
Abstract
Background:
Audio- and video-based educational tools may improve family members’ knowledge of and preferences for end-of-life care in intensive care units.
Objectives:
To determine and compare the effects of video and audio educational materials on knowledge of and preferences for life-sustaining treatment (LST) among family members of ICU patients in South Korea.
Design:
Pre-post study design.
Setting/Subjects:
Family members of ICU patients aged >18 years received audio or video educational materials.
Measurements:
Preferences for LSTs, knowledge regarding LSTs.
Results:
A total of 168 were enrolled and randomly divided equally into the verbal (n = 84) and video (n = 84) interventions. Preferences for most LSTs remained unchanged after the intervention, except for tracheostomy (10.7% (18/168) changed from “no” to “yes” versus 3.6% (6/168) from “yes” to “no”; p = 0.023). No significant changes in treatment preferences were observed when analyzing the video and audio groups separately. Knowledge scores significantly improved after the intervention for all participants (7.44 ± 1.57 to 8.49 ± 1.79, p < 0.005), with the video (7.48 ± 1.56 to 8.64 ± 1.52) and audio groups (7.40 ± 1.58 to 8.34 ± 2.03) showing similar improvements (p < 0.005).
Conclusion:
Preferences for most LSTs remained unchanged, likely due to high baseline knowledge, whereas knowledge improved significantly regardless of education type. Notably, a significant shift in preference was observed for tracheostomy, where baseline knowledge was lower, suggesting an educational effect.
Key Message
Educational videos and audios improved family members’ knowledge of end-of-life care but did not significantly change their preferences for life-sustaining treatments, except for tracheostomy.
Introduction
Advances in medical technology have significantly improved survival among critically ill patients; however, many still experience deterioration despite intensive care. When patients lose decisional capacity without having completed advance directives, end-of-life care decisions are typically made by surrogate decision-makers in consultation with clinicians. Previous studies have shown that patients often prefer comfort-oriented care rather than aggressive life-sustaining treatments (LSTs), yet many continue to receive intensive interventions in the ICU that are inconsistent with these values, compromising dignity and quality of life.1–7
Previous research on surrogate decision-making has primarily been conducted in Western countries, yet cultural norms surrounding family involvement and end-of-life communication vary significantly across regions. South Korea presents a unique context: it is one of the fastest-aging societies, with a low rate of advance directive completion, and family members frequently serve as surrogate decision-makers in intensive care units.8–10 In South Korean ICUs, family members participate in surrogate decision-making for most critically ill patients, as many patients have not completed an advance directive prior to acute deterioration.
At the same time, the modes of health information delivery have rapidly evolved in South Korea. More than 95% of adults own smartphones, and internet use is nearly universal (Korea Internet & Security Agency, 2023). Over two-thirds of Korean adults report obtaining health-related information online, and Korean-language YouTube videos on medical topics are widely produced and viewed.11,12
These findings indicate that audiovisual media have become an increasingly prominent channel for disseminating health information. Given this high level of digital literacy and the popularity of online video content, audiovisual educational tools may represent an effective and culturally acceptable approach to improving understanding of LSTs among family members who often act as surrogate decision-makers in the Korean ICU setting.
Despite these cultural and technological characteristics, few studies have examined how audiovisual educational interventions affect surrogate decision-making in South Korea. Existing evidence largely focuses on Western patients, with limited data on families of ICU patients in Korea. Therefore, this study aimed to evaluate whether brief educational materials delivered in audio or video format could improve families’ knowledge of, and influence their preferences for, LSTs in South Korea.
Methods
Design and setting
We conducted this pre–post questionnaire-based study at the 18-bed medical ICU at Seoul Metropolitan Government-Seoul University Boramae Medical Center. The Institutional Review Board of Boramae Hospital (No.: 30-2018-29-53) approved the study protocol. All participants provided written informed consent. When obtaining informed consent, the interviewer explained the outline of the study: (1) the goal, (2) the inclusion of 5-minute-long educational materials (verbal narrative audio or video), and (3) the requirement of completing a 5-minute questionnaire assessing knowledge regarding LSTs before and after education. Recruitment was conducted between September 1, 2019, and May 30, 2022.
