
Abstract
Background:
End-of-life dreams and visions (ELDVs) are vivid, often subjective experiences that occur during the dying process. Even though the patient and family experiences of ELDVs are well documented, there is limited knowledge regarding the perspectives, preparedness, and perceived needs of health care professionals. ELDVs also remain insufficiently addressed in clinical care.
Objective:
To describe how frequently clinicians encounter ELDVs, perceived preparedness/training, and approaches to clinician and family education and communication.
Methods:
We conducted a survey to explore health care professional’s perspectives and experiences surrounding ELDVs. The Checklist for Reporting Results of internet E-Surveys was followed. Our survey included 30 items across 7 sections. Professionals that take care of patients with serious or terminal illness were eligible for the study. We utilized a structured multimodal dissemination to achieve maximum diversity in participants.
Results:
Briefly, 247 participants were eligible for analysis. Frequent encounters for ELDVs were reported by participants. Participants perceived positive effects on patients more frequently than negative effects (W = 446.0, p < 0.001, r = 0.64). Clinical challenges were rated differently across categories (χ2 = 160.97, p < 0.001, Kendall’s W = 0.13). The most commonly endorsed clinical challenges were lack of institutional protocols and lack of standardized diagnostic criteria, both rated significantly higher than all other challenges (Bonferroni-corrected Wilcoxon tests: All p < 0.001). Participants endorsed multidisciplinary involvement and formal policy implementation.
Conclusion:
ELDVs are common, but clinicians feel underprepared to respond to them. There is a need for structured training and institutional protocols. Future studies should include patients and their families and analyze how their experiences are shaped by physician responses.
Keywords
Key Message
End-of-life dreams and visions (ELDVs) are common, clinically relevant experiences that may influence emotional, existential, and spiritual well-being near death. Despite frequent encounters, clinicians report limited preparedness to address ELDVs, highlighting the need for education, guidance, and interdisciplinary approaches within routine palliative care.
Introduction
End-of-life dreams and visions (ELDVs) are vivid, emotionally subjective experiences that commonly occur during the dying process. These experiences may involve deceased loved ones, spiritual figures, or comforting imagery and are frequently described by patients and families as meaningful and reassuring. Importantly, ELDVs are phenomenologically distinguishable from delirium, though the distinction can be clinically challenging. ELDVs are typically coherent, emotionally congruent, and often reported by individuals without obvious cognitive impairment. They occur due to neurocognitive changes and help with meaning-making and preparation for death. 1
Research has confirmed the prevalence, content, and impact of ELDVs in hospice and palliative care populations. Kerr et al. 2 conducted a longitudinal study revealing that up to 88% of hospice patients reported ELDVs, often describing them as a source of peace, closure, or spiritual connection. Other studies have reinforced these findings, documenting a wide range of themes, including reunion, transition, and forgiveness.3–5 Recent analyses suggest that ELDVs may also contribute to posttraumatic growth in bereaved caregivers and health care workers, highlighting their broader psychosocial impact.4,6–8
Despite their frequency and reported significance, ELDVs remain underrecognized and insufficiently addressed in clinical care. Although family caregivers often view ELDVs as meaningful, few institutions offer formal guidance on how to document, discuss, or support these phenomena. 9
Evidence suggests a persistent gap between physicians’ positive attitudes toward spirituality and their routine practice of taking spiritual histories.10–14 Koenig 10 has noted that, although spiritual beliefs frequently influence patients’ coping and decision-making, clinicians often lack the training to address them.
There is a gap between the recognized significance of ELDVs and their integration into clinical practice. While the patient and family experiences of ELDVs are well-documented, little is known about the perspectives, preparedness, and perceived needs of health care professionals. To address this gap, we conducted a multinational cross-sectional survey of palliative care professionals to examine their knowledge, experiences, and attitudes regarding ELDVs.
This study aimed to explore (1) how frequently clinicians encounter ELDVs, (2) their capacity to differentiate ELDVs from delirium, (3) the extent of training and institutional guidance available, and (4) preferred approaches to education, documentation, and family communication related to ELDVs.
Methods
We conducted a cross-sectional, anonymous, web-based survey to explore health care professionals’ (HCPs) perspectives, beliefs, and experiences surrounding ELDVs. The study followed the Checklist for Reporting Results of internet E-Surveys to ensure methodological rigor, transparency, and completeness of reporting. The survey was created and deployed using the SurveyMonkey® platform.
Survey development and theoretical framework
The survey instrument was developed through an iterative process informed by prior literature on ELDVs and clinics. In particular, the development of the instrument was guided by the concept of “total pain.” 15 Based on this conceptual foundation and prior empirical studies on ELDVs, the survey was designed to measure four key constructs relevant to clinical practice: (1) clinical exposure and phenomenology of ELDVs, (2) clinicians’ interpretive attitudes toward these experiences, (3) perceived clinical and diagnostic challenges, particularly the differentiation of ELDVs from delirium or hallucinations, and (4) system-level preparedness, including training needs, interdisciplinary collaboration, and institutional policies.
Draft questions were developed collaboratively by a multidisciplinary research group consisting of clinicians and researchers with expertise in geriatrics, palliative care, medical humanities, and spirituality in health care. The preliminary item pool was evaluated for conceptual clarity, redundancy, and clinical relevance. The resulting questionnaire consisted of 30 items organized into seven thematic sections (not to be interpreted as validated constructs).
Most items were structured as 5-point Likert-scale questions to assess agreement or frequency. Additional multiple-choice questions and optional open-text fields were included to capture contextual information and qualitative perspectives. Prior to dissemination, the survey underwent pilot testing with five health care professionals representing disciplines commonly involved in end-of-life care. Participants were asked to provide feedback on wording, response categories, and overall survey length. Based on this feedback, several items were rephrased to improve clarity, overlapping response categories were adjusted, and redundant items were eliminated. The final survey was designed to last approximately seven to eight minutes.
Participants and eligibility criteria
Participants were eligible if they were actively engaged in the care of patients with serious or terminal illness, including professionals in geriatrics, palliative care, oncology, and related disciplines. Eligible professions include physicians, nurses, chaplains, psychologists, social workers, and allied health care providers. Participation was voluntary.
A multimodal dissemination strategy was implemented to maximize diversity: Distribution through academic institutions and palliative care centers, professional societies, editorial networks, and a LinkedIn campaign. Data collection remained open for 60 days.
Ethics and data protection
This study involved only health care professionals and did not engage any of the ethical concerns outlined in the European Commission’s Horizon 2020 Program Guidance on completing an ethics self-assessment.
