
Abstract
Background/significance:
High rates of HIV infection and other sexually transmitted infections (STIs) related to high-risk sexual behaviors are a public health problem in the United States. Hispanics have the second highest rates of HIV infection among racial/ethnic minorities. Previous research with Hispanic men has identified a number of factors that influence sexual risk and render Hispanic men at risk for HIV/STIs that vary by sexual orientation. Despite these differences in sexual risk by sexual orientation, no study to date has compared the sexual behaviors of Hispanic men by sexual orientation.
Objective:
The purpose of this study was to compare the sexual behaviors of a sample of Hispanic men residing along the US-Mexico border by sexual orientation.
Method:
A descriptive, cross-sectional design was used to collect data from 103 Hispanic men in a US-Mexico border community. The sample included fifty heterosexual men and fifty-three men who have sex with men (MSM). Participants completed two measures of sexual health/sexual behaviors and a demographic questionnaire.
Results:
Among this sample of Hispanic men, fewer heterosexual men were tested for HIV infection compared to MSM, more MSM reported HIV infection, MSM had higher rates of certain STIs, and MSM reported more sexual partners. MSM were more likely to experience sexual violence. Heterosexual Hispanic men reported lower rates of condom usage when compared to Hispanic MSM.
Implications:
Hispanic men as a population may engage in high-risk sexual behaviors that place them at risk for HIV/STIs. More research focused on Hispanic men residing along the US-Mexico border can provide the foundation for intervention studies to help this population of men decrease their risk for HIV/STIs.
The high rates of new cases of HIV infection and other sexually transmitted infections (STIs) present a public health concern for the United States. Over nineteen million STIs including 56,000 cases of HIV infection are diagnosed each year in the United States. It is estimated that STIs cost the health-care system nearly US$16 billion dollars annually (USDHHS [US Department of Health and Human Services] 2013). These preventable infections in the United States are largely related to high-risk sexual behaviors (HIV/AIDS among Hispanics/Latinos 2014). High-risk sexual behaviors are those behaviors such as sexual activity without condoms, sex under the influence of drugs and/or alcohol, sex with multiple partners, and sex with persons whose HIV status is unknown. In order to reduce the risk of HIV/STIs, avoidance of high-risk sexual behaviors and engagement in safer sexual behaviors is recommended (HIV/AIDS among Hispanics/Latinos 2014).
Hispanic men are one vulnerable population in the United States that continues to experience health disparities in terms of HIV/STI rates. After blacks, Hispanics have the highest rates of new cases of HIV infection among racial/ethnic minorities. Although a small percentage of these cases are related to intravenous drug use, the major risk factor is sexual transmission, especially male-to-male sexual contact. In addition to HIV infection, Hispanic men have higher rates of all other STIs when compared to Caucasian men (Scott et al. 2010).
Some researchers have documented that the general population of Hispanic men engage in high-risk sexual behaviors more frequently than any other racial/ethnic group with the exception of black men. In fact, compared to Caucasian men, the general population of Hispanic men were more likely to engage in high-risk sexual behaviors and to maintain sexual risk behaviors over time (Dariotis et al. 2011). Some evidence is available that also suggested that Hispanic men who have sex with men (MSM) engage in high-risk sexual behaviors (De Santis et al. 2011; Xia et al. 2006).
Sexual Behaviors of Heterosexual Hispanic Men
Some researchers have documented participation in high-risk sexual behaviors among heterosexual Hispanic men. A large study of 591 unmarried Hispanic men reported that high-risk sex occurred when condoms were not available, when conversations between partners about condom use did not occur, and when men were involved in a consistent, monogamous relationship (Ibanez et al. 2005). Another study reported negative attitudes about condoms and decreased decision-making about condom use among partners resulted in high-risk sex among Hispanic men (Harvey and Henderson 2006). Another study of immigrant Hispanic men found that immigration to the United States resulted in sexual risk behaviors such as sex with commercial sex workers, sex under the influence of drugs and alcohol, and occasional sex with men (Sanchez et al. 2012). At highest risk were younger men and those who had immigrated within the previous five years (Sanchez et al. 2012). These three studies provide some evidence that heterosexual Hispanic men engage in high-risk sexual behaviors that place them at risk for HIV/STIs.
