
Abstract
Capturing context in public health evaluation remains challenging despite its recognized importance. The contextual factors framework (CFF) offers potential support for this process, but real-world applications are limited. This study applied the CFF to conduct contextual assessment of a rural Australian health promotion grant program and explore its utility in this setting. An exploratory qualitative approach involved an in-depth contextual assessment guided by the CFF, drawing on stakeholder interviews and program documents, followed by a focus group with program staff to refine findings and discuss framework utility. The assessment identified contextual barriers (e.g., infrastructure limitations), facilitators (e.g., community volunteering culture), and improvement opportunities (e.g., enhanced program documentation). Staff reported that the CFF supported communication and planning but did not fully capture dynamic contextual interrelationships. These findings position the CFF as a structured and practical entry point for contextual assessment, while suggesting that complementary approaches may be useful for capturing evolving interconnections and power dynamics in rural health promotion settings.
Keywords
Introduction
Intervention context is increasingly recognized as central in public health evaluation, with meaningful assessment beginning with consideration of the broader context in which interventions are delivered (BetterEvaluation, 2025; Kidder et al., 2024; Renger, 2022; Renger et al., 2015; Rog, 2012; Shoveller et al., 2015; Skivington et al., 2021; World Health Organization Europe, 2001). Early on, Rogers’ (2009) emphasized the need for evaluation designs that are tailored to the specific characteristics of interventions and their operating environments, describing this as a “situational responsiveness” approach to evaluation. Rog (2012) further argued that context should feature in the foreground of evaluation practice, asserting that robust contextual analysis could lead to more actionable and generalizable evaluation findings and provide explanatory power for understanding how and why interventions succeed or fail. Shoveller et al. (2015) extended this argument by proposing a paradigm shift toward viewing interventions through the lens of “intervention = intervention × context,” suggesting that the effectiveness of public health initiatives cannot be understood separately from the sociocultural environments in which they operate. More recently, evaluation guidance published by the U.K. Medical Research Council (Skivington et al., 2021) and the updated CDC Program Evaluation Framework (Kidder et al., 2024) reinforce context as a core element of public health and complex intervention evaluation. Additionally, international evaluation groups such as the Global Evaluation Initiative emphasize the influence of contextual factors such as geographic, socioeconomic, and political circumstances on intervention outcomes and the importance of incorporating contextual assessment across multiple stages of the evaluation process (BetterEvaluation, 2025; Global Evaluation Initiative, n.d.). These perspectives reflect a growing consensus that context is not a peripheral concern, but rather a central focus for producing meaningful, applicable evidence in public health evaluation.
Despite its recognized importance, thorough contextual assessment remains challenging in evaluation practice (Craig et al., 2018; May et al., 2016; Minary et al., 2018; Pfadenhauer et al., 2017; Squires et al., 2023). This reflects several interconnected issues. First, interventions and their context can range from simple to complicated to complex. While there is considerable variation in how “complicated” and “complex” are defined in the evaluation literature (Renger, 2022), for the purposes of this paper we adopt Rogers' (2009) definition in which “complicated” refers to interventions involving multiple components that operate in relatively stable and predictable ways, and “complexity” is characterized by dynamic, adaptive interactions in which relationships and outcomes shift over time. Second, interventions typically address only a subset of the contextual conditions shaping a problem, while many other influences remain outside program control but still affect outcomes (Renger, 2022; Renger et al., 2015). These influences may span multiple domains, including organizational, geographical, social, economic, cultural, epidemiological, political, and historical spheres and often involve numerous interacting actors and structures, requiring evaluators to consider how these interconnected elements shape implementation and outcomes (Craig et al., 2018; Nilsen & Bernhardsson, 2019; Squires et al., 2023). Finally, inconsistent evaluation frameworks and definitions of context can create confusion about how contextual factors should be identified, prioritized, and incorporated into evaluation practice (Craig et al., 2018; Fynn et al., 2020; Nilsen & Bernhardsson, 2019). These combined factors can create roadblocks for public health practitioners and evaluators seeking to capture, analyze, and interpret intervention context in a meaningful way.
In response to these challenges, a range of approaches, guidance, and frameworks have been developed to support the systematic conceptualization and operationalization of context. Systems-oriented evaluation approaches emphasize that contextual complexity can be managed by deliberate boundary decisions that determine what is considered within or outside the scope of inquiry (Williams, 2011). This principle is evident in system evaluation theory, which emphasizes the need to define a system, including its boundaries and subsystems, before proceeding to evaluate its functioning (Renger, 2015, 2022). In parallel, implementation science offers determinant frameworks, such as the context and implementation of complex interventions (CICI) framework (Pfadenhauer et al., 2017) and the Consolidated Framework for Implementation Research (CFIR; The Consolidated Framework for Implementation Research, 2020), that organize intervention and implementation context into defined domains and constructs.
Building on this body of work and drawing on principles from realist evaluation and improvement science, Vanderkruik and McPherson (2017) developed the contextual factors framework (CFF) to integrate these insights into a practical tool for public health evaluators and implementers (Vanderkruik & McPherson, 2017). The CFF organizes contextual influences across hierarchical levels, and its authors provide examples of its application within public health initiatives in the United States. Although the CFF is cited numerous times in academic literature, published examples of its practical application remain scarce. The present study addresses this gap by exploring the application of the CFF within the evaluation of a rural Australian health promotion intervention.
Study Context
The Australian Context
In Australia, publicly funded health services are organizations responsible for delivering hospital and community-based care to defined geographic populations (Health System Overview, 2024). These services operate within state and territory health systems and are primarily funded through a combination of federal and state government arrangements. They oversee acute care (including hospitals and emergency departments), sub-acute services such as rehabilitation and aged care, and a broad range of community health programs. Beyond direct clinical care, Australian health services also play a role in health promotion, disease prevention, population health planning, workforce development, and partnerships with local government and community organizations. In rural and regional areas in particular, health services often function as integrated providers, coordinating multiple services across large geographic distances to meet local population health needs (Department of Health, 2025).
