
Abstract
The purpose of this study was to examine the effects of special educators’ delivery of training that included an initial training session and follow-up coaching on paraprofessional implementation of an evidence-based practice for students with autism spectrum disorder (ASD). Three special educators each trained a paraprofessional in their classroom to implement functional communication training (FCT) to address the challenging behavior of a student with ASD. The training procedures incorporated the following aspects of behavioral skills training: instruction, modeling, rehearsal, and feedback. Training from special educators resulted in high levels of paraprofessional FCT implementation that maintained over time for two paraprofessionals. Special educators and paraprofessionals found the training to be practical and effective. We present implications for practice and future research directions for paraprofessional training models focused on challenging behavior interventions.
Keywords
Paraprofessionals serve an important role supporting special educators and other school members in providing special education and related services to students with disabilities in school settings (Individuals with Disabilities Education Act [IDEA], 2004). The reliance on paraprofessional supports has been well documented with the most recent federal data indicating that approximately 435,817 paraprofessionals support students with disabilities in the United States, a number exceeding that of special educators (U.S. Department of Education, 2019). Paraprofessionals support students receiving special education services under a range of IDEA eligibility categories. Carter et al. (2009) found that a large percentage of paraprofessionals reported working with students with learning disabilities (82%), autism spectrum disorder (ASD; 79%), and intellectual disability (74%). As paraprofessionals support students with a range of disabilities, they assume a variety of responsibilities that include, but are not limited to, delivering instruction in one-to-one, small-group, and large-group formats; collecting assessment data; facilitating social interactions; and managing challenging behavior (Carter et al., 2009; Fisher & Pleasants, 2012).
Supporting the behavioral and social needs of students with disabilities has been identified as a significant role among paraprofessionals. In fact, more than 79% of paraprofessionals have reported managing student challenging behavior at least weekly (Carter et al., 2009). Paraprofessionals may assist in the delivery of different school- and class-wide behavioral supports along with behavior support plans specific to individual students (Ashbaker & Morgan, 2015). The importance of this paraprofessional role is also emphasized in the Council for Exceptional Children’s (CEC, 2015) paraprofessional standards that set forth several knowledge and skill competencies related to the communicative intent of student behavior, implementation of individualized and positive behavioral supports identified by professionals, and compliance with legal and ethical guidelines concerning behavioral support. In addition, both special educators and paraprofessionals identify paraprofessional training in behavioral intervention as a high-priority training area (e.g., Mason et al., 2020; Sobeck & Robertson, 2019), suggesting that paraprofessionals are not always well prepared to address challenging behavior.
Fortunately, when paraprofessionals receive adequate training and supervision, their implementation of instructional practices and other supports improves, which ultimately enhances learning environments and outcomes for students. There is a growing body of paraprofessional training research that identifies several effective components of paraprofessional training, including modeling and coaching with performance feedback (e.g., Brock & Anderson, 2020; Rispoli et al., 2011). Coaching has been identified as a training strategy that is effective in promoting implementation of evidence-based practices and typically involves delivering follow-up support such as performance feedback to the trainee after initial training has occurred (Kretlow & Bartholomew, 2010). Focusing specifically on challenging behavior, Walker, Carpenter, et al. (2020) reviewed 17 studies involving paraprofessional-delivered interventions to address challenging behavior among students with disabilities. A variety of training strategies including instruction, modeling, and coaching with performance feedback were used to support paraprofessionals in behavioral intervention implementation, and generally resulted in positive paraprofessional and student outcomes. In another recent example, Walker, Coogle, et al. (2020) examined 23 paraprofessional training studies specific to students with ASD and found that a range of training strategies contributed to positive paraprofessional implementation of various practices (e.g., function-based intervention, discrete trial teaching) primarily to promote social/communication skills and address challenging behavior. Although promising, results from these reviews suggest that researchers largely have been responsible for training paraprofessionals, thus limiting the field’s understanding of the feasibility and efficacy of educator-delivered paraprofessional training.
A cascading model of support can be an effective way for researchers and other professionals to support educators in their supervisory role. Also referred to as a train-the-trainer model or pyramidal training model, a cascading model of support is beneficial in that it provides an efficient way of disseminating information to a range of school members. In the case of the current study, the cascading model begins with training special educators who subsequently train paraprofessionals in their classrooms. This is in contrast to the most common approach found in the paraprofessional training literature whereby researchers provide direct training to paraprofessionals. A few recent studies have explored cascading models of paraprofessional training and provide encouraging evidence that such models can be effective in preparing educators as coaches and, in turn, educators delivering effective training to paraprofessionals (e.g., Brock & Carter, 2016; Lerman et al., 2019; Probst & Walker, 2017). For example, Lerman et al. (2019) found that training educators to deliver behavioral skills training (BST) improved paraprofessional implementation of discrete trial teaching. Likewise, Brock and Carter (2016) found that special educators were successful in delivering a multicomponent training package consisting of an initial workshop session, video modeling, and coaching with performance feedback to paraprofessionals. As a result, paraprofessionals implemented peer support arrangements among students with severe disabilities with high levels of implementation fidelity.
