
Abstract
Background:
Hospice use is higher in the growing Medicare Advantage (MA) program compared to Traditional Medicare (TM). It is uncertain if this is due to different hospice referral patterns.
Objectives:
To compare hospice use patterns in MA versus TM across beneficiary characteristics.
Design:
Retrospective cohort study.
Setting/Subjects:
United States decedents in the Medicare Current Beneficiary Survey (2010–2022).
Measurements:
We employed a counterfactual modeling approach: among those in MA, we estimated the association between hospice use and sociodemographic, health, and regional characteristics. We then applied these coefficients to the TM population to predict hospice use had they been enrolled in MA.
Results:
Among 5153 decedents, 35.3% were in MA at death. Compared to TM decedents, MA decedents were younger, more likely to be Hispanic, less likely to reside in a facility, and less likely to report serious illnesses (dementia, cancer, stroke, heart disease, and lung disease). We estimated that if TM decedents had been enrolled in MA, hospice use would have been 6.1% higher (95% confidence interval, CI, 3.4%−8.8%) versus observed hospice use in TM. This difference was pronounced among those with higher education and serious illnesses in TM: for example, 10.1% higher for those with dementia (95% CI 6.9%−13.3%) versus without dementia (2.5% higher, 95% CI 1.2% lower–6.1% higher).
Conclusions:
Relative to TM, hospice use is highest among MA beneficiaries with higher education and specific serious illnesses. Future work needs to assess the drivers of this difference (e.g., palliative care, networks).
Key Message
Applying a counterfactual model to a national survey of Medicare beneficiaries, we find hospice use in Medicare Advantage (MA) is particularly high relative to Traditional Medicare among those with higher education levels and specific serious illnesses. This has implications for how the growing MA program is influencing end-of-life care.
Introduction
The majority of Medicare beneficiaries (54%) are now insured by a Medicare Advantage (MA) organization (MAO), more than double compared to 25% in 2010. 1 MAOs influence the care of people with serious illness in a range of ways and are highly diverse, with the average Medicare beneficiary choosing among 43 plans offered in their county. 2 MAOs contract with networks of care providers, which vary in their breadth and quality.3,4 They may use prior authorization processes to limit service use, such as for post-acute care. 5 They may contract or develop palliative care services, particularly as legislation has broadened the ability of MA organizations to provide supplemental benefits that are not covered under traditional Medicare (TM).6–8 Indeed, research and commercial efforts to identify MA enrollees who are approaching death and provide palliative care services have grown, given the incentives of MAOs to reduce the health care costs of this population.8–10
It is particularly important to understand how MA organizations are shaping the care of older adults with dementia and other serious illnesses. The proportion of older adults with dementia insured by MA plans, while lower than that of older adults without dementia, has steadily grown over time. 11 However, data are mixed on the experience of older adults with dementia in MA. Most studies have shown that older adults with dementia are more likely to switch from MA to traditional Medicare, as are other populations with serious illness such as those with cancer and functional impairment, possibly due to lower satisfaction in the MA program.11–14 When satisfaction around serious illness care in MA has been directly measured, either through surveys of PWD or those at the end of life, care and insurance quality have been found to be worse in MA versus TM.13,15 Decedents in MA plans are less likely to die in hospitals, but if they are, are more likely to receive care in intensive care units, a potential marker of burdensome care, but more likely to be referred to hospice, which is associated with improved end-of-life care. 16
The role of MA organizations in shaping hospice care is unique given that hospice has been carved out of MA, meaning that payments for hospice fall under TM. This means that MA organizations do not contract with hospice agencies to provide hospice care, negotiate rates, create networks of hospices for MA beneficiaries, or use mechanisms like prior authorizations to limit hospice use. However, their influence on services prior to hospice enrollment, including through the provision of palliative care, may result in more or different patients being steered to hospice use. While a carve-in of hospice into MA was trialed from 2021 to 2024 under the value-based insurance design model, this was limited in scope and was ended early by the Centers for Medicare and Medicaid Services due to low participation and administrative complexity of the payment model. 17
