
Abstract
Background:
Religious and spiritual (R/S) concerns are common among patients with serious illness. Attending to the R/S concerns of patients is a core component of quality palliative care.
Objectives:
Our aim was to describe the prevalence and demographic, medical, and religious correlates of R/S concerns in patients receiving palliative care.
Design:
Multisite, cross-sectional study.
Setting/Subjects:
Adult patients in the United States receiving inpatient or outpatient palliative care.
Methods:
Chaplains completed the PC-6, an interview-based spiritual assessment, as part of routine palliative care practice. The PC-6 evaluates six domains of R/S concern: relationships, meaning, legacy, dying, religious/spiritual struggle, and treatment decision-related concerns. Demographic, clinical, and religious affiliation data were obtained from the medical record.
Results:
A total of 172 palliative care patients were included. Fifty percent were assessed to have moderate or severe concerns in at least one of six spiritual domains, and 17% had concerns in two or more domains. The most prevalent concerns involved relationships (19.2%), dying (14.5%), meaning (14.0%), and legacy (11.0%). In multivariable analyses, patients with no religious affiliation were more than three times more likely to have moderate or severe spiritual concerns compared to those with a Protestant affiliation. Demographic characteristics and primary diagnosis were not associated with the presence of spiritual concerns.
Conclusions:
Moderate to severe spiritual concerns are prevalent among patients receiving palliative care, including among those without a religious affiliation. Integrating spiritual assessment into palliative care workflows may facilitate specialty spiritual care and comprehensive attention to patients’ multidimensional suffering.
Key Message
Using a chaplain spiritual assessment, this multisite study demonstrates that moderate to severe spiritual concerns are prevalent among palliative care patients. Routine use of the PC-6 may improve recognition of spiritual distress in palliative care patients at the end of life and support timely delivery of specialty spiritual care.
Introduction
For many patients receiving palliative care, religious and spiritual (R/S) beliefs and practices provide a framework for understanding suffering, cultivating meaning, and sustaining hope in the face of declining health and mortality.1–3 A growing body of evidence demonstrates that higher levels of R/S beliefs and practices are associated with improved quality of life, greater emotional well-being, and longer survival.4–9 Yet not all R/S coping is adaptive. Alongside positive forms of coping, such as faith, forgiveness, and connection, many patients experience R/S struggle, sometimes referred to as spiritual distress or spiritual pain. These experiences may include loss of meaning, anger toward God, abandonment, guilt, or conflict with faith communities.10–12
The reported prevalence of spiritual distress among patients with advanced illness is wide, ranging from 10% to 80%; variations in population and measurement may account for this.7,13–15 Using the 14 item Religious and Spiritual Struggles (RSS) scale, a study of 331 PC patients found that 66% experienced some level of R/S struggle, and 20% experienced moderate to high levels.10,13 Using a single-item measure of spiritual pain, a study of 292 PC patients found 22% had mild spiritual pain and 21% had moderate-to-severe spiritual pain. 16 Various levels of R/S distress have also been reported for palliative care patients outside the U.S., including 17% with spiritual distress in India, 57% with moderate/severe spiritual pain in Chile, and 89% longing for peace and contentment in Turkey.17–19
This research also reports on the prevalence of different domains of R/S distress. In a study by Damen and colleagues, the prevalence of R/S distress ranged from 17% for demonic struggles to 32% for interpersonal struggles. 13 In a study of 113 palliative care inpatients, a chaplain assessment found 32% experiencing despair. 20 While reports of the prevalence of R/S distress vary, the evidence of its harmful effects is consistent, including greater pain or symptom burden, more depressive symptoms, and poorer quality of life.1,7,8,13,16–18
Some studies that have examined the prevalence of R/S distress have also examined its predictors, including demographic, medical, and R/S factors. While several studies have found younger age to be associated with greater R/S distress,15,18,20 other studies found age, gender, and education were not predictors of R/S distress.13,14 R/S distress has been found to be associated with greater pain and symptom burden.13,20 One study found lower self-rated religiosity was associated with greater spiritual pain, 21 but another study found no associations between R/S struggle and three measures of religiousness. 13