The overarching purpose of the current study was to extend the field’s understanding of the effectiveness of a cascading model of support whereby special educators serve as coaches to paraprofessionals who support students with ASD. Given the continued reliance on paraprofessionals to support students with ASD and the significant role paraprofessionals play in addressing student challenging behavior, this study specifically focused on supporting special educators to train paraprofessionals to implement functional communication training (FCT; Carr & Durand, 1985), an evidence-based practice for addressing challenging behavior among students with ASD (Steinbrenner et al., 2020). FCT is a differential reinforcement procedure that involves determining the communicative function of challenging behavior through functional behavior assessment (FBA) and teaching an alternative communicative behavior that serves the same communicative function (i.e., functionally equivalent communicative response; FCR). Although practitioners in school environments can implement FCT successfully, researchers have primarily delivered training to support practitioner-implemented FCT and few studies have examined paraprofessional FCT delivery (Andzik et al., 2016; Walker et al., 2018). To address these limitations, we conducted a single-case intervention study to answer the following research questions: (a) What are the effects of special educator–delivered training consisting of an initial training session and follow-up coaching on paraprofessional implementation of FCT? And (b) Do special educators and paraprofessionals find the paraprofessional training intervention to be effective and feasible?
Method
Participants
Three classroom teams (triads) participated in the study. Each triad consisted of a special educator, paraprofessional, and student with ASD. To qualify for participation, special educators were required to (a) directly supervise a paraprofessional who assisted the special educator in supporting a student with ASD and (b) provide consent to serve as the paraprofessional’s coach throughout the study. Likewise, paraprofessionals were required to (a) directly support a student with ASD who was eligible to participate in the study and (b) provide consent to receive training from the supervising special educator. It should be noted that, although paraprofessionals directly supported student participants, they were not assigned to work exclusively with them, but instead provided supports to all students in the classroom during one-to-one, small-group, and whole-group activities throughout the school day. Finally, student participants were required to (a) receive special education services under the IDEA eligibility category of autism; (b) engage in persistent challenging behavior that interfered with learning or social opportunities, caused harm to self or others, and/or resulted in property destruction (as confirmed during FBA observations); and (c) have parent permission to receive FCT to address challenging behavior. Special educators nominated student participants based on their history of persistent challenging behavior in any form that occurred multiple times throughout one or more routines during the school day.
Triad 1
Special Educator 1 identified as a 41-year-old White female with a Bachelor of Science degree in special education. She had more than 15 years of experience supporting students with ASD as a therapist and teacher. She reported prior training in applied behavior analysis, crisis prevention, and the TEACCH® Autism Program. Paraprofessional 1 identified as a 46-year-old White female who had 15 years of experience working as a paraprofessional in elementary, middle, and high school settings and <1 year working under the direction of the special educator. She had an Associate’s degree and reported prior training in crisis prevention and social/emotional learning for early learners. Student 1 was identified as a 10-year-old White male with ASD and intellectual disability. He spent most of the day in a self-contained classroom for students with ASD. Prior to the study, Student 1 communicated at an emergent level (i.e., used single words in any mode or rote word combinations) using gestures, picture communication systems, and speech as his primary modes of communication. Student 1 was nominated for the study based on a history of climbing to the top of playground equipment and jumping off during recess. Paraprofessional 1 typically addressed these behaviors with redirection and timeout from recess.
Triad 2
Special Educator 2 identified as a 40-year-old White female who had 4 years of experience as a special educator and 8 years as a paraprofessional. She reported prior training in FBA delivered by the school district and crisis prevention. Paraprofessional 2 identified as a 58-year-old Black female who had 14 years of experience working as a paraprofessional in elementary, high, and special education school settings and 4 years working under the direction of the special educator. She had an Associate’s degree and reported prior training in crisis prevention. Student 2 was identified as a 6-year-old Black male with ASD and developmental delay. He spent most of the day in a self-contained classroom for students with ASD. Prior to the study, Student 2 communicated at an emergent level primarily using gestures, vocalizations, and a few manual signs. He was nominated to participate in the study due to a history of elopement, aggression, and nonparticipation during one-to-one and small- group math instruction. Paraprofessional 2 addressed these behaviors by delivering redirection and reprimands and blocking physically aggressive behavior.