The Intervention
The rural health promotion intervention discussed in this study is a health service-funded small grants program managed by the service's health promotion team. The health service serves a large, mainly agricultural catchment classified as Modified Monash Model 5 (“small rural towns”; Australian Government, Department of Health and Aged Care, 2021). The program provides grants of up to AUD 5,000 to support locally designed health-promoting activities led by individuals and community groups within the health service catchment area. Since its inception in 2019, multiple funding rounds have supported initiatives such as physical activity programs (e.g., Qigong classes), creative arts workshops (e.g., mosaic and expert-led art sessions), health promotion activities within sporting clubs (e.g., dietitian workshops and healthy canteen modifications), place-based environmental projects (e.g., walking photo trails and community gardens), and social connection initiatives (e.g., welcome dinners for newcomers). Key program features, including eligibility criteria, governance arrangements, and funding priorities, are summarized in Box 1.
Overview of the Health Service Grant Program
Grant amounts: Up to AUD 5,000 per project. Eligible applicants: Individuals, community groups, sporting clubs, schools, and local government entities within the health service catchment area. Non-incorporated applicants are required to be auspiced by an incorporated organization. Projects are required to demonstrate community benefit and alignment with health promotion principles. Funding priorities: Broad and flexible guidelines with emphasis on community engagement and health and well-being outcomes. Priority groups include older adults with cognitive decline, people with disabilities, youth experiencing vulnerability, migrant and refugee communities, people experiencing or at risk of homelessness, individuals facing transport disadvantage, socially or geographically isolated people, LGBTQI+ community members. Application cycle: Annually, promoted via word of mouth, social media, printed materials, and a webpage. Application process: Short online form, with prior mandatory consultation with the health promotion team to assess project suitability. Assessment and selection: Reviewed by a panel comprising a health promotion officer, an academic partner, and a senior executive from the health service. Ongoing support: Each grantee is paired with a health promotion officer; regular check-ins focus on implementation support and improving accessibility. Reporting and accountability: Annual progress reports from grantees and annual public forums to present project outcomes and progress.
The Initial Evaluation
This paper reports on the contextual analysis component of a broader multi-method evaluation of the health service grant program conducted between 2021 and 2024. In 2020, the health service partnered with a university rural health school to support the evaluation of the grant program. As part of this partnership, an industry-embedded PhD scholarship was established through a co-funded arrangement between the university and the health service (La Trobe University, 2025). The doctoral project was jointly developed to address health service needs and priorities, and evaluation planning commenced in 2021 as part of MC's PhD research.
The development of the evaluation framework resulted from a co-design process between MC, academic supervisors (ES, SM), health service staff (an executive staff member and the health promotion team, including DM), and grant recipients. This process has been described in detail elsewhere (Conlin et al., 2023). During the co-design phase of the evaluation, the program logic model was developed collaboratively (Figure 1). Two participatory workshops were held in 2021 and 2023, involving grant recipients, health service staff, and members of the research team. The first workshop focused on developing the initial logic model, and the second provided an opportunity to review and refine the model as new grant recipients and staff became involved in the program. This logic model mapped the program's context, inputs, activities, target audience, outputs, and intended outcomes, while also identifying key assumptions and external factors that could influence program success. Rather than being treated as a static planning artifact, the logic model was conceptualized as a living document and incorporated into the grant program's core suite of operational and evaluation documents. Following the first logic model workshop, priority evaluation questions linked to the logic model were identified through an online follow-up survey distributed to health service staff and grant recipients. Based on these priorities, the grant program evaluation focused on exploring participation, short-term outcomes, and the perceived value of program activities.
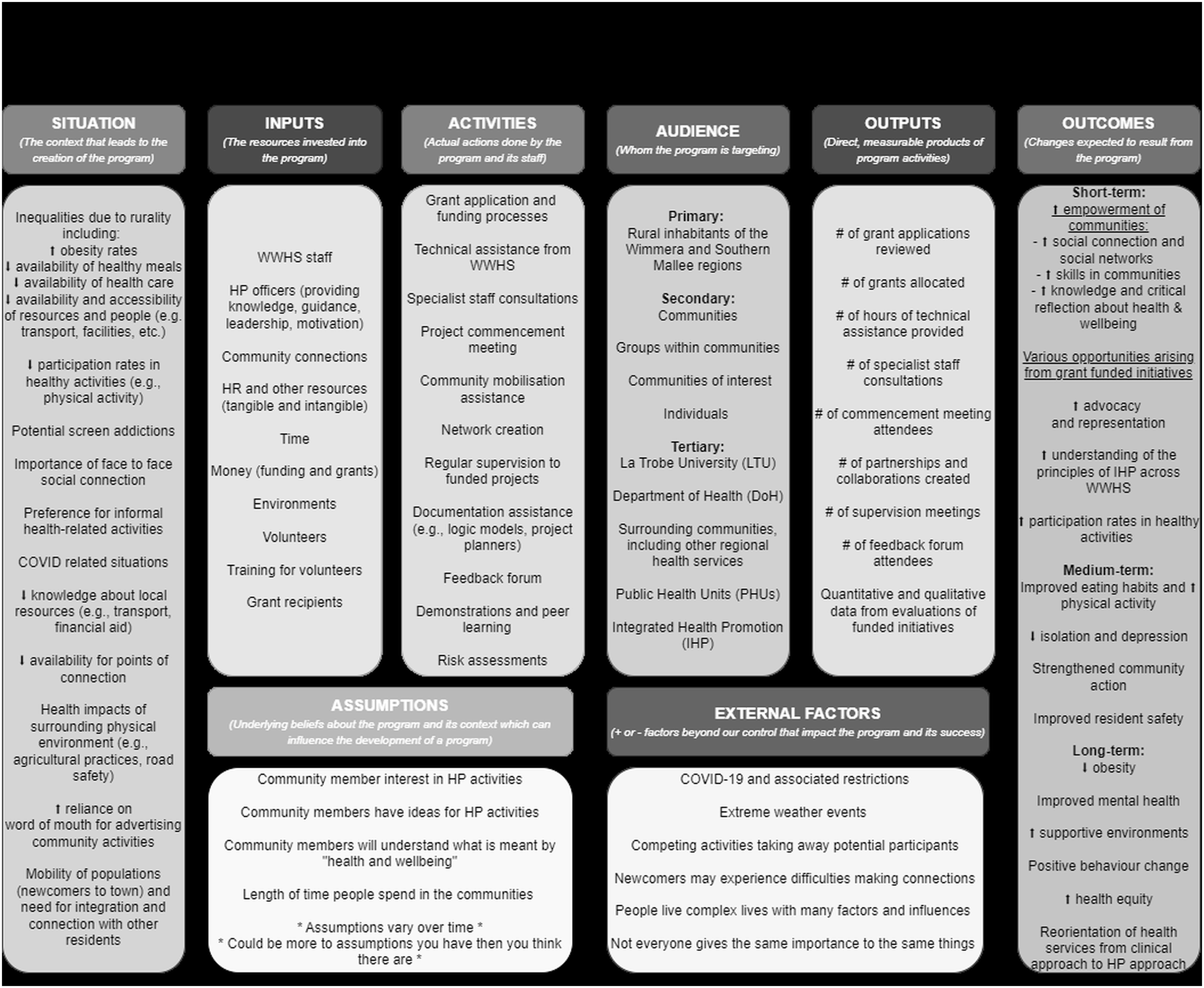
The health service grant program logic model developed collaboratively with grant recipients, health service staff, and the research team. Note. CHWGs = The Health Service's Community Health & Wellbeing Grants program; HP = health promotion; HS = health service; WWHS = West Wimmera Health Service.