Most of the research examining the prevalence of R/S distress has used survey items for measurement. Only three studies report findings from clinician-rated R/S distress; two of these studies involved chaplains, and one relied on non-chaplain clinicians. In a study by Haufe and colleagues, 387 non-chaplain clinicians used the Diamond Conversation Model to determine that patients most commonly experienced distress related to pain and suffering (88%), difficulty letting go (82%), conflicts related to end of life wishes (69%), unresolved past issues (67%), and the meaning of death (67%). 22 Hui and colleagues described spiritual distress among 113 PC inpatients, using a spiritual assessment conducted by the site’s chaplain. 20 They found distress in 44% of patients across seven existential and religious domains including despair, dread, and brokenness. 20 Kestenbaum and colleagues have described how chaplains assessed the spiritual needs of 156 cancer patients in an outpatient PC clinic, using the Spiritual AIM assessment model. 23 They identified issues of self-worth for 55.3%, of meaning and direction for 21.3%, and a need to love and be loved among 10.6% of these patients. 23
The present study used a chaplain spiritual assessment to examine R/S concerns in a multisite cohort of patients receiving palliative care. In this study, we used the PC-6, a validated spiritual assessment developed specifically for palliative care chaplains to measure the intensity of R/S concerns.24,25 We examined the prevalence and demographic, medical, and religious correlates of R/S concerns with the aim of identifying which patient factors may signal heightened spiritual needs.
Methods
Participants
Participants in the present study primarily came from five medical centers, three in the Midwest and one each in the Northeast and South. Of these, four were academic medical centers; two of the five institutions were faith-based. Two other facilities (an academic medical center and senior living community) contributed several cases before withdrawing from the study due to recruitment challenges. Two-thirds of the participants (N = 110) in the present project were also participants in another study about the PC-6. 25 All centers recruited inpatients; one site also recruited outpatients, and another included outpatients and home care patients. Eligible participants were English-speaking patients aged 18 years or older who had received a referral to the PC team for discussion of goals of care. Data were collected from March 2021 to February 2024 and overlapped the COVID-19 pandemic. The IRB of each participating site approved all study procedures.
Measures
The PC-6 Spiritual Assessment. The PC-6 is an interview-based, chaplain-completed assessment of the intensity of R/S concerns in palliative patients.24,25 Six R/S concerns are assessed: need for meaning in the face of suffering; need for integrity, a legacy; concerns about relationships; concern or fear about dying or death; issues related to treatment decision-making; and R/S struggle. These six domains reflect an intentionally holistic conceptualization of spirituality in palliative care. Although domains such as relationships, meaning, and legacy include content that may also be characterized as psychosocial, they are treated as core dimensions of spiritual well-being because they address existential sources of suffering and connectedness near the end of life, consistent with consensus frameworks that define spirituality in serious illness as encompassing relational and existential dimensions alongside explicitly religious ones.1,2
After the assessment interview, the chaplain rates each spiritual concern on a 4-point scale where 0 = no evidence of spiritual concern, 1 = some evidence, 2 = evidence of moderate spiritual concern, and 3 = evidence of severe concern. Specific indicators distinguishing levels of concern within each domain, along with inter-rater and intra-rater reliability data supporting the consistency of chaplains’ ratings, are detailed in the PC-6 development and validation studies.24,25 Clinically, this approach prioritizes concerns that exceed the patient’s internal coping resources and thus warrant specialist spiritual care. Scores of 1 on the 0–3 scale reflect minimal or well-managed concerns that do not typically rise to the level of spiritual distress. For analysis, the score for each theme is dichotomized: ratings of 2 (moderate) or 3 (severe) are treated as indicating clinically significant concerns and assigned a value of 1, while chaplain ratings of 0 or 1 are treated as 0. This yields a total PC-6 score ranging from 0 to 6, reflecting the number of themes with moderate to severe concerns.
Palliative Performance Scale (PPS). The PPS, a modified version of the Karnofsky Performance Scale, measures 5 functional domains: ambulation, activity level and evidence of disease, self-care, oral intake, and level of consciousness. 26 Its scores range in 10% increments from 0% to 100%, with a score of 0% indicating death, 10% indicating a totally bed-bound patient who is unable to do any activity and needs total assistance, and 100% indicating the patient can carry on normal activity and work without any special care. For purposes of analysis in this study, PPS scores were converted to an ordinal scale ranging from 1 to 11 corresponding to the original 0%–100% increments. Information regarding age, gender, race, ethnicity, marital status, religious affiliation, primary diagnosis, time since diagnosis, PPS, and treatment setting (inpatient vs. outpatient or home care) were extracted from the patients’ medical records.