Participants
Family members of patients admitted to the ICU were invited to participate in the study. The eligibility criteria were as follows: (1) aged over 18 years, (2) able to provide informed consent, (3) able to communicate in Korean, and (4) were within 72 hours of patient admission to the medical ICU. After obtaining informed consent, the interviewers administered a baseline questionnaire concerning demographics, self-reported health status, and baseline preference for, and knowledge of, LSTs.
After confirming eligibility and obtaining informed consent, participants completed a baseline questionnaire and were subsequently randomized 1:1 to either a verbal arm (recorded narration) or a video arm (video with identical narration). Randomization was performed using a computer-generated list with block sizes of 2, 4, and 6; assignments were kept in sequentially numbered, opaque, sealed envelopes.
Measures
The baseline questionnaire assessed demographics, self-reported health status, and baseline preferences for and knowledge of LSTs. Participants were asked about their willingness to receive or continue the following treatments if their condition worsened despite receiving intensive care: cardiopulmonary resuscitation (CPR), intubation with mechanical ventilation (MV), tracheostomy, and continuous renal replacement therapy (CRRT). This question was phrased as: “If you were admitted to the ICU and your condition worsened despite treatment, would you wish to receive or continue the following treatments? “(Please check all that apply). A self-referent, hypothetical scenario was used to minimize the emotional and ethical burden associated with answering on behalf of an actual ICU patient and to reduce potential bias related to the patient’s clinical condition. Participants were therefore asked to respond based on their own hypothetical treatment preferences. This design was intended to assess value orientations relevant to surrogate decision-making when patient preferences are not explicitly known. This design allowed the study to assess family members’ baseline knowledge and underlying values relevant to surrogate decision-making. Additionally, a 10-item True/False questionnaire assessed knowledge of CPR, mechanical ventilation, tracheostomy, and hemodialysis.
The study’s end-of-life care preferences and 10 knowledge items were developed based on the Korean Professional Consensus for Comfort Care and Withdrawing/Withholding in the Intensive Care Unit and previous studies of end-of-life care decisions using questionnaires.13,14 They were iteratively reviewed and revised to ensure content and face validity through three expert advisors and five pilot cognitive interviews until ≥80% comprehension for each item was achieved. A post-intervention questionnaire included the same preference and knowledge questions.
Interventions
Participants assigned to the verbal group filled out the baseline questionnaire and listened to a 5-minute-long recorded narration. This recorded verbal narration described LSTs, including CPR, intubation or MV care, tracheostomy, and CRRT. After listening to the audio, they were asked to complete the same knowledge and preference questionnaire as at baseline.
Participants assigned to the video group viewed the video support tool on a laptop. Based on the video (https://www.youtube.com/watch?v=PAcUlVg0DtY) posted by the Korea National Institute for Bioethics Policy and National Agency for Management of Life-Sustaining Treatment, we added additional details (about tracheostomy). The contents were the same as in the verbal narration group. The video clip included text and 2D or 3D animated images of the aforementioned LSTs. The interviewers were not allowed to comment on or answer any questions from the participants during the intervention. The video group completed the same baseline and post-intervention questionnaires as the verbal group.
Data collection
Two interviewers, who were not blinded to the intervention, administered the structured questionnaire to participants before and after they listened to the verbal narrative alone or viewed the video with narration. The baseline self-report questionnaire contained the following variables: age, gender, education, marital status, religion, health status, economic status, relation to patient, self-reported level of knowledge of LSTs, prior experience with LSTs (seen or heard), and route of exposure. Before and after intervention, we also questioned participants about whether they were willing to choose LSTs (CPR, intubation, tracheostomy, CRRT) if their own medical condition were worsening despite treatment in the ICU. The knowledge of life-prolonging treatment was evaluated using 10 true/false questions, each worth 1 point, for a total score of 0–10, with a higher score reflecting greater knowledge.
Outcome measurement
The primary outcome was the within-group change in preferences for LSTs before and after the intervention in each group (verbal and video). The secondary outcomes included within-group changes in knowledge scores before and after the intervention in each group.
Statistical analysis
Baseline demographics were presented as mean ± standard deviation or frequencies (percentages). The chi-square test or Fisher’s exact test was used for categorical variables and two-sample t-tests for continuous variables to compare demographic differences between the verbal and video arms. To compare the preference for LSTs before and after intervention, McNemar’s test was performed. p < 0.05 was considered significant. The Wilcoxon rank-sum and signed rank-sum tests were used to compare nonnormally distributed means of each group’s knowledge score before and after intervention. All statistical analyses were performed with SPSS version 18.0 (SPSS Inc., Chicago, IL, USA) and SAS 9.4 (SAS Institute, Cary, NC, USA).