All data were anonymized, securely stored in encrypted form on a password-protected institutional server, and handled in accordance with the General Data Protection Regulation (GDPR).
Statistical analysis
All statistical analyses were conducted using Python. Only fully completed questionnaires were retained for analysis. Participants with extreme durations (i.e., defined as values below the 4th percentile or above the 96th percentile of the completion time distribution) were removed.
Geographic location was inferred from participants’ Internet Protocol (IP) addresses to estimate country-level distributions. Because this method does not allow precise verification of participant location, these estimates were used descriptively and interpreted with caution.
Open-text responses, including those describing professional role, clinical setting, and religious affiliation, as well as several items in Sections 2–7, were systematically reviewed. Similar responses were grouped into higher-order categories.
Descriptive statistics were computed for all variables. Categorical and demographic data are reported as absolute and relative frequencies (n, %). For Likert-scale items, which were treated as ordinal variables, descriptive summaries include the median, first quartile (Q1), third quartile (Q3), and interquartile range (IQR).
Inferential analyses were conducted using nonparametric tests due to the ordinal nature of the data and the absence of normality assumptions. Paired comparisons between two related items were tested using the Wilcoxon signed-rank test, while comparisons involving more than two related items were evaluated using the Friedman test. When appropriate, post hoc pairwise Wilcoxon tests with Bonferroni correction were applied to adjust for multiple comparisons. All statistical tests were two-tailed, and results were considered statistically significant at an adjusted α = 0.05, unless specified otherwise.
We conducted post hoc exploratory group comparisons across four variables: Profession, clinical setting, years of clinical experience, and geographic region (only groups with n ≥ 30). For each survey item, we fitted an Ordinary Least Squares (OLS) regression model with all four grouping variables entered simultaneously as predictors (N = 170). These analyses were exploratory and not pre-specified; p values are reported as descriptive indicators only. Full results are provided in the Supplementary Data.
Results
Participants
Of the 303 questionnaires submitted, 271 were fully completed (89%). Incomplete responses were excluded from the dataset. An additional 24 participants were removed due to atypical completion times, below three minutes (n = 12, 4%) or above 30 minutes (n = 12, 4%). The final sample consisted of 247 participants, who required, on average, seven and a half minutes to complete the questionnaire.
Participants were located across multiple world regions. Most participants were based in North America (n = 151, 61.1%), followed by Asia (n = 41, 16.6%), and Europe (n = 35, 14.2%). Smaller proportions of participants were in Africa (n = 19, 7.7%) and South America (n = 1, 0.4%).
About half of the participants identified as Christian (n = 126, 51.0%). Smaller proportions reported being spiritual but not formally religious (n = 29, 11.7%), Hindu (n = 27, 10.9%), Muslim (n = 21, 8.5%), atheist or agnostic (n = 20, 8.1%), Jewish (n = 14, 5.7%), and Buddhist (n = 10, 4.0%). The majority of participants were physicians (n = 166, 67.2%), followed by nurses (n = 30, 12.1%) and advanced practice providers, including nurse practitioners and physician assistants (n = 22, 8.9%).
Over half of the participants reported working in hospital or inpatient settings (n = 127, 51.4%). A substantial proportion were affiliated with hospice, palliative, or long-term care facilities (n = 62, 25.1%), and nearly one in five worked in outpatient or clinic environments (n = 45, 18.2%). Smaller groups of participants reported working in home-based care (n = 5, 2.0%), primary care or general practice (n = 3, 1.2%), or other and unspecified settings (n = 3, 1.2%).
Participants varied in years of experience: 34.0% had more than 16 years (n = 84), 28.7% had 0–5 years (n = 71), 21.5% had 6–10 years (n = 53), and 15.8% had 11–15 years (n = 39). Only a small proportion of participants reported having received training related to ELDVs (n = 23, 9.3%), whereas the vast majority had not (n = 224, 90.7%).
Descriptive and inferential statistics for the questionnaire items
Awareness and experience
Most participants reported having encountered patients who described ELDVs at least occasionally (median = 3.0, Q1 = 2.0, Q3 = 3.5, IQR = 1.5), with 18.6% of participants indicating that they had never encountered ELDV-related reports (Fig. 1). The most frequently reported contents of these experiences involved deceased family members or friends (72.9%), followed by memories of important life events (47.4%), spiritual figures (26.7%), living persons (25.5%), and 7.7% indicating all of the above (Fig. 2).
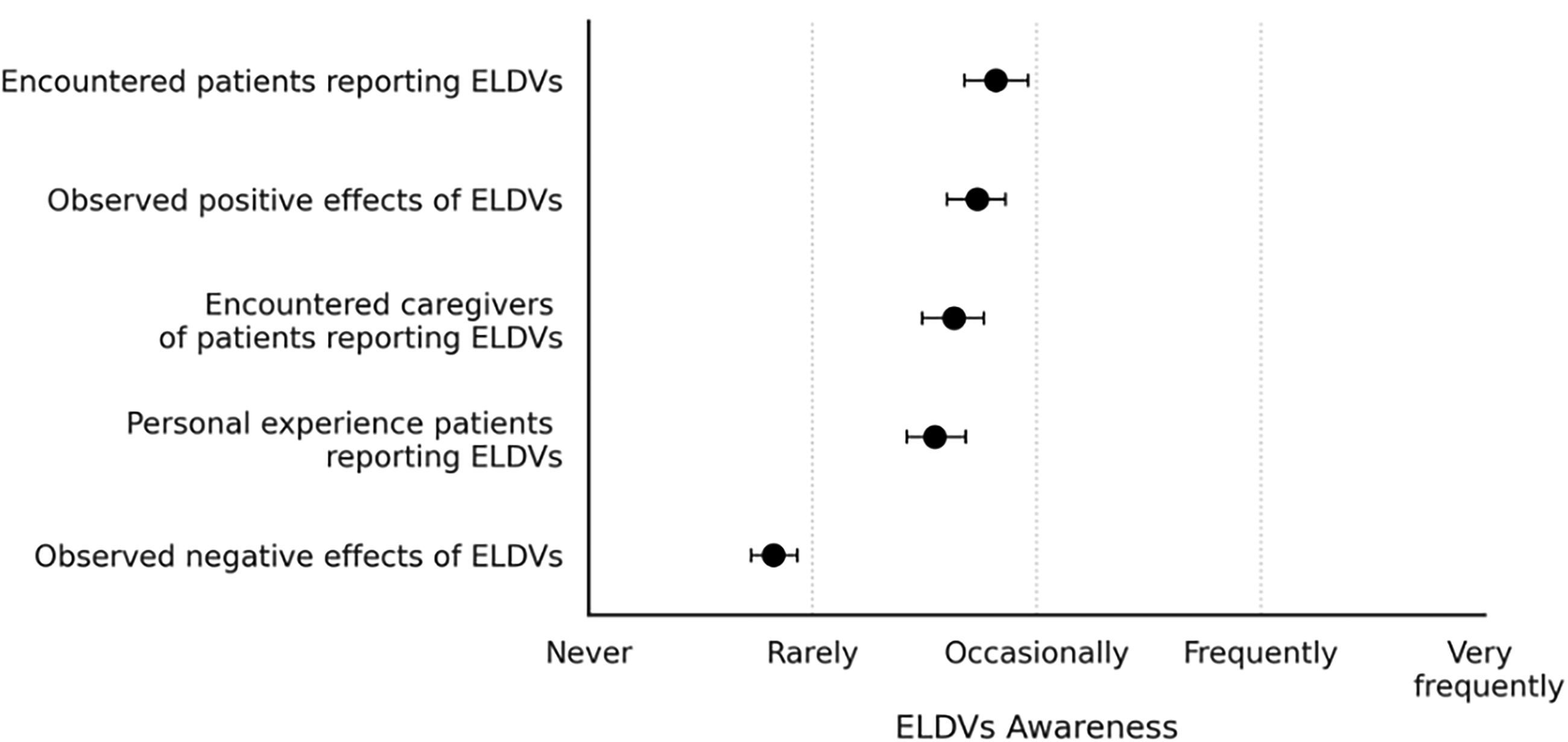
ELDV awareness and experience items (Section 2). Mean ratings (dots) and 95% confidence intervals (horizontal bars) for participants’ reported awareness and experiences with ELDVs. Responses were given on a 5-point Likert scale. ELDV, end-of-life dreams and vision.
