
Abstract
Case reports serve an important entry point for scholarship in palliative care (PC), yet many clinicians lack a practical roadmap for moving from an interesting encounter to a publishable article. In this inaugural article for the Journal of Palliative Medicine “Scholarly Skills Series,” we provide a concise, replicable framework for writing case reports with a PC lens. We focus on the PC adaptation of the CAse Report (CARE) guidelines while providing a structured three-phase framework. Organized into a “Before, During, After” structure, we outline key steps and common pitfalls, including selecting a publishable case, establishing authorship roles, obtaining informed consent, conducting a literature search, and framing the report using the CARE guidelines. We offer pragmatic guidance on article construction, journal targeting, submission logistics, and navigating revision, rejection, and resubmission. A summary table of “Do’s and Don’ts” highlights actionable practices to streamline the process and improve the likelihood of publication. This guide is designed for those seeking a standardized approach that supports academic development, team-based and trainee scholarship, and dissemination of clinically meaningful lessons in serious illness care to positively impact patient care outcomes.
What Are Case Reports and Why Are They Important?
Case reports are concise, focused, and structured articles that highlight an interesting or unique clinical case. 1 They detail a patient’s medical condition (symptoms, signs, diagnosis, treatment, and follow-up) in a way that supports clinical learning, advances medical education, and can spark hypotheses for future research. 2 A strong case report distills clinical experience into a teachable unit by highlighting a new or easily missed insight, clarifying how clinicians should recognize a pattern, or illustrating a management decision that improves care.
They serve as an accessible entry point into scholarship in the academic ecosystem, with a favorable effort-to-yield ratio when a case has a clear teaching point. The process of writing a case report builds transferable skills in literature appraisal, academic writing, project management, and dissemination. Case reports are well suited to team-based scholarship because they can involve the interdisciplinary team and learners with appropriately scoped roles. For many clinicians, writing a case report can serve an additional function as a structured way to process a clinically and emotionally demanding encounter, transforming moral distress, ethical tensions, or uncertainty into a teachable narrative that benefits future patients and teams. 3
In palliative care (PC), case reports serve additional functions because the specialty routinely navigates complexity that is not easily captured in trials or large datasets. 3 A well-crafted PC case report can illuminate nuanced symptom management, communication challenges, goals-of-care (GOC) discussions, family and caregiver dynamics, and the systems-level barriers that shape serious illness care. For readers outside the subspecialty, PC case reports offer a practical window into the clinical and values-based reasoning that underpins palliative approaches and can translate directly to care in other settings.
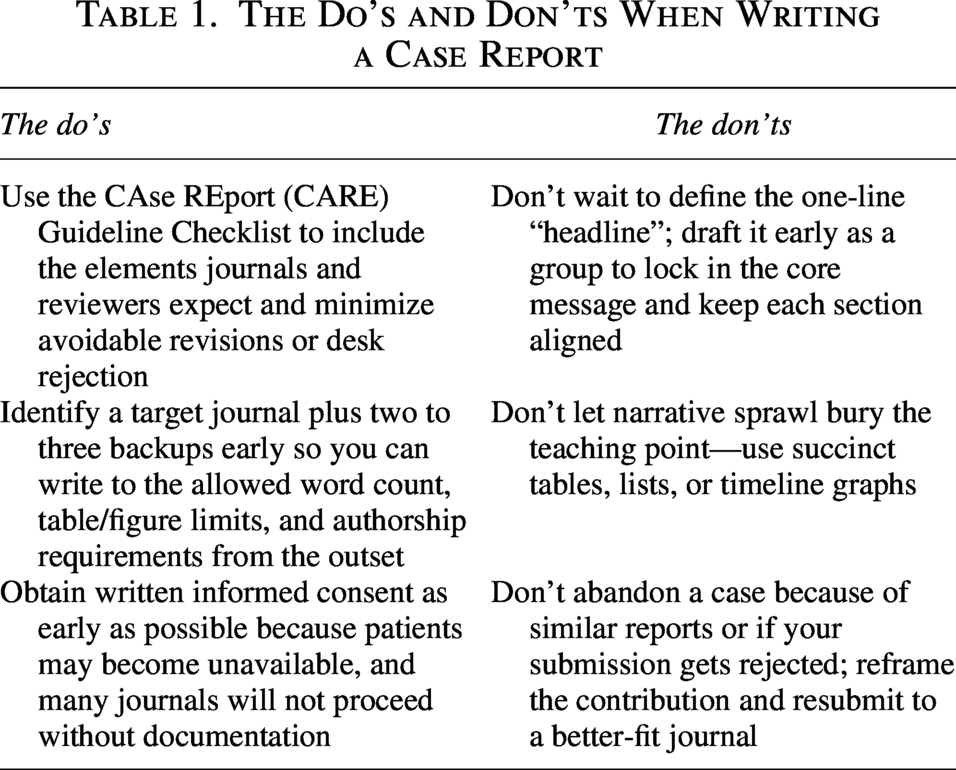
Despite their value, many clinicians lack a clear roadmap for moving from an interesting clinical encounter to a publishable article, particularly in the setting of competing clinical demands and limited formal training in writing and publication. Using a three-phase structure—Before, During, and After—we offer a practical, PC-centered framework for case reporting. Table 1 summarizes practical “Do’s” and “Don’ts” to streamline the process and increase the likelihood of successful publication.