Results
Participants and baseline demographics
The analytic sample consisted of 168 participants, equally divided into the verbal (n = 84) and video (n = 84) groups, as shown in Figure 1. Demographic factors including gender, age, relationship to the patient, marital status, educational attainment, religion, self-reported status, and income status are displayed in Table 1. The mean age was 53.2 (standard deviation = 15.3) years, and 58.3% were women. Most of the participants were spouses (24.4%) and children of patients (50%). About 76.8% (129/168) of the participants reported having heard of LSTs before the study and that they had received this information via traditional mass media (46.4%), family experience (16.7%), and the internet (13.7%).
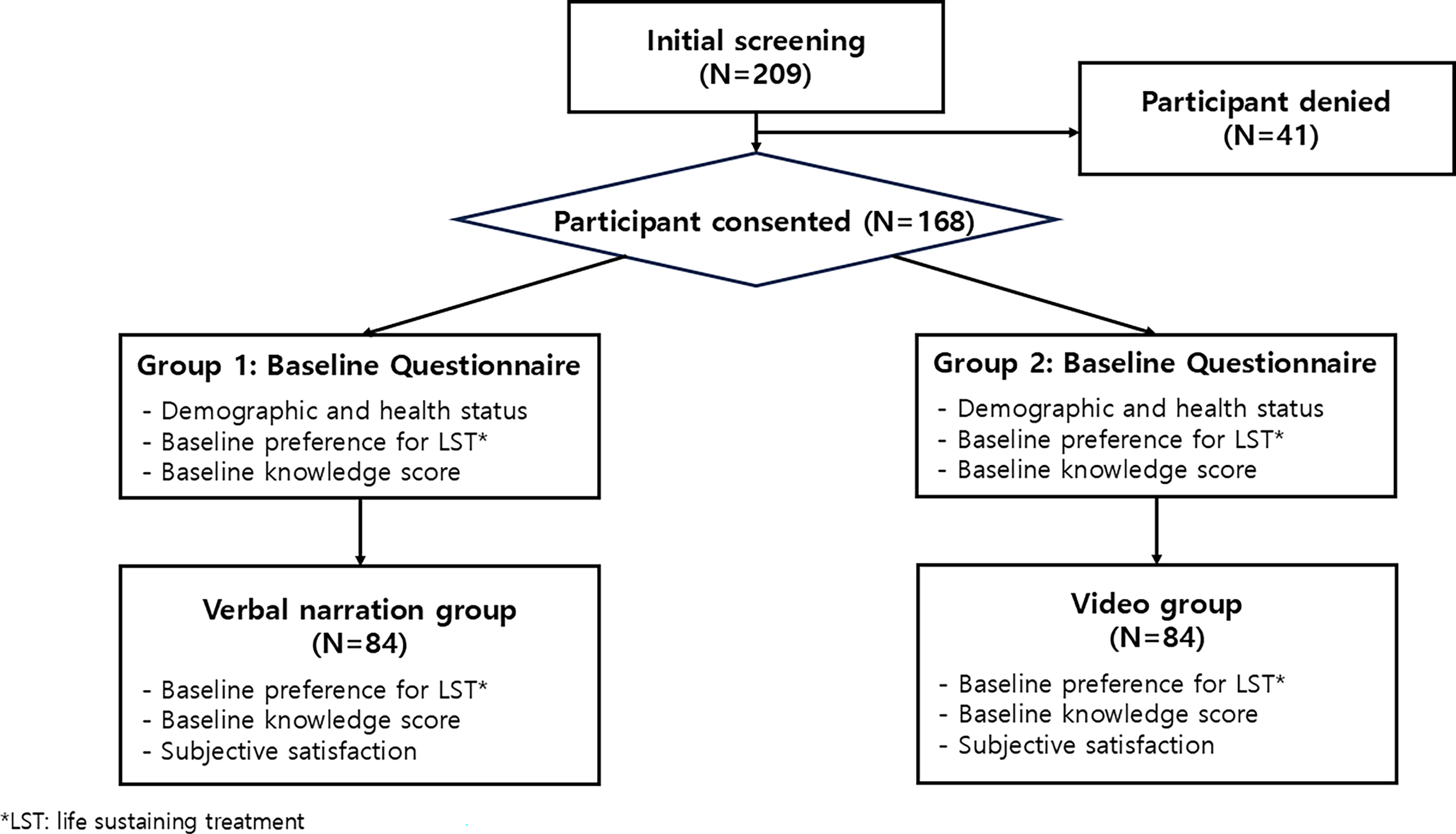
Flow chart of study sample.