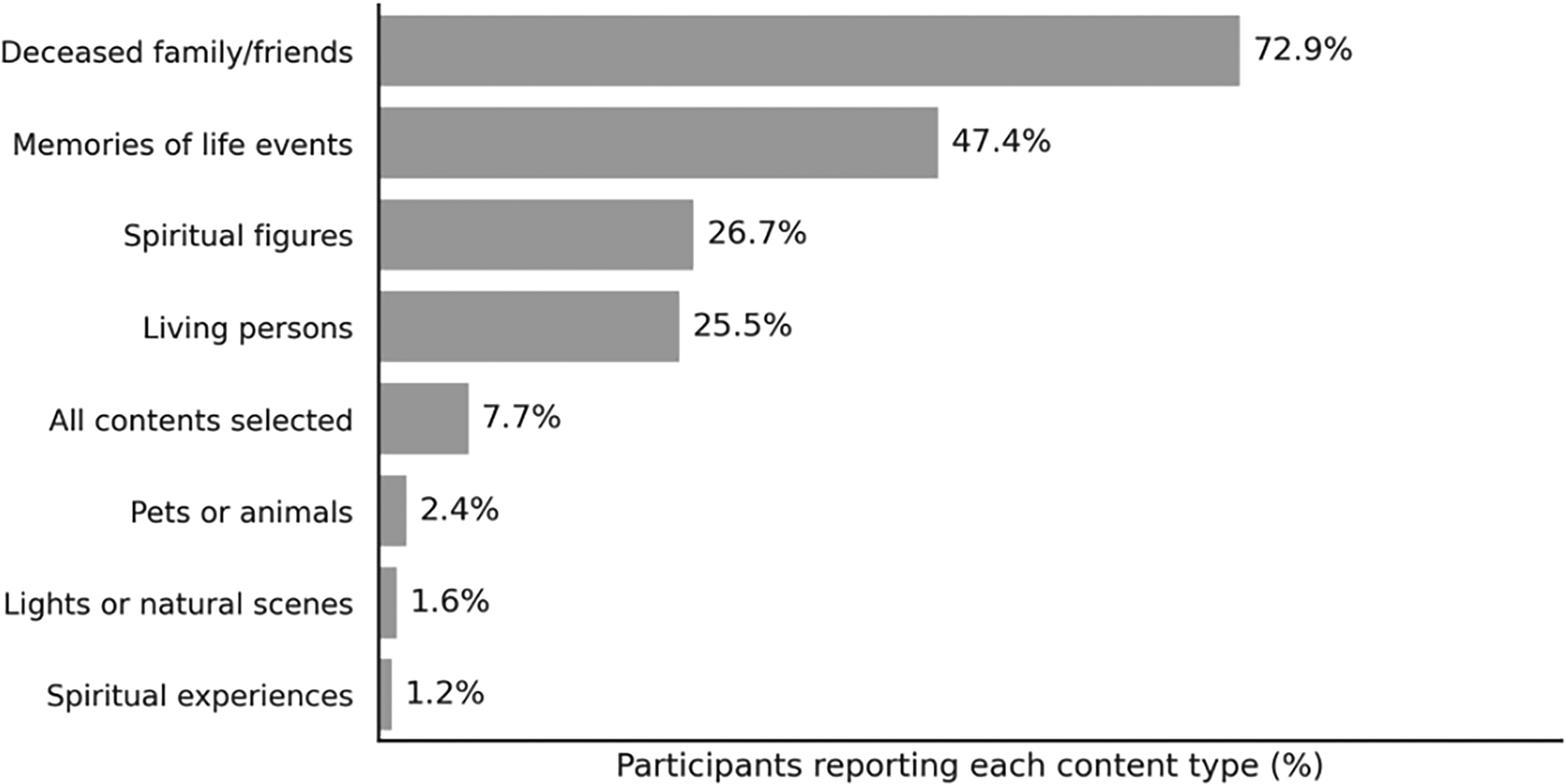
Reported ELDV content (Section 2). Percentages of participants reporting each content type of ELDVs. Bars represent the proportion of participants endorsing each category (N = 247). Percentages are based on the total sample, including those who had never encountered ELDVs (which are N = 46).
Participants also reported personal experience with patients who described ELDVs (median = 3.0, IQR = 1.0), as well as with family members or caregivers who reported such phenomena (median = 3.0, IQR = 1.0). Positive emotional or psychological effects of ELDVs on patients were observed more frequently (median = 3.0, IQR = 2.0) than negative ones (median = 2.0, IQR = 1.0). A Wilcoxon signed-rank test confirmed that this difference was statistically significant (W = 446.0, p < 0.001***).