Analysis
Descriptive statistics were used to report demographic and clinical characteristics of the sample, including frequency and percent for categorical variables and mean and standard deviation (SD) or median and interquartile range (IQR) for numerical variables. Because the PC-6 score was heavily skewed, it was dichotomized to no spiritual concerns (PC-6 score = 0) and any spiritual concerns (PC-6 score ≥ 1). Bivariate associations between categorical variables and PC-6 score were evaluated using the chi-square test. Where cell counts remained less than 5, Fischer’s exact test was used in place of the chi-square test. Numerical variables (PPS, time since diagnosis) had non-normal distributions based on the Shapiro-Wilk test and were analyzed using the nonparametric Mann–Whitney U test to evaluate association with PC-6 score.
For analysis related to religious affiliation, we chose Protestant affiliation as the reference category, as it was the largest. We used logistic regression for multivariable analysis of predictors of PC-6 scores. Although missing values represented less than 3% of data for each variable, multivariable regression would see missingness compounded to almost 10% of the cases in the dataset (n = 16). Multiple imputation was utilized to fill in missing values with estimated values. Five imputations were conducted, resulting in five independent complete datasets that were then analyzed; results of each analysis were pooled to achieve a single analytic result. All analyses were conducted using IBM SPSS Statistics (Version 29). Statistical significance was set at a two-tailed p value of 0.05.
Results