Baseline Demographics of Total Participants
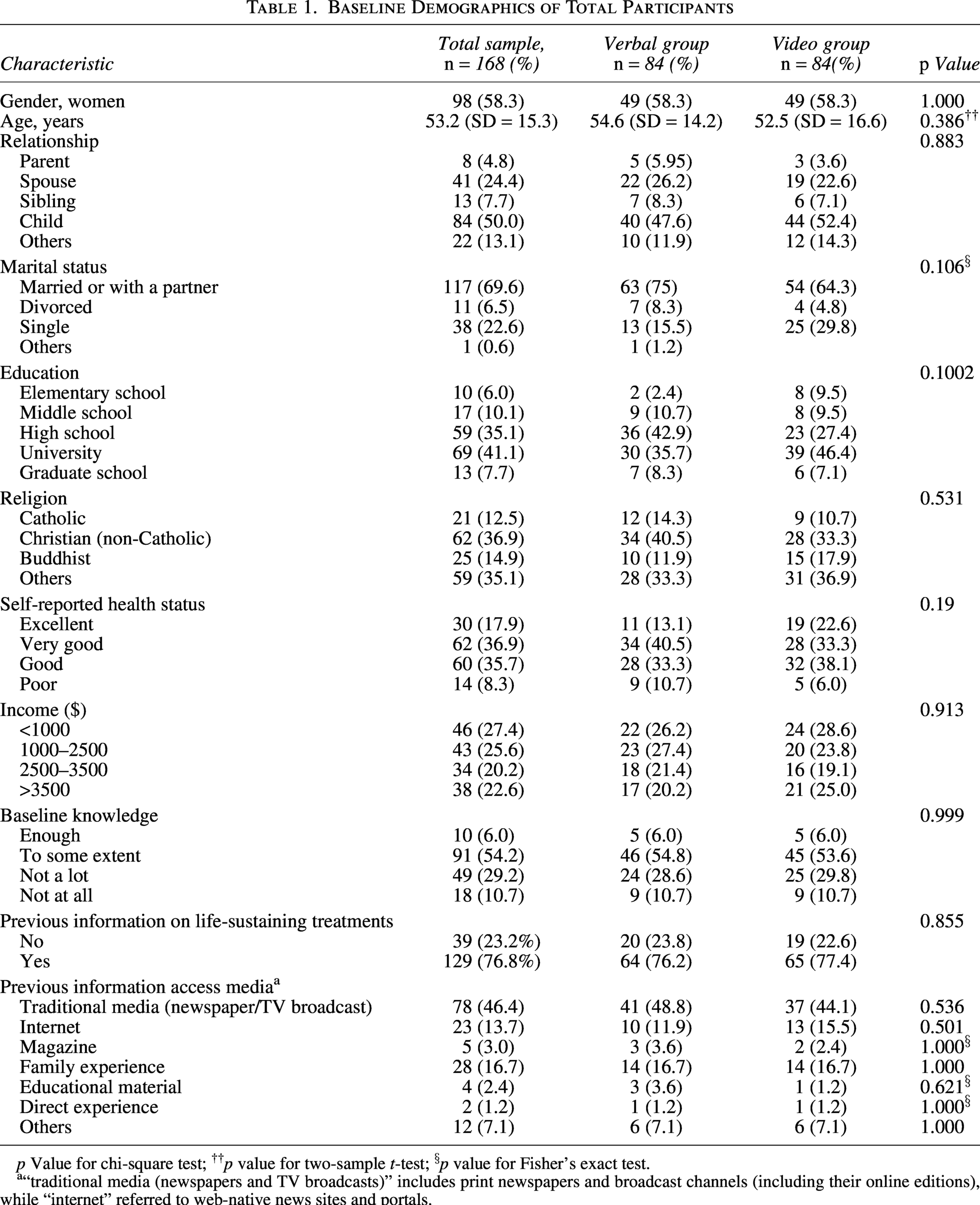
p Value for chi-square test; ††p value for two-sample t-test; §p value for Fisher’s exact test.