Attitudes and beliefs
Participants generally endorsed positive attitudes toward ELDVs (Fig. 3). They largely agreed that ELDVs are a natural part of the dying process (median = 4.0, IQR = 1.0) and that patients can be emotionally and spiritually impacted by discussing them (median = 4.0, IQR = 1.0). Similarly, most participants believed that ELDVs should inform patient care (median = 4.0, IQR = 1.0) and be a standard component of end-of-life discussions (median = 4.0, IQR = 2.0).
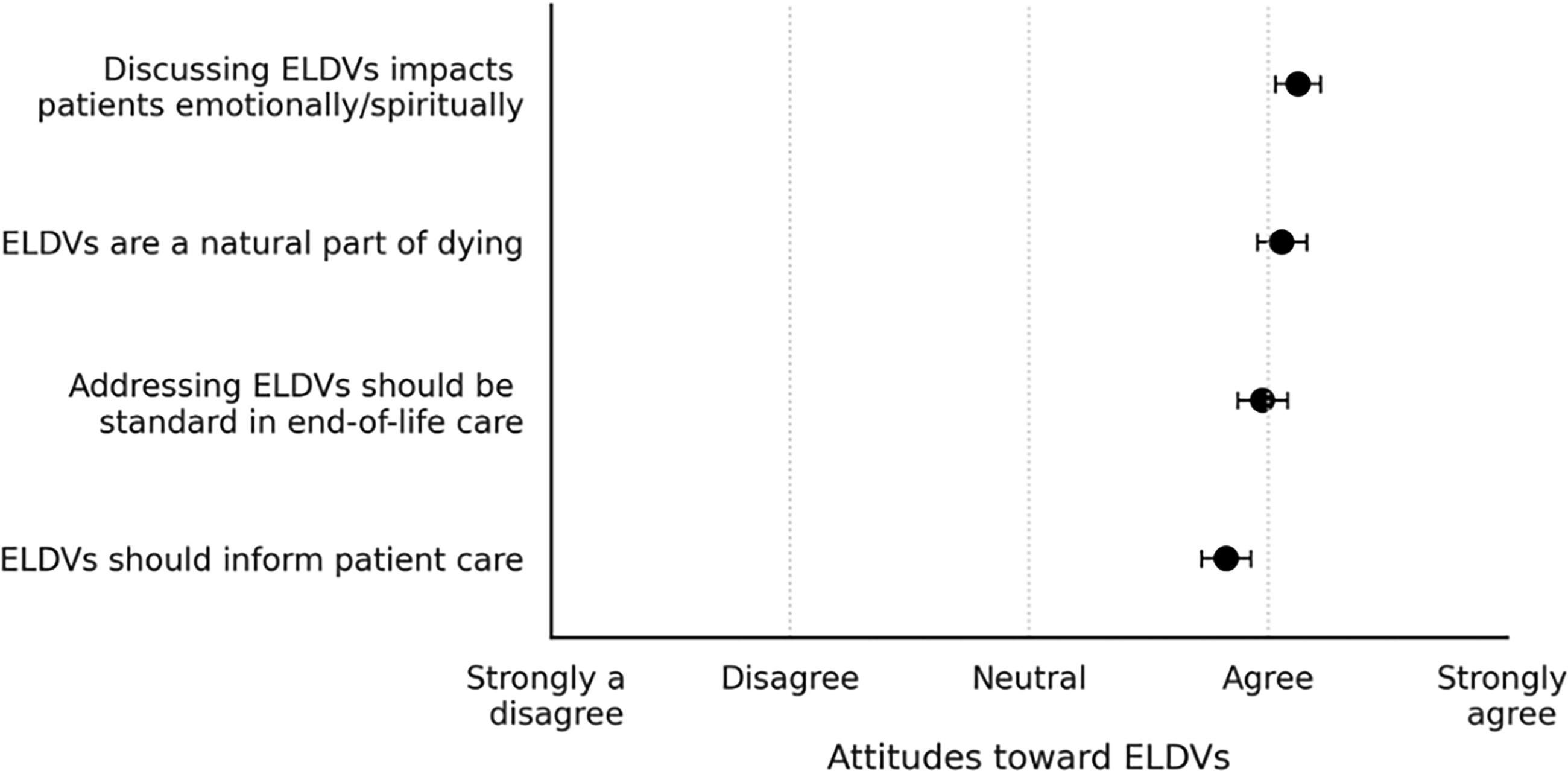
Attitudes towards ELDV items (Section 3). Mean ratings (dots) and 95% confidence intervals (horizontal bars) for items assessing participants’ attitudes toward ELDVs. Responses were given on a 5-point Likert scale.
Clinical challenges and differential diagnosis
Clinicians reported a range of challenges related to the evaluation and management of ELDVs (Fig. 4). The highest perceived challenges were the lack of institutional protocols (median = 4.0, IQR = 2.0) and lack of standardized diagnostic criteria (median = 4.0, IQR = 1.0), followed by lack of clinical time (median = 3.0, IQR = 2.0) and patient/family unawareness (median = 3.0, IQR = 2.0). The lowest perceived challenges, rated as moderate, were the fear of medicalizing (median = 3.0, IQR = 2.0) and difficulty distinguishing ELDVs from delirium/hallucinations (median = 3.0, IQR = 2.0). A Friedman test indicated that ratings differed across challenges, χ2(5) = 160.97, p < 0.001***. Post hoc Bonferroni-corrected tests showed institutional protocols and lack of standardized criteria were rated significantly higher than all other challenges (all p < 0.001).
