalization (see Tip #6). Passive SI without plan or intent may be managed outpatient when protective factors, supervision, and follow-up are sufficient. However, it still requires careful assessment and treatment of contributing factors such as pain, depression, anxiety, demoralization, isolation, and other sources of suffering. 35 Passive death wishes also warrant exploration of the patient’s symptoms, values, supports, and sources of distress. In one study of 200 seriously ill patients, 45% reported occasional wishes for death, but only 9% endorsed a serious and persistent desire to die. 36 Similarly, among patients with advanced cancer, 10% made a desire-for-death statement, which was associated with lower well-being, higher rates of depression, and greater symptom burden on the Edmonton Symptom Assessment Scale.37,38 These data underscore that expressions of wanting death may be common in serious illness, but their meaning, acuity, and clinical implications vary.
Tip 4: Employ Validated Questionnaires, Including the Columbia-Suicide Severity Rating Scale and PHQ-9, to Assess and Trend Symptom Burden
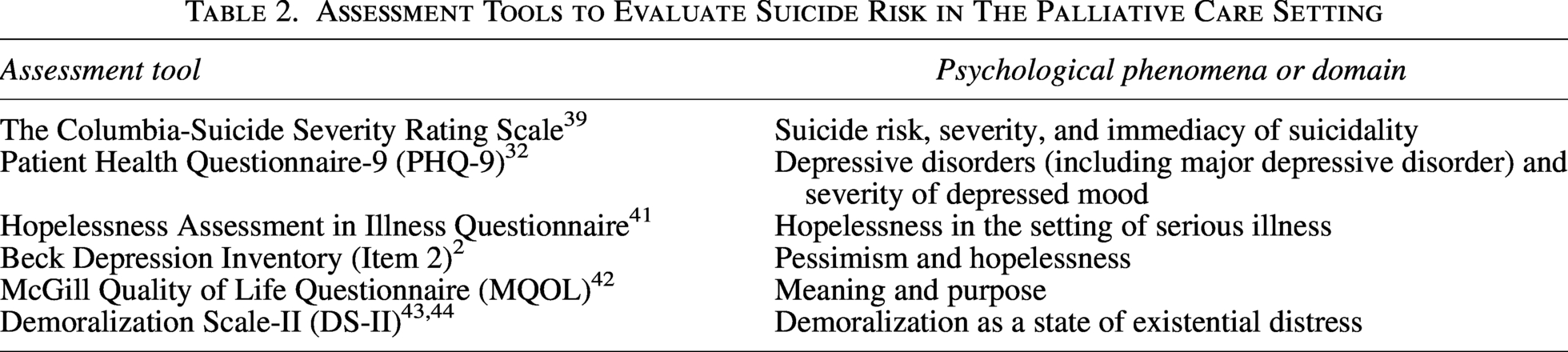
Validated tools can help PC clinicians clarify suicide risk, assess acuity, and track changes over time, but they should supplement rather than replace direct conversation and clinical judgment. The Columbia-Suicide Severity Rating Scale can help characterize suicidal ideation, intent, behavior, and preparatory acts. 39 The PHQ-9 can identify co-occurring depressive symptoms, although depression screening alone is not sufficient to assess suicide risk. 32
Because suicidality in serious illness may be shaped by hopelessness, demoralization, loss of meaning, and diminished quality of life, clinicians may also use tools that assess these domains.2,40 Table 2 summarizes validated measures that can help guide assessment and interdisciplinary care.2,32,39,41–44
Assessment Tools to Evaluate Suicide Risk in The Palliative Care Setting
Tip 5: Skip the Contract: Use Evidence-Based Strategies to Lower Risk of Completed Suicide Among Those with SI
A “no-suicide” contract asks a patient to contact the care team rather than attempt suicide during acute SI. Although this approach may reassure clinicians, it lacks evidence for reducing suicide risk. 45 Evidence-based alternatives include means safety planning and structured safety planning interventions.
Means safety planning identifies potentially lethal means in the patient’s environment and develops strategies to reduce access. 46 For patients with SI who are prescribed opioids, for example, a care partner may hold and dispense medications to reduce overdose risk. Blister packs, timed-release dispensers, and lockboxes can also delay impulsive attempts. Similar strategies apply to firearms, knives, ropes, and other lethal means.