“traditional media (newspapers and TV broadcasts)” includes print newspapers and broadcast channels (including their online editions), while “internet” referred to web-native news sites and portals.
Most participants (101/168, 60.1%) reported having at least some baseline knowledge about LSTs. There were no significant differences between the two intervention groups across any baseline characteristics (Table 1).
Preference for life-sustaining treatments
More than two-thirds of the participants declined LSTs before and after intervention. Overall, changes in preferences for LSTs were limited, with no statistically significant differences observed except for tracheostomy (Table 2). Specifically, a significantly higher proportion of respondents changed their preference from “no” to “yes” (10.7%) compared to those who changed from “yes” to “no” (3.6%) (p = 0.023). Subgroup analysis by relationship revealed that both the child and spouse groups showed a greater preference for tracheostomy following the training. When analyzed by intervention group, neither the video nor the audio group demonstrated statistically significant changes in preferences for any of the LSTs (Table 3).
Comparison of Preferences for Life-Sustaining Treatments before and after Intervention in Total Participants
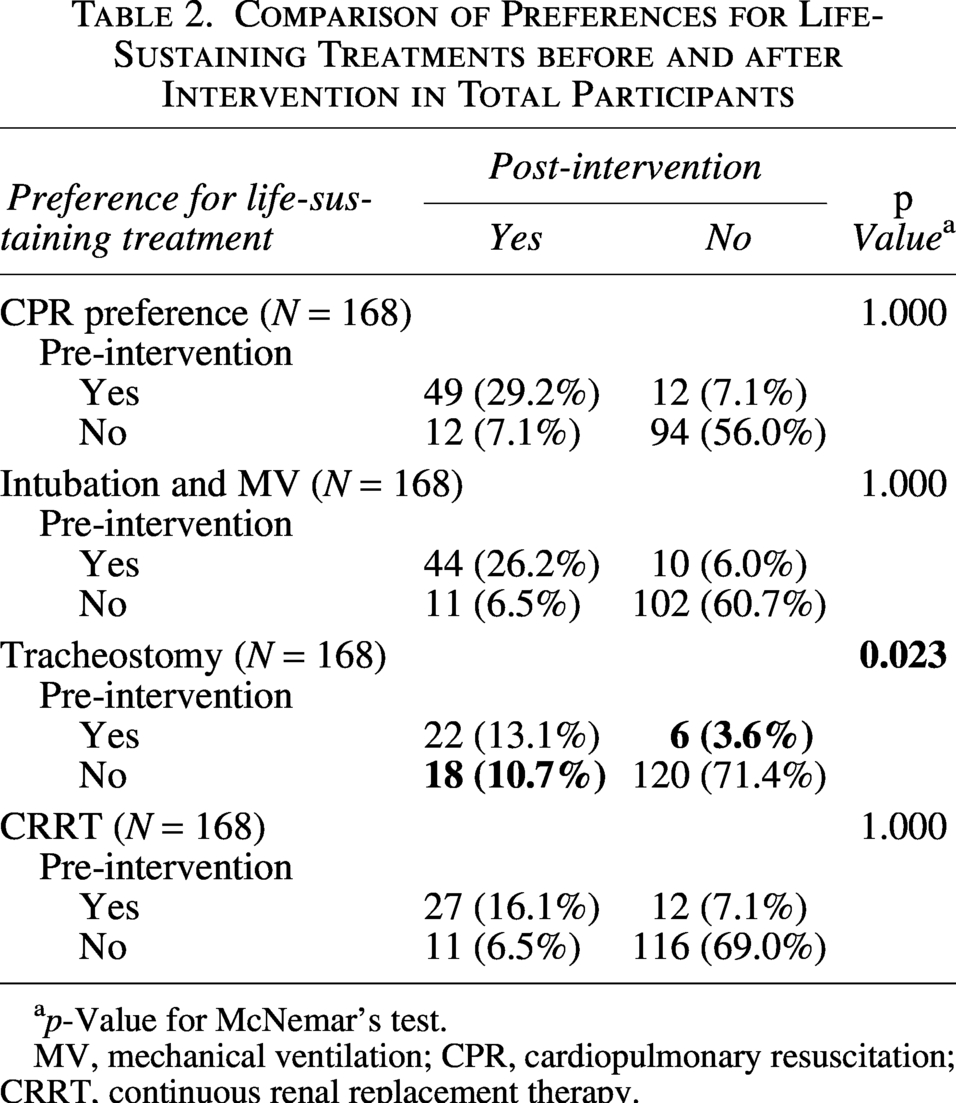
p-Value for McNemar’s test.