Initial Evaluation Findings and Emerging Questions
Across three funding rounds, 14 community initiatives were funded and either fully or partially implemented at the time of evaluation. Evaluation results showed that grant recipients were active community members with multiple roles, often with previous experience in applying for grants. Expected short-term outcomes were partially met: the program goal of community empowerment did not entirely meet its established indicators (namely around increasing community self-capacity, self-determination, and knowledge and capacity for critical reflection on community health). However, there was a notable impact on participants’ perception of and relationship with the health promotion team. Additionally, there was consensus that the program supported the creation of opportunities for community members, which were thought to be otherwise lacking in the rural catchment (e.g., exposure to art through painting or mosaic workshops, or bridging of social groups through welcome dinners; Conlin et al., 2024). These mixed findings raised important questions about how contextual factors may have influenced program implementation and outcomes, particularly in relation to the uneven achievement of empowerment-related goals.
From Initial Findings to This Study’s Objectives
To better interpret the initial evaluation's findings and gain a better understanding of why certain aspects of the intervention succeeded while others presented challenges, a more robust contextual assessment was undertaken, supported by the CFF. This approach was adopted to enable a more systematic examination of contextual influences that may not have been fully captured in the initial evaluation.
This study has two objectives:
To conduct an in-depth contextual assessment as part of the broader evaluation of a rural health promotion intervention, identifying contextual facilitators, barriers, and opportunities for improvement using the CFF. To provide a practical example of how the CFF was applied in a rural health promotion context and to critically reflect on the framework's strengths, limitations, and lessons learned from its real-world use.
Methods
Study Design and Overview
The research activities described here were part of MC's broader PhD work, which encompassed a participatory evaluation of the health service grant program. For this study, which focused on assessing the program's context, an exploratory, qualitative approach was adopted, carried out in two phases between May 2023 and March 2024.
The first phase consisted of an in-depth contextual assessment led by the research team (MC, SM, ES, and DM). The second phase involved a focus group with the health service health promotion team to refine the findings and tease out the most relevant program facilitators, barriers, and improvement opportunities from the contextual assessment. The focus group also served to discuss the strengths and limitations of the contextual assessment guided by the CFF. An overview of the study methods is provided in Figure 2 and detailed below.
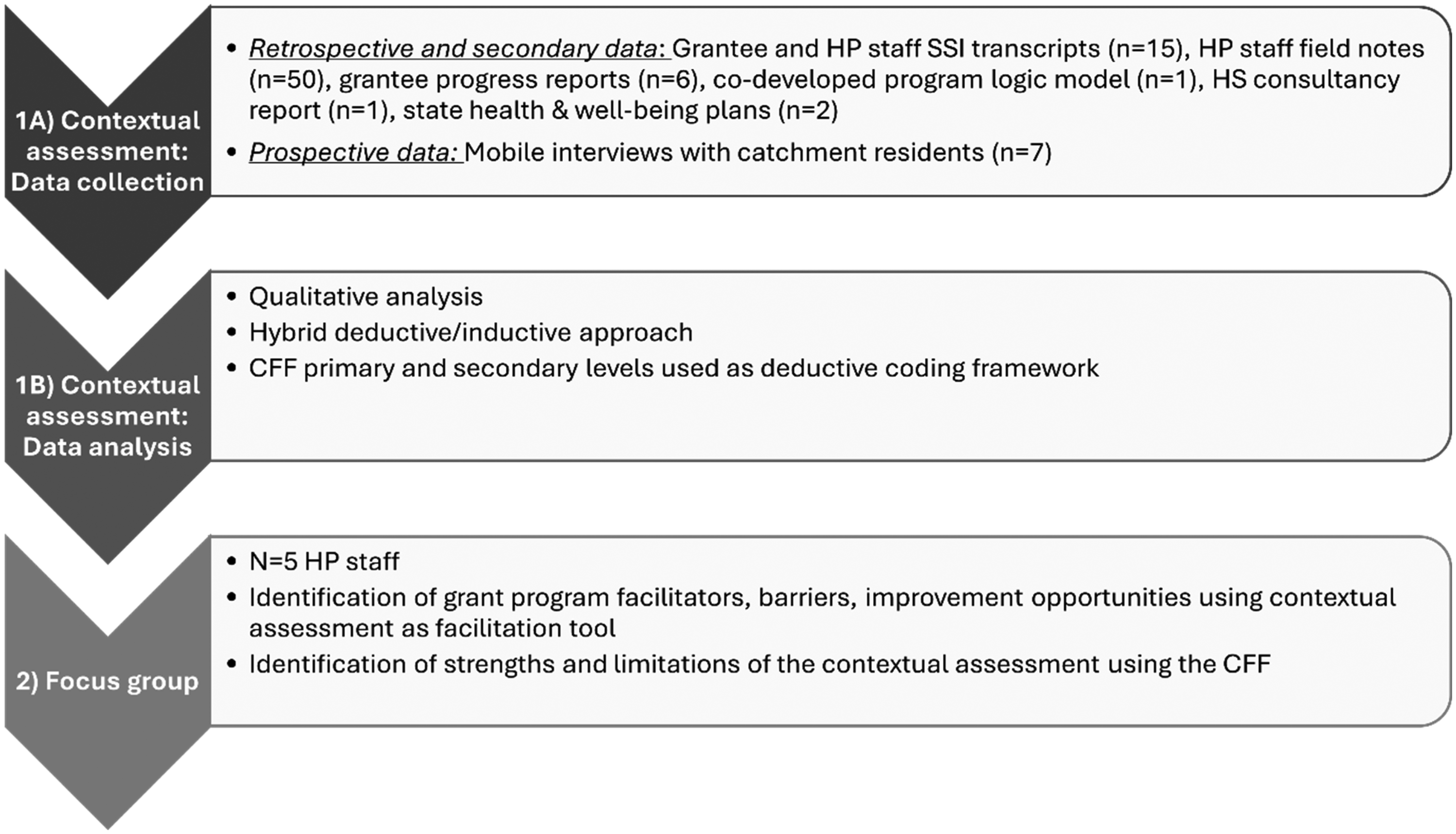
Overview of the study phases and methods. Note. HP = health promotion; SSI = semi-structured interviews; HS = health service; CFF = contextual factors framework.