For patients with SI who do not require immediate hospitalization, teams may use the Stanley–Brown Safety Planning Intervention (SBSPI). 45 The SBSPI combines means safety planning with identification of warning signs, coping strategies, and supportive contacts. When paired with brief follow-up contacts focused on reassessment, safety plan review, and psychiatric care coordination, the intervention reduced suicidal behavior by up to 45% within six months compared with brief counseling and referral alone. 47
Tip 6: Know the Institutional and Community-Based Resources Available to Patients Which May Include Interdisciplinary Teams, Collaborative Care with Mental Health Professionals, Crisis Services, and More
Expressions of suicidality in serious illness reflect a complex web of personal history, relationships, and circumstance, warranting individualized responses supported by different professionals and resources. It is therefore within the purview of the PC clinician to have a working knowledge of available services and providers, both institutionally and within the greater community. 48
Institutional resources form the backbone of the SI response. Palliative social workers play a critical role as frontline mental health professionals, although supply is vastly outstripped by demand. Psychiatry and crisis response teams are important for emergent situations, and case managers are essential for complex care coordination. With patient consent, engaging primary care providers and subspecialists allows for more touchpoints and frequent opportunities to request help. Regardless of faith background, spiritual support from hospital chaplains or religious leaders can be invaluable.
Clinicians should also be familiar with community resources, including crisis hotlines, text lines, outpatient mental health services, peer support programs, support groups, and faith or community networks. These resources can expand support beyond the clinical encounter and help patients access care between visits or during periods of escalating distress. 49
Tip 7: Management Strategies for SI Include Aggressive Control of Physical Symptoms, Psychotherapy, and Medications Including Selective-Serotonin Reuptake Inhibitors and Serotonin-Norepinephrine Reuptake Inhibitors If Prognosis Permits; Emerging Literature Suggests a Potential Role for Psychedelics
For patients with SI in the setting of serious illness, treatment should target modifiable contributors such as depression, anxiety, demoralization, pain, insomnia, fatigue, isolation, and existential distress. Psychotherapy can be especially useful because it does not require oral medication and may provide faster benefit than pharmacologic treatment alone. Cognitive behavioral therapy (CBT), dialectical behavior therapy (DBT), and collaborative assessment and management of suicidality (CAMS) have evidence for reducing suicidal thoughts and behaviors. 16 CBT and DBT require specialized training, whereas CAMS may be more feasible for palliative mental health clinicians to incorporate with appropriate preparation. 50
Medications may also reduce symptom burden and suicide risk when prognosis allows time for benefit. 51 Selective-serotonin reuptake inhibitors, serotonin-norepinephrine reuptake inhibitors, and other antidepressants are generally most useful when prognosis is longer than several weeks. Medication choice should consider comorbid symptoms, adverse effects, prognosis, renal and hepatic function, and drug–drug interactions. For example, methylphenidate may be considered in selected patients with limited prognosis, fatigue, or opioid-associated sedation, and may also improve depressive symptoms. 52 Clinicians may prescribe within their scope of practice or collaborate with psychiatry when symptoms are severe, complex, or treatment-refractory (Table 3).