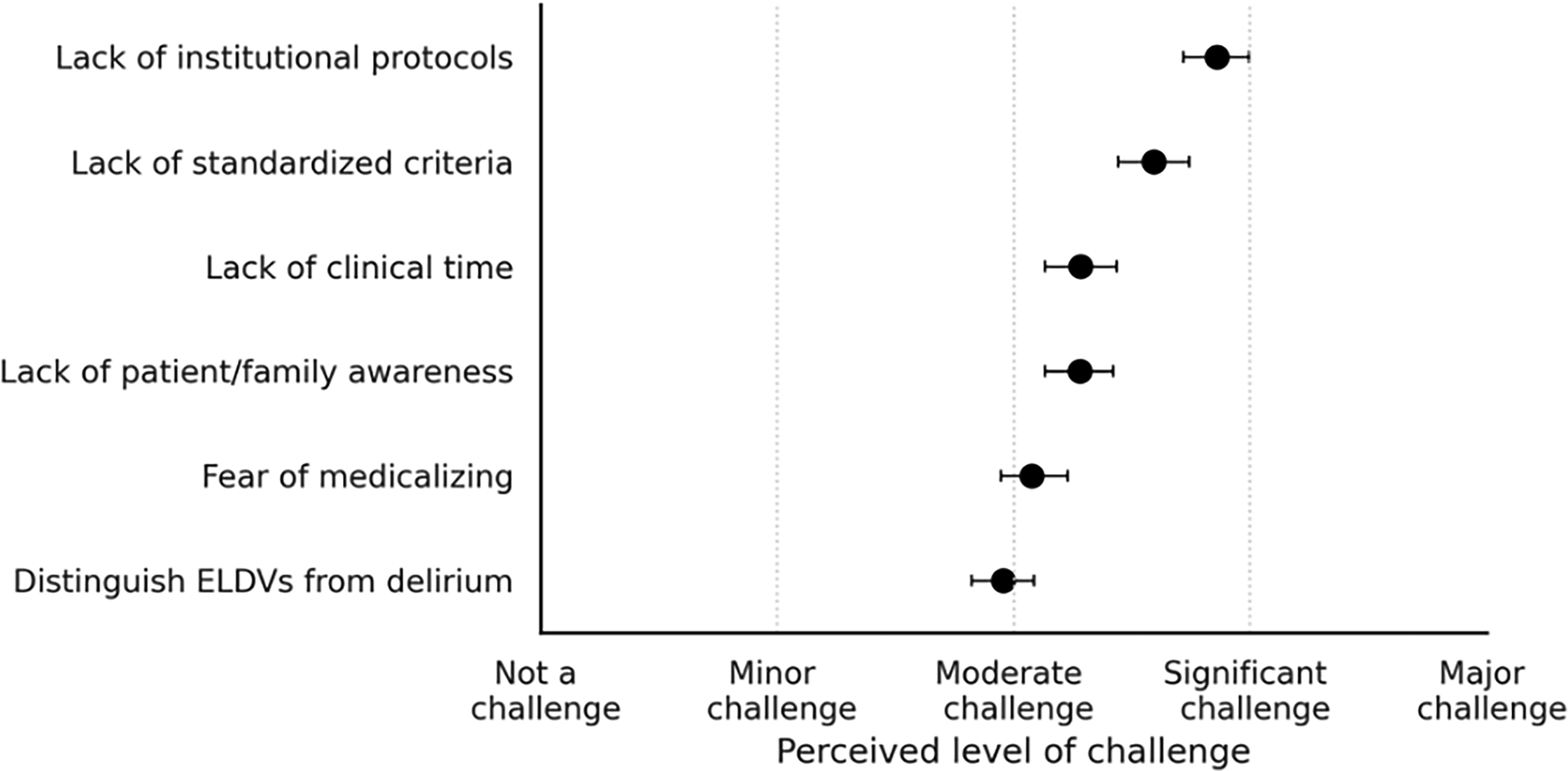
Perceived level of challenge items (Section 4). Mean ratings (dots) and 95% confidence intervals (horizontal bars) for participants’ perceived challenges in evaluating and managing ELDVs. Responses were given on a 5-point Likert scale.
Education and training
Participants expressed strong support for incorporating ELDV-related content in medical education (Fig. 5). They agreed that all medical education should include training to differentiate ELDVs from delirium or psychiatric conditions (median = 4.0, IQR = 1.0), while rejecting the notion that this should be limited to hospice or palliative care training (median = 2.0, IQR = 2.0).
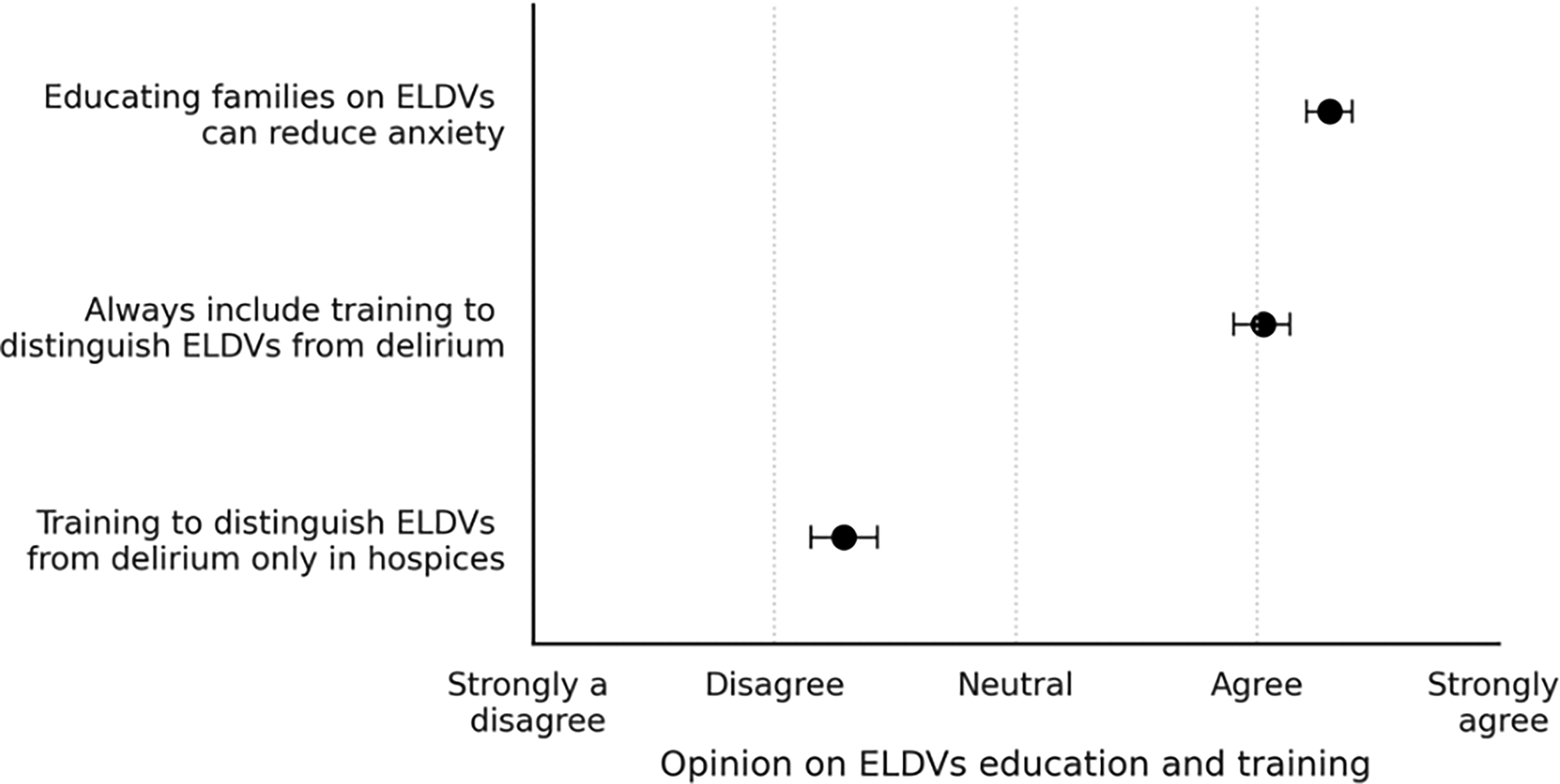
Education and training opinions items (Section 5). Mean ratings (dots) and 95% confidence intervals (horizontal bars) for participants’ opinion on ELDV education and training. Responses were given on a 5-point Likert scale.