Ethics
All research activities described in this study were reviewed and approved by the La Trobe University ethics committee (HEC20505). Informed consent was obtained electronically from all participants prior to data collection through REDCap electronic data capture tools hosted at La Trobe University (Harris et al., 2019). Participants were informed of their right to withdraw from the study at any time without penalty. All data were de-identified and stored securely in accordance with university protocols.
Phase 1: The Contextual Assessment
Framework Identification and Selection
To identify different approaches suitable for assessing contextual factors influencing a rural, community-based health promotion intervention, a review of published frameworks was undertaken. Vanderkruik and McPherson's CFF (Figure 3) was ultimately chosen for its simplicity, adaptability, and intended uses as outlined in the framework development publication (i.e., for interventions implemented across multiple settings and for facilitating communication with stakeholders; Vanderkruik & McPherson, 2017).
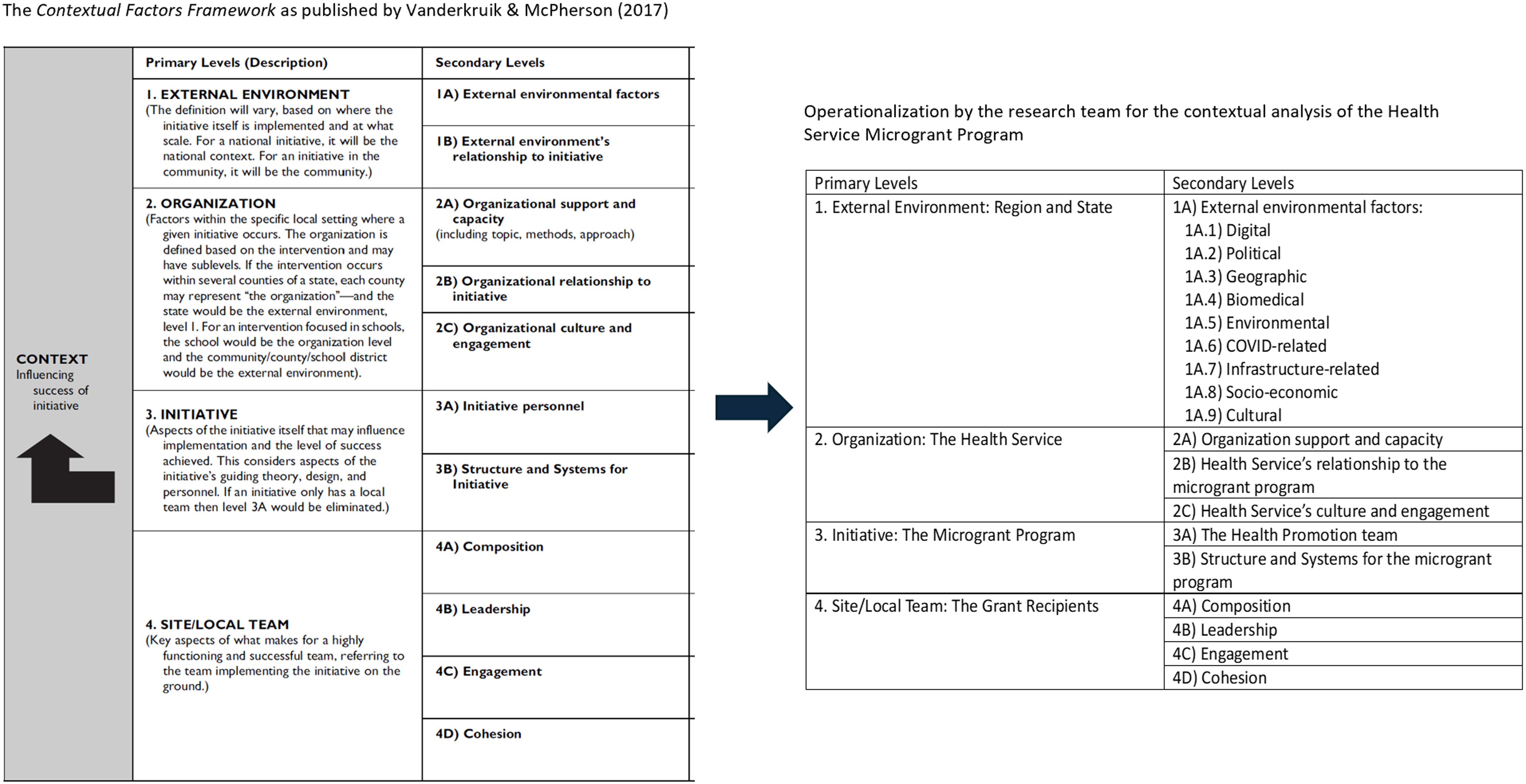
The contextual factors framework and its operationalization for use with the Health Service Grant Program. Note. Adapted from “A Contextual Factors Framework to Inform Implementation and Evaluation of Public Health Initiatives,” by R. Vanderkruik and M. E. McPherson, 2017, American Journal of Evaluation, 38(3), pp. 348–359 (https://doi.org/10.1177/1098214016670029). Copyright 2017 by Sage Publications.