Pharmacotherapy for Major Depressive Disorder in Serious and Chronic Illness
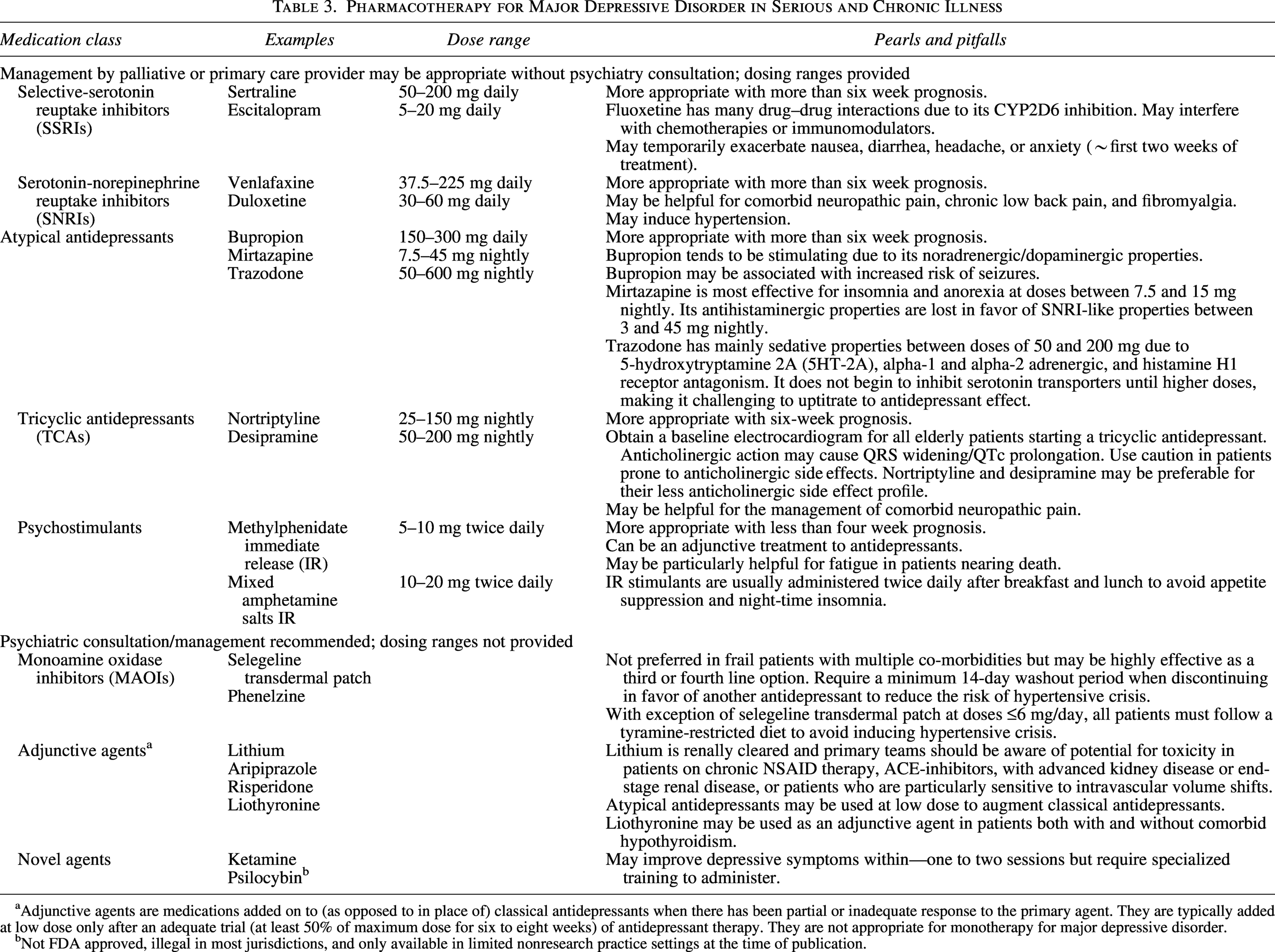
Adjunctive agents are medications added on to (as opposed to in place of) classical antidepressants when there has been partial or inadequate response to the primary agent. They are typically added at low dose only after an adequate trial (at least 50% of maximum dose for six to eight weeks) of antidepressant therapy. They are not appropriate for monotherapy for major depressive disorder.
Not FDA approved, illegal in most jurisdictions, and only available in limited nonresearch practice settings at the time of publication.
Interventional treatments may be appropriate for selected patients who need a more rapid response or have refractory symptoms. Electroconvulsive therapy, transcranial magnetic stimulation, intravenous ketamine, and intranasal esketamine may improve depressive symptoms more quickly than standard antidepressants in some patients, including those with serious illness, but require specialized assessment and delivery.17,51,53,54 Psilocybin-assisted psychotherapy remains investigational and is not legally available in most jurisdictions; it should be framed as an emerging area of research rather than a routine clinical option.55,56
Tip 8: In Pediatrics, There Are Several Unique Considerations and Challenges; Confidentiality is a Key Component of Providing High Quality Care to Adolescents, but Confidentiality Must be Broken If Safety is at Risk, Including for SI
Confidentiality is essential to high-quality adolescent care. It helps adolescents disclose sensitive information, including mental health concerns, without fear of a parent or guardian’s immediate reaction.57,58 However, confidentiality has limits when safety is at risk.