A total of 172 patients were included in the study. Patients’ mean age was 62.7 years (SD = 15.4; range 22–94 years) and the sample was majority female (62.2%). Among the study participants, 82.7% identified as White and 13.1% as Black; 47.3% were married or partnered. Most patients identified as Protestant (52.1%), followed by Catholic (19.2%), with 15.6% having no religious affiliation. The most common primary diagnosis was cancer (60.6%). The median time since diagnosis was 12 months (IQR: 2.4–46 months). Patients’ mean PPS score was 5.4 (SD = 1.4), and 72% of patients participated in the study while in the inpatient setting [Table 1].
Patient Sample Characteristics and Spiritual Concern (N = 172)
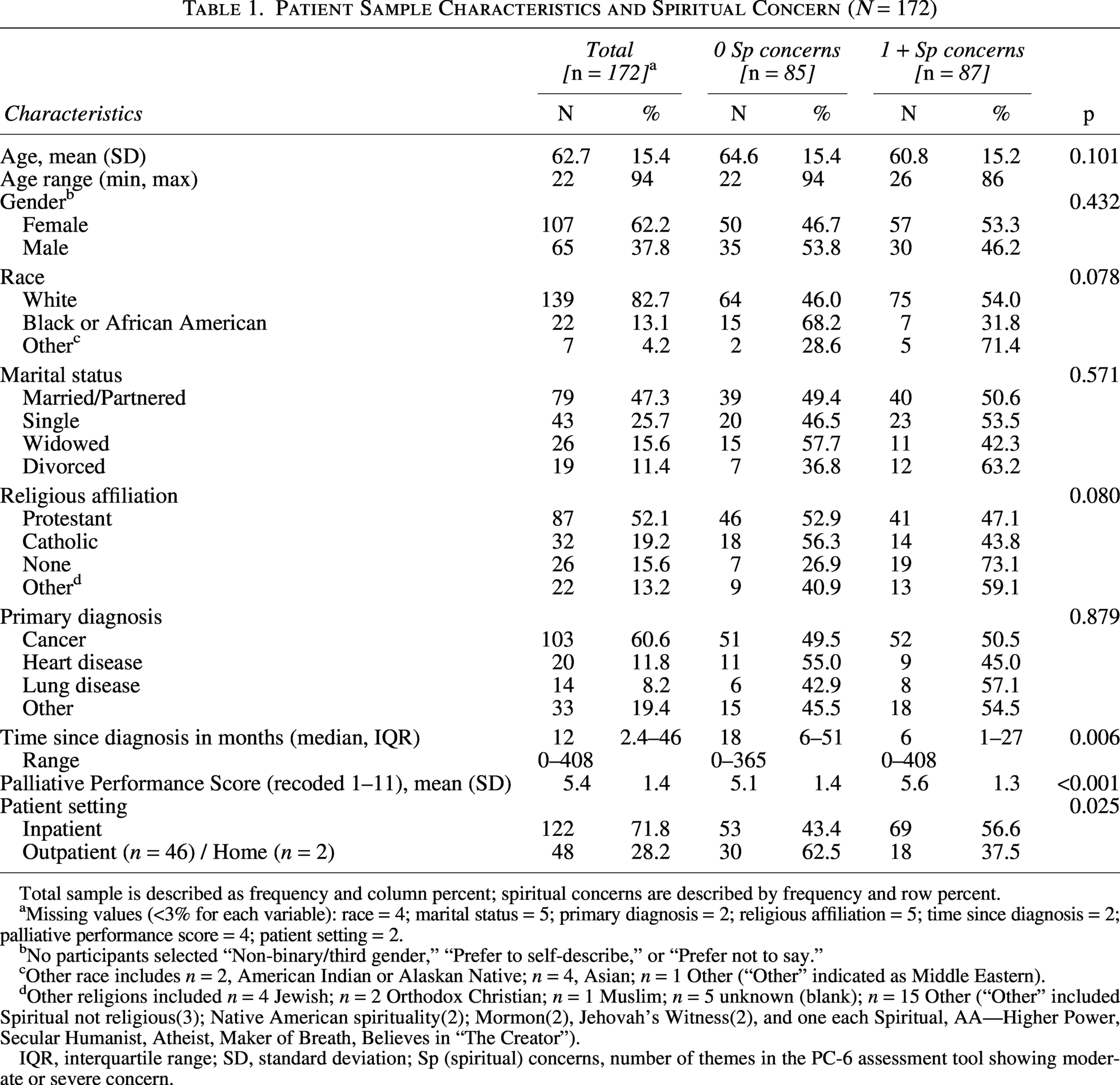
Total sample is described as frequency and column percent; spiritual concerns are described by frequency and row percent.
Missing values (<3% for each variable): race = 4; marital status = 5; primary diagnosis = 2; religious affiliation = 5; time since diagnosis = 2; palliative performance score = 4; patient setting = 2.
No participants selected “Non-binary/third gender,” “Prefer to self-describe,” or “Prefer not to say.”
Other race includes n = 2, American Indian or Alaskan Native; n = 4, Asian; n = 1 Other (“Other” indicated as Middle Eastern).
Other religions included n = 4 Jewish; n = 2 Orthodox Christian; n = 1 Muslim; n = 5 unknown (blank); n = 15 Other (“Other” included Spiritual not religious(3); Native American spirituality(2); Mormon(2), Jehovah’s Witness(2), and one each Spiritual, AA—Higher Power, Secular Humanist, Atheist, Maker of Breath, Believes in “The Creator”).
IQR, interquartile range; SD, standard deviation; Sp (spiritual) concerns, number of themes in the PC-6 assessment tool showing moderate or severe concern.
Fifty percent of patients were assessed to have moderate or severe concerns in at least one of six spiritual domains, and 17% were assessed to have such concerns in two or more domains [Table 2]. Moderate or severe concerns were most common in relationships (19.2%), dying (14.5%), meaning (14.0%), and legacy (11.0%), with lower rates of R/S struggle (9.9%) and treatment-related concerns (4.7%) [Table 3].