Triad 3
Special Educator 3 identified as a 24-year-old White female who had 3 years of experience as a lateral entry special educator, meaning that she pursued an alternative route to licensure that allowed her to teach while receiving training to become fully licensed. She reported prior training in FBA and function-based intervention delivered by the school district and coursework in applied behavior analysis. Paraprofessional 3 identified as a 53-year-old White female who had 3 years of experience working as a paraprofessional in an elementary school; she spent all 3 years working under the supervision of Special Educator 3. She had some college experience and reported training in crisis prevention and the TEACCH Autism Program. Student 3 was identified as an 8-year-old Black male with ASD. He spent most of the day in a self-contained classroom for students with ASD. Prior to the study, Student 3 communicated at a multiword level (i.e., used non-rote combination of words in any mode) using a device with speech output (i.e., Accent® 1000), gestures, and a few manual signs. He was nominated to participate in the study due to his history of aggression, disruptive vocal behavior, and nonparticipation during math instruction. The paraprofessional typically redirected and reprimanded the student to address challenging behavior.
Settings
All special educators provided training consisting of an initial training session and follow-up coaching to paraprofessionals who delivered FCT to student participants. Training sessions took place in either a quiet location in the classroom or in the special educator’s office during school hours. Paraprofessional 1 delivered FCT during recess on the playground. During recess, all eight students from the student’s self-contained classroom for students with ASD were present along with the special educator and two paraprofessionals. Students from this classroom consisted of six male and two female students, ages 10 to 12, all of whom had a diagnosis of ASD. In addition, other third-grade general education classes were on the playground at that time. Each general education class had one teacher and approximately 25 students. Paraprofessional 2 implemented FCT at a small table in the back of a self-contained classroom for students with ASD during one-to-one math instruction while other students received academic instruction at various centers in the classroom. The classroom consisted of nine male students, ages 5 to 7, and two paraprofessionals. All students had diagnoses of ASD. Two of these students also had multiple disabilities and three had a developmental delay. Similarly, Paraprofessional 3 delivered one-to-one math instruction in a self-contained classroom for students with ASD while other students in class also worked on math activities at their desks. The classroom consisted of 11 male students, ages 6 to 8 years, and two paraprofessionals. Eight of the students had a diagnosis of ASD, and the other three had a developmental delay.
Study Design
To examine the effects of special educator–delivered training on paraprofessional FCT implementation, we used a multiple baseline across participants design (Ledford & Gast, 2018). We introduced intervention to Paraprofessional 1 when stability was observed across all three paraprofessionals for three consecutive sessions. We defined stability as 80% of baseline data falling within a 20% range (Ledford & Gast, 2018). For Paraprofessionals 2 and 3, we introduced intervention following a clear level change in the previous paraprofessional’s implementation data with at least two consecutive sessions with no overlapping data with baseline. To determine whether a functional relation was present, we visually inspected graphed data to examine level, trend, variability, overlap, and immediacy of effects within and between conditions. It should be noted that, because paraprofessional implementation was the primary dependent measure that drove decisions about intervention introduction, we were unable to experimentally evaluate the effects of paraprofessional-implemented FCT on challenging behavior and FCR outcomes. Nonetheless, we collected student outcome data to descriptively examine student behavior across the duration of the study.
Dependent Measures
Paraprofessional-implemented FCT
To measure paraprofessional-implemented FCT across all phases, we collected implementation fidelity data specific to the procedural elements for each response prompting system (i.e., system of least prompts, constant time delay; Brown et al., 2019) used to teach students FCRs. Procedural elements that were common across all prompting systems were the delivery of an attentional cue, an instructional cue, response prompts, error correction contingent on incorrect student responses, and reinforcement contingent on correct student responses. Because Paraprofessional 1 implemented the system of least prompts, we measured implementation of the defined prompting hierarchy. Paraprofessionals 2 and 3 implemented constant time delay. As such, we measured implementation of the controlling prompt during sessions with a 0-s response interval and those with a 3-s response interval.
Procedures
FBA
Prior to developing the FCT intervention, the researchers conducted an FBA for each student participant during the target routine in which challenging behavior most often occurred to identify a hypothesized function. The FBA for Student 1 focused on inappropriate climbing and jumping on playground equipment. Inappropriate jumping was defined as both feet leaving the boundaries of the playground equipment from higher than 3 ft off the ground. Climbing was defined as at least one foot on an area of the playground not meant to be climbed on (e.g., stair railings). The FBA for Student 2 focused on off-task behavior and aggression. Off task behavior was defined as any behavior that interfered with the student’s ability to complete the math task including turning his back to the task or paraprofessional, not responding to the paraprofessional’s request within 5 s, hugging the paraprofessional, putting task materials in mouth, and leaving the work area. Aggression included scratching (i.e., student makes contact with the paraprofessional using his fingernail or attempts to do so), biting (i.e., student makes contact with the paraprofessional’s skin or clothing with an open mouth or attempts to do so), and hair pulling (i.e., student grabs paraprofessional’s hair with hand or attempts to do so).