Clinicians should explain these limits before screening for SI so adolescents understand when disclosure to a parent, guardian, or other responsible adult may be necessary. Proactively naming the limits of confidentiality can help preserve trust even when disclosure becomes ethically or legally necessary. Although federal privacy regulations apply broadly, state laws governing adolescent confidentiality vary, and clinicians should know the relevant requirements in their jurisdiction. 59 Regardless of state-specific rules, imminent risk to the adolescent’s life generally requires breach of confidentiality and guardian involvement. 58 Safety planning may still be useful for adolescents with SI, but it should be adapted developmentally and paired with appropriate caregiver involvement when risk is present.
Tip 9: Care Must be Taken to Distinguish Between a Desire for Medical Aid in Dying (Where Legal) and SI in the Context of Mitigatable Factors
Clinicians must distinguish suicidality associated with psychiatric illness, physical, or existential distress from requests for medical aid in dying (MAID). While both involve a desire for death, their underlying motivations, clinical context, and levels of decisional capacity differ in essential ways. 60 Table 4 outlines the core differences between MAID requests and suicidality in the context of mental illness.
Distinguishing Features of Medical Aid in Dying Requests Versus Suicidality Related to Psychiatric Illness
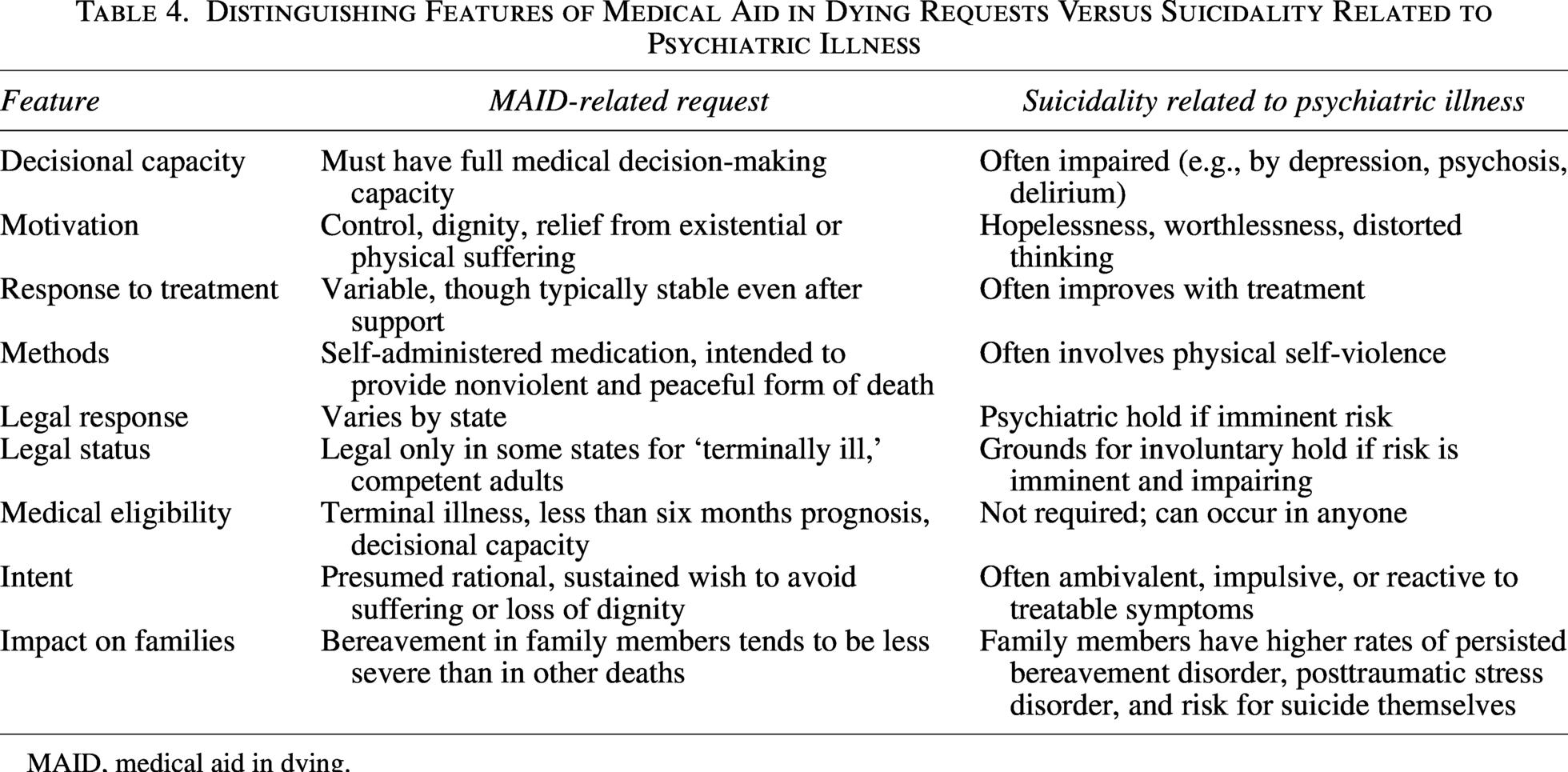
MAID, medical aid in dying.