The Do’s and Don’ts When Writing a Case Report
Before Starting a Case Report
Prewriting
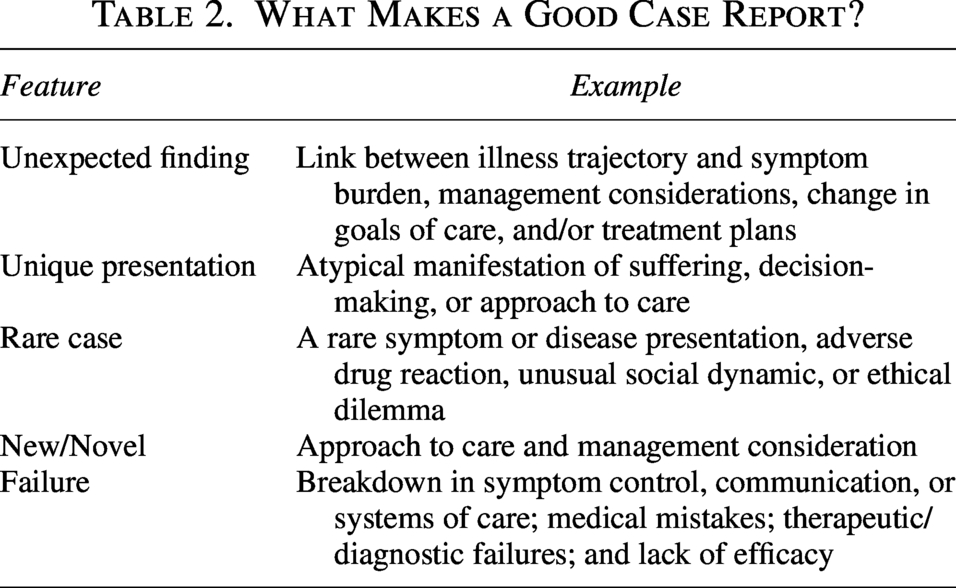
Determining whether you have a publishable case depends as much on framing as it does on rarity or impact. In practice, most cases can be published if the teaching point is well-framed and the narrative is disciplined. Table 2 outlines classical categories of case reports that lend themselves well to publication. 4 Systems and process failures are often especially publishable in PC because they expose barriers, inequities, and communication breakdowns that affect patient outcomes, with the aim for publication to improve quality care. A well-written case report can help not only to broaden the impact of the clinical case beyond other providers’ clinical practices but also to include impacts to other departments or a hospital system.
What Makes a Good Case Report?
Once decided that a case is worth writing, the next task is to define the “headline,” a one-sentence statement of what the reader should do differently in practice. A strong headline is action-oriented and clinically directive, prioritizing one dominant teaching point and using the case details to support it. For example, “severe dyspnea in end-stage heart failure alleviated with low-dose morphine” or “management of opioid-induced neurotoxicity in advanced illness.” It also serves as a scope statement for the writing team, guiding what to include, what to cut, and how to structure the discussion toward a concrete, bedside-relevant conclusion. This discipline prevents unfocused, long sections and helps reviewers see why the case matters. A useful checkpoint is whether a reader can scan the title and the first paragraph of the discussion and state the teaching point without ambiguity.