Finally, the FBA for Student 3 focused on aggression, disruptive behavior, and nonparticipation. Aggression included pinching (i.e., student makes contact with paraprofessional’s skin or clothing using a pincer grasp or attempts to do so), hitting (i.e., student makes contact with paraprofessional using an open or closed fist or attempts to do so), kicking (i.e., student makes contact with paraprofessional with his foot or attempts to do so), and throwing items (i.e., student throws an item in the direction of an adult or peer). Disruptive behavior included screaming (i.e., any vocalization at a volume above that of his current environment), crying (i.e., persistent vocalizing while his face was scrunched, with or without tears), and stomping (i.e., moving one or both feet toward the floor with sufficient force to make an audible sound). Nonparticipation was defined as not responding to a paraprofessional request within 5 s of delivery.
To conduct the FBA, a member of the research team first administered the Functional Assessment Interview (FAI; O’Neill et al., 2015) with the classroom teacher. Next, the teacher and paraprofessional completed the Questions About Behavior Functioning (QABF; Paclawskyj et al., 2000) form. Based on data from the FAI and QABF, researchers formulated a tentative hypothesis about behavior function. Finally, researchers conducted observations using the Functional Observation Assessment (FAO; O’Neill et al., 2015) to mitigate the ambiguity in the hypothesis statements. The hypothesis statements resulting from the FBA process were as follows: Student 1: When playing alone on the playground without adult eye contact, the student will climb on the outside of playground equipment and jump off to obtain teacher attention; Student 2: When presented with a math task, the student will engage in off-task behavior and aggression to escape the math task; and Student 3: When presented with a math task, the student will engage in aggression, disruptive behavior, and nonparticipation to escape task demands.
FCT plan development
After completing the FBA, researchers met with special educators to develop an instructional plan for FCT implementation based on the FBA outcomes for each student. The researcher shared the results of the FBA and developed a competing behavior pathway (O’Neill et al., 2015) with the educator to illustrate FBA outcomes and pinpoint the FCR to target for FCT. Next, the researcher guided the special educator through a series of decision-making prompts (available from first author) to finalize the FCT plan. These prompts resulted in decisions regarding the mode of augmentative and alternative communication (AAC) for the FCR, instructional procedures (i.e., appropriate response prompting system and response prompts to teach the FCR, reinforcement), and other instructional considerations (i.e., precursor behaviors, FCT instructional arrangement, days/times for FCT instruction, setting for FCT instruction). The researcher and special educator incorporated these decisions into a lesson plan shared with the paraprofessional before baseline.
The lesson plan for Student 1 included the system of least prompts (Brown et al., 2019) to teach the student to request attention from an adult. The prompting hierarchy for teaching the student to select the communicative message on the Key Chain Talker (Attainment Company) was as follows: verbal (i.e., saying, “touch button”) → model (i.e., paraprofessional touching her lanyard to prompt the student to activate the single message “watch me” on the Key Chain Talker that was attached to the student’s personal lanyard). Reinforcement for correct prompted and unprompted responses involved the immediate delivery of paraprofessional attention in the form of eye contact and pleasant conversation for a period of 5 to 10 s. The lesson plans for Student 2 and 3 included a constant time delay procedure (Brown et al., 2019) to teach each student to request a short break during math instruction. For Student 2, full physical assistance (i.e., hand-over-hand prompting to activate the BIGmack® with the single message “I need a break”) served as the controlling prompt and reinforcement involved immediately providing the break (i.e., access to bubbles for 30 s). For Student 3, a gesture (i.e., pointing to the Accent 1000 to prompt the student to construct the sentence “I need a break” on the device) served as the controlling prompt and reinforcement involved immediately providing the break (i.e., access to a pre-identified toy for 30 s). For both of these students, paraprofessionals used a 0-s response interval throughout baseline and initial intervention sessions and a 3-s response interval during all subsequent sessions after having met the performance criteria for the 0-s delay constant time delay procedures.
Baseline
During baseline sessions, paraprofessionals delivered FCT to students during the target routines. Special educators provided a copy of the lesson plan to paraprofessionals and instructed them to follow the procedures outlined in the plan, including delivering FCT when precursor behaviors were observed. For Paraprofessionals 2 and 3, the special educators indicated that procedures for a 0-s response interval as noted in the lesson plan should be followed. The special educators did not provide additional directions or support to paraprofessionals during baseline.