Potential reversibility is a key differentiating clinical clue and is linked to motivation. Suicidality related to psychiatric illness often improves when distressing symptoms are effectively treated. Psychopathology, in contrast, appears to potentially play a limited role in documented MAID cases.61–63
Motivationally, suicide associated with psychiatric illness is most often a desperate attempt to escape psychological suffering. These acts are typically impulsive, shaped by cognitive distortions that impair judgment, often occur in private, and are characterized by shame, hopelessness, and ambivalence about living.4,64–70 By contrast, MAID requests arise in the setting of progressive medical decline and are usually deliberate, openly discussed, and framed as efforts to preserve autonomy, dignity, or control at life’s end.71,72 Importantly, this structure does not in itself confirm decisional soundness or the absence of psychopathology. Clinicians must remain vigilant for untreated depression, demoralization, or existential distress that may underlie a patient’s request and could resolve with appropriate care.
Tip 10: All Members of the Interdisciplinary Team Must Reflect on Their Experiences as Well as Their Biases, and They Must Care for Themselves and Their Colleagues, as They Navigate SI in Their Patients
Our own histories inform our practice with patients with SI. Stigmatizing attitudes must be avoided, as they can create barriers to adequate care. 73 Clinicians should be vigilant in their care, acknowledging that even those with good intentions can be susceptible to unconscious biases and fears.
It is similarly important for multidisciplinary team members to reflect on how the experience of caring for a patient with SI impacts them personally. Conversations about suicide are inherently difficult and may evoke anxiety, guilt, sadness, or fear of saying the wrong thing. Structured team discussion and debriefing can help clinicians process these responses and support one another. Senior clinicians can model vulnerability and self-reflection, which may reduce stigma and encourage trainees and junior team members to seek support when needed. 74 Ultimately, thoughtful self-care among clinicians can result in better outcomes for both patients and providers.
Conclusion
PC clinicians’ longitudinal patient relationships, frequent care of high-risk populations, and expertise in empathic communication make them well positioned to identify and assess suicidality with nuance. To do so effectively, clinicians should be trained in SI screening and acuity assessment; be familiar with safety planning, pharmacologic and psychotherapeutic interventions, relevant laws, and local resources; and be prepared to support patients, colleagues, and themselves in this emotionally demanding and clinically important work.
Authors’ Contributions
E.P.T. developed the concept for the paper. Each author wrote one tip and had the opportunity to review and edit the final article. R.L. also wrote the abstract, introduction, and conclusion. C.O., G.A.R.-W., and N.S. each contributed significantly to a second tip and developed the tables. All of the named authors above reviewed and edited the article several times for content, length, grammar, and flow.
Ethical Considerations
There are no human participants in this article. Informed consent is not required.
Footnotes
Acknowledgments
The authors are grateful to the patients whose experiences prompted the reflections that ultimately resulted in this work.
Author Disclosure Statement
OpenEvidence, a generative AI tool, was utilized for assistance with literature review, but for no other purposes. G.R.-W. serves as a section editor for the Journal of Palliative Medicine. No other authors have any conflicts to disclose.
Funding Information
No funding was required for this article.