Literature Search for Existing Applications
The research team also carried out a forward citation search to identify additional real-world examples and insights from the application of the CFF, but none were found. This prompted the team to consider that the framework may hold unrealized potential for contextual assessment, leading to this study's second research question about the framework's strengths and weaknesses within a worked example.
Framework Application in This Study
The CFF was applied to guide contextual assessment of the grant program (Figure 3). The four primary levels of the framework, as conceptualized by Vanderkruik and McPherson (2017), were retained without modification. These include:
the external environment (e.g., the national, regional, or community context), the organization delivering the intervention, the initiative (or intervention), the site/local team implementing the intervention.
While the overarching structure of the CFF remained intact, secondary categories within each level (Figure 3) were operationalized to reflect the specific characteristics of the rural health promotion setting under study:
For the external environment, the original secondary category “external environmental factors” was disaggregated into context-specific domains. The secondary category “external environment's relationship to initiative” was examined analytically rather than represented as a separate structural level. The context-specific domains were drawn from examples in national and state-level health promotion documents and are labeled as follows: digital, political, geographic, biomedical, environmental, infrastructure, socioeconomic, cultural, and COVID-related (Australian Government Department of Health, 2021; State of Victoria, 2019, 2023). The organizational level was not changed and is considered to be the health service. The initiative is the grant program, with the initiative personnel being the health promotion team. The site/local team is considered in this case to be the grant recipients, as they are responsible for local implementation of funded activities.
These specifications were intended to clarify how the framework's secondary levels manifested in this context, rather than to alter the underlying structure of the CFF.
Data Collection
A comprehensive qualitative data collection strategy was employed to capture diverse contextual information for the assessment. Data were drawn from both previously generated materials and newly collected qualitative data (Figure 2). Participants included individuals directly involved in the grant program, as well as community members external to the program, to gather community perspectives and help inform the external environment level of the CFF.
Previously Generated Qualitative Data
Qualitative data collected during earlier phases of the grant program evaluation were re-analyzed for the contextual assessment (Conlin et al., 2024):
Transcripts from semi-structured interviews with grant recipients and the health promotion team (n = 15) Field notes from the health promotion team (n = 50 documents) Progress reports completed by grant recipients (n = 6) The grant program logic model (n = 1; Figure 1) A consultancy report informing the health service's earlier health promotion model re-design (n = 1) Recent state-level health and wellbeing plans (n = 2; State of Victoria, 2019, 2023).
Newly Collected Qualitative Data
Additional data collection specific to the contextual assessment involved the use of mobile interviews, or “guided tours” (n = 7 participants across six tours; Conlin et al., 2025). Progress association members and town advisory committee members, as well as service club members from the health service's nine catchment towns, were invited to hold guided tours of their towns for one researcher (MC), with the general theme being “What in your town helps or hinders community health?” Guided tours occurred on foot or by car, with one to two participants per tour. Audio recordings were made of the tours with the consent of participants, and field notes were taken for better accuracy and reflexivity. Recordings were transcribed verbatim.
Data Analysis
Transcripts and documents were uploaded to NVivo 14 to facilitate the analysis (Lumivero, 2023). A qualitative hybrid deductive/inductive thematic analysis approach was adopted using the framework levels as the main codes (Figure 3; Braun & Clarke, 2006). As a first step, one researcher (MC) was responsible for the initial deductive coding and then the inductive identification of major and minor themes. Within each main code, inductive open coding was undertaken to identify patterns across transcripts and documents. These initial descriptive codes were reviewed iteratively and grouped into candidate themes based on conceptual similarity and explanatory relevance. Themes were renamed and refined as analysis progressed to better capture the underlying meaning of the data. For example, early codes such as “local pub as social hub,” “power of word of mouth,” and “knowing your neighbors” were initially treated as discrete concepts. Through comparison, these were consolidated under the broader interpretive theme “value of/focus on social and personal connections,” which was situated within the cultural factors domain of the external environment. As a second step, the coding and themes were reviewed independently by another researcher (SM). Discussion and consensus were used when the researchers had different perspectives on identified themes. The themes were then organized in the CFF table (Figure 3) under their respective headings, forming the completed contextual assessment.
Phase 2: Focus Group with the Health Promotion Team
Participants and Setting
At the time of the focus group (March 2024), the health service health promotion team consisted of four officers and one manager. Their educational qualifications ranged from undergraduate to postgraduate degrees in diverse disciplines (Health Promotion, Public Health, Nutrition, Philosophy of Science and Applied Social Science, Medicine, Dentistry). Experience levels varied from early-career professionals to extensively experienced practitioners with up to 25 years in health promotion and community development. The focus group was held in an online format (Zoom videoconference; Zoom, 2025) and recorded. It comprised the five members of the health promotion team and MC as the facilitator.
Focus Group Process
The focus group was conducted as a structured consensus and refinement step to review and strengthen the contextual assessment. The aim was to confirm the relevance and completeness of the findings, as well as reflect on the practical utility of the framework in the rural health promotion setting. The focus group was conducted within a single session, which proceeded in four stages:
Framework presentation: The aim of the contextual assessment and the methods used were explained to the health promotion team. The original and applied versions of the CFF were presented, and feedback was solicited about the way the framework was operationalized. Initial impressions: Participants were invited to share their initial impressions on how the CFF could help understand contextual factors influencing the grant program and the team's rural health promotion work more broadly. Contextual assessment review: The research team's contextual assessment was then presented to the health promotion team, who were encouraged to suggest modifications to the analysis (e.g., missing elements, alternative perceptions). Barrier/facilitator/opportunity identification: Following this review, the health promotion team was then asked to identify which contextual factors and themes represented barriers, facilitators, and opportunities to their work within the grant program.