We do have some information that indicates that MA plans may be influencing hospice use, even in the carve-out. Multiple studies and reports from the Medicare Payment Advisory Commission have demonstrated slightly higher rates of hospice use among decedents in MA versus TM, with a narrowing gap over time.16,18 MA enrollees were more likely to enroll in hospice from community settings as opposed to following inpatient stays than their counterparts in TM. 19 However, length of stay in hospice has not substantially varied for beneficiaries in MA versus TM. While the general MA beneficiary is served by hospices of equal quality to those serving TM beneficiaries, MA beneficiaries in Special Needs Plans and Medicare-Medicaid plans were served by lower-quality hospices than those in TM. 20 It is unclear if MAOs steer different populations to hospice compared to those electing hospice in TM, and assessing this is complicated by the different demographics of MA enrollees compared to those in TM. 21 For example, MA organizations may strategically use care management or serious illness programs to focus on high-cost members with particular serious illnesses, such as individuals with metastatic cancers, with a goal of increasing hospice use. This may increase hospice use for these populations, but not for others. In this study, we use a counterfactual model that allows us to apply the predictors of hospice use among decedents in MA to those in TM. This approach helps us to understand if hospice use is particularly high (or low) for any sociodemographic or illness subpopulations in MA, which in turn may give insight on why hospice use is higher and how expanding MA enrollment will impact hospice access.
Methods
Data and cohort
We use data from the Medicare Current Beneficiary Survey (MCBS) from 2010 to 2022, excluding data from 2014 as the MCBS did not release data from that year. The MCBS is a nationally representative survey of Medicare enrollees, linked to Medicare claims, who are followed for 4 sequential years or until death. 22 We included decedents age ≥65 at death, excluding those with missing values for key measures. This study was approved by the Icahn School of Medicine at Mount Sinai Institutional Review Board.
Key measures
Enrollment in TM or MA was determined via MCBS files and defined as enrollment in TM or an MA plan in the month of death. Given that prior research has demonstrated that beneficiaries are likely to leave MA in the last year of life, and particularly after hospice enrollment, as a sensitivity analysis, we additionally defined MA and TM status 365 days prior to death. Hospice use was defined as having any hospice claim in the last year of life. Sociodemographic, health, and regional characteristics were obtained from the MCBS survey, using the last survey conducted prior to death and substituting prior-year survey responses in the case of missing data. These included age at death, sex, race and ethnicity, census region, education, last reported housing type (private home, non-nursing home residential setting, and nursing home), any receipt of help for activities of daily living (dressing, bathing, toileting, eating, transferring in/out of a chair, and walking). Serious illnesses, also obtained from survey data, were defined as ever having received a diagnosis of: dementia, cancer, stroke, heart disease, or lung disease. Every having a serious illness was defined as having any of the listed conditions.
Analytic approach
We first compared the sociodemographic, health, functional, and regional characteristics of decedents in MA versus TM. Among decedents in MA, we then built a logistic regression model predicting use of hospice and adjusting for all sociodemographic, health, and regional characteristics as well as year of death. We then saved the predicted rates of hospice based on this model and applied the model to those in TM. This allowed us to compare the observed rate of hospice use among decedents in TM versus the predicted rate (i.e., the predicted rate of hospice use based on the actual use in the MA population). We then calculated the difference between the observed and predicted rates of hospice use in the entire TM population and in each subgroup as defined by sociodemographic, health, and regional characteristics. All analyses used survey commands and weighting to account for MCBS sampling and design and were performed with Stata 17.0.