When asked about specific training components (Fig. 6), participants most frequently endorsed structured communication-based frameworks (82.2%), toolkits (66.4%), and simulation-based training (55.9%). In total, 39.7% of participants endorsed all the above components.
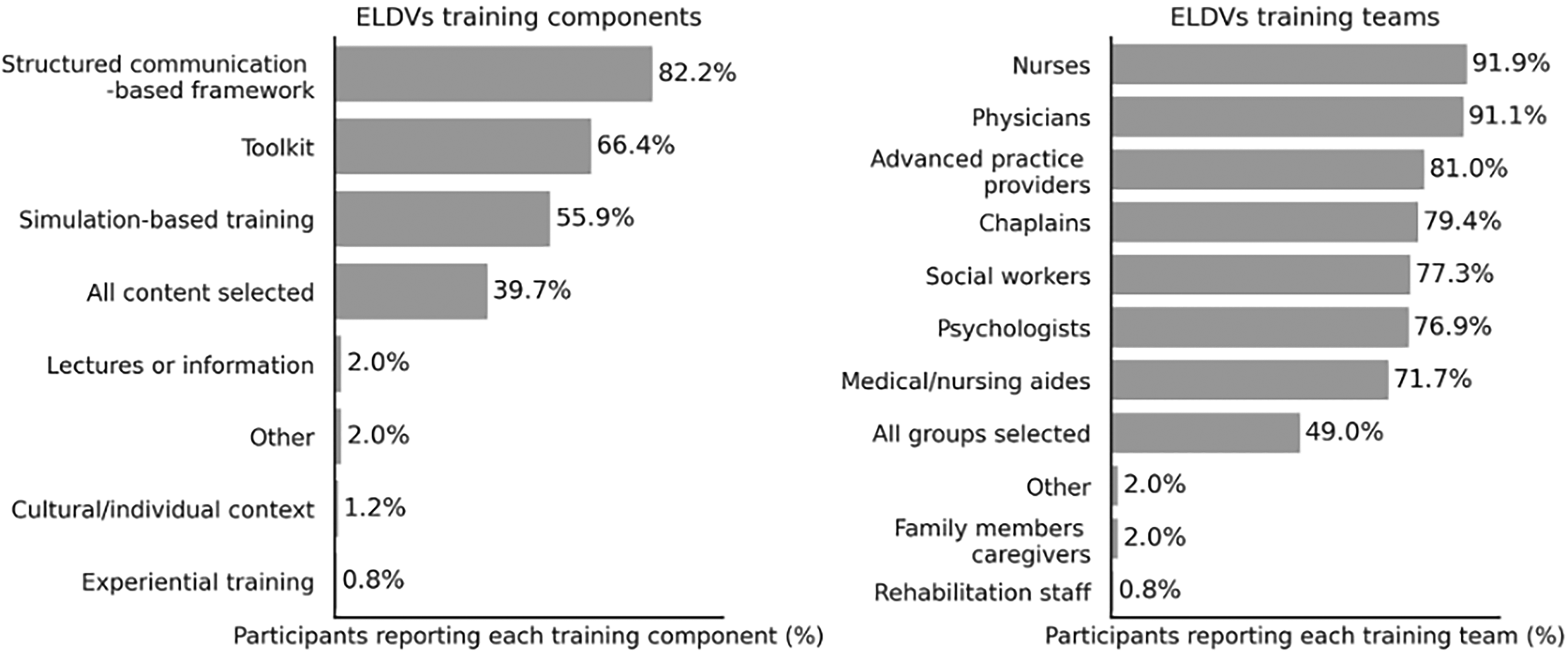
Preferred components and team members for ELDV-related training (Section 5). Left: Percentages of participants endorsing each proposed ELDV training component (N = 247). Bars show the proportion of participants selecting each option. Right: Percentages of participants indicating which professional groups should receive ELDV-related training (N = 247). Bars show the proportion of participants selecting each option.
A majority also supported educating multiple professional groups (Fig. 6), especially nurses (91.9%), physicians (91.1%), advanced practice providers (81.0%), chaplains (79.3%), social workers (77.3%), psychologists (76.9%), and medical or nursing aids (71.7%). Nearly half (49.0%) indicated that all above professions should receive training.
Finally, participants strongly agreed that educating families about ELDVs could reduce anxiety and confusion (median = 4.0, IQR = 1.0).
Institutional policy and interdisciplinary collaboration
Participants consistently supported institutional engagement with ELDVs (Fig. 7). They agreed that hospitals and hospices should implement formal policies (median = 4.0, IQR = 1.0), that ethics consultation teams should be available (median = 4.0, IQR = 1.0), and that multidisciplinary collaboration is essential (median = 4.0, IQR = 1.0). Moreover, institutional support for health care providers was strongly endorsed (median = 4.0, IQR = 1.0).