MV, mechanical ventilation; CPR, cardiopulmonary resuscitation; CRRT, continuous renal replacement therapy.
Comparison of End-of-Life Care Preferences before and after Intervention in the Verbal and Video Group
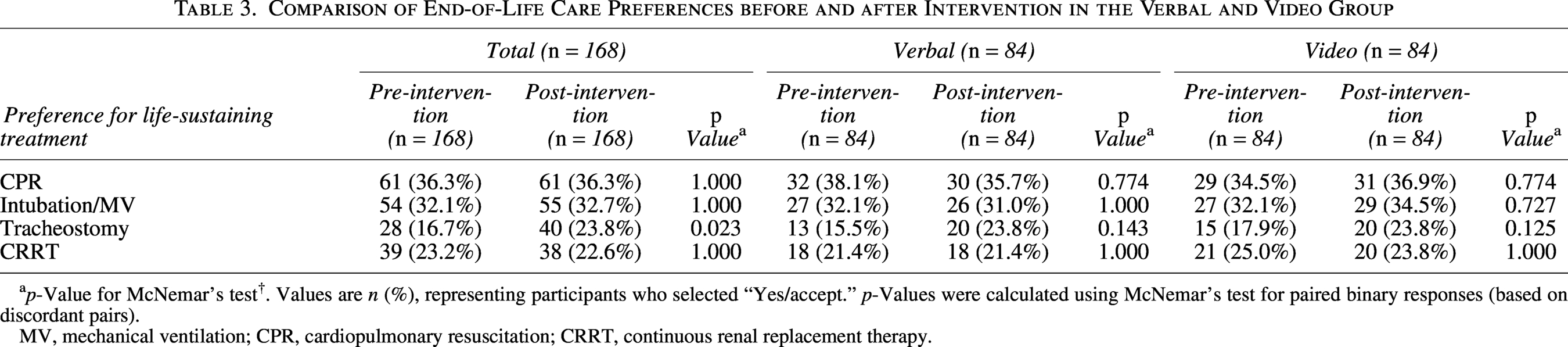
p-Value for McNemar’s test†. Values are n (%), representing participants who selected “Yes/accept.” p-Values were calculated using McNemar’s test for paired binary responses (based on discordant pairs).
MV, mechanical ventilation; CPR, cardiopulmonary resuscitation; CRRT, continuous renal replacement therapy.
Knowledge scores
The mean knowledge score (range 0–10) is presented in Table 4. The total sample’s knowledge score was significantly improved post-intervention (7.44 ± 1.57 versus 8.49 ± 1.79, p < 0.005). When analyzing the video and audio groups separately, knowledge scores also increased from pre- to post-intervention in both groups (verbal: 7.40 ± 1.58 versus 8.34 ± 2.03, p < 0.005, video: 7.48 ± 1.56 versus 8.64 ± 1.52, p < 0.005).
Knowledge Score Comparison Between Groups Before and After Education

p Value for Wilcoxon signed rank test.
Additionally, we analyzed the responses of the knowledge assessment in detail. Table 5 summarizes the pre- and post-test results for each knowledge question. There were no statistically significant differences between the two groups across all 10 knowledge questions. Notably, question 2, “CPR is a first-aid procedure that artificially compresses the heart to supply blood to the heart and brain in the event of a heart attack,” had the highest proportion of correct responses among the 10 questions before and after intervention (97% vs. 95%). For the statement, “When a tracheostomy is performed, the person is unable to speak,” the proportion of participants answering correctly increased substantially from pre- to post-intervention (56% vs. 87%). Among the total sample, the proportion of correct answers increased significantly after the intervention for questions 1, 3, 5, 6, 7, 9, and 10 (p < 0.05).