Results
We identified 5837 decedents, 5542 of whom were age ≥65 at the time of death, and 5153 who had complete data for all key measures. An estimated 35.3% were enrolled in MA at the time of death, ranging from 21.7% in 2011 to 49.4% in 2022. Of those who were in MA 365 days prior to death, 3.6% subsequently switched to TM, and of those who were in TM 365 days prior to death, 3.9% subsequently switched to MA. As shown in Table 1, decedents in MA were younger (30.2% were age 65–75 in MA versus 24.1% in TM), less likely to be non-Hispanic White (73.9% vs. 81.7% in TM), and more likely to be Hispanic (11.1% vs. 4.9% in TM). They were more likely to live in the community at death (75.7% vs. 68.1% in TM) and less likely to live in a nursing home (13.3% vs. 20.1% in TM). They were less likely to have ADL impairments on the last survey prior to death (59.8% vs. 66.4% in TM), to have dementia (34.4% vs. 47.7% in TM), stroke (22.3% vs. 25.7% in TM), and heart disease (42.3% vs. 57.6% in TM). They were more likely to have none of the measured serious illnesses (13.1% vs. 6.9% in TM). They were less likely to live in the Northeast (15.4% vs. 19.0% in TM) and more likely to live in the West (23.3% vs. 17.7% in TM).
Characteristics of Decedents by Medicare Enrollment Type
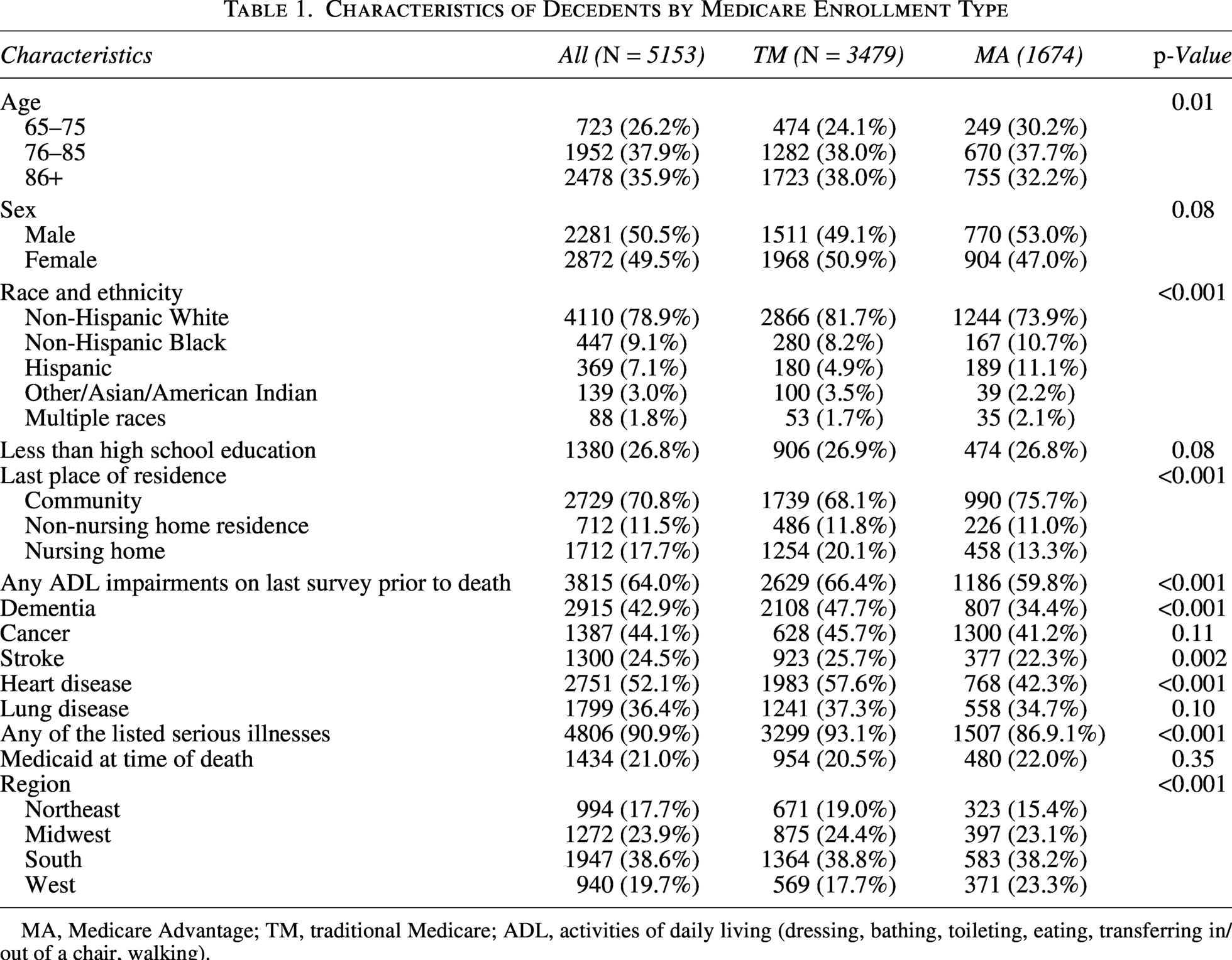
MA, Medicare Advantage; TM, traditional Medicare; ADL, activities of daily living (dressing, bathing, toileting, eating, transferring in/out of a chair, walking).