Paraprofessional training intervention
Prior to delivering paraprofessional training, each special educator met with a research team member to participate in a single training session lasting between 25 and 43 min (M = 36 min). The purpose of the special educator training was twofold. First, we wanted to ensure each special educator was prepared to supervise and coach paraprofessionals in FCT implementation and had the knowledge and skills necessary to provide feedback on paraprofessional implementation of the identified response prompting system. Second, we wanted special educators well prepared to implement the paraprofessional training procedures. The training on FCT involved the following four components of BST (Reed et al., 2018): instruction, modeling, rehearsal, and feedback. Instruction was delivered through a PowerPoint presentation containing information about the student’s FBA results, an overview of FCT, and the FCT lesson plan specific to the target student. After viewing several video models of FCT implementation, the special educator and research team member engaged in a role-play to practice the response prompting system identified in the FCT lesson plan, with performance feedback provided by the research team member. The role-play continued until the special educator performed the response prompting system with 100% accuracy across two trials. Next, the research team member shared a PowerPoint containing information about the coaching process and facilitated a question and answer session.
After participating in the training with the researcher, special educators scheduled an initial training session with paraprofessionals. This session followed the same procedures as were implemented during the special educator training session, except that the special educator now delivered the training to the paraprofessional. Once the paraprofessional demonstrated 100% accuracy across two trials during role-play, the special educator instructed the paraprofessional to continue implementing FCT as outlined in the lesson plan. Subsequently, the special educator delivered follow-up coaching until the paraprofessional implemented FCT with 90% or higher across two consecutive sessions and, if implementation fidelity dropped below 90% at any point during intervention, coaching was reinstated. Follow-up coaching sessions also reflected the core components of BST and involved (a) reviewing the FCT lesson plan, (b) identifying and sharing video clips of procedural steps implemented correctly and incorrectly, (c) role-playing to practice procedures implemented incorrectly, and (d) providing performance feedback during and after role-plays. Coaching sessions were on average 10 min in length (range = 1–23 min). All components of BST were implemented in all coaching session, except the 1-min session to inform the paraprofessional she implemented with 100% fidelity and share video clips of procedural elements implemented correctly.
We measured treatment fidelity by collecting information on the extent to which the special educators adhered to the initial training and follow-up coaching protocols. After each training session, the special educator reported whether each training element was implemented by indicating “yes,” “no,” or “no opportunity to implement” using a checklist of training elements. Treatment fidelity was 100% across all special educators. A secondary observer accessed recorded training sessions to collect interobserver agreement (IOA) data across 33 to 50% of sessions. IOA for treatment fidelity was 100%.
Data Collection
During all sessions, a member of the research team video recorded paraprofessional implementation of FCT and student behavior during the target routines. Observations occurred one to three times per week depending on the classroom schedule and student attendance and spanned the course of 4 to 6 weeks for baseline and intervention depending on the triad. The first 10 min of recess were recorded for Triad 1. The average length of observations was 11 min (range = 7–13 min) for Triad 2 and 15 min (range = 14–15 min) for Triad 3. In addition, a member of the research team video recorded maintenance sessions for Triads 1 and 2 a month after the conclusion of intervention. Due to changes in classroom routine and behavior, we were unable to collect maintenance data for Triad 3. A member of the research team viewed the recordings and measured paraprofessional implementation of FCT using an implementation fidelity checklist. For each step on the checklist, the researcher marked “yes,” “no,” or “no opportunity” to indicate if the paraprofessional implemented each step correctly. We divided the number of steps implemented correctly by the number of steps the paraprofessional had the opportunity to implement and multiplied by 100 to calculate the percentage of steps implemented correctly. Mastery criteria were set at 90% or higher across three consecutive sessions.
A trained secondary observer collected IOA data across 33% to 43% of sessions in each condition. The secondary observer met with research team members to discuss coding disagreements and reach a consensus. Item-by-item agreement was calculated as the percentage of codes selected by both data collectors. The average IOA for paraprofessional FCT implementation was 99.6% (range = 96.7%–100%).
Social Validity
To examine the social validity of the special educator–delivered paraprofessional training intervention, we asked the special educators and paraprofessionals to participate in an anonymous social validity survey. Survey items were derived from the Training Acceptability Rating Scale (Davis et al., 1989). Participants reported their level of agreement (1 = strongly disagree, 6 = strongly agree) across items related to the training. The survey also included an open-ended item that allowed special educators and paraprofessionals to offer additional feedback related to the paraprofessional training intervention.