Knowledge Assessment Scores Before and After the Intervention
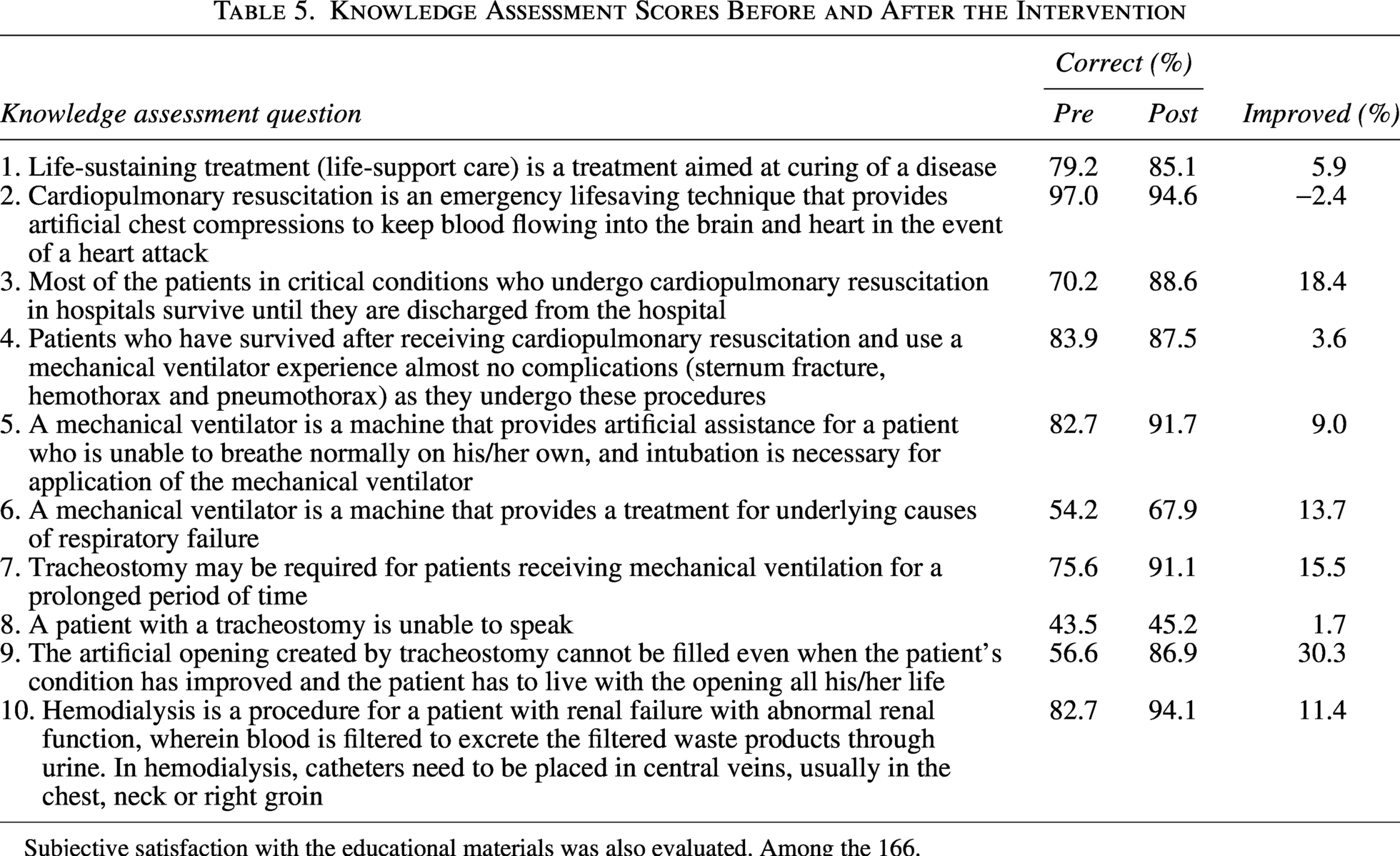
Subjective satisfaction with the educational materials was also evaluated. Among the 166.