Applying the logistic regression predicting hospice use among those in MA to those in TM, we found predicted differences in hospice use for those in MA versus TM, as described in Figure 1. If the rates of hospice use observed in MA were applied to the entire TM population, hospice use would have been 6.1% higher (95% CI 3.4%−8.8%). Across some individual characteristics, the association differed: for example, for those with less than a high school education, hospice use was predicted to be 4.6% (95% CI 1.3%−7.9%) versus 10.1% (95% CI 6.5%−13.8%) for those who completed high school. There were not meaningful differences in the impact of MA on hospice use by age, sex, race and ethnicity, residence, or function. The predicted impact of MA enrollment on hospice use differed more across illness categories: for those with dementia in TM, MA enrollment was predicted to increase the rate of hospice use by 10.1% (95% CI 6.9%−13.3%) compared to 2.5% (95% CI 2.3% decrease–6.1% increase) for those in TM without dementia. For those with cancer, MA enrollment was predicted to increase hospice use by 9.1% (95% CI 5.5%−12.8%) versus 3.5% (95% CI 0.3%−6.8%) for those without cancer; for those with stroke 11.8% higher (95% CI 7.5%−16.1%) versus 4.1% higher (95% CI 1.0%−7.2%) for those without stroke; and for lung disease, 9.4% higher (95% 5.6%−13.1%) versus 4.1% higher (1.0%−7.3%) for those without lung disease. Indeed, for the majority with any of the serious illnesses, the rate of hospice use in MA was predicted to be 7.1% higher (95% CI 4.2%−10.0%) versus 7.6% lower (95% CI 16.5% lower–1.3% higher) for those without any serious illness.
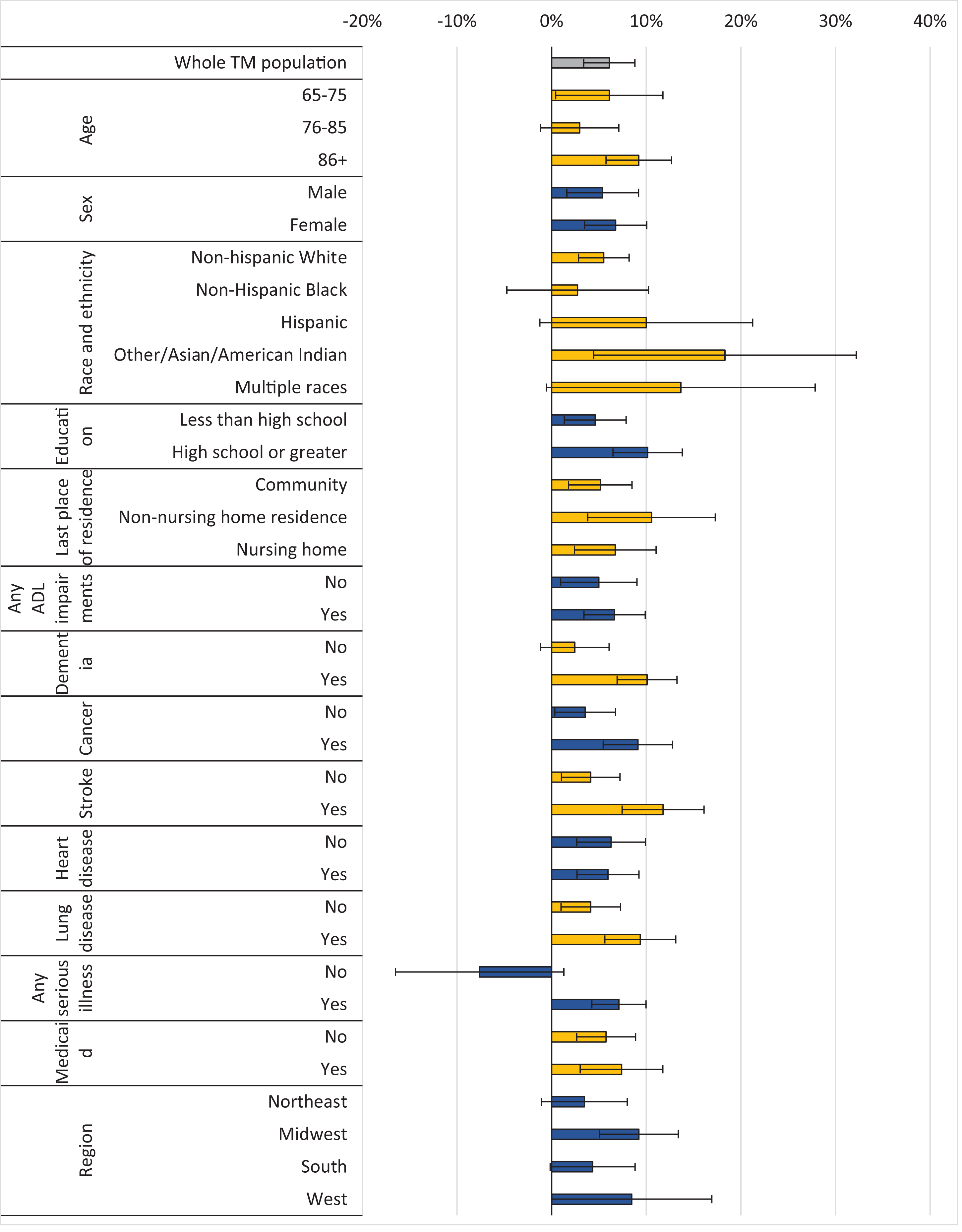
Percentage point higher hospice use if the population were in MA (counterfactual) versus TM (observed).
In our sensitivity analysis ascertaining MA and TM status 365 days prior to death, 51.6% in MA received hospice and 49.5% in TM. Among the entire TM population in this analysis, hospice use would have been 5.9% higher (vs. 6.1% higher in our primary model) when applying the enrollment patterns seen in MA (95% CI 3.4%−8.4%). Table 1S in the Supplementary Appendix displays the full counterfactual model results.
Discussion
This study shows that although hospice enrollment rates are slightly higher in MA than in TM, hospice enrollment varies across beneficiary characteristics in different ways across the two programs. Higher hospice enrollment in MA is observed among beneficiaries with higher levels of education and among those with certain serious illnesses (e.g., dementia, cancer, stroke, and lung disease), relative to similar beneficiaries in TM.