Hispanic MSM
Compared to what is known about high-risk sexual behaviors among heterosexual Hispanic men, more studies have focused on the high-risk sexual behaviors of Hispanic MSM. Sexual risk factors among Hispanic MSM are slightly different than those for heterosexual Hispanic men. High-risk sex for Hispanic MSM includes failure to negotiate safer sex with partners and contact with the partner’s bodily fluids (De Santis 2012). A number of studies (De Santis 2012; Fernandez et al. 2009; Jarama et al. 2005) have noted that a significant source of risk is sex with multiple partners that involves unprotected anal intercourse, the most risky sexual behavior. An additional risk factor for high-risk sex among Hispanic MSM is substance use before or during sex (De Santis 2012; Fernandez et al. 2009; Jarama et al. 2005). Some evidence also suggests that cultural factors such as machismo and stigma may also influence high-risk sex among Hispanic MSM (Jarama et al. 2005).
Comparing Sexual Behaviors of Hispanic Men by Sexual Orientation
Only three studies could be located that compared the sexual behaviors of Hispanic men by sexual orientation. A large study of 680 Hispanic men in California (628 heterosexuals and fifty-two MSM) found that Hispanic men that engaged in sex with both men and women were more likely to engage in unprotected sex, have a history of an STI, and report sex under the influence of alcohol and drugs (Zellner et al. 2009). A second study conducted in Puerto Rico found that MSM were more likely than heterosexual men to have a sexual debut before the age of fifteen years, were more likely to have ten or more lifetime sexual partners, were more likely to use drugs and alcohol during sex, and were thirteen times more likely to be HIV infected (Colon-Lopez et al. 2013). A study conducted in Miami, Florida, that enrolled near equal numbers (n = 163; eighty heterosexual men and eighty-three MSM) of heterosexual Hispanic men and Hispanic MSM reported few differences in sexual behaviors when compared by orientation. No differences were found in terms of sexual behaviors, HIV testing history, and substance use during sex when the men were compared by sexual orientation. Differences were found in terms of STI rates, as MSM were more likely to have a lifetime history of any STI except for Hepatitis C when compared to heterosexual men (De Santis et al. 2014).
Researchers have documented that Hispanic men engage in high-risk sexual behaviors and are therefore at risk for HIV infection and other STIs. Because a limited number of studies have been conducted which compared sexual risk behaviors by sexual orientation among Hispanic men, it is not possible to know with confidence at this point if sexual risk behaviors of Hispanic men vary by sexual orientation. In addition, no studies to date have been conducted that examined sexual risk behaviors of Hispanic men by sexual orientation among Hispanic men residing along the US-Mexico border. Accordingly, the purpose of this cross-sectional study was to compare selected health determinants and sexual health indicators among a sample of Mexican–American men in a large binational community in the Texas–Mexico border region.
Methods
Participants and Procedures
The project was approved by the University of Texas at El Paso Institutional Review Board. Participants (n = 103) were recruited from a variety of clinical and community settings, most of which provide services for people living with HIV/AIDS (Mata et al. 2014). This study was part of a larger study that examined relationships between intimate partner violence, HIV risk, and substance use among Hispanic men in the US-Mexico border region.
Data Collection
Participants provided written informed consent and were interviewed by trained graduate student research assistants. The bilingual and bicultural research assistants both had prior nursing and public health research experience and are focusing their graduate research in HIV-related disparities among Hispanics in the US-Mexico border region. In addition, the research assistants both had substantial health promotion education experience and strong relationships with community partners. The structured interviews were conducted in person in Spanish or English, as participants preferred. Data reported here reflect sexual health indicators and sexual debut in addition to sociodemographic characteristics and selected health determinants.