In practice, cases that evoke strong emotions often provide the motivation to do the work of writing and publishing, which is an asset in a busy clinical environment. At the same time, emotional resonance can be a poor proxy for publishability. Even when a case feels powerful, it still needs a clear, generalizable teaching point, and attachment does not automatically create novelty. A useful reality check is whether you can name the lesson in one sentence. If possible, clarify what others would learn and sharpen that message into a strong headline, as a lack of clarity would likely receive a rejection. For example, caring for a refugee with ALS may evoke emotions in the care team warranting consideration for publication. “Use of communication tools by the interdisciplinary team to provide trauma-informed care in the setting of ALS” is a more pointed headline than “Palliative Care in ALS.”
Literature search
A focused literature search early in the process helps position the case within existing scholarship, clarify what is already known, and define what your case adds. Comprehensive instruction on literature searching is beyond the scope of this article, and the basic process is similar to literature searches used for other scholarly and clinical endeavors. 5 For case reports, however, a practical stopping rule is to search until you can support three points with citations: What is known, what remains uncertain, and what your case adds.
To ensure a PC lens, consider a simple two-lane approach. One lane focuses on the clinical topic, such as diagnosis, symptom syndrome, intervention, or adverse effect. The other lane focuses on the PC context that makes the case consequential, such as serious illness, hospice, end-of-life decision-making, GOC, symptom tradeoffs, caregiver experience, clinician distress, ethics, equity, or care transitions. For example, search terms may include Opioid Induced Neuropathy + advanced illness, in the aforementioned example. Combining these lanes clarifies where the novelty lies in PC, which is frequently less about rare pathophysiology and more about decision-making under uncertainty, communication, and systems barriers.
Trainees can contribute meaningfully to this step when given a clear question and a defined output for the team. They can run an initial search in databases such as PubMed/MEDLINE, Google Scholar, and others, then return a brief synthesis aligned with the case headline. 5 Features such as “similar articles” and “cited by” can help expand efficiently and track emerging work in evolving or interdisciplinary areas. When available, partnering with an institutional medical librarian can further improve the rigor and efficiency of the search.
A reference manager can make the literature-search phase substantially more efficient and prevent downstream rework. Tools such as Zotero, EndNote, or Mendeley allow teams to store PDFs, deduplicate results, tag and annotate key articles, and maintain a shared library aligned with the case headline. 6 This becomes especially helpful during drafting and resubmission because citations can be inserted directly into the article and then reformatted to a new journal style with minimal effort.
The key interpretive step is deciding whether your case adds something meaningfully distinct. A common error is concluding that a case is not worth writing because related reports already exist. Similar reports can validate that the topic is publishable and help you identify a distinctive angle, such as a specific risk factor, a management nuance, a unique setting, or a PC perspective. Existing reports can also serve as practical templates for structure and framing and signal that editors and reviewers already recognize the topic’s relevance.
Case capture
During the prewriting phase, it also helps to be intentional about case capture. Many clinicians keep an “interesting cases” list in the EMR, with brief, non-identifying reminders of what made each case notable. This habit reduces missed opportunities and supports scholarship even when clinical workload delays writing. Clinicians outside your specialty may help identify what is unusual or high-impact in your case, and experienced mentors often have “unwritten cases” that can become collaborative projects. These strategies help prevent a common barrier, since many of the most interesting cases are recognized only in hindsight, when key details are harder to reconstruct.
Journal selection
Journal selection should occur before drafting, as journal requirements shape the article’s format and scope. In addition to fitting with the headline, authors should consider practical constraints such as word count, the permitted number of authors, limits on tables and figures, expectations for the depth of the literature review, and whether the journal is subscription-based or open access. Many PC clinicians also publish case-based work outside of PC journals when the primary teaching point is best matched to a non-PC specialty audience. Approached systematically, journal selection becomes the process of matching the headline to the most appropriate article format, then generating a short list of realistic destinations that can accommodate the structure, length, and authorship team anticipated.