Following the focus group, the audio recording of the session was reviewed to ensure that all recommendations and suggested modifications were accurately captured and addressed within the contextual assessment table. The revised table was sent to the participants via email for member-checking and final comments. The focus group findings have been summarized narratively below.
Findings
The comprehensive data collection and analysis process yielded substantial contextual information, resulting in an extensive and detailed contextual assessment of the health service grant program. Given the volume of findings, the complete contextual assessment table, including all major and minor themes, is presented in Supplemental Material A. Table 1 presents an abridged version of the contextual assessment, featuring major themes identified through the research team's analysis and those prioritized by the health promotion team during the focus group as having particular significance for the grant program. The contextual program facilitators (“F”), barriers (“B”), and improvement opportunities (“O”) have been highlighted and indicated as such in the table.
Contextual Assessment of the Rural Health Promotion Grant Program Using the Adapted Contextual Factors Framework: Major Themes and Identified Barriers (B), Facilitators (F), and Opportunities (O).
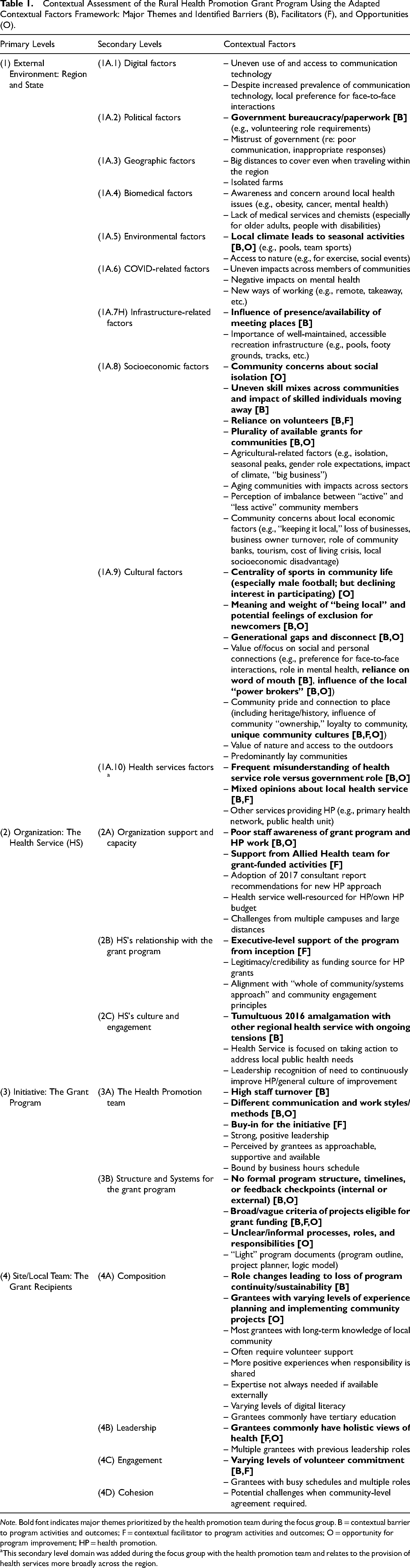
Note. Bold font indicates major themes prioritized by the health promotion team during the focus group. B = contextual barrier to program activities and outcomes; F = contextual facilitator to program activities and outcomes; O = opportunity for program improvement; HP = health promotion.
This secondary level domain was added during the focus group with the health promotion team and relates to the provision of health services more broadly across the region.
Grant Program Facilitators, Barriers, and Opportunities for Improvement
The External Environment
Barriers identified within the external environment included administrative and regulatory requirements that created challenges for community members and funded projects. As one grant recipient explained, “The biggest hindrance … is just seeking all of the land permissions and things like that….” Legal requirements related to working with children, while important for safeguarding, meant that one planned intergenerational event had to be restructured into separate sessions for different age groups.
Role confusion between the health service and local government, particularly around service provision (e.g., homecare support), contributed to mixed community opinions about the health service. This was compounded by the organization's status as a major local employer, which meant that community members at times had multidimensional experiences with the organization (as consumers of healthcare, employees, and potential grant recipients). One grant recipient described that this occasionally led to tensions within the community: “I did have some animosity in the community … there was some quite really nasty comments: That's not fair. She should be excluded [from receiving a grant as a health service staff member].”
Infrastructure limitations were also identified, including limited public meeting venues and seasonal closures. Sociocultural dynamics such as reliance on word-of-mouth communication and the influence of community “gatekeepers” were also described as shaping community engagement. A health promotion team member reflected on these dynamics, noting that “[this planning event] led to a discussion about the difficulty of advertising in small towns … and the reliance … on word of mouth and how that can work with you and against you at times.”
Despite these barriers, several facilitating factors were identified within the external environment. These included community members with positive opinions of the health service, high volunteering rates, and distinctive community cultures that could be leveraged for engagement. As one health promotion team member explained, “Each community is a bit different … so the priorities, or the things that they want, is different….”Opportunities identified during focus group discussions included popular seasonal activities like men's Australian Football as strategic engagement gateways, post-COVID community re-engagement desires, and intentional community linking when reviewing grant applications to address “local” versus “non-local” social dynamics (where concerns were identified about the potential social exclusion of newer residents).
The Organization
At the health service level, most factors were deemed to be facilitating the team's work with the grants specifically and with other implemented programs. There was consensus around having executive-level and clinical-level support (i.e., through the allied health team) for the grants, and that there was general alignment between the core values of the program (i.e., the importance of place-based activities and community engagement) and the organizational culture. One health promotion team member recalled that “both the [health service] executive director and the CEO immediately said, absolutely,” when the initial proposal for the grant program was presented.
A factor that was identified as both a barrier and an opportunity within the organization was a perception of poor staff awareness and understanding of the grant program and of health promotion work more generally. One team member noted, “I still don't think a lot of [health service staff] know what health promotion is or that we have the grants.” At the time of discussion, plans were in motion to address this limitation with the hopes of harnessing more momentum for the program.