Measures
Condom use, HIV/STI history, sex outside a primary relationship, sexual debut, and history of forced sex were assessed through selected questions from the sexual health history and the partner table (Peragallo et al. 2005). Both of these instruments have been widely used with Hispanic populations in the past decade to assess sexual health, relationship history, and sexual behavior (Peragallo et al. 2005; González-Guarda et al. 2011; Peragallo et al. 2012).
Analyses
Descriptive and inferential analyses were conducted with Statistical Package for the Social Sciences Version 20. Descriptive participant characteristics and health determinant data are reported separately for heterosexual (n = 50) and gay and bisexual men (n = 53). t-Tests for independent groups and χ2 tests of independence were conducted to compare sexual health history and sexual behaviors by sexual orientation.
Results
Participant Characteristics and Selected Health Determinants
As shown in Table 1, 103 men (fifty heterosexual and fifty-three MSM) participated in the study. Almost half of the heterosexual men were married or in a relationship, as were 23 percent of the MSM. On average, participants had at least a high school education. Thirty-six percent of heterosexual men and 53 percent of MSM had less than US$999 of monthly income. To provide a more accurate picture of available income, we also report a ratio of the income range (one being less than US$999 ranging through five being more than US$4,000) which is the income category (USDHHS 2013; HIV/AIDS among Hispanics/Latinos 2014; Scott et al. 