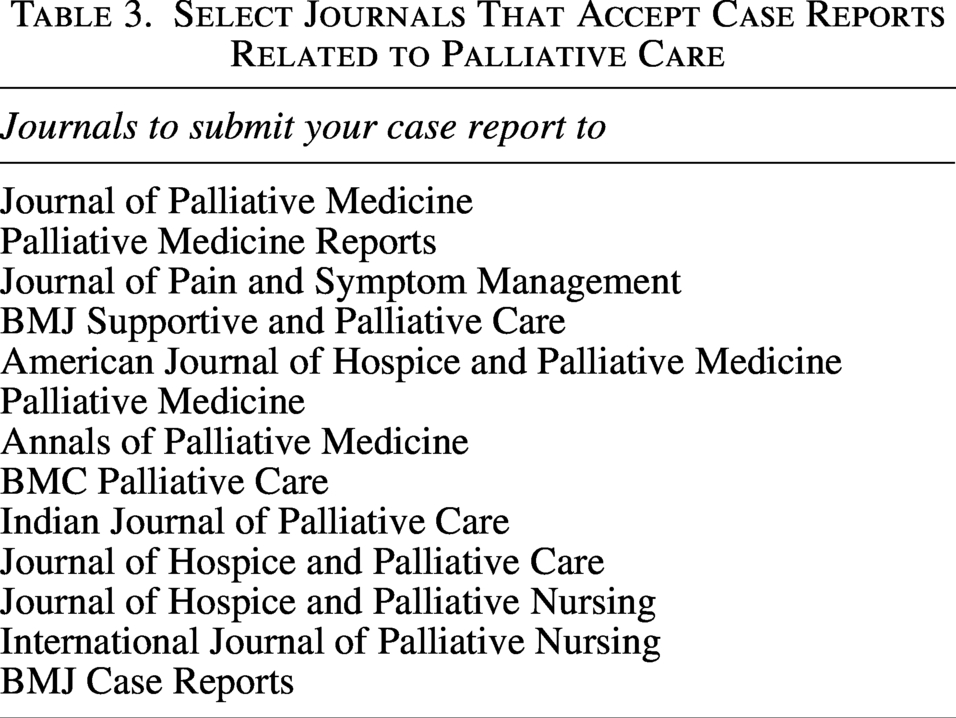
It is also important to recognize that a “case report” is not a single format. Common options include a letter to the editor, a traditional case report, an image-based or brief clinical communication, a case conference format, and, in some journals, a video or medical education format. These categories differ in length, acceptable complexity, and the amount of interpretive work expected from authors. A letter to the editor or brief report can be ideal when the teaching point is narrow, the key data are straightforward, and the goal is rapid dissemination. A traditional case report is often the best fit when the case requires more clinical context or when the discussion needs enough space to synthesize the literature and articulate a PC lens. A case conference format may be most useful when the educational value hinges on differential diagnosis, uncertainty, or clinical reasoning that evolves over time. Some journals also accept image- or figure-centered case formats, which work well when a single photograph, radiograph, waveform, or timeline is the clearest way to teach the point. Table 3 provides a list of journals one may consider while reviewing journal options.
Select Journals That Accept Case Reports Related to Palliative Care
In open access publishing, the final article is freely available to readers, but authors may be charged an article processing fee. Plan for this early, since the cost can determine whether a journal is feasible. If departmental, institutional, or grant support is not available, it is often best to prioritize journals without processing charges rather than discovering the barrier at the end of the process.
In parallel, novice authors should actively screen for predatory journals. When in doubt, authors can check whether a journal is indexed in reputable databases, review previously published articles for quality and fit, and seek mentor or librarian input; reference Beall’s list before submitting. 7 Practical warning signs include unsolicited email invitations to submit, vague or overly broad journal scope, unrealistic promises of rapid acceptance, unclear or absent peer review processes, nontransparent fees, and editorial boards that are difficult to verify. Other resources to reference include the Committee on Publication Ethics and Directory of Open Access Journals.8,9
Selecting a target journal is inseparable from selecting backup journals. Rejection is common for case reports, so it is practical to identify two to three backup journals that accept the same article type and have similar formatting, word counts, author limits, and consent policies. 10 This forethought prevents a common workflow challenge: Drafting an article that cannot be easily resubmitted after rejection because the backup journals require a different structure or permit fewer authors. Some journals offer transfer to a related “journal family” title, which can reduce administrative burden and avoid full resubmission. Transfer options are helpful but should not replace the discipline of selecting plausible backups in advance.