Results
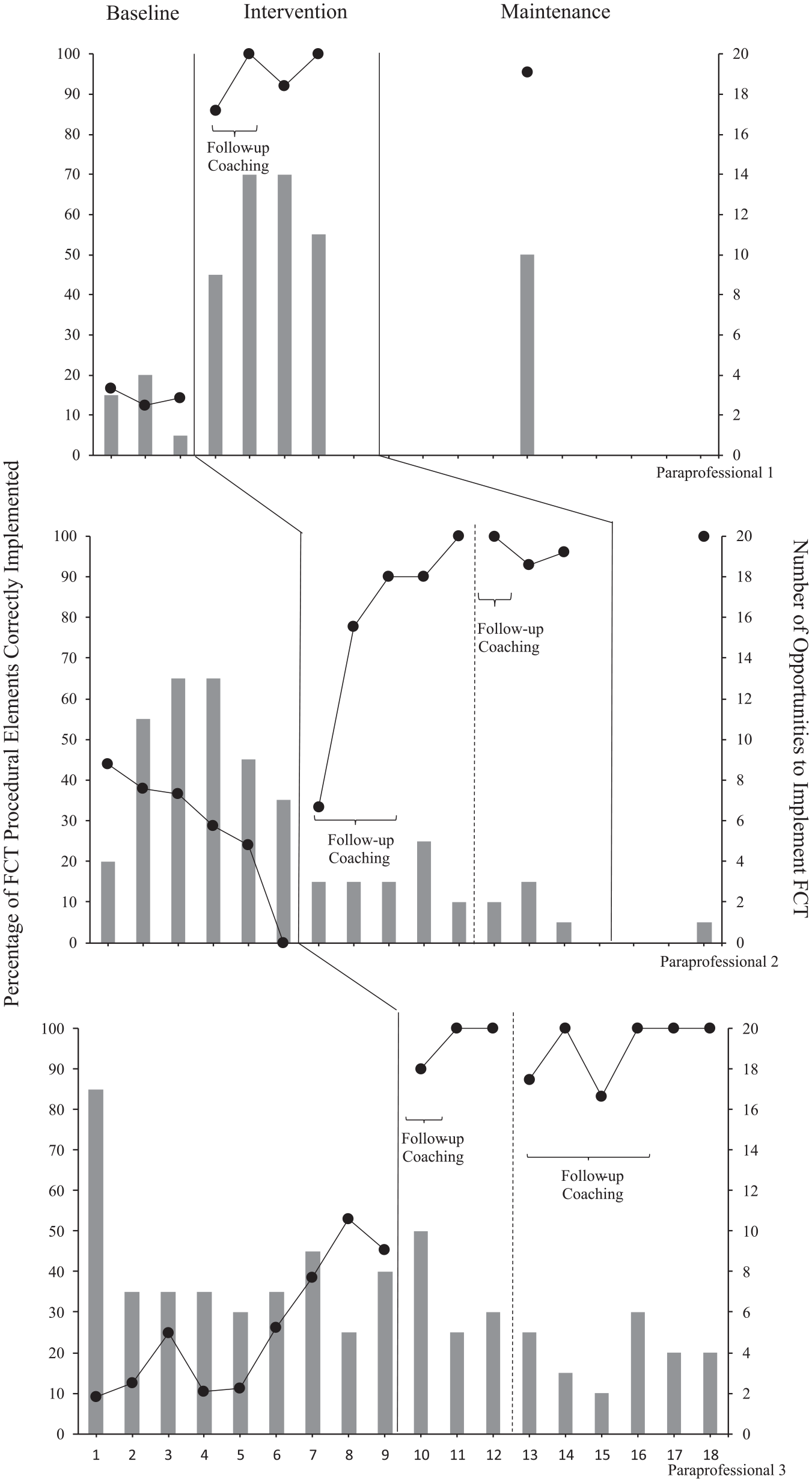
Our findings indicate a functional relation between the special educator–delivered paraprofessional training and paraprofessional implementation of FCT. Figure 1 depicts paraprofessional implementation data, including paraprofessional implementation fidelity and number of opportunities to implement FCT in the presence of precursor behaviors.
Paraprofessional implementation and opportunities to implement.
Triad 1
During baseline, Paraprofessional 1 displayed low levels of implementation with no trend and minimal variability (M = 14.5%, range = 12.5%–16.7%). After the initial training session, there was an immediate change in level with limited variability for the duration of the intervention. The mean implementation fidelity for Paraprofessional 1 during intervention was 94.5% (range = 86%–100%). Paraprofessional 1 required two additional sessions of follow-up coaching due to the performance requirements of implementing at 90% accuracy or greater across three consecutive sessions before discontinuation of coaching. Implementation fidelity was maintained at follow-up 1 month after the conclusion of intervention. Paraprofessional 1 met the mastery criteria in four sessions.
Triad 2
During baseline, Paraprofessional 2 displayed low levels of implementation with a decreasing trend and minimal variability (M = 28.5%, range = 0–43.8%). There was an immediate change in level after the initial training session with an increasing trend and limited variability during subsequent intervention sessions. The mean implementation fidelity during intervention was 84.9% (range = 33.3–100%). Paraprofessional 2 received a total of four follow-up coaching sessions before meeting the implementation requirements for the 0-s and 3-s response interval phases. Implementation fidelity was maintained at follow-up 1 month after the conclusion of intervention. Paraprofessional 2 met the mastery criteria for the 0-s response interval phase in five sessions and the 3-s response interval phase in three sessions.