Discussion
This study examined whether short audio and video educational materials could influence family members’ knowledge and preferences regarding LSTs in South Korea. Both interventions significantly improved knowledge but produced little change in treatment preferences, except for tracheostomy, where acceptance increased after education. These findings suggest that audiovisual interventions primarily enhance understanding rather than alter deeply rooted attitudes toward end-of-life care.
The limited change in treatment preferences observed in this study may therefore reflect the stability of such value systems. In South Korea, where discussions about death remain sensitive and the concept of patient autonomy is less emphasized than in Western contexts, family members often perceive the continuation of treatment as an expression of devotion or moral duty.15,16 Furthermore, Korean ICUs tend to maintain LSTs for terminally ill patients, including those with hypoxic-ischemic encephalopathy or septic shock, more actively than Western or other Asian settings. 17 This deeply ingrained approach may have reduced the impact of a brief five-minute intervention, as participants likely held pre-established opinions about end-of-life care prior to the study.
Another possible explanation for the limited change in preference is that participants entered the study with a relatively high baseline familiarity with common LSTs such as CPR and mechanical ventilation. The participants were family caregivers, a group typically more exposed to medical information than the general public due to their involvement in patient care. Previous research has also shown that family members of ICU patients demonstrate higher LST knowledge than the general population. 18 Our sample’s high prior information rate (77.0%) likely reflects this caregiver advantage, further enhanced by their younger, more educated profile and the high-intensity care environment in South Korea. 19 Therefore, our participants’ high prior exposure likely resulted in a ceiling effect, leaving less room for significant improvement following the intervention.
This high baseline familiarity is further supported by our survey results, which showed that correct response rates for CPR and mechanical ventilation were high at baseline and remained nearly unchanged after education. This can be attributed to frequent exposure through mass media and popular medical dramas. Furthermore, since pneumonia is the third leading cause of death in South Korea and often progresses to severe respiratory failure in elderly patients,MVis a common high-intensity intervention in clinical settings.19,20 Consequently, surrogate decision-makers are frequently exposed to these clinical and social information sources, which may explain the high baseline understanding.
In contrast, the pattern of preference change for tracheostomy reflects how newly acquired knowledge can shift clinical choices within a specific cultural framework. While participants already had high baseline knowledge of CPR and MV, their awareness of tracheostomy was initially limited. Our results show that after the intervention effectively bridged this knowledge gap, there was a significant increase in the acceptance of tracheostomy. This shift toward choosing to perform tracheostomy is likely rooted in the cultural context of South Korea.15,16 In a society where filial piety and moral duty are paramount, family members often feel a strong obligation to provide every possible treatment as an expression of devotion. Before the intervention, a lack of information might have caused hesitance; however, once participants gained a clear understanding of the procedure, they likely perceived tracheostomy as a viable and necessary option to fulfill their moral duties. Therefore, the significant increase in preference suggests that for less familiar procedures, providing clear information allows caregivers to align medical interventions with their cultural values.
Despite the minimal shift in preferences, the significant improvement in knowledge remains clinically meaningful. In our study, knowledge scores for LSTs significantly increased after education regardless of modality, indicating that both audio and video materials effectively enhanced understanding among family members. Participants were, on average, around 50 years old, and most had completed at least a high school education. Given this profile, their relatively higher educational background and younger age likely contributed to a better understanding of the materials. Furthermore, unlike the very elderly, this cohort is generally more familiar with audiovisual content, which may have allowed them to absorb complex clinical information more effectively. This combination of educational attainment and media familiarity likely explains the significant knowledge gains observed in our sample. Consequently, these findings highlight the potential of structured audiovisual tools to facilitate more informed and collaborative decision-making in clinical practice.
There are several limitations to our study. First, because families of patients within 72 hours of ICU admission were included, it is possible that they were already exposed to information about end-of-life medical care prior to the study. Second, the study population consisted primarily of relatively younger and more educated surrogate decision-makers in a high-resource health care environment, which may limit generalizability to older populations, particularly among married dyads, where spouses are more likely to serve as surrogate decision-makers.
Conclusion
We evaluated the impact of video and audio education materials on preferences for and knowledge of LSTs among families of patients in the ICU. The preference for LSTs was not impacted by either video or verbal education materials; the only exception was tracheostomy. However, both video and verbal education were effective in increasing knowledge about LSTs, indicating the usefulness of educational materials in informing surrogates and caregivers about end-of-life care options.