Consent
Written informed consent and privacy planning should also be handled early, ideally while the patient is still available, as failure to obtain consent is a common reason promising work never becomes publishable. Journals frequently require written consent on specific forms, and some institutions have additional requirements even when a journal does not. It is advised to review these forms to help guide the consent process. Verbal permission is often insufficient. De-identification alone may not adequately protect patients, particularly in rare or distinctive cases where re-identification risk is higher.
In PC, authors should apply a high ethical standard even when journal requirements seem permissive. Teams should understand the consent expectations of the target and backup journals, obtain written consent before drafting when possible, and store documentation according to institutional policy, often including placement in the medical record. There is additional complexity in obtaining consents posthumously—consent from next of kin may be permissible depending on journal policy. If the patient has a guardian, consent may be sought from the legally authorized representative, recognizing that this may be logistically challenging in some systems. When cases involve photographs, radiographical imaging, or other potentially identifying materials, teams should assume higher identifiability risk and follow the most conservative applicable consent and privacy standards.
Team dynamics
Success in case reporting, as in other academic writing, depends on assembling a functional authorship team and setting explicit expectations early. When roles, author order, and deadlines are not clarified at the outset, projects commonly stall or generate conflict. 11 This “authorship ambiguity” is among the most preventable barriers, and it often reflects mismatched assumptions about what each contributor will do, including what mentorship entails.
Mentorship, while not specific to case reports, is best understood as coaching, critical review, and conceptual guidance rather than an expectation that senior authors will rewrite the article at the end. Although full guidance on mentorship and conflict resolution is beyond the scope of this article, early agreement on responsibilities and timelines helps prevent confusion and miscommunication later. 11
The author instructions page for the target journal should be reviewed early so that expectations align with the team’s goals and the planned article type. The team can decide whether the first author will draft the entire article or whether sections will be divided across authors, but all authors should meet the International Committee of Medical Journal Editors authorship criteria, including contribution to the concept or analysis, drafting or critically revising the work, final approval, and accountability for the work. 11
Regardless of workflow, teams benefit from a shared understanding that the first author is responsible for managing edits, producing the final draft, and communicating with the journal throughout submission and revision. Making these expectations explicit at the outset is both a professional practice and a practical mechanism that keeps the project moving.
While Writing a Case Report
Structuring the article
A well-structured case report pairs a focused case description with a discussion that makes the teaching point explicit. Standard components include a title, abstract, introduction, case description, and discussion. The title and abstract should state the teaching point clearly and signal the intended audience. The introduction should be brief and answer why this case matters now. The case description should be tightly curated and include only details that support the teaching point, usually key demographics, the relevant clinical history, diagnostic reasoning, interventions and decision points, response to treatment, and follow-up. Writing in forward chronological order and in the past tense improves clarity, and authors should use generic medication names, include units for laboratory values, and follow institutional and journal privacy requirements. A timeline or table can help compress complexity and keep the narrative moving visually. The discussion should then synthesize the literature, explain why the case warrants attention, and translate the lesson into a practical implication for clinicians.
The CAse Report (CARE) guidelines are an international reporting standard for clinical case reports that outline essential items to include and recommend a transparent, structured way to present them. 2 Using CARE promotes consistent reporting and reduces missing or unclear information, helping readers and reviewers understand what happened, how decisions were made, and what can reasonably be concluded from the case. In practice, the CARE checklist is a drafting tool that helps authors avoid omissions, keep the narrative aligned with the teaching point, and connect the discussion to the existing literature. Many journals encourage or require CARE adherence, stating that the report follows CARE signals rigor and can increase reviewer confidence in the article’s reporting quality. Figure 1 presents a practical writing guide that integrates key CARE elements as labeled with PC-specific considerations and examples to support efficient, high-quality case report development.