Prevalence of Spiritual Concerns in Palliative Care Patients Using PC-6 (N = 172)
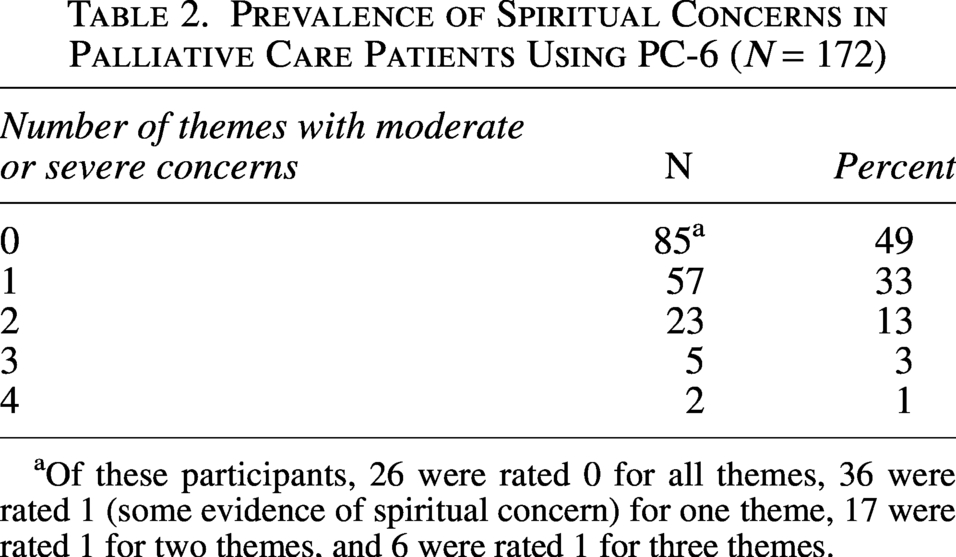
Of these participants, 26 were rated 0 for all themes, 36 were rated 1 (some evidence of spiritual concern) for one theme, 17 were rated 1 for two themes, and 6 were rated 1 for three themes.
Distribution of Moderate or Severe Spiritual Concerns by Religious Affiliation a
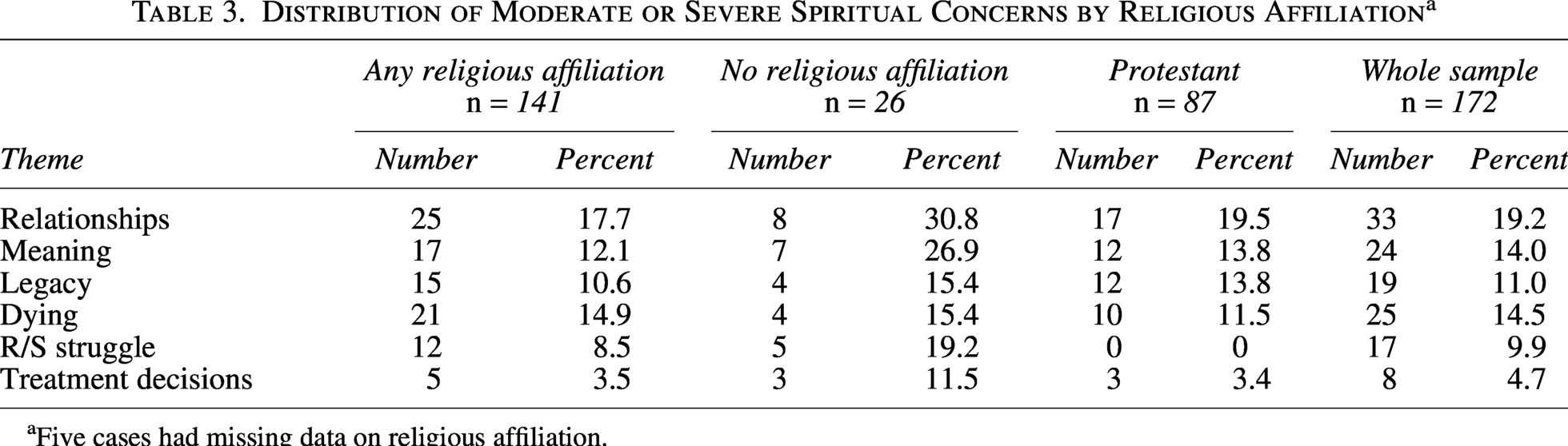
Five cases had missing data on religious affiliation.
In our bivariate analysis, none of the demographic characteristics had a statistically significant association with having no spiritual concerns (PC-6 score = 0) versus any spiritual concerns (PC-6 score ≥ 1), nor did religious affiliation. Among the medical factors, primary diagnosis was not associated with having any spiritual concerns. The statistically significant bivariate indicators of none versus any spiritual concerns were the patient’s setting, the time since diagnosis, and the PPS score. In terms of setting, inpatients were more likely to have any spiritual concerns compared to outpatients (p = 0.025). Where chaplains found 1 or more spiritual concerns, the average time since diagnosis was 6 months, compared to 18 months among patients for whom chaplains found no evidence of spiritual concern (p = 0.006). Patients assessed to have spiritual concerns had slightly higher Palliative Performance Scores (p = < 0.001) [Table 1].