2010; Dariotis et al. 2011; De Santis et al. 2011) divided by the number of people supported by that income. Of note, 70 percent of participants had no health insurance. Fourteen percent of heterosexual men and 60 percent of MSM reported HIV infection; this is not surprising, given that many participants were recruited from clinics or agencies providing services to people with HIV or through their social networks.
Participant Characteristics of the Sample (N = 103) by Sexual Orientation.
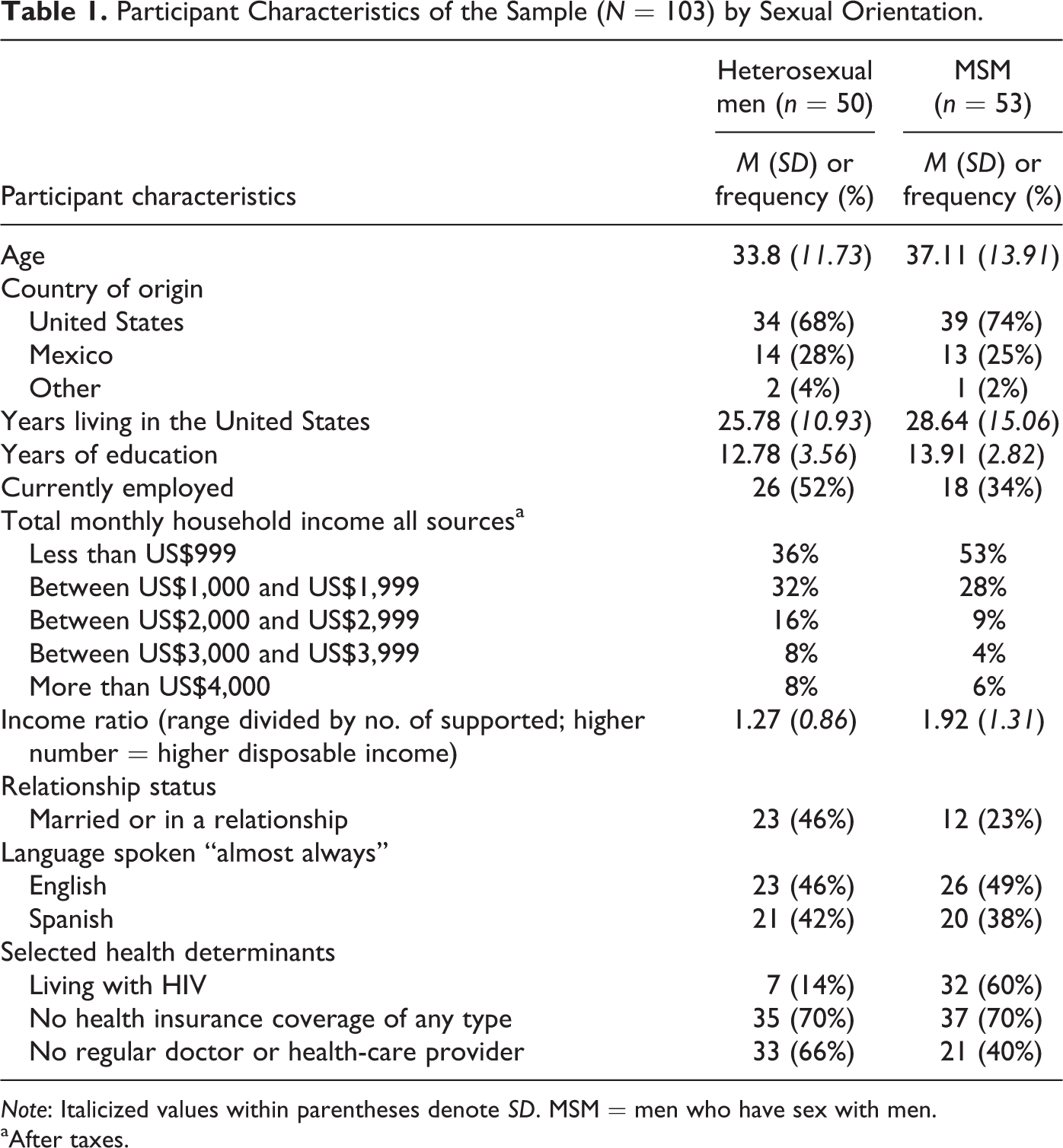
Note: Italicized values within parentheses denote SD. MSM = men who have sex with men.
aAfter taxes.
Sexual Health History and Sexual Behavior
HIV/STI’s
Table 2 contains detailed comparisons between heterosexual men and MSM. As shown, heterosexual men were less likely than MSM to report that they had ever been tested for HIV or other STI (70 percent and 98 percent, respectively). This difference was statistically significant, χ2 (1) = 15.51, p < .001. In this sample, 14 percent of the heterosexual men compared with 60 percent of the MSM reported HIV infection, and this was also statistically significant, χ2 (1) = 23.52, p < .001. MSM were more likely to have been told they have gonorrhea, χ2 (1) = 9.30, p = .003, or chlamydia/urethritis, χ2 (1) = 10.45, p < .001. Participants were also asked if they had ever been told they have pubic lice, hepatitis A, or trichomonas; however, because only one participant said yes to lice and none of the men reported the latter two, no comparisons are reported.
Sexual Health Indicators and Behaviors.
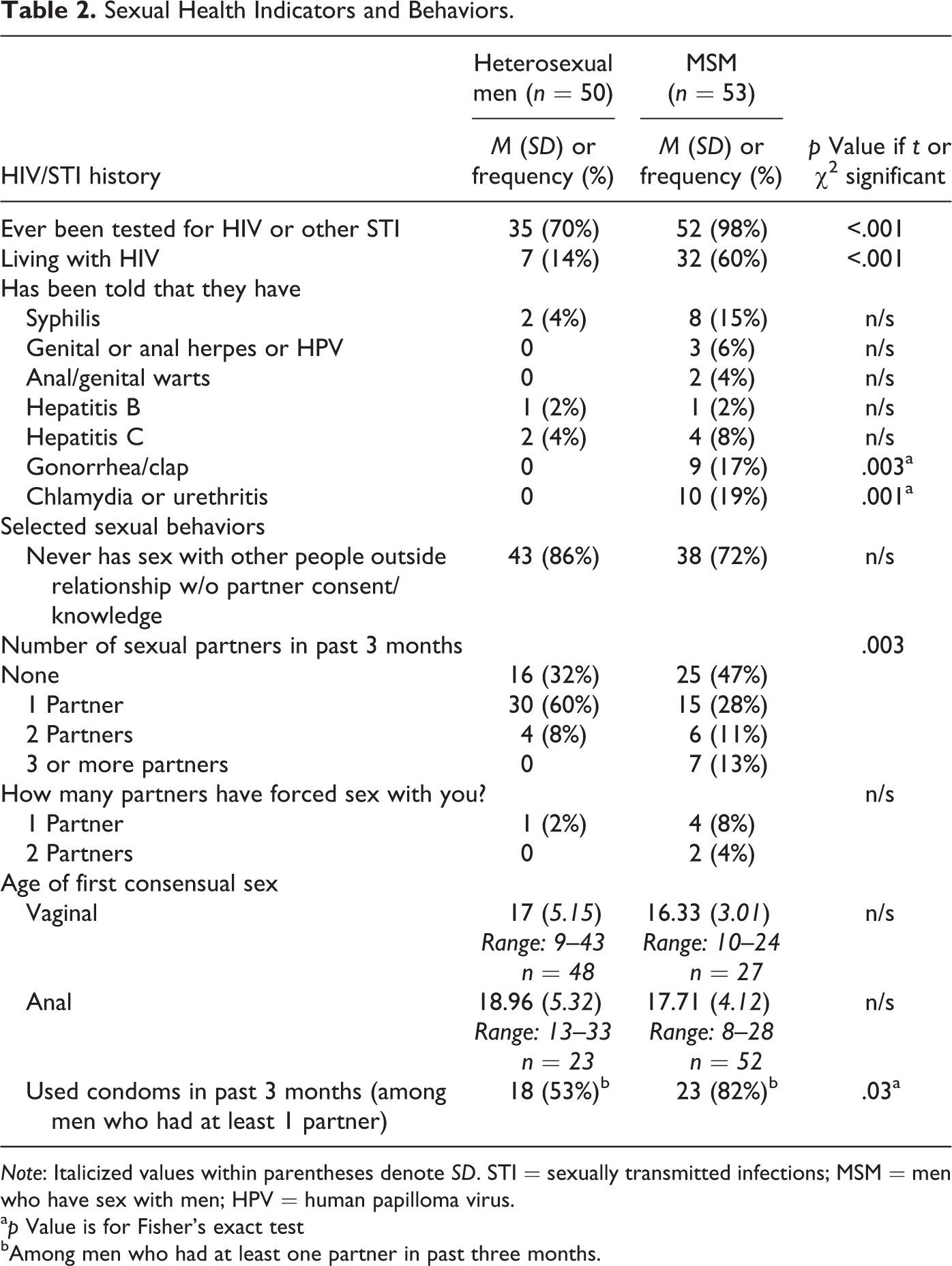