Triad 3
Paraprofessional 3 displayed low-to-moderate levels of implementation during baseline with an overall increasing trend and minimal variability (M = 26.1%, range = 10.5–45.5%). After the initial training session, there was an immediate change in level and limited variability for the duration of the intervention. The mean implementation fidelity for Paraprofessional 3 during intervention was 94.6% (range = 83.3–100%). Paraprofessional 3 met the mastery criteria for the 0-s response interval phase in three sessions and the 3-s response interval phase in six sessions and required a total of five follow-up coaching sessions before meeting these criteria.
Social Validity
Two paraprofessionals and three special educators completed the anonymous social validity survey. In regard to the general acceptability of the teacher-delivered training intervention, paraprofessionals and special educators agreed that the training procedures were appropriate for paraprofessionals and learning about FCT. Overall, paraprofessionals agreed or strongly agreed (M = 3.94; SD = 0.24) with items related to the effectiveness, delivery, and value of the teacher-delivered training procedures, though one paraprofessional reported that her confidence in supporting the student’s challenging behavior improved only slightly. Likewise, special educators generally agreed or strongly agreed with these same items (M = 3.36; SD = 0.81). However, one special educator reported that her paraprofessional’s confidence improved only slightly and continued implementation after the conclusion of the study was unlikely.
Discussion
We conducted this study to examine the efficacy of special educator–delivered paraprofessional training on paraprofessional implementation of FCT among students with ASD. Given the continued reliance on paraprofessionals to assist educators in the delivery of special education and related services (U.S. Department of Education, 2019), it is critical to develop effective and sustainable training models to support paraprofessionals in their numerous roles. The results of this study extend the paraprofessional training literature in several ways. Although research suggests FCT is feasible to implement in school environments, there is limited research on paraprofessional implementation of FCT for students with ASD (Andzik et al., 2016; Walker et al., 2018). Paraprofessionals must be equipped with the knowledge and skills necessary to assist educators in delivering FCT when appropriate, especially given that paraprofessionals spend a significant portion of the school day addressing behavior, yet may not be adequately prepared to do so (Carter et al., 2009; Mason et al., 2020; Sobeck & Robertson, 2019). Another important way this study contributes to the literature is by examining whether special educators can deliver initial training and follow-up coaching with performance feedback to paraprofessionals. Although paraprofessionals can implement a wide range of behavioral interventions under the direction of a researcher, including function-based interventions like FCT (Walker, Carpenter et al., 2020), it is critical to develop training models that can be implemented in school settings by those who supervise paraprofessionals (Breton, 2010; Sobeck & Robertson, 2019). Knowing whether special educator–delivered training models are effective and socially valid from the perspective of both the trainer and trainee will provide the field with important information to inform guidelines for paraprofessional training programming.
Key Findings and Implications
The results of this study have several implications for practice. First, we found that special educators were able to implement paraprofessional training that was designed around BST, an evidence-based training practice that incorporates instruction, modeling, rehearsal, and feedback (Reed et al., 2018). Each special educator delivered an initial training session and subsequent follow-up coaching sessions until the paraprofessional met the performance criteria for mastery; the initial training and coaching protocols were followed with 100% implementation fidelity across participants and training sessions. Because BST has been highly effective across a range of contexts (e.g., Kirkpatrick et al., 2019), researchers have encouraged its use among special educators for paraprofessional training purposes (Yates et al., 2020). It should be noted that, in the current study, research team members supplied initial training, a structured coaching checklist, and consultative support to guide special educators’ delivery of the BST training elements. Although we strongly encourage special educators to consider BST for paraprofessional training, schools will need to identify strategies for preparing and supporting special educators to do so (Yates et al., 2019), as relying on outside researchers is not practical or sustainable. For example, a school team might assign a support person to oversee special educator paraprofessional training (e.g., school psychologist, behavior specialist) who can address logistics concerning scheduling and observations and ensure that coaching protocols are followed with fidelity while providing guidance on critical next steps in implementation (e.g., teaching tolerance of delays to reinforcement after initial FCT; Muharib & Pennington, 2019).
Second, our findings indicate that special educator–delivered training improved paraprofessional FCT implementation. In fact, paraprofessionals met the performance criteria for mastery with only a few relatively brief follow-up coaching sessions. This outcome is not surprising given that BST consists of approaches that have been identified as producing positive paraprofessional training outcomes (e.g., Brock & Anderson, 2020). It also was promising that high levels of FCT implementation were maintained 1 month after intervention ended and that Paraprofessional 2 began to accurately apply delayed reinforcement procedures (Muharib & Pennington, 2019) per our suggestion without any further coaching. Paraprofessional 1 also reported generalizing the procedures to other routines (e.g., lunch, reading). Although our study focused on one particular evidence-based practice, paraprofessionals could benefit from this type of training to acquire skills across a range of practices that reflects the numerous responsibilities they perform (Carter et al., 2009; Fisher & Pleasants, 2012). However, it will be important for educators to first determine the level of support needed as available training time might be limited and therefore might need to be prioritized for those skills that require a more intensive level of coaching (Wood et al., 2016).