Consistent with the bivariate analysis, in the multivariable logistic regression analysis there was no association between any of the demographic factors and none versus any spiritual concerns. In contrast to the bivariate analysis, there were statistically significant associations between religious affiliation and the presence of spiritual concerns. Compared to those with a Protestant affiliation, patients with no religious affiliation were three and a half times more likely to have any spiritual concerns (p = 0.023). In the multivariable analysis, there were no statistically significant associations between spiritual concerns and patient setting, time since diagnosis, or PPS score, although the result for PPS score approached significance with a p value of 0.058 [Table 4].
Logistic Regression Predicting PC-6 Score Using Demographic, Religious, and Clinical Variables
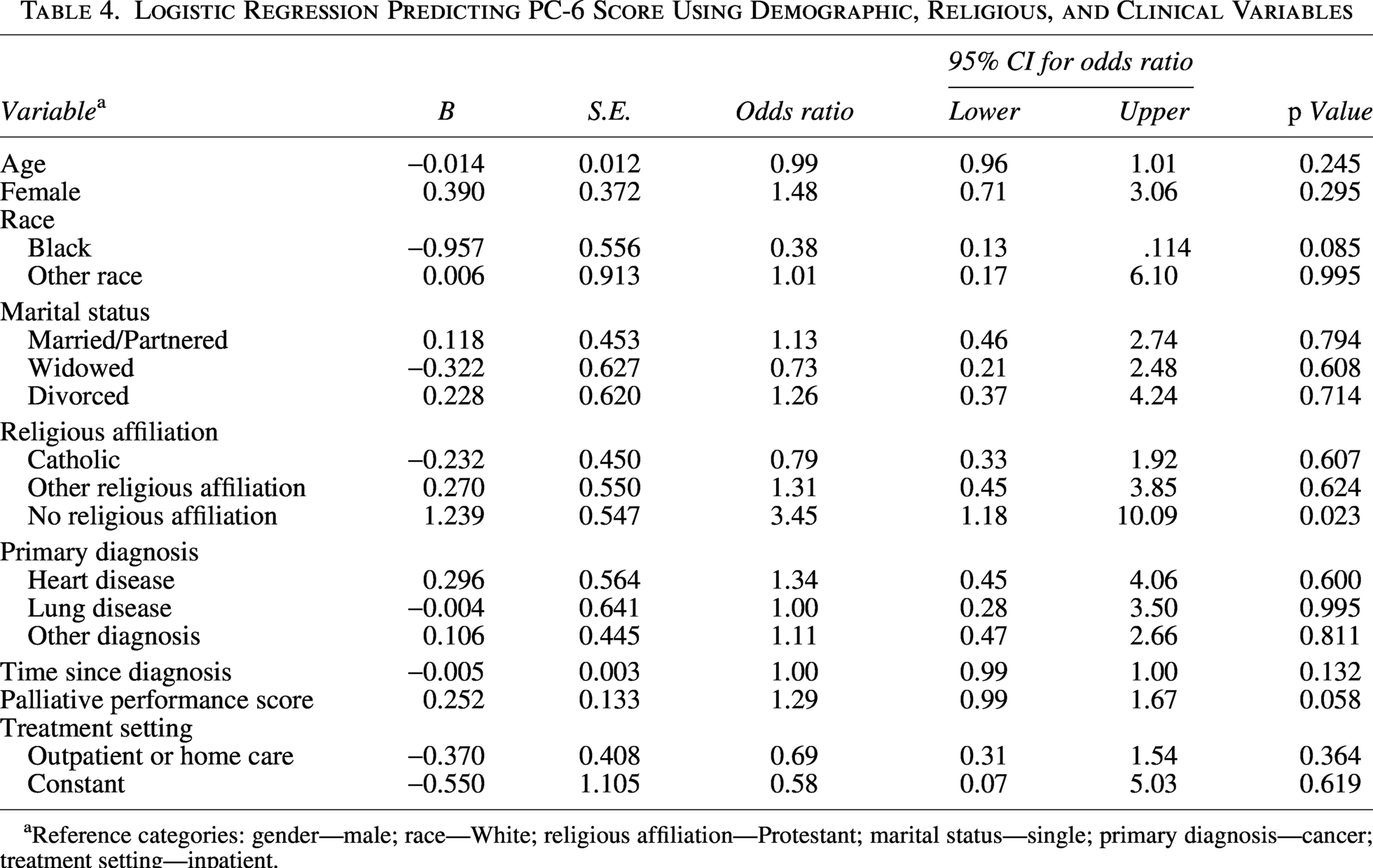
Reference categories: gender—male; race—White; religious affiliation—Protestant; marital status—single; primary diagnosis—cancer; treatment setting—inpatient.