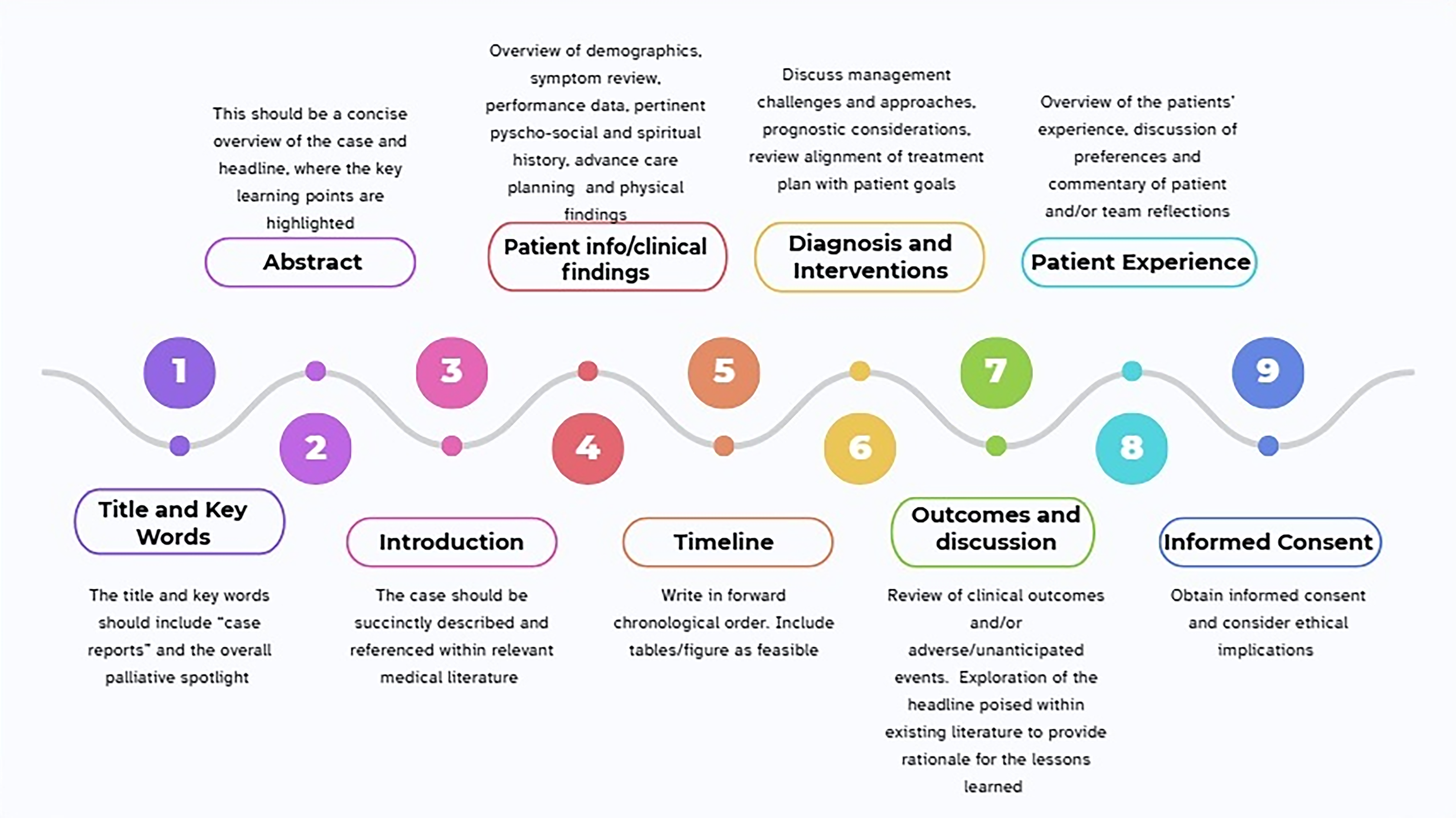
Palliative adaptation of CAse REport (CARE) guidelines.
Revision and team feedback
Once the first draft is complete, circulate it to the full author team for structured feedback with deadlines to ensure the project moves forward. Early drafts often suffer from predictable problems, including being overwritten, overly inclusive of clinical detail, and shaped more like a chart review than a focused teaching case. Lack of direction at this stage usually reflects unclear prioritization rather than a lack of content, and it can be addressed by pausing and returning to the one-line headline. Revision should focus on removing details that do not serve the teaching point, replacing rambling narrative with a tighter timeline or table when helpful, sharpening the discussion, and ending with a clear practice implication. Incorporation of edits is ultimately at the discretion of the first author; however, this should be clarified at the outset.