Note: Italicized values within parentheses denote SD. STI = sexually transmitted infections; MSM = men who have sex with men; HPV = human papilloma virus.
a p Value is for Fisher’s exact test
bAmong men who had at least one partner in past three months.
Selected sexual behaviors
As shown in Table 2, 86 percent of heterosexual men and 72 percent of MSM never have sex with other people outside relationship w/o partner consent/knowledge. This was not a statistically significant difference. Regarding number of partners in the past three months, MSM were more likely to report “no partners” (47 percent vs. 32 percent) and were also more likely to report “2” or “3 or more partners.” Heterosexual men were more likely to report having one partner (60 percent vs. 28 percent), χ2 (3) = 14.30, p = .003. A total of seven (14 percent) men reported that at least one partner had forced sex with them; this did not differ by sexual orientation. Forty-eight (96 percent) of the heterosexual men and twenty-seven (50.9 percent) of MSM reported having vaginal sex, while twenty-three (46 percent) of heterosexual men and fifty-two (98 percent) of MSM reported having anal sex. The age of first consensual sex did not differ significantly by sexual orientation for either vaginal or anal sex. Finally, out of the thirty-four (68 percent) of heterosexual men and twenty-eight (53 percent) of MSM who reported having at least one partner in the past three months, MSM were much more likely to report using condoms in the past three months (82 percent vs. 53 percent), χ2 (1) = 5.85, p = .03.