In light of the significant results for participants with no religious affiliation in the logistic regression model, we examined the level of concerns for each of the themes in the PC-6 for those with and without religious affiliations. Participants without a religious affiliation had higher proportions of moderate or severe spiritual concerns across all six PC-6 domains. These differences were most pronounced for concerns related to meaning, R/S struggle, treatment decision-making, and relationships [Table 3].
Discussion
In this multisite cohort, three key findings emerged: (1) spiritual concerns were common, with half of patients reporting at least one moderate or severe concern; (2) these concerns were not associated with demographic or clinical characteristics, indicating that risk cannot be identified in advance and underscoring the need for universal screening; and (3) patients with no religious affiliation had higher odds of concerns across multiple spiritual distress domains.
These prevalence estimates are consistent with prior studies reporting rates of spiritual distress among palliative care patients. The findings from this study closely mirror those of Hui and colleagues who also found spiritual distress in 44% of the palliative care patients in their study. 20 Our results also align with a study of veterans with serious illness in which 55.8% scored in the medium or high range on the Spiritual Needs subscale of the I-SPIRIT. 8
In our multivariable model, compared to those with a Protestant religious affiliation, those who reported no religious affiliation had a threefold greater risk of having moderate or severe spiritual concerns. Notably, as shown in Table 3, the pattern of higher rates of moderate or severe spiritual concerns among patients with no religious affiliation persisted when compared both with Protestants alone and with all patients reporting any religious affiliation. Specifically, patients with no affiliation had a greater proportion of moderate or severe spiritual concerns in the domain of relationships, and at least twice the proportion of moderate or severe concerns related to meaning, R/S struggle, and treatment decisions. Prior research has reported mixed findings regarding the association between religious affiliation and R/S distress. Delgado-Guay and colleagues reported similar levels of spiritual pain in patients with lower self-reported religiosity. 7 In contrast, Damen and colleagues, also using multivariable models, found no association between total RSS scores and religious affiliation. 13
Among the largest religious subgroup—patients with a Protestant affiliation—R/S struggle was assessed to be minimal, even though moderate or severe concerns related to relationships, meaning, and dying were each reported in more than one in 10 patients [Table 3]. This suggests that for Protestant patients in this sample, spiritual distress manifested primarily through relational and existential concerns rather than through doctrinal or faith-based struggle. This finding may reflect the value of a multi-dimensional spiritual assessment, as a tool focused narrowly on religious or doctrinal struggle could underestimate the spiritual care needs of religiously affiliated patients whose distress is expressed relationally or existentially rather than theologically.
Importantly, the higher burden of concerns among study patients with no religious affiliation may challenge the assumption that spiritual distress is concentrated only among those with religious identities. These findings suggest that patients without a religious framework may have fewer established resources for meaning-making and coping, placing them at increased risk for multidimensional concerns. Clinically, this underscores the need for screening and assessment of spiritual concerns among all patients. These findings highlight the importance of team collaboration to ensure that spiritual concerns—particularly among patients who do not self-identify as religious—are recognized and addressed.