The Initiative
Contextual factors around the grant program itself were divided into two levels as per the CFF: initiative personnel (the health promotion team) and the structures and systems for the grant program. The health promotion team were perceived by grantees as being very approachable and available, and both the grantees and the team identified the positive influence of strong leadership within the team. As one grant recipient noted, “[The health promotion manager] is a real leader in this space … she literally held my hand to put through the grant application.” These characteristics were considered facilitating factors within the grant program activities. However, high staff turnover and differences in communication styles within the team were seen as hurdles. A health promotion team member explained that “[the team] also had a lot of staff changes … and that's another weakness because you build a rapport and then people leave.”
At the level of program structures and systems (e.g., program outline and processes), several challenges were identified. For example, the health promotion team described the grant processes as being complex and unclear at times. One health promotion team member reflected, “…the application process keeps changing from year to year … it seems to be becoming more complicated.” Nonetheless, actionable opportunities for improvement in this space were highlighted, such as the review and formalization of program documentation into accessible digital formats.
Local Teams
The biggest challenges ascertained at the grant recipient level were the multiplicity of roles held by grantees, leading to busy schedules and negative impacts on funded activity sustainability when leadership changed hands. A grant recipient explained: “Anyone that's got … any kind of motivation to help out with community health is flat out busy in their work, their paid work, their families.” Additionally, as mentioned in the external environment level, the common reliance on volunteers could quickly become a challenge when commitment to the funded activity or general availability fluctuates. Another grant recipient commented: “I guess with volunteers, some really own it and some don't and some don't have time….” A facilitating factor, however, was the grant recipient's holistic perceptions of health and the opportunity this created for potential continued education with grantees around the principles of health promotion and the social determinants of health.
Discussion
Study Contributions
Although the importance of context in public health evaluation is well established, operationalizing contextual assessment in applied settings remains challenging. The CFF offers a structured approach to support contextual assessment, yet its real-world application remains limited in the literature, with questions about its utility and applicability across diverse settings. This study addresses this gap by providing a worked example of the CFF within a rural Australian health promotion grant program.
The initial program evaluation findings prompted further exploration of the factors shaping program outcomes, raising questions about why certain aspects of the intervention were more or less successful. The CFF was selected because it enables a broad, multi-level examination of contextual influences. Although alternative approaches such as root cause analysis are commonly employed to investigate and diagnose implementation issues (Coşkun et al., 2012), the research team considered that such approaches are typically oriented toward identifying discrete causes of specific problems and may be less suited to capturing multidimensional contextual factors shaping diverse program outcomes (Peerally et al., 2017). In addition to its conceptual fit, the CFF was selected for its accessibility and practical utility for stakeholders involved in the evaluation. The framework's relatively simple structure and terminology made it suitable for use by practitioners with varying levels of evaluation experience, supporting engagement among early-career professionals and those with limited formal evaluation training. This was particularly important given the applied nature of the evaluation and the intention to support the ongoing use of evaluation tools within the health service beyond the life of the study.
Over two qualitative phases, this study identified contextual program facilitators and barriers across the four levels of the CFF: the external environment, the organization, the initiative, and local teams. In doing so, the study demonstrates how structured contextual assessment can move evaluators beyond general awareness of context toward systematic analysis that informs program improvement. Importantly, applying the CFF not only generated contextual insights but also supported stakeholder engagement, explanatory interpretation of evaluation findings, and the identification of actionable opportunities for program refinement. These considerations are reflected in the strengths and limitations of the framework discussed below.
Strengths of the Contextual Factors Framework
One of the intended purposes of the CFF is to function as a communication tool with stakeholders (Vanderkruik & McPherson, 2017). In this study, the framework successfully structured dialogue between the research and health promotion teams. The focus group discussion and member-check feedback indicated that the framework stimulated reflection, surfaced diverse interpretations of contextual influences, and facilitated shared understanding. Participants also indicated that the way the framework had been operationalized for the rural health promotion setting was intuitive and helpful for structuring contextual information. One refinement suggested by the team was the addition of a new domain within the external environment level to better capture regional and state health service provision, which was subsequently incorporated into the contextual assessment. The structured approach enhanced transparency and supported a more systematic interpretation of how contextual factors influenced program delivery in ways that more informal contextual consideration may not have achieved. In this regard, the framework aligns with the CDC Evaluation Standard of Relevance and Utility, which emphasizes that evaluations should focus on information important to stakeholders, generate actionable findings, and present them in understandable and timely ways (CDC, 2024). The CFF supported these aims by presenting contextual information in a structured and accessible format that responded to stakeholder interests and was directly linked to program planning.
Applying the CFF also enhanced the explanatory interpretation of program outcomes. For example, it helped contextualize why certain grant-funded initiatives struggled to gain momentum, highlighting influences such as leadership capacity constraints and the low community profile of specific grantees. It also illuminated the influence of community “gatekeepers” and aging demographic patterns. Without structured contextual assessment, these influences may have remained anecdotal observations rather than analytically integrated explanations.
Another challenge in evaluation is translating contextual information into concrete recommendations. In this study, the CFF supported moving from contextual description to action by identifying leverage points across levels. For example, the assessment highlighted opportunities to formalize and digitize program documentation, refine engagement strategies with community leaders, incorporate succession planning discussions into grant processes, and align planning with seasonal community dynamics. In this way, the CFF functioned not only as an analytic tool but also as a planning instrument, reinforcing the utility of structured contextual assessment for rural health promotion practice.
Limitations of the Contextual Factors Framework
While the CFF provided structural clarity and practical value, several limitations were identified. Compared with more expansive contextual frameworks such as CICI (Pfadenhauer et al., 2017) or CFIR (Damschroder et al., 2022), the CFF offers a more bounded structure. Its four-level categorization may not fully capture the breadth of contextual domains conceptualized in implementation science or health promotion literature (Nilsen & Bernhardsson, 2019; Poland et al., 2009). In particular, the framework gave limited attention to power relations, which are central to health promotion theory (Poland et al., 2008). Although refinement of secondary levels can address some gaps, the framework does not inherently foreground these dimensions.