Our study findings must be contextualized in the challenges of assuming causality in observational studies assessing the MA program, given the differences in who decides to enroll in MA. For example, decedents with dementia are far less likely to be in MA versus TM, but among decedents with dementia, hospice use is higher among those enrolled in MA than among otherwise similar decedents in TM. While hospice has been shown to improve end-of-life care quality, higher hospice use among MA decedents should not be interpreted as evidence of a causal benefit of MA enrollment, particularly given known selection into and out of MA. 23 It is possible that other negative experiences in MA lead people with dementia to avoid or switch out of MA and into TM.11,15,24 Both quality measures capturing experience in MA, such as hospice use, as well as a deeper understanding of why some populations enroll in MA at lower rates, are necessary to appropriately measure quality. While it is challenging to imagine a study design that approaches causality (given the difficulty of assigning MA enrollment to a given population), future research leveraging qualitative interviews with hospices, MA organizations, and people with serious illness will help us to understand what is driving observed patterns.
There are several potential explanations for why hospice use might be higher in MA and specifically among those with particular serious illnesses at the end of life that are worth of further examination. First, the carve-out of hospice may incentivize MAOs to steer decedents with high levels of utilization (relative to the amount that the MA plan is paid from CMS to insure the individual) to hospice. The serious illness populations we study have particularly high levels of utilization.25–27 In addition, under the carve-out, CMS continues to pay MAOs large premium and rebate payments for beneficiaries electing hospice, and yet the MA plan is only responsible for costs not related to the beneficiaries’ terminal illness. 28 This may further create financial incentives for MAOs to steer beneficiaries to hospice. Individuals with specific serious illnesses, such as cancer or dementia, may be easier for MA organizations to identify via claims analyses as high utilizers who may be hospice eligible. 27 MA organizations may then be able to use mechanisms like care management or palliative care that could result in higher hospice use. 29 Alternatively, MAOs might consider rates of hospice referrals when building networks of providers and facilities, or MAOs may be selecting markets for expansion where hospice use is high for reasons not driven by the MAO, such as regional end-of-life treatment intensity. 30 Further research to identify which mechanisms are most contributing to higher hospice access may inform initiatives to increase hospice use in TM, such as through accountable care organizations and health systems.
Our analysis is strengthened by the counterfactual approach and our ability to include a range of covariates (e.g., functional status, residential setting); however, we are likely still limited in our ability to account for all the characteristics that are associated with selection into an MA plan. Given the lower proportion of decedents in MA with specific serious illnesses, it is possible that those who are enrolled are different than their counterparts in TM in ways that we cannot measure. While we can hypothesize about the mechanisms of higher hospice use, we lack direct data on the provision of services like palliative care that could help us to understand this higher rate, and further qualitative work will be useful to examine the reasons for greater hospice use in MA. Our data are from 2010 to 2022, during which time rates of MA enrollment among Medicare beneficiaries ranged from 25% to 48%. 31 While our models account for secular trends over this period, we do not yet have available data to assess if the association between MA enrollment and hospice use is changing, as MA is now the dominant source of insurance for Medicare beneficiaries. When we characterize dementia rates in hospice, as for other conditions, we cannot ascertain if dementia is a comorbidity or the terminal illness, which is challenging to ascertain from claims data. 32 Finally, we are not able to survey decedents on their care preferences or on any differences capturing reported quality of end-of-life care, which other studies have shown is worse in MA. 13
As enrollment in MA continues to grow dramatically, it becomes more crucial to understand not only the differences in health care utilization, such as hospice use, in MA, but the mechanisms for these differences. Mixed-methods research is needed to understand how insurers may be shaping hospice use, such as through care management programs to identify beneficiaries who might qualify for hospice or supplemental benefits providing palliative care with the goal of increasing hospice use. Identifying the mechanisms by which MA plans increase hospice use may serve to inform efforts to innovate hospice delivery in traditional Medicare. Furthermore, qualitative interviews of people with serious illness and their caregivers regarding their preferences for insurer involvement in shaping end-of-life care are critically important given the ethics and perceptions of insurer motivations. This will both provide insight in how to expand access to hospice throughout the TM program and to ensure that all Medicare beneficiaries receive the highest possible end-of-life care.
Footnotes
Acknowledgments
The authors did not use generative AI or AI-assisted technologies in the writing process for this article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
C.K.A. and M.D.A. are funded by the