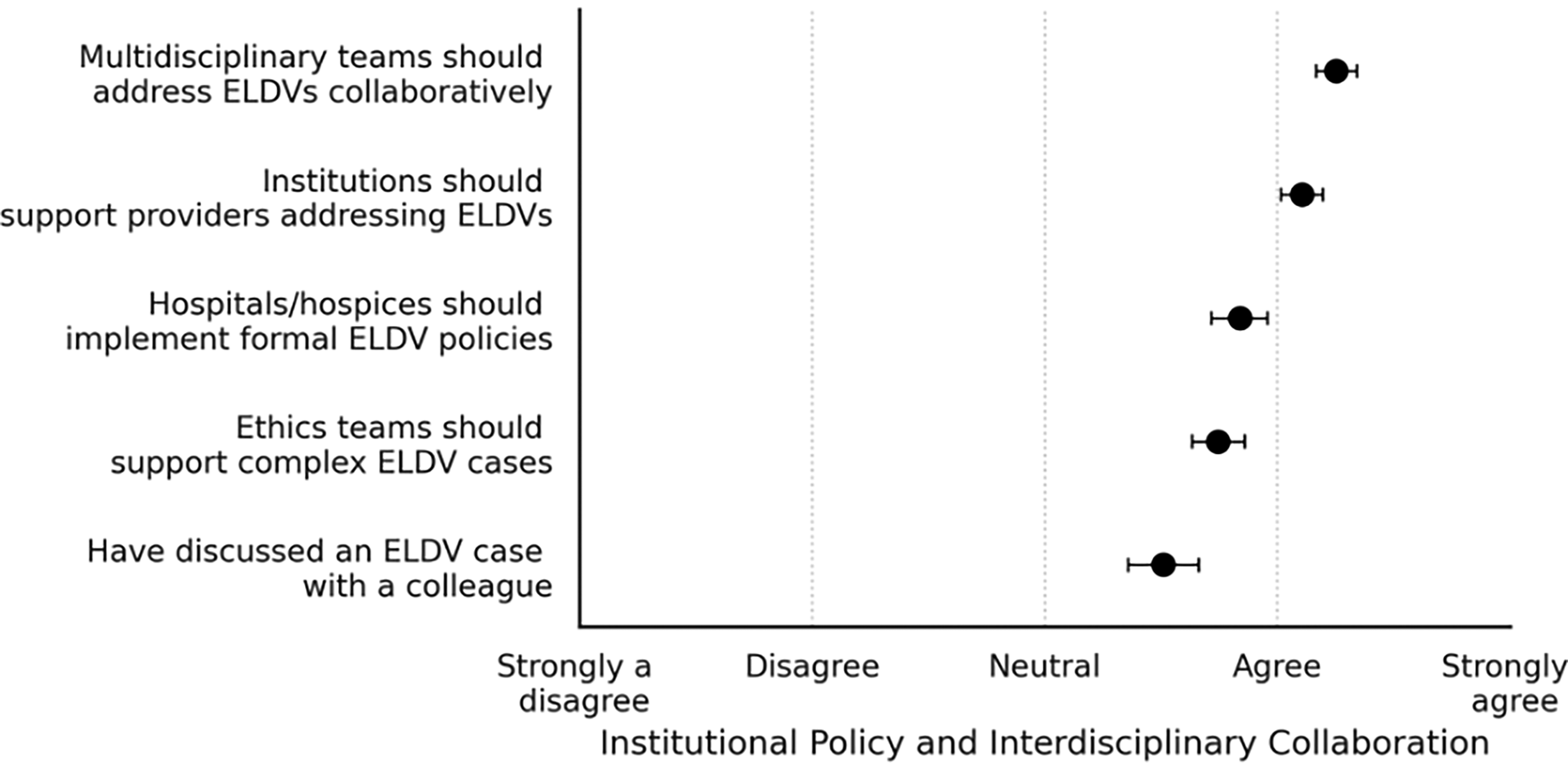
Institutional policy and interdisciplinary collaboration items (Section 6). Mean ratings (dots) and 95% confidence intervals (horizontal bars) for participants’ agreement with statements regarding institutional policies and interdisciplinary collaboration on ELDVs. Responses were given on a 5-point Likert scale.
Research, advocacy, and public awareness
Participants attributed high importance to further research and public engagement regarding ELDVs (Fig. 8). Most rated as ‘very important’ the need to differentiate ELDVs from pathological conditions (median = 4.0, IQR = 1.0), identify best-practice cases, and study pharmacological influences. Participants also supported public awareness campaigns and national guidelines on ELDV recognition and management (all medians = 4.0).
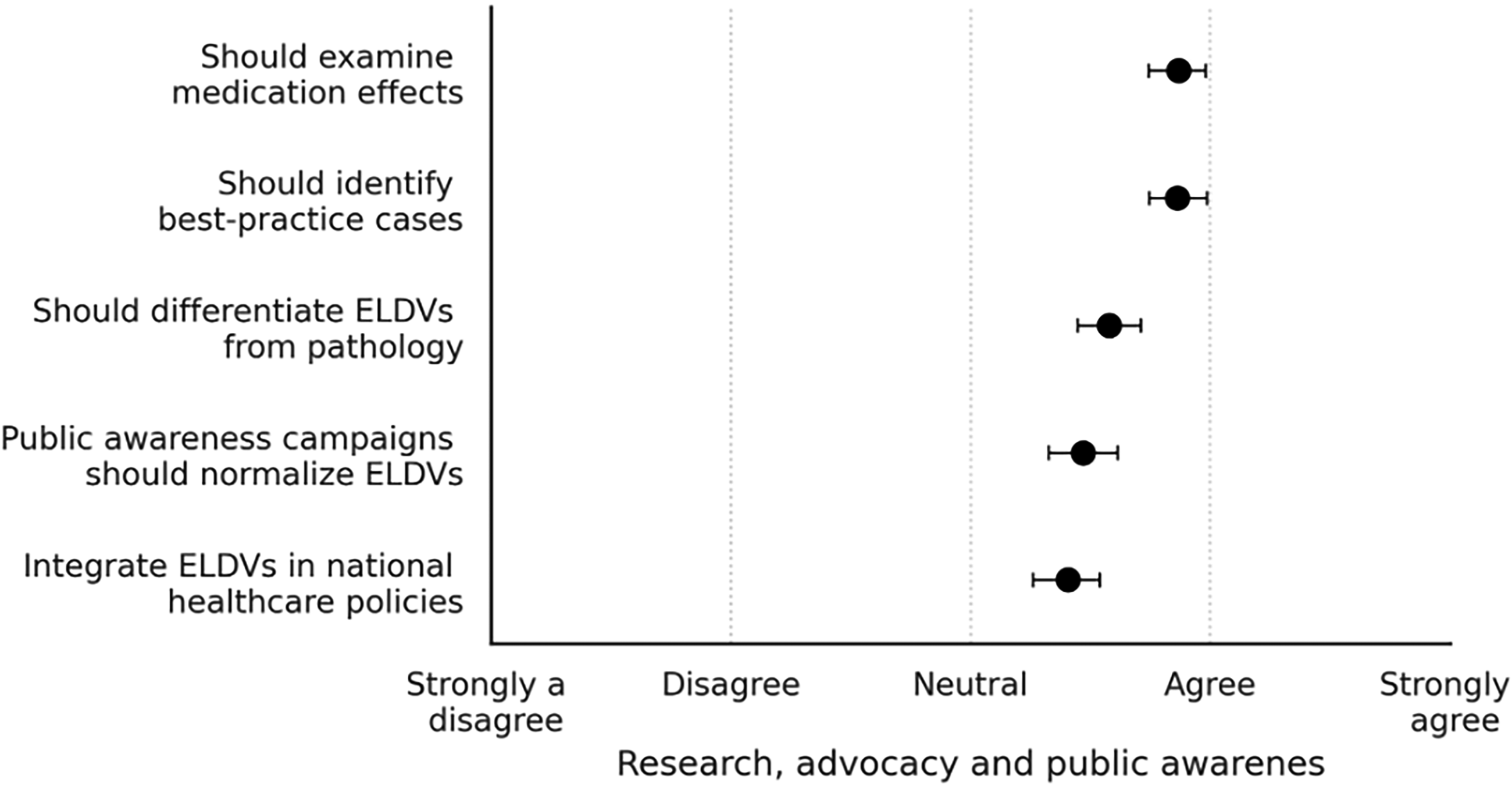
Research, advocacy, and public awareness items (Section 7). Mean ratings (dots) and 95% confidence intervals (horizontal bars) for participants’ evaluations of research, advocacy, and policy priorities related to ELDVs. Responses were given on a 5-point Likert scale.