Discussion
The purpose of this study was to compare selected health determinants and sexual health indicators by sexual orientation among a sample of Mexican–American men residing in a large community along the Texas–Mexico border. This study adds some new findings to the established but small knowledge base on this topic.
In terms of HIV/STI testing, more MSM participants reported being tested for HIV infection and other STIs when compared to heterosexual men. These findings are supported by the research conducted by Fernandez and colleagues (2002). In a large study that enrolled over 1,000 Hispanic men, MSM were about five times more likely to be tested for HIV infection and other STIs when compared to heterosexual men (Zellner et al. 2009). Because MSM are more at risk for HIV infection (HIV/AIDS among Hispanics/Latinos 2014), it makes sense that more MSM would be tested for HIV infection when compared to heterosexual men.
More MSM participants were diagnosed with HIV infection when compared to the heterosexual men. This finding is not surprising because the results mirror the epidemiology of HIV infection. More MSM than heterosexual men have been diagnosed with HIV infection since the emergence of HIV infection in 1981 (HIV/AIDS among Hispanics/Latinos 2014).
Because more MSM reported a diagnosis of HIV infection, it could be assumed that MSM would also have higher rates of other STIs. This is related to the fact that both HIV infection and STIs are a result of high-risk sexual behaviors (HIV/AIDS among Hispanics/Latinos 2014). However, in this study, the only statistically significant differences between the two groups of men were found in terms of gonorrhea and chlamydia/urethritis. This result is probably due to the fact that these two STIs are among the most commonly diagnosed (HIV/AIDS among Hispanics/Latinos 2014). These differences among STI rates by sexual orientation support previous research (Zellner et al. 2009; De Santis et al. 2014) noting that certain STIs are more likely among MSM when compared to heterosexual men.
Participants were asked about sex outside of their primary relationships. More MSM reported sex outside of the primary relationship when compared to heterosexual men (28 percent vs. 14 percent), but these results were not statistically significant. The fact that nearly one-third of the MSM participants in this study had sex outside of the primary relationship is supported in the literature (Beougher, Gomez, and Hoff 2011). However, no studies could be located to support or refute the findings related to heterosexual men.
MSM participants had more sexual partners when compared to heterosexual participants. The higher rates of HIV infection among the MSM participants have been supported by previous research (Colon-Lopez et al. 2013). These findings are not surprising because more MSM in this sample reported being HIV infected and being diagnosed with more STIs than did heterosexual men. Higher numbers of sexual partners within the context of unprotected sex places these men at risk for both HIV infection and STIs (HIV/AIDS among Hispanics/Latinos 2014; CDC 2010).
Forced sex with sexual partners during adulthood was not a common finding among the participants in this sample. Six MSM reported forced sex as compared to one heterosexual man, but the numbers were too small to be statistically significant. Some literature is available that notes that Hispanic MSM may experience sexual violence within their primary relationships (De Santis 2012). The six MSM participants (12 percent) that reported sexual violence is evidence that suggests this may be an issue among Hispanic MSM in the US-Mexico border region.
No differences were found among the two groups of Hispanic men in terms of sexual debut. This finding is supported by the previous work of De Santis and colleagues (2014) that also reported that no differences were found between the two groups of men in terms of sexual debut. However, this finding is not supported by the work of Colon-Lopez and colleagues (2013) who noted that MSM were more likely to have an earlier sexual debut than heterosexual Puerto Rican men. More research in this area with a larger sample of Mexican–American men is needed.
Condom use varied between the two groups of Hispanic men in this sample. MSM were more likely to use condoms compared to heterosexual men. There are at least two possible explanations for the differences in condom use by sexual orientation found in this study. First, because MSM were more likely to have more sexual partners, perhaps MSM used condoms more because of the number of different sexual partners. Second, because more MSM were HIV infected and reported more STIs, MSM may be more likely to use condoms in an effort not to transmit HIV or other STIs to their sexual partners.