It should be noted that of the 85 patients in our study who were assessed not to have moderate or severe spiritual concerns, 59 (34% of the total sample) were identified as having some concern in at least one of the six domains assessed. The lower prevalence of spiritual concerns observed here is consistent with prior findings, including 44% of veterans reporting some level of spiritual needs 8 and 22% reporting mild distress using a single-item measure of spiritual pain. 16
Our study also examined the prevalence of moderate or severe concerns for each of the six PC-6 domains. Moderate or severe concerns about relationships were the most common (19%). This includes the need to attend to unfinished business in relationships or perceiving oneself as a burden to loved ones. Chaplains identified moderate or severe concerns about dying in 14.5% of study patients. This includes feeling unready for death, experiencing struggle between holding on and letting go, fearing pain, or worrying about what happens after death. Other models for measurement of R/S distress do not explicitly address concerns about dying, although subscales of the QUAL-E capture similar concerns. 27 Chaplains also assessed 14% of the patients to have moderate or severe concerns about meaning. These concerns include coming to terms with how illness has changed one’s identity.
We also examined several factors that might be associated with spiritual concerns. We found no associations for four demographic factors: age, gender, race, or marital status. This is consistent with some other research.13–14 In contrast, several studies have reported higher levels of R/S distress in younger patients, 15 including studies that used multivariable analysis. 20 Beyond primary diagnosis, our study included three other measures related to health status: time since diagnosis, PPS score, and setting (inpatient vs. outpatient or home care). Each of these three measures demonstrated significant bivariate associations with having moderate/severe spiritual concerns, but none of these associations retained significance in the multivariable model. Taken together, these findings suggest that spiritual distress is not confined to demographic or clinical subgroups, supporting the use of routine spiritual screening approaches in clinical care.
Our study findings should be interpreted in light of its limitations. Although the study drew on multiple sites, the sample was predominantly white and Christian. A more comprehensive examination of R/S concerns across key racial/ethnic and religious subgroups will require a more diverse sample. The cross-sectional design of the study allowed us to examine correlates of spiritual concern; a longitudinal study is needed to examine predictors of spiritual concerns and their trajectory. Future research should address these limitations and evaluate how use of the PC-6 informs spiritual care for palliative care patients, along with the trajectory of spiritual distress among those who receive such care.
These findings, using a validated chaplain-administered assessment, extend prior evidence that a substantial proportion of PC patients experience moderate or high levels of spiritual concerns that may compromise well-being and coping.7,8,13,14,20 These findings support the recommendations of a recent systematic review to “routinely incorporate spiritual care into the medical care of patients with serious illness,” and to “include specialty practitioners of spiritual care (e.g., chaplains) in the care of patients with serious illness.” 1 Routine screening for R/S distress should serve as a central component of this care, along with timely referral for a chaplain assessment using the PC-6 or other validated models when indicated.25,28–30 Addressing suffering in all its dimensions—physical, psychological, social, and spiritual—remains a core component of high-quality palliative care.
Authors’ Contributions
Study concept and design: G.F. and D.L.; Subject recruitment and enrollment: B.C., I.C., S.B.D., M.L.H., S.B.-M., E.P., and K.A.U.; Analysis and interpretation: P.K.P., S.B.-M., D.L., and G.F.; Article preparation: S.B.-M., P.K.P., D.L., and G.F. All the authors have reviewed and approved this article.
Ethical Considerations
The study was approved by the IRBs of Rush University Medical Center (IRB#20010203), Essentia Health (IRB#EH20671), Northwestern University (IRB#STU00214802), the University of Illinois College of Medicine at Peoria (IRB#00000688 and #00000689), Massachusetts General Hospital (IRB#2020P002899), and Vanderbilt University Medical Center (IRB# #201044).
Footnotes
Acknowledgments
The authors express their gratitude for the patients who participated in the study. They thank Abraham Labrada-Santiago, Sara Paasche-Orlow and Jeanne Wirpsa for their valuable contributions. They are grateful for the consultation on analysis of missing data provided by the Rush University Biostatistics Core. They would also like to thank all the research assistants and chaplains who contributed to and/or participated in this study.
Consent to Participate
Written informed consent was provided by participants recruited at Essentia Health, Northwestern Memorial Hospital, and OSF Healthcare. At Massachusetts General Hospital and Vanderbilt University Medical Center, all study data came from usual care and those IRBs determined informed consent was not required.
Data Availability
The study data are available from the corresponding author upon reasonable request.
Author Disclosure Statement
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The study was supported by a research grant from the College of Health Sciences, Rush University Medical Center. Work by Essentia Health team members was supported in part by grant A2003 from the Essentia Health Foundation.