A central limitation identified by participants was the framework's tendency to represent context as relatively static and segmented. External environmental influences were described by the health promotion team as exerting “trickle-down” effects across organizational and initiative levels, yet the framework did not explicitly model these interrelationships. Dynamic and evolving contextual processes, such as the shifting impacts of the COVID-19 pandemic, were not easily represented within discrete levels and domains. This limitation reflects broader critiques of contextual frameworks that categorize context into domains without capturing feedback loops or synergistic effects (May et al., 2016; Pfadenhauer, 2022). While systems-based approaches may offer greater analytic depth in representing such complexity, they can be less accessible to non-specialist audiences (Barbrook-Johnson & Penn, 2022). In this study, the simplicity of the CFF supported collaborative dialogue but limited the representation of interdependence.
Practical Implications for Evaluation Practice
This study suggests that the CFF serves as a practical scaffold for embedding structured contextual assessment directly into evaluation design, enabling evaluators to systematically organize contextual inquiry and integrate contextual analysis into interpretation and planning rather than treating it as a peripheral or purely descriptive exercise. Importantly, the framework supports moving from contextual awareness to prioritized action. By categorizing influences across external, organizational, initiative, and local team levels, evaluators and stakeholders can distinguish between contextual factors that require strategic navigation and those that represent modifiable leverage points. In this study, for example, inconsistent program documentation initially appeared as a minor operational issue. When situated within the initiative level and interpreted alongside staff turnover and communication challenges, it was reframed as a modifiable influence on program processes and stakeholder communication. This structured interpretation supported prioritizing the formalization and digitization of documentation processes as a feasible improvement.
For evaluators working in rural and community-based health promotion settings, the framework may therefore serve not only as a mapping tool but also as a decision-support structure. It can guide data collection, stakeholder discussions, and analytic synthesis, linking contextual conditions more clearly to program outcomes and clarifying where intervention is possible within existing capacity. The findings of this study also indicate that elaborating the external environment level through multiple domains may enhance applicability in health promotion contexts, particularly where diverse, intersecting systems shape intervention feasibility, implementation, and impact. Explicitly considering power dynamics may further strengthen contextual analysis in equity-oriented programs. At the same time, when evaluation aims require analysis of dynamic feedback loops or complex system interactions, the CFF may be supplemented with systems-based approaches. A layered strategy, using the CFF for structural clarity and complementary tools for modeling interrelationships, may balance accessibility with analytic depth. Collectively, these implications position the CFF not as a comprehensive solution to contextual complexity, but as a structured and usable entry point for strengthening the integration of context into applied evaluation practice.
Strengths and Limitations of This Study
This study addresses a gap in the literature by offering a practical example of the CFF applied to the rural health promotion setting. The integration of stakeholder input with varied perspectives (program staff, grant recipients, external community members) generated contextually grounded insights with direct utility for program improvement, highlighting the CFF's value as both an assessment and communication tool. However, several limitations warrant consideration. The staged design of the evaluation, in which the CFF was applied following the initial evaluation, has implications for the evaluation standard of feasibility (e.g., practicality and cost-effectiveness; Better Evaluation Knowledge, 2024). Earlier integration of the framework may have supported a more streamlined and efficient approach to data collection by incorporating comprehensive contextual analysis from the outset. However, this was not feasible as the timing of the initial evaluation coincided with the COVID-19 pandemic, which constrained data collection to virtual methods that were not considered sufficient to capture the depth and nuance of contextual influences. As such, the staged approach may be less practical in resource-constrained evaluation settings. Other considerations include that further application of the CFF across diverse settings and intervention types would be valuable to assess its robustness. Additionally, the framework was used over a relatively short period, and an extended application may reveal additional strengths or limitations. Finally, the absence of a comparative analysis with other contextual frameworks restricts the study's capacity to assess the CFF's relative utility or comprehensiveness.
Conclusion
This study applied the CFF to conduct an in-depth contextual assessment of a rural health promotion grant program while critically evaluating the framework's strengths and limitations in this setting. The CFF provided a structured and practical approach to identifying key contextual barriers, facilitators, and opportunities for program improvement, while also supporting communication and planning with stakeholders. Its application in a rural health promotion context demonstrated the framework's capacity to accommodate complex, community-based intervention settings, but also highlighted its limited ability to capture dynamic contextual interrelationships and power dynamics. These findings position the CFF as a useful entry point for contextual assessment in evaluation practice, while suggesting that complementary approaches may be needed to better account for evolving interconnections in rural health promotion contexts. In doing so, this study contributes to both a practical understanding of contextual influences in rural health promotion and methodological insights for strengthening contextual assessment in evaluation practice.
Supplemental Material
sj-docx-1-aje-10.1177_10982140261455349 - Supplemental material for Contextual Assessment in Evaluation: Applying the Contextual Factors Framework to Inform the Findings of a Rural Health Promotion Program Evaluation
Supplemental material, sj-docx-1-aje-10.1177_10982140261455349 for Contextual Assessment in Evaluation: Applying the Contextual Factors Framework to Inform the Findings of a Rural Health Promotion Program Evaluation by Michele Conlin, Dorothy McLaren, Sean MacDermott, Evelien Spelten and Corina Modderman in American Journal of Evaluation
Footnotes
Acknowledgments
The research team thanks West Wimmera Health Service for their patience and interest in exploring innovative approaches to health promotion and to the community members who shared their perspectives and demonstrated a commitment to research and improving community health.
Author Contributions
Michele Conlin: conceptualization (lead), data curation, formal analysis (lead), investigation, methodology, project administration, visualization, and writing—original draft preparation. Dorothy McLaren: conceptualization, supervision (equal), and writing—review and editing (equal). Sean MacDermott: conceptualization, formal analysis, supervision (equal), and writing—review and editing (equal). Evelien Spelten: conceptualization, formal analysis, supervision (equal), and writing—review and editing (equal). Corina Modderman: supervision (equal) and writing—review and editing (equal).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
All procedures were performed in compliance with relevant laws and institutional guidelines and have been approved by the La Trobe University ethics committee (HEC20505). Privacy rights of participants have been observed, and informed consent was obtained.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is part of the main author's Industry PhD, which is co-funded by West Wimmera Health Service and La Trobe University. No external funding was received.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.