All but one participant completed a social validity questionnaire and confirmed that the training was effective and practical for FCT implementation. Although participants in the current study did not report concerns about feasibility (e.g., limited training time, reduced classroom supervision during coaching sessions), noteworthy barriers to paraprofessional training and supervision have been raised by others (e.g., Douglas et al., 2016; Sobeck & Robertson, 2019). As such, schools will need to take these concerns into consideration and form creative solutions to encourage paraprofessional training among special educators (e.g., administrators scheduling dedicated time for training; assigning support person to oversee and facilitate training).
We descriptively examined student behavior over the course of the study. Challenging behavior decreased during baseline after FAO and remained low during intervention for Triad 1. Although implementation levels were not high in baseline, error analysis revealed that reinforcement serving the same function as challenging behavior was often delivered, which likely explains low levels during baseline. For Triads 2 and 3, challenging behavior decreased over the duration of the entire study, though data were highly variable, possibly due to missed opportunities to initiate FCT in the presence of precursor behavior. In the case of Triad 3, challenging behavior began to increase midway through intervention, possibly due to improved paraprofessional implementation leading to an extinction burst. Although students consistently emitted FCRs when prompted, the variability in independent responses raises important questions about the relationship between the response prompting systems and AAC devices selected by the team and FCT dosage that could not be explored in the current study.
Limitations and Future Research
In this section, we describe study limitations and how such limitations provide guidance for future research. First, the small number of participants limits the extent to which our findings can generalize to the broader population of special educators and paraprofessionals who support students with ASD. Replications will be needed across a larger and more diverse group of participants. Second, we did not measure generalization of paraprofessional FCT implementation nor did we examine the extent to which special educators could apply the same training process to teach different practices. This is a common limitation among paraprofessional training studies (e.g., Walker, Coogle, et al., 2020) and should be addressed in future research given the practical importance of applying newly acquired skills across different conditions (Stokes & Baer, 1977). We also were unable to examine variables that contributed to training dosage (e.g., prompting system used to teach FCR, differences in academic and social contexts). This will be an important area of future research given that time is often a limited resource for educators.
Third, the limited number of data points for Triad 1 and increasing baseline trend for Triad 3 may present limitations concerning establishing a functional relation. However, it is important to note that the What Works Clearinghouse (2017) guidelines for single case design studies provide flexibility in terms of the number of required data points for interventions involving dangerous challenging behavior. The student in Triad 1 inappropriately climbed and jumped off playground equipment which posed significant safety risks; therefore, a decision was made to avoid prolonging baseline beyond three sessions. Although the increasing baseline trend for Triad 3 is a concern, paraprofessional implementation decreased prior to intervention and remained at a low-to-moderate level over the course of baseline with an immediate change in level upon the introduction of coaching. The increase in implementation during baseline might have been attributed to maturation during a prolonged baseline.
Fourth, intervention was delivered in self-contained special education classrooms for two of the triads. Because paraprofessionals support students with disabilities in general education and special education classrooms, it is critical to explore models of support that address the unique characteristics of inclusive, general education environments. Research evidence indicates that individualized, function-based interventions can be implemented in inclusive school settings (Goh & Bambara, 2012; Walker et al., 2018). However, knowledge of paraprofessional-delivered function-based interventions in inclusive settings and the feasibility of paraprofessional training by general and special educators specific to such settings is severely limited. We highly recommend future research efforts directed toward exploring how to best support paraprofessionals and those with paraprofessional supervisory roles to address challenging behavior in inclusive settings. A fifth and final limitation is that our training model did not incorporate strategies to promote self-monitoring. Paraprofessional 1 frequently requested access to her implementation data as these data improved her motivation. Strategies to promote paraprofessionals in their own growth (e.g., access to visual representations of implementation progress, self-monitoring checklists) have the potential to reduce reliance on outside sources of feedback and promote independence in implementation (Douglas et al., 2016).
Conclusion
Although prior research suggests paraprofessionals can implement evidence-based practices to address challenging behavior with training, the research on special educator-implemented paraprofessional training is limited (Walker, Carpenter, et al., 2020). Our findings suggest that special educators can effectively and feasibly deliver initial training and follow-up coaching for paraprofessionals to implement FCT (Steinbrenner et al., 2020). We encourage special educators to consider training based on BST to improve paraprofessional implementation fidelity of behavior support plans. In addition, it will be important to continue and expand research in this area to inform paraprofessional training programming.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was sponsored by the Organization for Autism Research.