Implications for Practice
The results of this study have implications for clinicians providing care for Hispanic men. Clinicians need to encourage HIV testing among Hispanic men, especially heterosexual Hispanic men. Based on the findings of this study, heterosexual Hispanic men may not be routinely advised to accept HIV testing when offered. Despite recommendations by the CDC (Branson et al. 2006) that encourage annual HIV testing of all adults aged thirteen to sixty-four, some clinicians may not offer HIV testing to clients they deem as not “high risk.” In addition, heterosexual Hispanic men may not perceive themselves as at risk for HIV infection and may decline testing even when offered. Clinicians should be aware of the high rates of HIV infection among Hispanic men and encourage HIV testing among all adults based on the guidelines (Branson et al. 2006).
In addition to HIV testing, clinicians should encourage STI testing among Hispanic men, and especially MSM, who engage in high-risk sexual behaviors. Health-care providers should be aware that STI testing should be offered to any client who reports high-risk sexual behaviors. This is important because a diagnosis of any STI increases the risk of transmission of HIV infection by three to five times (CDC 2010).
Health-care providers and clinicians must be comfortable performing an accurate sexual history, including an assessment of sexual orientation. This is important because many Hispanic men may not identify as gay or bisexual or may not be willing to disclose their sexual orientation for fear of judgment or discrimination (Bernstein et al. 2008). A direct, nonjudgmental approach to issues surrounding sexual orientation may make these clients more comfortable in disclosing their sexual orientation. Disclosure will allow a more in-depth risk assessment, appropriate testing, and prevention education (Bernstein et al. 2008).
For self-identified gay and bisexual men, it is important for clinicians to assess these men for any form of relationship violence. Relationship violence includes physical, psychological, and sexual violence. It is important to screen for relationship violence and to appreciate its association with HIV/STI risk among Hispanic MSM (De Santis et al. 2012).
Lastly, clinicians should have frank discussions with all Hispanic men regarding safer sex behaviors and reinforcement of the need to use condoms to reduce sexual risk. Previous research (Harvey and Henderson 2006; Sanchez et al. 2012; Jones et al. 2015; Jones et al. 2013) reported that condom usage is low among all Hispanic men. This could be related to the fact that discussions of the importance of condom use to decrease HIV/STIs are often not incorporated into primary care (Bernstein et al. 2008). Primary care encounters may be the only opportunity for these men to receive reinforcement of safer sex messages. If this information is not provided during the health-care encounter, a perfect opportunity for primary prevention is lost.
Limitations
Several limitations of this study should be noted. The first limitation is the relatively small sample size (n = 103). The small sample size limits the ability to generalize the findings; however, because this study is a pilot study that gathered exploratory data on a population that has not been studied previously in this particular area of the United States, these findings provide some new information on the sexual behaviors of these two groups of Hispanic men. Second, the sexual health history and the partner table (Peragallo et al. 2005) lack reported reliability and validity. However, both instruments have been used successfully to collect data on the sexual behaviors of Hispanic men and women (De Santis et al. 2014; Peragallo et al. 2005; González-Guarda et al. 2011; Peragallo et al. 2012), and the results of this study are comparable to data collected using these two instruments in a different region in the United States with a different Hispanic population (De Santis et al. 2014). Overall, this study has provided some new information on sexual risk behaviors among Hispanic men residing along the US-Mexico border, a population of Hispanic men that require further study in terms of sexual risk behaviors.
Conclusion
As a population, Hispanic men are at risk for HIV/STIs related to high-risk sexual behaviors. Compared to other groups of men, little is known about Hispanic men, and even less is known about Hispanic men residing along the US-Mexico border. Continued work is needed with this population to develop interventions to address high-risk sexual behaviors among both groups of Hispanic men.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute on Minority Health and Health Disparities of the National Institutes of Health under Award Number P20MD002287. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.