Discussion
Our study suggests that clinicians encounter ELDVs at least occasionally, consistent with prior work among palliative care professionals. Nyblom et al. 16 found that most palliative care physicians encountered patients who described vivid and meaningful dreams or visions that involved their deceased family and friends. 16 Our participants reported a higher frequency of positive emotional effects associated with ELDVs. This pattern was consistent with the positive themes of ELDVs described by patients like comforting, preparing to go, and unfinished business. 1 Clinician acknowledgment can invite meaning-making and facilitate emotional reconciliation. 13 In contrast, not acknowledging ELDVs is a missed opportunity for holistic, person-centered care and may inadvertently intensify isolation during the dying process.17–20 When clinicians respond supportively, prior studies suggest patients may feel more peaceful and dignified, and caregivers may experience less burden.2,19,20
We found that despite frequent exposure of clinicians to ELDVs, they felt that they lacked a structured approach to take care of such encounters. Nyblom et al. and Kerr et al. observed that many physicians recognized ELDVs but had limited training and knowledge to navigate ELDV conversations with their patients.16,21 Hession et al. noted limited guidance within palliative care regarding ELDVs’ diagnostic criteria, documentation standards, and clinical pathways. 22 This becomes especially important in multicultural settings where there are disparities in health care and supportive care provision.23,24
Ethical practice requires respecting their interpretations even when they might be different from biomedical theories or individual convictions.25,26 Furthermore, the principle of beneficence highlights that physicians should recognize the potential psychological comfort of ELDVs.22,27,28 Very few participants reported receiving formal ELDV education, which is similar to other research studies that have observed insufficient clinical preparation.22,25,29 Our participants expressed their preference for communication based teaching and structured toolkits, which was similar to Grant et al.’s recommendation for reflective educational programs for clinicians. 25 In our survey we found that many participants preferred a multidisciplinary approach across all professional groups. This supports findings from previous studies that shared training enhances spiritual literacy and reduces distress. Given that distinguishing ELDVs from delirium was rated as a moderate challenge, training should include specific guidance on phenomenological features that may help differentiate these experiences, while acknowledging that clinical overlap can occur.16,21,22
Additionally, participants preferred institutional policies, clinical guidelines, and ethical support to adequately address ELDVs. Integrating ELDV-related education into palliative care curricula, communication training programs, and spiritual assessment frameworks may therefore improve clinician preparedness and confidence. Institutional policies and case-based interdisciplinary discussions may further support clinicians in navigating the complex intersection between spiritual experience, psychological meaning-making, and neurocognitive changes near the end of life.28,29
Some participants reported family and community education to be equally effective. Prior research suggests that when clinicians respond with openness and respect, caregivers often perceive these experiences as comforting or meaningful, which may reduce anxiety and contribute to healthier bereavement processes.30,31
Within this framework, ELDVs can be understood as potentially meaningful experiences that occur during the dying process rather than as phenomena that are inherently pathological. A supportive clinical response therefore aligns with the central goals of palliative care: Reducing distress, supporting existential well-being, and maintaining dignity during the final stages of life. In clinical practice, ELDVs may be addressed through a structured approach involving four key steps: Recognition, exploration, clinical differentiation, and interdisciplinary support.
First, clinicians acknowledge and validate the experience without prematurely medicalizing it. Second, patients are invited to describe the experience in their own terms, allowing personal, cultural, or spiritual interpretations to emerge. Third, clinicians evaluate whether the experience may also reflect delirium, medication effects, or other neurocognitive conditions, as there can be overlap with pathological states. Finally, interdisciplinary support involving chaplains, psychologists, nurses, or social workers can help patients and families integrate the experience within their broader emotional and spiritual context.
Exploratory group comparisons revealed that profession and clinical setting were the most consistent sources of variation: Hospice care providers reported greater ELDV awareness and more positive attitudes, while nurses reported more positive attitudes toward ELDVs and more strongly endorsed the introduction of formal ELDV policies in hospitals and public awareness campaigns. Participants based in North America reported higher ELDV awareness, while participants based in Asian and European regions reported greater perceived challenges. Participants based in Asia also reported stronger support for policies (in hospitals but also nationwide). These patterns suggest that training needs and implementation barriers are not uniform across professional roles and health care contexts and that future interventions may need to be tailored accordingly. A selection bias is present within our study since this was a self-administered online questionnaire. There is limited generalizability of our study because of nonuniform cultural representation. There is also some recall bias associated with the study because of reliance on self-reporting estimated frequencies. Future research should include patients and their families, study ELDVs through the dying process, and analyze how patient comfort, peace, and family bereavement are shaped by clinician responses.
Conclusion
This study highlights that even though ELDVs are common, clinicians feel unprepared to respond to them. It is a moderate challenge for clinicians to differentiate ELDVs from delirium, and clinical tools specifically designed to aid this distinction are currently lacking. There is a need for structured training and institutional protocols for the management of ELDVs for all physicians and should not be limited to hospice or palliative care training. The way ELDVs are perceived varies widely across cultures, so acknowledging cultural and spiritual variability is essential. Future studies should be done to include patients and their families and analyze how patient comfort and family bereavement are shaped by physician responses.
Footnotes
Acknowledgments
The authors would like to acknowledge Oshani Wijesooriya for assisting us with organizing the references for this article.
Ethical Approval and Informed Consent Statements
Ethical approval was not obtained since the survey only included health care professionals and did not include patients or any identifiable data. Participation was voluntary and the survey constituted informed consent.
Data Availability Statement
The dataset collected is not publicly available.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
The authors did not receive any external funding for this project.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.