After Writing a Case Report
Submission
Submitting a case report is largely similar to submitting any other article and is beyond the scope of this guide to describe in detail. In most journals, authors use an online submission portal to upload the article and required forms and to communicate with the editorial office. What is more case-report specific is that there are predictable administrative friction points that can derail an otherwise strong case. Before uploading files, confirm that the article fits the journal’s operational rules, including author limits, word count, figure and table limits, and any required templates or forms. Case report submissions also commonly require documentation beyond the article itself, such as a journal-specific patient consent form or a consent attestation and, in some venues, a completed reporting checklist. A brief cover letter is usually sufficient and should state the one-sentence teaching point and why the case is relevant to the journal’s readership, without re-summarizing the full narrative.
After submission, timelines are variable. Case reports may be triaged quickly because of limited space, but if they are sent for review, decisions may take weeks to months. When revisions are invited, they usually focus on clarity and focus rather than on additional analyses. Common requests include tightening the case narrative, trimming background, clarifying the rationale for key decisions, strengthening the novelty claim in relation to prior reports, and reducing identifiable detail while preserving clinical meaning. Respond with a concise, point-by-point letter and make changes easy to locate. For case reports, it is often more effective to narrow and better support the novelty claim, clarify diagnostic or decision-making reasoning, and streamline background than to argue about rarity. If feedback repeatedly targets length or scope, consider reframing the same case into a different article type, such as a letter, brief report, or image-based vignette, rather than abandoning the work. Keeping routine correspondence centralized with the first author helps avoid duplicated or inconsistent communication and simplifies deadlines.
Rejection and resubmission
Rejection should be anticipated and normalized as part of scholarly publishing, particularly for case reports. Common reasons for desk rejection include missing patient consent or institutional documentation, failure to follow journal word limits, incomplete author contribution statements, or a mismatch between the article and the journal’s scope.
Ideally, this possibility has already been addressed by identifying appropriate backup journals before drafting. While simultaneous submission of the same article to multiple journals is not acceptable, resubmission to another journal after rejection is standard practice. When appropriate, a traditional case report may also be reframed as a brief communication, brief report, or other forms of publication.
Resubmission of work generally follows one of two strategies, depending on confidence in the original framing. If the teaching point and positioning are solid, the focus should be on efficiently aligning the article with the next journal’s requirements. This commonly includes reformatting to a new word count and revising tables or figures to meet different limits. If reviewer feedback suggests problems with clarity, novelty, or fit, take a deeper revision approach. Revisit the discussion for a new audience, tighten and appropriately narrow the novelty claim, and sharpen the “so what” so it is immediately clear to the next journal’s readers.
Reviewer comments remain useful even after rejection. They often highlight where the narrative was unclear, claims felt overstated, or the discussion did not sufficiently distinguish the case from existing reports. Incorporate this feedback when appropriate and adjust the framing and emphasis of the discussion to fit the priorities of the next journal’s audience. Thoughtful revision following rejection often strengthens the article and increases the likelihood of eventual publication.
Conclusion
Case reports are a practical entry point into PC scholarship but may feel intimidating to the unfamiliar clinician. Many clinicians and trainees lack a clear roadmap for moving from an interesting encounter to a publishable article, and we have presented a strategy to guide authors through bringing a case from the bedside to publication. Using the three-phase framework of Before, During, and After provides a practical approach to transforming clinical encounters with a clear teaching point into scholarship. This framework has limitations. It is not derived from a systematic review but instead reflects expert opinion, experiential knowledge, and established reporting guidance. Early and transparent planning, focused literature review with concurrent journal selection, and disciplined writing guided by CARE can prepare authors for the realities of submission, revision, and resubmission. This standardized, replicable process supports team-based scholarship and helps busy clinicians translate clinically meaningful lessons into publications that improve patient-centered quality care across health care settings.
Footnotes
Acknowledgment
The authors thank Dr. Craig Blinderman for invaluable mentorship and critical feedback.
Author Disclosure Statement
G.A.R.-W. is an Associate Editor of the Journal of Palliative Medicine.
Funding Information
No funding was received for this article.